
Multiple Injections of Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-Analysis of Current Evidence in Randomized Controlled Trials

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Outcome Measures
2.5. Assessment of Methodological Quality
2.6. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics
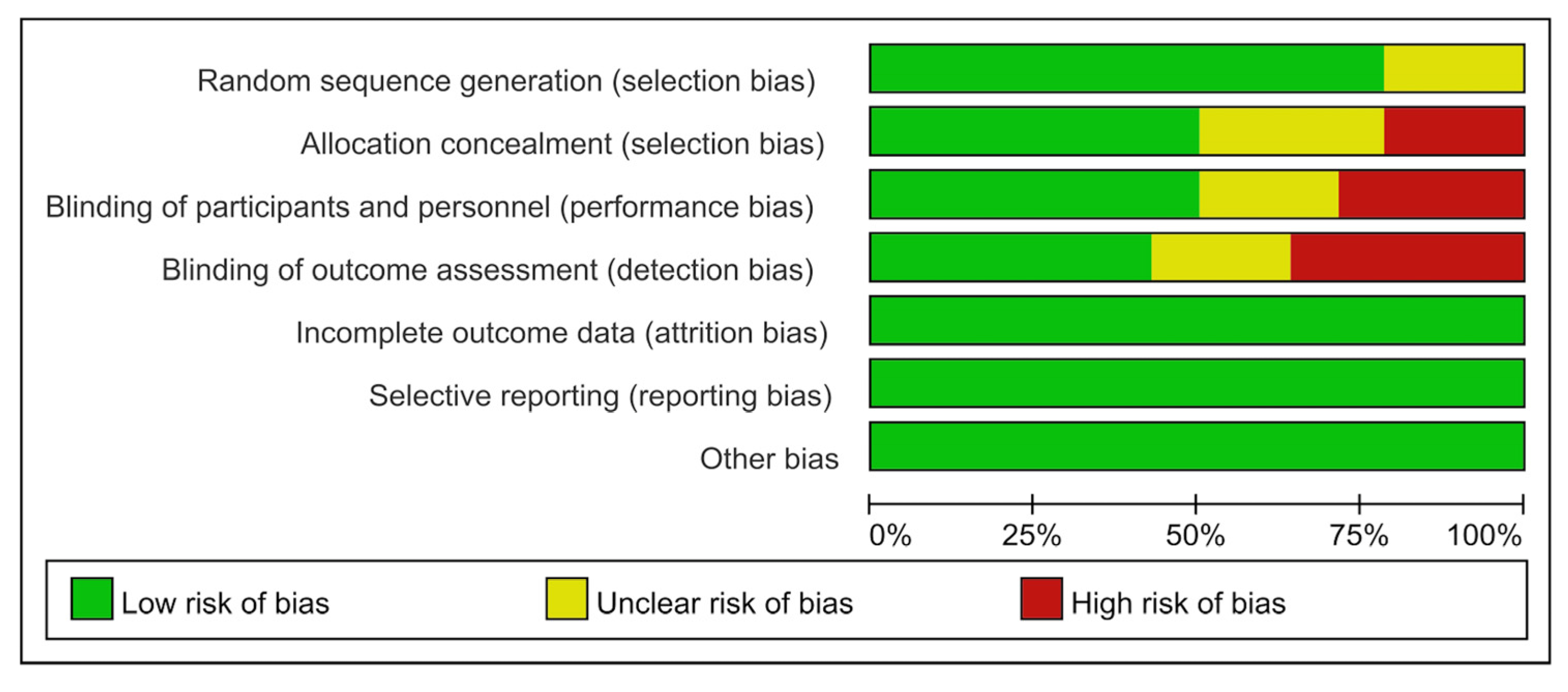
3.3. Risk of Bias
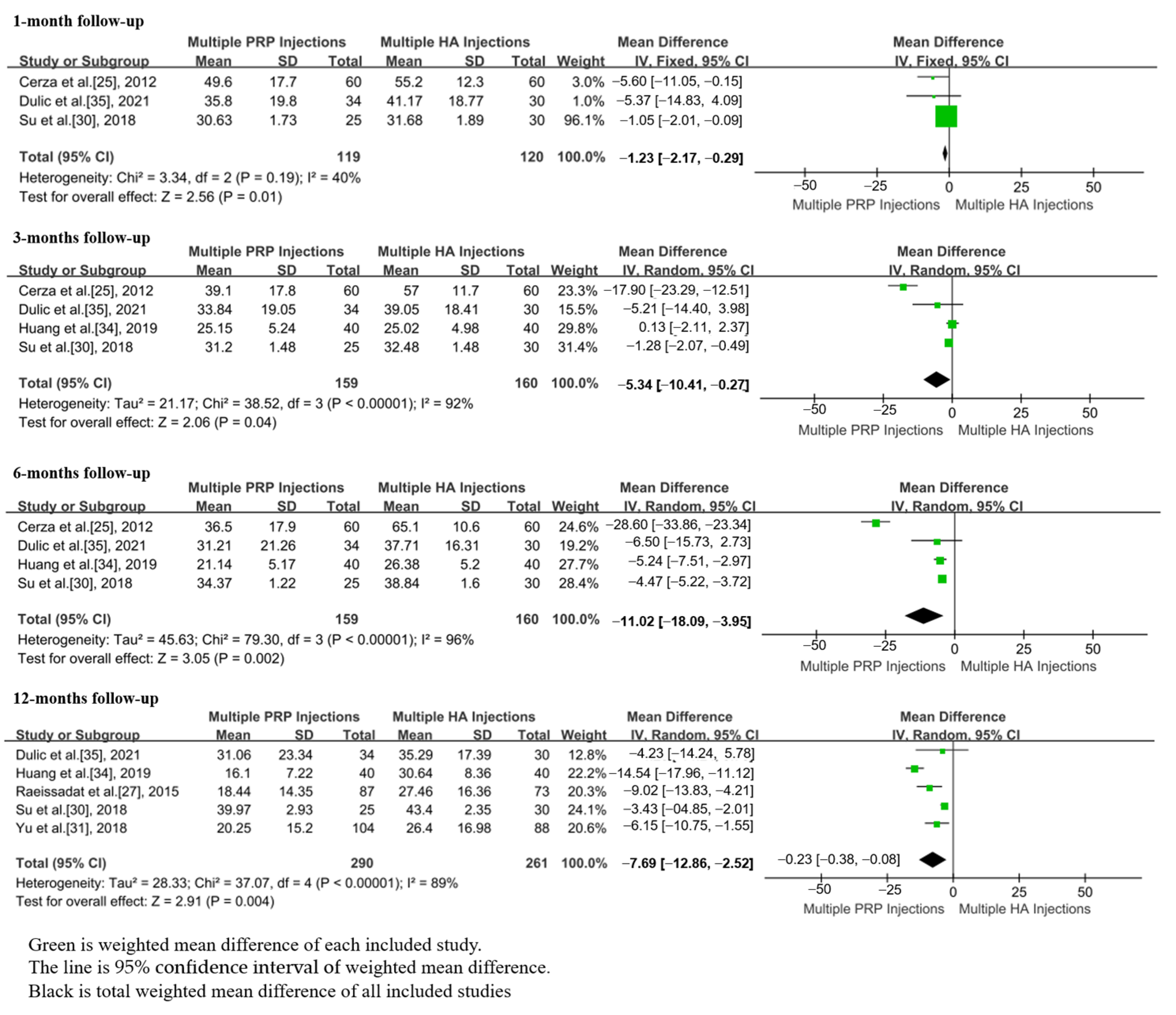
3.4. VAS Scores
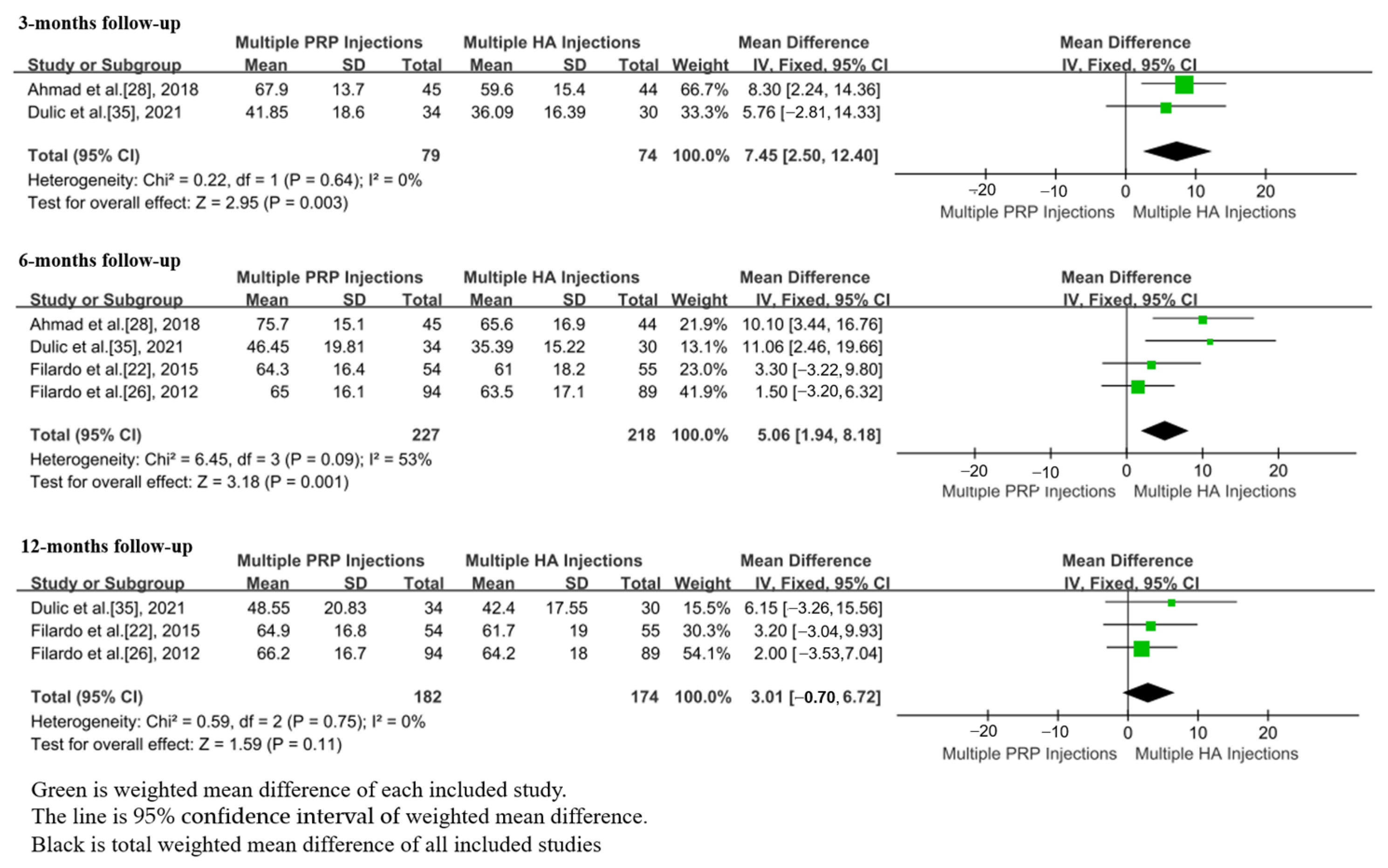
3.5. WOMAC Scores
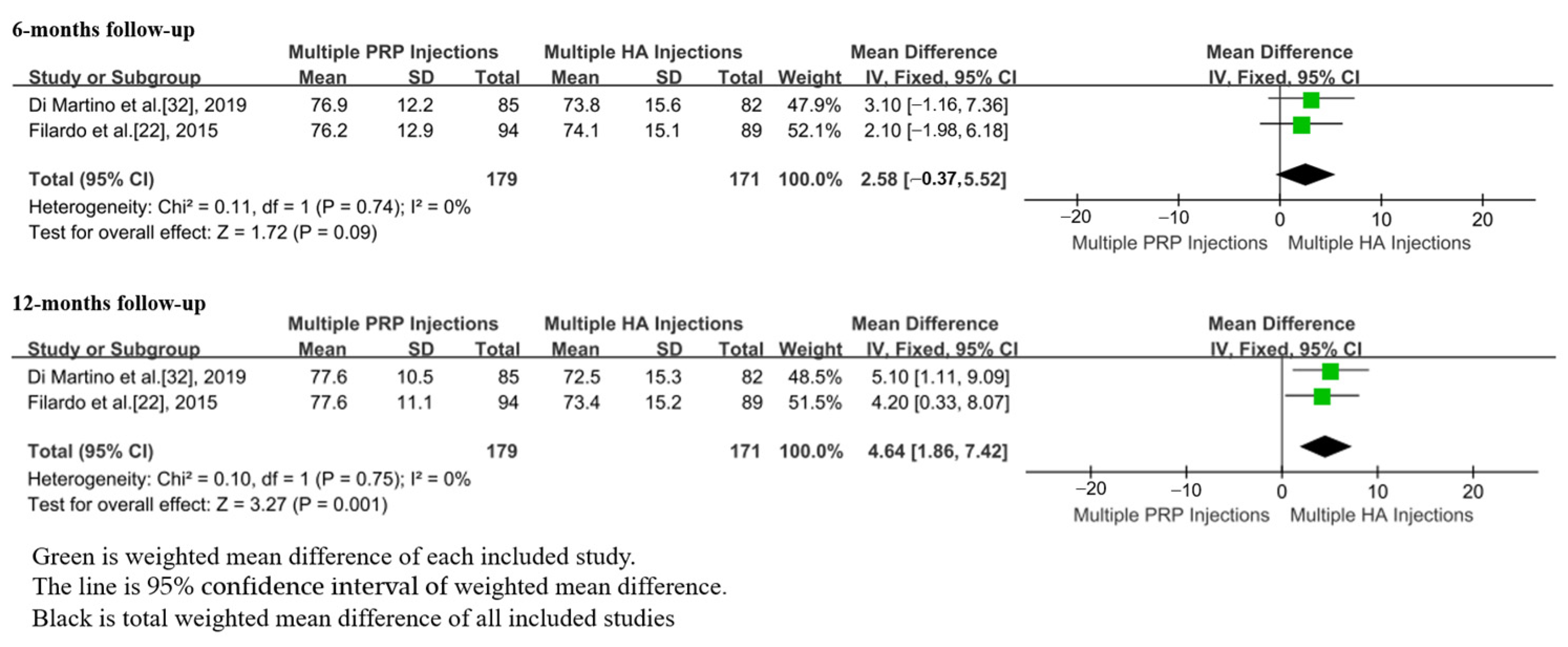
3.6. IKDC Scores
3.7. EQ-VAS Scores
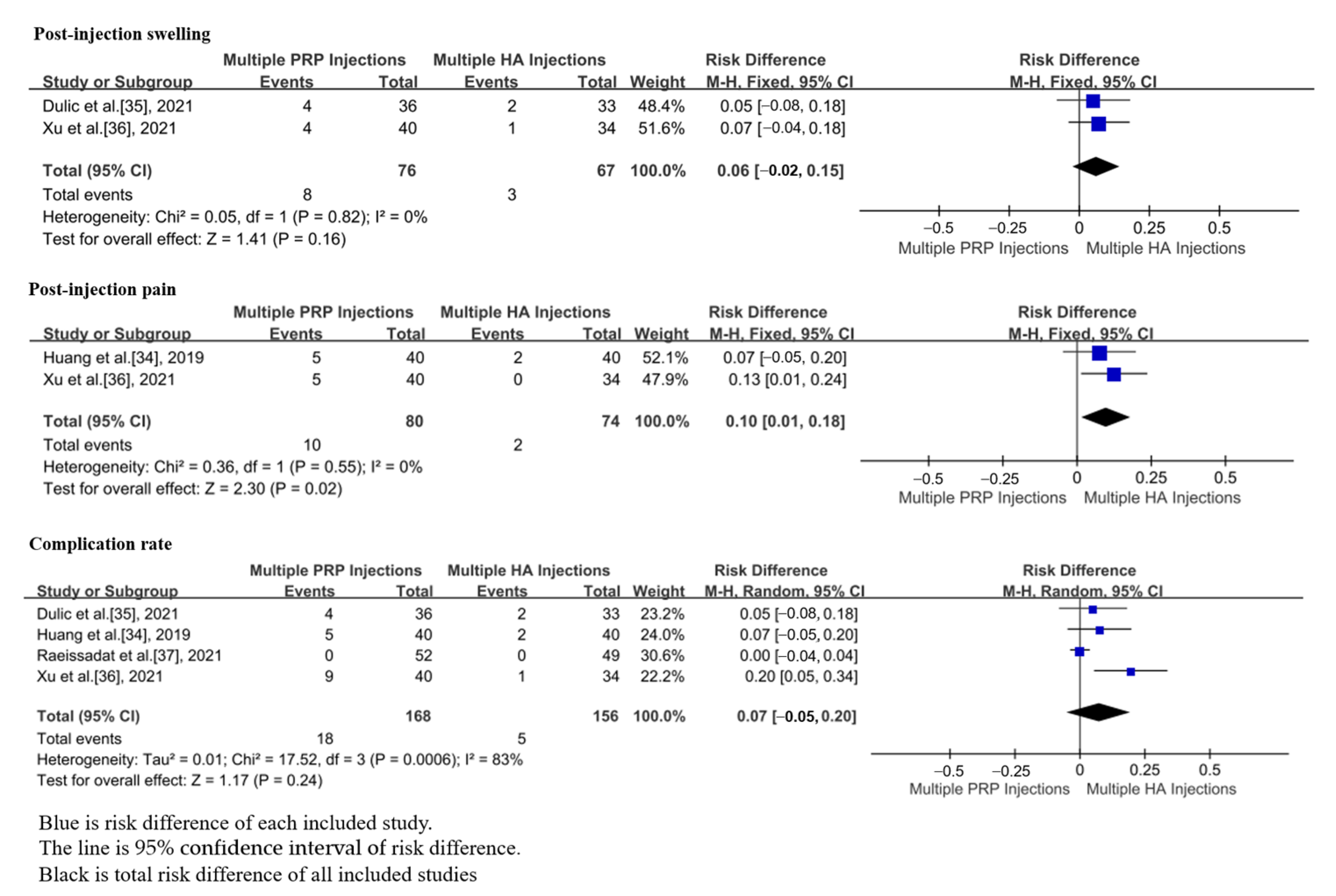
3.8. Adverse Effects
3.9. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, X.-X.; He, S.-H.; Liang, X.; Li, W.; Li, T.-F.; Li, D.-F. Aging, Cell Senescence, the Pathogenesis and Targeted Therapies of Osteoarthritis. Front. Pharmacol. 2021, 12, 728100. [Google Scholar] [CrossRef]
- Yi, N.; Mi, Y.; Xu, X.; Li, N.; Zeng, F.; Yan, K.; Tan, K.; Kuang, G.; Lu, M. Baicalein Alleviates Osteoarthritis Progression in Mice by Protecting Subchondral Bone and Suppressing Chondrocyte Apoptosis Based on Network Pharmacology. Front. Pharm. 2021, 12, 788392. [Google Scholar] [CrossRef]
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. Eclinicalmedicine 2020, 29–30, 100587. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Zong, Z.; Su, Z.; Chen, H.; Huang, J.; Niu, Y.; Zhong, H.; Wei, B. Recent Advances in Pharmacological Intervention of Osteoarthritis: A Biological Aspect. Front. Pharmacol. 2021, 12, 772678. [Google Scholar] [CrossRef]
- Liao, C.-D.; Huang, S.-W.; Huang, Y.-Y.; Lin, C.-L. Effects of Sarcopenic Obesity and Its Confounders on Knee Range of Motion Outcome after Total Knee Replacement in Older Adults with Knee Osteoarthritis: A Retrospective Study. Nutrients 2021, 13, 3817. [Google Scholar] [CrossRef] [PubMed]
- Yan, B.; Lv, S.; Tong, P.; Yan, L.; Chen, Z.; Zhou, L.; Yuan, Q.; Guo, L.; Shan, L. Intra-Articular Injection of Adipose-Derived Stem Cells Ameliorates Pain and Cartilage Anabolism/Catabolism in Osteoarthritis: Preclinical and Clinical Evidences. Front. Pharmacol. 2022, 13, 854025. [Google Scholar] [CrossRef]
- van Middelkoop, M.; Arden, N.; Atchia, I.; Birrell, F.; Chao, J.; Rezende, M.; Lambert, R.; Ravaud, P.; Bijlsma, J.; Doherty, M.; et al. The OA Trial Bank: Meta-analysis of individual patient data from knee and hip osteoarthritis trials show that patients with severe pain exhibit greater benefit from intra-articular glucocorticoids. Osteoarthr. Cartil. 2016, 24, 1143–1152. [Google Scholar] [CrossRef] [Green Version]
- Tenti, S.; Cheleschi, S.; Mondanelli, N.; Giannotti, S.; Fioravanti, A. New Trends in Injection-Based Therapy for Thumb-Base Osteoarthritis: Where Are We and where Are We Going? Front. Pharmacol. 2021, 12, 637904. [Google Scholar] [CrossRef]
- Webb, D.; Naidoo, P. Viscosupplementation for knee osteoarthritis: A focus on Hylan G-F 20. Orthop. Res. Rev. 2018, 10, 73–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, J.; Hu, Y.; Huang, L.; Huang, Z.-F.; Jiang, W.-Z.; Luo, Y.-Q.; Jia, M.-Y.; Chen, D.; Shi, Z.-J. Injection route affects intra-articular hyaluronic acid distribution and clinical outcome in viscosupplementation treatment for knee osteoarthritis: A combined cadaver study and randomized clinical trial. Drug Deliv. Transl. Res. 2020, 11, 279–291. [Google Scholar] [CrossRef]
