
Readiness to Accept Genetic Testing for Personalized Medicine: Survey Findings on the Role of Socio-Demographic Characteristics, Health Vulnerabilities, Perceived Genetic Risk and Personality Factors
Abstract
:1. Introduction
2. Materials and Methods
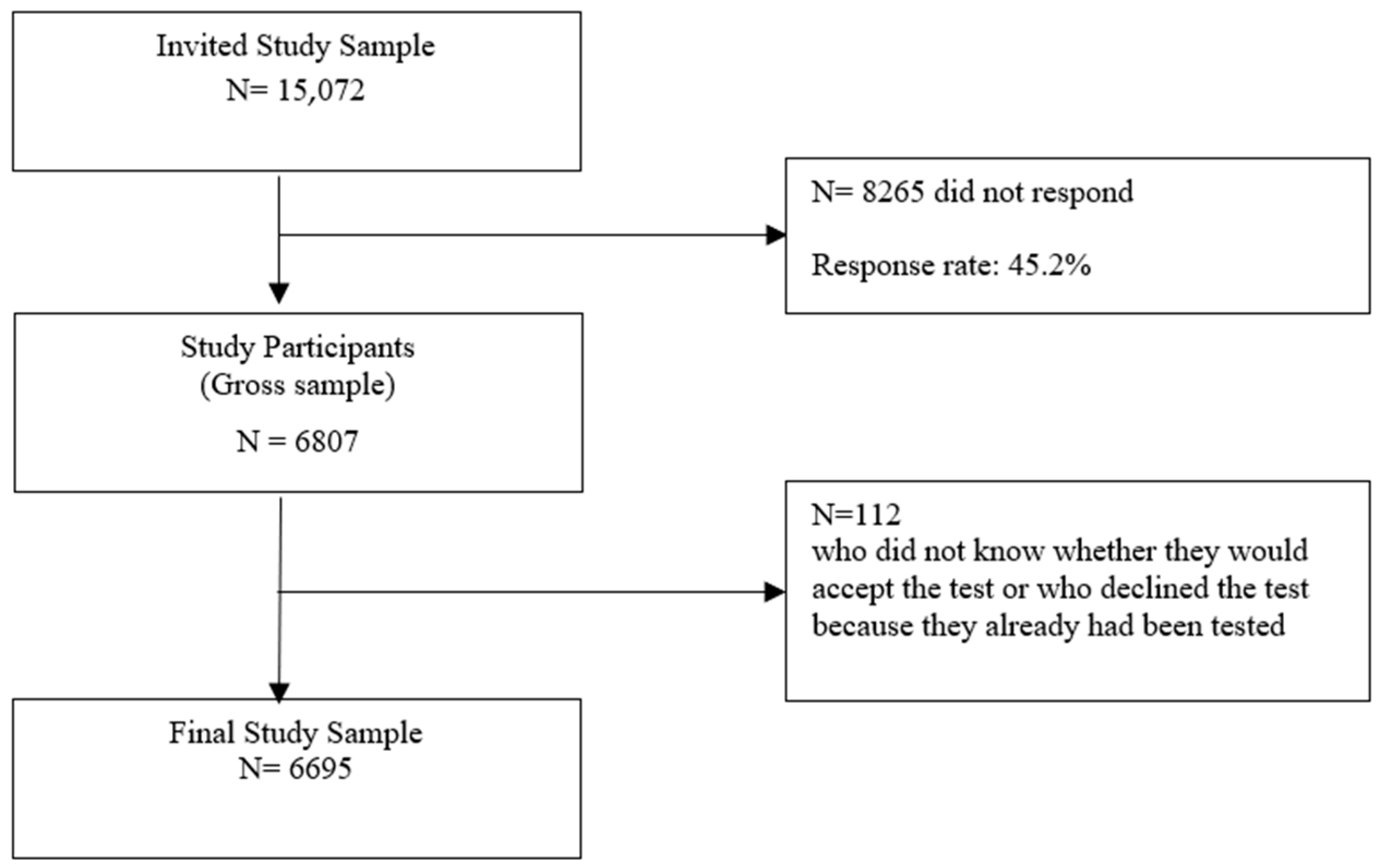
2.1. Sample and Procedure
2.2. Measurement
2.2.1. Outcome Variable
2.2.2. Exposure Variables
2.3. Statistical Analyses
3. Results
3.1. Sample Characteristics
3.2. Awareness of Personalized Medicine
3.3. Readiness for Treatment-Related Genetic Testing
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Council of the European Union. Council Conclusions on Personalized Medicine for Patients. 15054/15. Brussels. Available online: http://data.consilium.europa.eu/doc/document/ST-15054-2015-INIT/en/pdf (accessed on 9 November 2021).
- Collins, F.S.; Varmus, H. A new initiative on precision medicine. N. Engl. J. Med. 2015, 372, 793–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Belvis, A.G.; Pellegrino, R.; Castagna, C.; Morsella, A.; Pastorino, R.; Boccia, S. Success factors and barriers in combining personalized medicine and patient centered care in breast cancer. Results from a systematic review and proposal of conceptual framework. J. Pers. Med. 2021, 11, 654. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; McLeod, H.L.; Weinshilboum, R.M. Genomics and drug response. N. Engl. J. Med. 2011, 364, 1144–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schleidgen, S.; Klingler, C.; Bertram, T.; Rogowski, W.H.; Marckmann, G. What is personalized medicine: Sharpening a vague term based on a systematic literature review. BMC Med. Ethics 2013, 14, 55–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faulkner, E.; Holtorf, A.P.; Walton, S.; Liu, C.Y.; Lin, H.; Biltaj, E.; Brixner, D.; Barr, C.; Oberg, J.; Shandhu, G.; et al. Being precise about precision medicine: What should value frameworks incorporate to address precision medicine? A report of the Personalized Precision Medicine Special Interest Group. Value Health 2020, 23, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Aminkeng, F.; Bhavsar, A.P.; Shaw, K.; Carleton, B.C.; Hayden, M.R.; Ross, C.J.D. The emerging era of pharmacogenomics: Current successes, future potential, and challenges. Clin. Genet 2014, 86, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Sharp, C.N.; Linder, M.W.; Valdes, R. Polypharmacy: A healthcare conundrum with a pharmacogenetic solution. Crit. Rev. Clin. Lab. Sci. 2019, 57, 1–20. [Google Scholar] [CrossRef]
- Asiimwe, I.G.; Zhang, E.J.; Osanlou, R.; Jørgensen, A.L.; Pirmohamed, M. Warfarin dosing algorithms: A systematic review. Brit. J. Clin. Pharmacol. 2021, 87, 1717–1729. [Google Scholar] [CrossRef]
- Bousman, C.A.; Bengesser, S.A.; Aitchison, K.J.; Azmeraw, T.A.; Aschauer, H.; Baune, B.T.; Asl, B.B.; Bishop, J.R.; Burmeister, M.; Chaumette, B.; et al. Review and consensus on pharmacogenomic testing in psychiatry. Pharmacopsychiatry 2021, 54, 5–17. [Google Scholar] [CrossRef]
- Philips, K.A.; Deverka, P.A.; Sox, H.C.; Khoury, M.J.; Sandy, L.G.; Ginsburg, G.S.; Tunis, S.R.; Orlando, L.A.; Douglas, M.P. Making genomic medicine evidence-based and patient-centered: A structured review and landscape analysis of comparative effectiveness research. Genet Med. 2017, 19, 1081–1091. [Google Scholar] [CrossRef]
- Virelli, C.R.; Mohiuddin, A.G.; Kennedy, J.L. Barriers to clinical adoption of pharmacogenetic testing in psychiatry: A critical analysis. Transl. Psychiatry 2021, 11, 509–517. [Google Scholar] [CrossRef]
- Khoury, M.J.; Iademarco, M.F.; Riley, W.T. Precision public health for the era of precision medicine. Am. J. Prev. Med. 2016, 50, 398–401. [Google Scholar] [CrossRef] [Green Version]
- Green, R.F.; Dotson, W.D.; Bowen, S.; Kolor, K.; Khoury, M.J. Genomics in public health: Perspective from the Office of Public Health Genomics at the Centers for Disease Control and Prevention (CDC). Healthcare 2015, 3, 830–837. [Google Scholar] [CrossRef] [Green Version]
- Horgan, D.; Jansen, M.; Leyens, L.; Lal, J.A.; Sudbrak, R.; Hackenitz, E.; Bußhoff, U.; Ballensiefen, W.; Brand, A. An index of barriers for the implementation of personalized medicine and pharmacogenomics in Europe. Public Health Genom. 2014, 17, 287–298. [Google Scholar] [CrossRef]
- Ashley, E.A. The Precision Medicine Initiative: A new national effort. JAMA 2015, 313, 2119–2120. [Google Scholar] [CrossRef]
- Mills, R.; Voora, D.; Peyser, B.; Haga, S.B. Delivering pharmacogenetic testing in a primary care setting. Pharm. Pers. Med. 2013, 18, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Horne, R. The human dimension: Putting the person into personalized medicine. New Bioeth. 2017, 23, 38–48. [Google Scholar] [CrossRef]