- Miller, L.E.; Block, J.E. US-Approved Intra-Articular Hyaluronic Acid Injections are Safe and Effective in Patients with Knee Osteoarthritis: Systematic Review and Meta-Analysis of Randomized, Saline-Controlled Trials. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2013, 6, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Concoff, A.; Sancheti, P.; Niazi, F.; Shaw, P.; Rosen, J. The efficacy of multiple versus single hyaluronic acid injections: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2017, 18, 542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albanese, A.; E Licata, M.; Polizzi, B.; Campisi, G. Platelet-rich plasma (PRP) in dental and oral surgery: From the wound healing to bone regeneration. Immun. Ageing 2013, 10, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qian, Y.; Han, Q.; Chen, W.; Song, J.; Zhao, X.; Ouyang, Y.; Yuan, W.; Fan, C. Platelet-Rich Plasma Derived Growth Factors Contribute to Stem Cell Differentiation in Musculoskeletal Regeneration. Front. Chem. 2017, 5, 89. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Xing, F.; Luo, R.; Duan, X. Platelet-Rich Plasma for Bone Fracture Treatment: A Systematic Review of Current Evidence in Preclinical and Clinical Studies. Front. Med. 2021, 8, 676033. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Xing, F.; Luo, R.; Liu, M. Effectiveness of Platelet-Rich Plasma for Patients With Carpal Tunnel Syndrome: A Systematic Review and meta-Analysis of Current Evidence in Randomized Controlled Trials. Front. Pharmacol. 2022, 13, 834213. [Google Scholar] [CrossRef]
- Belk, J.W.; Kraeutler, M.J.; Houck, D.A.; Goodrich, J.A.; Dragoo, J.L.; Mccarty, E.C. Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Am. J. Sports Med. 2020, 49, 249–260. [Google Scholar] [CrossRef]
- Negrini, F.; De Lucia, F.; Negrini, S.; Tornese, D.; Facchini, F.; Vecchio, M.; de Girolamo, L. Case Report: Rehabilitation After Platelet-Rich Growth Factors’ Intra-Articular Injections for Knee Osteoarthritis: Two Case Reports of a Home-Based Protocol. Front. Pharmacol. 2021, 12, 718060. [Google Scholar] [CrossRef]
- Vilchez-Cavazos, F.; Millán-Alanís, J.; Blázquez-Saldaña, J.; Álvarez-Villalobos, N.; Peña-Martínez, V.; Acosta-Olivo, C.; Simental-Mendía, M. Comparison of the Clinical Effectiveness of Single Versus Multiple Injections of Platelet-Rich Plasma in the Treatment of Knee Osteoarthritis: A Systematic Review and Meta-analysis. Orthop. J. Sports Med. 2019, 7, 2325967119887116. [Google Scholar] [CrossRef] [Green Version]
- Yurtbay, A.; Say, F.; Çinka, H.; Ersoy, A. Ersoy, Multiple platelet-rich plasma injections are superior to single PRP injections or saline in osteoarthritis of the knee: The 2-year results of a randomized, double-blind, placebo-controlled clinical trial. Arch. Orthop. Trauma Surg. 2021, 142, 2755–2768. [Google Scholar] [CrossRef]
- Feller, J. Platelet-Rich Plasma Injections Were Not Better Than Hyaluronic Acid Injections for Knee Joint Degeneration. J. Bone Jt. Surg. 2016, 98, 315. [Google Scholar] [CrossRef] [PubMed]
- Filardo, G.; Di Matteo, B.; Di Martino, A.; Merli, M.; Cenacchi, A.; Fornasari, P.; Marcacci, M.; Kon, E. Platelet-Rich Plasma Intra-articular Knee Injections Show No Superiority Versus Viscosupplementation: A Randomized Controlled Trial. Am. J. Sport. Med. 2015, 43, 1575–1582. [Google Scholar] [CrossRef] [PubMed]
- van Tulder, M.W.; Assendelft, W.J.J.; Koes, B.W.; Bouter, L.M. Method guidelines for systematic reviews in the Cochrane Collaboration Back Review Group for spinal disorders. Spine 1997, 22, 2323–2330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oremus, M.; Wolfson, C.; Perrault, A.; Demers, L.; Momoli, F.; Moride, Y. Interrater reliability of the modified Jadad quality scale for systematic reviews of Alzheimer’s disease drug trials. Dement. Geriatr. Cogn. Disord. 2001, 12, 232–236. [Google Scholar] [CrossRef]
- Cerza, F.; Carnì, S.; Carcangiu, A.; Di Vavo, I.; Schiavilla, V.; Pecora, A.; De Biasi, G.; Ciuffreda, M. Comparison between hyaluronic acid and platelet-rich plasma, intra-articular infiltration in the treatment of gonarthrosis. Am. J. Sport. Med. 2012, 40, 2822–2827. [Google Scholar] [CrossRef]
- Filardo, G.; Kon, E.; Di Martino, A.; Di Matteo, B.; Merli, M.L.; Cenacchi, A.; Fornasari, P.M.; Marcacci, M. Platelet-rich plasma vs hyaluronic acid to treat knee degenerative pathology: Study design and preliminary results of a randomized controlled trial. BMC Musculoskelet. Disord. 2012, 13, 229. [Google Scholar] [CrossRef] [Green Version]
- Raeissadat, S.A.; Rayegani, S.M.; Hassanabadi, H.; Fathi, M.; Ghorbani, E.; Babaee, M.; Azma, K. Knee Osteoarthritis Injection Choices: Platelet- Rich Plasma (PRP) Versus Hyaluronic Acid (A one-year randomized clinical trial). Clin. Med. Insights Arthritis Musculoskelet. Disord. 2015, 8, 1–8. [Google Scholar] [CrossRef]
- Ahmad, H.S.; Farrag, S.E.; Okasha, A.E.; Kadry, A.O.; Ata, T.B.; Monir, A.A.; Shady, I. Clinical outcomes are associated with changes in ultrasonographic structural appearance after platelet-rich plasma treatment for knee osteoarthritis. Int. J. Rheum. Dis. 2018, 21, 960–966. [Google Scholar] [CrossRef]
- Lisi, C.; Perotti, C.; Scudeller, L.; Sammarchi, L.; Dametti, F.; Musella, V.; Di Natali, G. Treatment of knee osteoarthritis: Platelet-derived growth factors vs. hyaluronic acid. A randomized controlled trial. Clin. Rehabil. 2017, 32, 330–339. [Google Scholar] [CrossRef]
- Su, K.; Bai, Y.; Wang, J.; Zhang, H.; Liu, H.; Ma, S. Comparison of hyaluronic acid and PRP intra-articular injection with combined intra-articular and intraosseous PRP injections to treat patients with knee osteoarthritis. Clin. Rheumatol. 2018, 37, 1341–1350. [Google Scholar] [CrossRef]
- Yu, W.; Xu, P.; Huang, G.; Liu, L. Clinical therapy of hyaluronic acid combined with platelet-rich plasma for the treatment of knee osteoarthritis. Exp. Ther. Med. 2018, 16, 2119–2125. [Google Scholar] [CrossRef] [Green Version]
- Di Martino, A.; Di Matteo, B.; Papio, T.; Tentoni, F.; Selleri, F.; Cenacchi, A.; Kon, E.; Filardo, G. Filardo, Platelet-Rich Plasma Versus Hyaluronic Acid Injections for the Treatment of Knee Osteoarthritis: Results at 5 Years of a Double-Blind, Randomized Controlled Trial. Am. J. Sports Med. 2019, 47, 347–354. [Google Scholar] [CrossRef]