- Barr, M.T.; Rose, D. The great ambivalence: Factors likely to affect service user and public acceptability of the pharmacogenomics of antidepressant medication. Sociol. Health Illn. 2008, 30, 944–958. [Google Scholar] [CrossRef]
- Holden, C.; Bignell, L.; Mukhopadhyay, S.; Jones, C. The public perception of the facilitators and barriers to implementing personalized medicine: A systematic review. Per. Med. 2019, 16, 409–420. [Google Scholar] [CrossRef]
- Gray, S.W.; Hicks-Courant, K.; Lathan, C.S.; Garraway, L.; Park, E.R.; Weeks, J.C. Attitudes of patients with cancer about personalized medicine and somatic genetic testing. J. Oncol. Pract. 2012, 8, 329–335. [Google Scholar] [CrossRef]
- Trinidad, S.B.; Coffin, T.B.; Fullerton, S.M.; Ralston, J.; Jarvik, G.P.; Larson, E.B. “Getting off the bus closer to your destination”. Patients’ view about pharmacogenetic testing. Perm. J. 2015, 19, 21–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Marco, M.; Cykert, S.; Coad, N.; Doost, K.; Schaal, J.; White, B.; Young, D.; Isler, M.R.; Corbie-Smith, G. Views on personalized medicine: Do the attitudes of African Americans and White prescription drug consumers differ? Public Health Genom. 2010, 13, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Issa, A.M.; Tufail, W.; Hutchinson, J.; Tenorio, J.; Baliga, M.P. Assessing patient readiness for the clinical adoption of personalized medicine. Public Health Genom. 2009, 12, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Almarsdottír, A.B.; Bjørnsdottir, I.; Traulsen, J.M. A lay prescription for tailor-made drugs—Focus group reflections on pharmacogenetics. Health Policy 2005, 71, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Bombard, Y.; Abelson, J.; Simeonov, D.; Gauvin, F.P. Citizens’ perspectives on personalized medicine: A qualitative public deliberation study. Eur. J. Hum. Genet 2013, 21, 1197–1201. [Google Scholar] [CrossRef] [Green Version]
- Haddy, C.A.; Ward, H.M.; Angley, M.T.; McKinnon, R.A. Consumers’ views of pharmacogenetics: A qualitative study. Res. Soc. Admin. Pharm. 2010, 6, 221–231. [Google Scholar] [CrossRef]
- Haga, S.B.; Tindall, G.; O’Daniel, J.M. Public perspectives about pharmacogenetic testing and managing ancillary findings. Gen. Test Mol. Biomark. 2012, 16, 193–197. [Google Scholar] [CrossRef]
- Chapdelaine, A.; Lamoureux-Lamarche, C.; Poder, T.G.; Vasiliadis, H.M. Socio-demographic factors and beliefs about medicines in the uptake of pharmacogenomic testing in older adults. Pharmacogenomics 2021, 22, 125–135. [Google Scholar] [CrossRef]
- Kobayashi, E.; Satoh, N. Public involvement in pharmacogenetic research: A national survey on public attitudes towards pharmacogenomics research and the willingness to donate DNA samples to a DNA bank in Japan. Cell Tissue Bank 2009, 10, 281–291. [Google Scholar] [CrossRef]
- Haga, S.B.; O’Daniel, J.M.; Tindall, G.M.; Lipkus, I.R.; Agans, R. Survey of U.S. public attitudes toward pharmacogenetic testing. Pharm. J. 2012, 12, 197–204. [Google Scholar]
- Nielsen, F.L.; Møldrup, C. The diffusion of innovation: Factors influencing the uptake of pharmacogenetics. Community Genet. 2007, 10, 231–241. [Google Scholar] [CrossRef]
- O’Daniel, J.O.; Lucas, J.; Deverka, P.; Ermentrout, D.; Silvey, G.; Lobach, D.F.; Haga, S.B. Factors influencing uptake of pharmacogenetic testing in a diverse patient population. Public Health Genom. 2010, 13, 48–54. [Google Scholar] [CrossRef]
- Rogausch, A.; Prause, D.; Schallenberg, A.; Brockmoeller, J.; Himmel, W. Patients’ and physicians’ perspectives on pharmacogenetic testing. Pharmacogenomics 2006, 7, 49–59. [Google Scholar] [CrossRef] [Green Version]