- Lin, K.-Y.; Yang, C.-C.; Hsu, C.-J.; Yeh, M.-L.; Renn, J.-H. Intra-articular Injection of Platelet-Rich Plasma Is Superior to Hyaluronic Acid or Saline Solution in the Treatment of Mild to Moderate Knee Osteoarthritis: A Randomized, Double-Blind, Triple-Parallel, Placebo-Controlled Clinical Trial. Arthrosc. J. Arthrosc. Relat. Surg. 2019, 35, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Liu, X.; Xu, X.; Liu, J. Intra-articular injections of platelet-rich plasma, hyaluronic acid or corticosteroids for knee osteoarthritis: A prospective randomized controlled study. Orthopade 2019, 48, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Dulic, O.; Rasovic, P.; Lalic, I.; Kecojevic, V.; Gavrilovic, G.; Abazovic, D.; Maric, D.; Miskulin, M.; Bumbasirevic, M. Bone Marrow Aspirate Concentrate versus Platelet Rich Plasma or Hyaluronic Acid for the Treatment of Knee Osteoarthritis. Medicina 2021, 57, 1193. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; He, Z.; Shu, L.; Li, X.; Ma, M.; Ye, C. Intra-Articular Platelet-Rich Plasma Combined With Hyaluronic Acid Injection for Knee Osteoarthritis Is Superior to Platelet-Rich Plasma or Hyaluronic Acid Alone in Inhibiting Inflammation and Improving Pain and Function. Arthrosc. J. Arthrosc. Relat. Surg. 2020, 37, 903–915. [Google Scholar] [CrossRef] [PubMed]
- Raeissadat, S.A.; Hosseini, P.G.; Bahrami, M.H.; Roghani, R.S.; Fathi, M.; Ahangar, A.G.; Darvish, M. The comparison effects of intra-articular injection of Platelet Rich Plasma (PRP), Plasma Rich in Growth Factor (PRGF), Hyaluronic Acid (HA), and ozone in knee osteoarthritis; a one year randomized clinical trial. BMC Musculoskelet. Disord. 2021, 22, 134. [Google Scholar] [CrossRef] [PubMed]
- Paik, J.; Duggan, S.T.; Keam, S.J. Triamcinolone Acetonide Extended-Release: A Review in Osteoarthritis Pain of the Knee. Drugs 2019, 79, 455–462. [Google Scholar] [CrossRef] [Green Version]
- Kraus, V.; Conaghan, P.; Aazami, H.; Mehra, P.; Kivitz, A.; Lufkin, J.; Hauben, J.; Johnson, J.; Bodick, N. Synovial and systemic pharmacokinetics (PK) of triamcinolone acetonide (TA) following intra-articular (IA) injection of an extended-release microsphere-based formulation (FX006) or standard crystalline suspension in patients with knee osteoarthritis (OA). Osteoarthr. Cartil. 2017, 26, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Xing, F.; Zhou, C.; Hui, D.; Du, C.; Wu, L.; Wang, L.; Wang, W.; Pu, X.; Gu, L.; Liu, L.; et al. Hyaluronic acid as a bioactive component for bone tissue regeneration: Fabrication, modification, properties, and biological functions. Nanotechnol. Rev. 2020, 9, 1059–1079. [Google Scholar] [CrossRef]
- Temple-Wong, M.M.; Ren, S.; Quach, P.; Hansen, B.C.; Chen, A.C.; Hasegawa, A.; D’Lima, D.D.; Koziol, J.; Masuda, K.; Lotz, M.K.; et al. Hyaluronan concentration and size distribution in human knee synovial fluid: Variations with age and cartilage degeneration. Thromb. Haemost. 2016, 18, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, R.C.; Lall, R.; Srivastava, A.; Sinha, A. Hyaluronic Acid: Molecular Mechanisms and Therapeutic Trajectory. Front. Veter-Sci. 2019, 6, 192. [Google Scholar] [CrossRef] [Green Version]
- Maheu, E.; Zaim, M.; Appelboom, T.; Jeka, S.; Trc, T.; Maasalu, K.; Berenbaum, F. Comparative efficacy and safety of two different molecular weight (MW) hyaluronans F60027 and Hylan G-F20 in symptomatic osteoarthritis of the knee (KOA). Results of a non inferiority, prospective, randomized, controlled trial. Ann. Rheum. Dis. 2011, 29, 527–535. [Google Scholar]
- Gigis, I.; Fotiadis, E.; Nenopoulos, A.; Tsitas, K.; Hatzokos, I. Comparison of two different molecular weight intra-articular injections of hyaluronic acid for the treatment of knee osteoarthritis. Hippokratia 2016, 20, 26–31. [Google Scholar] [PubMed]
- Li, S.; Xing, F.; Luo, R.; Liu, M. Clinical Effectiveness of Platelet-Rich Plasma for Long-Bone Delayed Union and Nonunion: A Systematic Review and Meta-Analysis. Front. Med. 2022, 8, 771252. [Google Scholar] [CrossRef]
- Xing, F.; Li, L.; Zhou, C.; Long, C.; Wu, L.; Lei, H.; Kong, Q.; Fan, Y.; Xiang, Z.; Zhang, X. Regulation and Directing Stem Cell Fate by Tissue Engineering Functional Microenvironments: Scaffold Physical and Chemical Cues. Stem Cells Int. 2019, 2019, 2180925. [Google Scholar] [CrossRef] [Green Version]
- Fei, X.; Lang, L.; Lingjiao, H.; Wei, C.; Zhou, X. Platelet-rich plasma has better mid-term clinical results than traditional steroid injection for plantar fasciitis: A systematic review and meta-analysis. Orthop. Traumatol. Surg. Res. 2021, 107, 103007. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Zhu, T.; Xue, J.; Zhang, Y.; Lu, Y.; Yang, H.; Yu, Z.; Zhu, Y.; Zhu, X. Influence of bFGF on in vitro expansion and chondrogenic construction of articular cartilage-derived progenitor cells. Ann. Transl. Med. 2022, 10, 36. [Google Scholar] [CrossRef]
- Sun, J.; Xing, F.; Zou, M.; Gong, M.; Li, L.; Xiang, Z. Comparison of chondrogenesis-related biological behaviors between human urine-derived stem cells and human bone marrow mesenchymal stem cells from the same individual. Stem Cell Res. Ther. 2021, 12, 366. [Google Scholar] [CrossRef]
- Bennell, K.L.; Hunter, D.J.; Paterson, K. Platelet-Rich Plasma for the Management of Hip and Knee Osteoarthritis. Curr. Rheumatol. Rep. 2017, 19, 24. [Google Scholar] [CrossRef]
- Xing, F.; Li, S.; Yin, D.; Xie, J.; Rommens, P.M.; Xiang, Z.; Liu, M.; Ritz, U. Recent progress in Mg-based alloys as a novel bioabsorbable biomaterials for orthopedic applications. J. Magnes. Alloy. 2022, 10, 1428–1456. [Google Scholar] [CrossRef]
- Wang, M.; Gao, W. Fixation of platelet-rich plasma and fibrin gels on knee cartilage defects after microfracture with arthroscopy. Int. Orthop. 2022, 46, 1761–1766. [Google Scholar] [CrossRef]
- Meheux, C.J.; McCulloch, P.C.; Lintner, D.M.; Varner, K.E.; Harris, J.D. Harris, Efficacy of Intra-articular Platelet-Rich Plasma Injections in Knee Osteoarthritis: A Systematic Review. Arthrosc. J. Arthrosc. Relat. Surg. 2016, 32, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Han, S.-B.; Seo, I.-W.; Shin, Y.-S. Intra-Articular Injections of Hyaluronic Acid or Steroids Associated With Better Outcomes Than Platelet-Rich Plasma, Adipose Mesenchymal Stromal Cells, or Placebo in Knee Osteoarthritis: A Network Meta-analysis. Arthrosc. J. Arthrosc. Relat. Surg. 2020, 37, 292–306. [Google Scholar] [CrossRef]
- Aw, N.M.-Y.; Yeo, S.-J.; Wylde, V.; Wong, S.B.; Chan, D.; Thumboo, J.; Leung, Y.Y. Impact of pain sensitisation on the quality of life of patients with knee osteoarthritis. RMD Open 2022, 8, e001938. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.-D.; Huang, Y.-Y.; Chen, H.-C.; Liou, T.-H.; Lin, C.-L.; Huang, S.-W. Relative Effect of Extracorporeal Shockwave Therapy Alone or in Combination with Noninjective Treatments on Pain and Physical Function in Knee Osteoarthritis: A Network Meta-Analysis of Randomized Controlled Trials. Biomedicines 2022, 10, 306. [Google Scholar] [CrossRef] [PubMed]
- Previtali, D.; Capone, G.; Marchettini, P.; Candrian, C.; Zaffagnini, S.; Filardo, G. High Prevalence of Pain Sensitization in Knee Osteoarthritis: A Meta-Analysis with Meta-Regression. Cartilage 2022, 13, 19476035221087698. [Google Scholar] [CrossRef]
- E Vriezekolk, J.; Peters, Y.A.S.; Steegers, M.A.H.; Davidson, E.N.B.; Ende, C.H.M.V.D. Pain descriptors and determinants of pain sensitivity in knee osteoarthritis: A community-based cross-sectional study. Rheumatol. Adv. Pract. 2022, 6, rkac016. [Google Scholar] [CrossRef]
- Edwards, R.R.; Campbell, C.; Schreiber, K.L.; Meints, S.; Lazaridou, A.; Martel, M.O.; Cornelius, M.; Xu, X.; Jamison, R.N.; Katz, J.N.; et al. Multimodal prediction of pain and functional outcomes 6 months following total knee replacement: A prospective cohort study. BMC Musculoskelet. Disord. 2022, 23, 302. [Google Scholar] [CrossRef]
- Pavone, V.; Vescio, A.; Turchetta, M.; Giardina, S.M.C.; Culmone, A.; Testa, G. Injection-Based Management of Osteoarthritis of the Knee: A Systematic Review of Guidelines. Front. Pharmacol. 2021, 12, 661805. [Google Scholar] [CrossRef]
- Altman, R.; Hackel, J.; Niazi, F.; Shaw, P.; Nicholls, M. Efficacy and safety of repeated courses of hyaluronic acid injections for knee osteoarthritis: A systematic review. Semin. Arthritis Rheum. 2018, 48, 168–175. [Google Scholar] [CrossRef]
- Lu, Z.; Li, X.; Chen, R.; Guo, C. Kinesio taping improves pain and function in patients with knee osteoarthritis: A meta-analysis of randomized controlled trials. Int. J. Surg. 2018, 59, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar] [PubMed]
- Rossi, M.; Lubowitz, J.; Guttmann, D. Development and validation of the International Knee Documentation Committee Subjective Knee Form. Am. J. Sport. Med. 2002, 30, 152. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Yun, S.; Hong, J. Health-related quality of life measured with the EQ-5D-5L in critical care survivors: A cross-sectional study. Intensiv. Crit. Care Nurs. 2022, 72, 103252. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Country | Patients (P/H) | Age (Years) (P/H) | Male (P/H) | Interventions (P/H) | Follow-Up (Months) |
|---|---|---|---|---|---|---|
| Cerza et al. [25], 2012 | Rome, Italy | 60/60 | 66.5 (11.3)/66.2 (10.6) | 25/28 | PRP 4 IA/HA 4 IA | 6 |
| Filardo et al. [26], 2012 | Bologna, Italy | 54/55 | 55/58 | 37/31 | PRP 3 IA/HA 3 IA | 12 |
| Filardo et al. [22], 2015 | Bologna, Italy | 94/89 | 53.32 ± 13.2/57.55 ± 11.8 | 60/52 | PRP 3 IA/HA3 IA | 12 |
| Raeissadat et al. [27], 2015 | Tehran, Iran | 87/73 | 56.85 ± 9.13/61.13 ± 7.48 | 8/15 | PRP 2 IA/HA 3 IA | 12 |
| Ahmad et al. [28], 2018 | Mansoura, Egypt | 45/44 | 56.2 ± 6.8/56.8 ± 7.4 | 14/14 | PRP 3 IA/HA 3 IA | 6 |
| Lisi et al. [29], 2018 | Pavia, Italy | 30/28 | 54.4(15.1)/57.1(10.0) | 20/16 | PRP 3 IA/HA 3 IA | 6 |
| Su et al. [30], 2018 | Hebei, China | 25/30 | 54.16 ± 6.56/53.13 ± 6.41 | 11/12 | PRP 2 IA/HA 5 IA | 18 |
| Yu et al. [31], 2018 | Shanxi, China | 104/88 | 46.2 ± 8.6/51.5 ± 9.3 | 50/48 | PRP 4 IA/HA 4 IA | 12 |
| Lin et al. [33], 2019 | Taiwan | 31/29 | 61.17 ± 13.08/62.53 ± 9.9 | 9/10 | PRP 3 IA/HA3 IA | 12 |
| Huang et al. [34], 2019 | Jining, China | 40/40 | 54.5 ± 1.2/54.8 ± 1.1 | 25/19 | PRP 3 IA/HA3 IA | 12 |
| Di Martino et al. [32], 2019 | Bologna, Italy | 85/82 | 52.7 ± 13.2/57.5 ± 11.7 | 53/47 | PRP 3 IA/HA3 IA | 24 |
| Dulic et al. [35], 2021 | Belgrade, Serbia | 34/30 | 58.8 ± 11.2/59.4 ± 14.0 | 15/13 | PRP 3 IA/HA3 IA | 12 |
| Xu et al. [36], 2021 | Guiyang, China | 40/34 | 56.9± 4.2/57.1 ± 3.4 | 10/5 | PRP 3 IA/HA3 IA | 12 |
| Raeissadat et al. [37], 2021 | Tehran, Iran | 52/49 | 56.09 ± 6.0/57.91 ± 6.7 | 13/12 | PRP 2 IA/HA 3 IA | 12 |
| Author (Year) | Injection Frequency | PRP Preparation | Excluding Platelet Count | HA Component | PRP Dosage | HA Dosage |
|---|---|---|---|---|---|---|
| Cerza et al. [25], 2012 | Both PRP and HA were performed once a week. | No reported preparation. LP-PRP | Less than 150,000/μL | 20 mg/2 mL (Hyalgan, Fidia, Abano Terme, Italy) | 5.5 mL | 2 mL |
| Filardo et al. [26], 2012 | Both PRP and HA were performed once a week. | 150 mL venous blood underwent 2 centrifugations (1480 rpm for 6 min and 3400 rpm for 15 min), producing 20 mL PRP; 5 mL every time; LR-PRP | Less than 150,000/μL | Molecular weight < 1500 kDa, (Hyalubrix, Fidia, Abano Terme (PD), Italy) | 5 mL | NR |
| Filardo et al. [22], 2015 | Both PRP and HA were performed once a week. | 150 mL venous blood underwent 2 centrifugations (1480 rpm for 6 min and 3400 rpm for 15 min) producing 20 mL PRP; 5 mL every time; LR-PRP | Less than 150,000/μL | Molecular weight < 1500 kDa, (Hyalubrix 30 mg/2 mL, Fidia SpA) | 5 mL | 2 mL |
| Raeissadat et al. [27], 2015 | PRP was performed once every 4 weeks; HA was performed once a week. | 35–40 mL venous blood underwent 2 centrifugations (1600 rpm for 15 min and 2800 rpm for 7 min), producing 4–6 mL PRP. LR-PRP | Less than 150,000/mL | Molecular weight 500,000–730,000 Da. (Hyalgan, Fidia Farmaceutici S.p.A., Abano Terme, Italy) | 4–6 mL | 2 mL |
| Ahmad et al. [28], 2018 | Both PRP and HA were performed once every 2 weeks. | 8 mL venous blood underwent centrifugation (3500 rpm for 9 min) producing 4 mL PRP; LR-PRP | NR | NR | 4 mL | 2 mL |
| Lisi et al. [29], 2018 | Both PRP and HA were performed once every 4 weeks. | 20 mL venous blood underwent centrifugation (900 rpm for 7 min), producing PRP. | NR | 20 mg/2 mL (Hyalgan; Fidia, Abano Terme, Italy) | NA | 2 mL |
| Su et al. [30], 2018 | PRP was performed once every 2 weeks; HA was performed once a week. | 45 mL venous blood underwent 2 centrifugations (1480 rpm for 6 min and 3400 rpm for 15 min) producing 7 mL PRP. LR-PRP | NR | Molecular weight was 0.6–1.5 million Daltons. (Freda, Shandong, China) | 6 mL | 2 mL |
| Yu et al. [31], 2018 | Both PRP and HA were performed once a week. | PRP from Sigma-Aldrich (Merck KGaA, Darmstadt, Germany) | NR | Only HA (Sigma-Aldrich; Merck KGaA) | 2–14 mL | NR |
| Lin et al. [33], 2019 | Both PRP and HA were performed once a week. | 10 mL venous blood underwent centrifugation (1500 rpm for 8 min), producing 5 ± 0.5 mL PRP. LP-PRP. | Less than 150,000/μL | Hyruan Plus, 20 mg/2 mL; molecular weight > 2500 kDa; (LG Chem, Seoul, Republic of Korea) | 2 mL | 2 mL |
| Huang et al. [34], 2019 | PRP was performed once every 3 weeks; HA was performed once a week. | 8 mL venous blood underwent centrifugation (3500 rpm for 5 min), producing PRP. LP-PRP. | Less than 150,000/L | Sodium hyaluronate, molecular weight 500–730 kDa (SK chemical research Co., Ltd., Tokyo, Japan) | NR | NR |
| Di Martino et al. [32], 2019 | Both PRP and HA were performed once a week. | 150 mL venous blood underwent 2 centrifugations (1480 rpm for 6 min and 3400 rpm for 15 min), producing 20 mL PRP. LR-PRP. | Less than 150,000/μL | Molecular weight > 1500 KDa, 30 mg/2 mL, (Hyalubrix; Fidia SpA). | 5 mL | 2 mL |
| Dulic et al. [35], 2021 | Both PRP and HA were performed once a week. | 60 mL venous blood underwent 2 centrifugations producing PRP. LP-PRP. | NR | Molecular weight 4000 kDa, (Cartinorm, Goodwill Pharma, Hungary) | NR | 2 mL |
| Xu et al. [36], 2021 | Both PRP and HA were performed once every 2 weeks. | 36 mL venous blood underwent 2 centrifugations (160 G for 10 min and 250 G for 15 min), producing PRP. LP-PRP. | NR | Molecular weight 2500 kDa, (SOFAST, 2 mL/20 mg, Shandong, China) | 4 mL | 2 mL |
| Raeissadat et al. [37], 2021 | PRP was performed once every 3 weeks; HA was performed once a week. | 35 mL venous blood underwent 2 centrifugations (1600 rpm for 15 min and 3500 rpm for 7 min), producing 2 mL PRP. LR-PRP. | Less than 150,000/μL | Molecular weight between 500 to 730 kDa, (Hyalgan, Fidia Farmaceutici S.p.A., Abano Terme, Italy) | 2 mL | NR |
| Study (Year) | Randomization | Concealment of Allocation | Double Blinding | Total Withdrawals and Dropouts | Total |
|---|---|---|---|---|---|
| Cerza et al. [25], 2012 | * | - | - | * | 2 |
| Filardo et al. [26], 2012 | ** | ** | ** | * | 7 |
| Filardo et al. [22], 2015 | ** | ** | ** | * | 7 |
| Raeissadat et al. [27], 2015 | ** | - | - | * | 3 |
| Ahmad et al. [28], 2018 | * | * | * | * | 4 |
| Lisi et al. [29], 2018 | ** | ** | ** | * | 7 |
| Su et al. [30], 2018 | ** | - | - | * | 3 |
| Yu et al. [31], 2018 | * | * | * | * | 4 |
| Lin et al. [33], 2019 | ** | ** | ** | * | 7 |
| Huang et al. [34], 2019 | * | - | - | * | 2 |
| Di Martino et al. [32], 2019 | * | * | ** | * | 5 |
| Dulic et al. [35], 2021 | ** | - | - | * | 3 |
| Xu et al. [36], 2021 | * | ** | ** | * | 6 |
| Raeissadat et al. [37], 2021 | ** | ** | ** | * | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, S.; Xing, F.; Yan, T.; Zhang, S.; Chen, F. Multiple Injections of Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-Analysis of Current Evidence in Randomized Controlled Trials. J. Pers. Med. 2023, 13, 429. https://doi.org/10.3390/jpm13030429
Li S, Xing F, Yan T, Zhang S, Chen F. Multiple Injections of Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-Analysis of Current Evidence in Randomized Controlled Trials. Journal of Personalized Medicine. 2023; 13(3):429. https://doi.org/10.3390/jpm13030429
Chicago/Turabian StyleLi, Shang, Fei Xing, Tongtong Yan, Siya Zhang, and Fengchao Chen. 2023. "Multiple Injections of Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-Analysis of Current Evidence in Randomized Controlled Trials" Journal of Personalized Medicine 13, no. 3: 429. https://doi.org/10.3390/jpm13030429