- Kichko, K.; Marschall, P.; Flessa, S. Personalized medicine in the U.S. and Germany: Awareness, acceptance, use and preconditions for the wide implementation into the medical standard. J. Per. Med. 2016, 6, 15. [Google Scholar] [CrossRef]
- Pereira, N.L.; So, D.; Bae, J.-H.; Chavez, I.; Jeong, M.H.; Kim, S.W.; Madan, M.; Graham, J.; O’Cochlain, F.; Pauley, N.; et al. International survey of patients undergoing percutaneous coronary intervention and their attitudes towards pharmacogenetic testing. Pharm. Genom. 2019, 29, 76–83. [Google Scholar] [CrossRef]
- Sundheds- og Ældreministeriet og Danske Regioner. Danskernes Tanker om og Holdninger til Personlig Medicin og Gentest. 2016. Available online: https://www.regioner.dk/media/4401/rapport-om-danskernes-holdning-til-personlig-medicin-og-gentest.pdf (accessed on 25 November 2021).
- Calabrò, G.E.; Sassano, M.; Tognetto, A.; Boccia, S. Citizen attitudes, knowledge, and education needs in the field of Omics sciences: A systematic literature review. Front. Genet. 2020, 11, 570649. [Google Scholar] [CrossRef]
- Garfeld, S.; Douglas, M.P.; MacDonald, K.V.; Marshall, D.A.; Philips, K.A. Consumer familiarity, perspectives and expected value of personalized medicine with a focus on applications in oncology. Per. Med. 2015, 12, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Chan, S.L.; Low, J.W.L.; Chia, K.S.; Wee, H.-L. Attitudes on Warfarin pharmacogenetic testing in Chinese patients and public. Int. J. Technol. Assess Health Care 2014, 30, 113–120. [Google Scholar] [CrossRef]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social Learning Theory and the Health Belief Model. Health Educ Quart 1988, 15, 175–183. [Google Scholar] [CrossRef]
- Rogers, R.W. Cognitive and physiological processes in attitude change: A revised Theory of Protection Motivation. In Social Psychophysiology; Cacioppo, J., Petty, R., Eds.; Guilford Press: New York, NY, USA, 1983; pp. 153–176. [Google Scholar]
- McCrae, R.R.; Costa, P.T., Jr. A five-factor theory of personality. In Handbook of Personality: Theory and Research, 2nd ed.; Pervin, L.A., John, O.P., Eds.; Guilford Press: New York, NY, USA, 1999; pp. 139–153. [Google Scholar]
- Zhang, S.C.; Bruce, C.; Hayden, M.; Rieder, M.J. Public perceptions of pharmacogenomics. Pediatrics 2014, 133, e1258–e1267. [Google Scholar] [CrossRef] [Green Version]
- Sundhedsstyrelsen. Forebyggelsespakke—Alkohol, 2nd ed.; Sundhedsstyrelsen: Copenhagen, Denmark, 2018. [Google Scholar]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef]
- WHO. Obesity: Preventing and Managing the Global Epidemic; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Wallston, K.A.; Wallston, B.S.; DeVellis, R. Development of the Multidimensional Health Locus of Control (MHLC) Scales. Health Educ. Monogr. 1978, 6, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Gosling, S.D.; Rentfrow, P.J.; Swann, W.B., Jr. A very brief measure of the Big-Five personality domains. J. Res. Personal. 2003, 37, 504–528. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, Version 26.0; IBM Corp: Armonk, NY, USA, 2019. [Google Scholar]
- Ek, S. Gender differences in health information behaviour: A Finnish population-based survey. Health Promot. Int. 2015, 30, 736–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rice, R.E. Influences, usage, and outcomes of internet health information searching: Multivariate results from the Pew surveys. Int. J. Med. Informat. 2006, 75, 8–28. [Google Scholar] [CrossRef]
- Renahy, E.; Parizot, I.; Chauvin, P. Determinants of the frequency of online health information seeking: Results of a web-based survey conducted in France in 2007. Inf. Health Soc. Care 2010, 35, 25–39. [Google Scholar] [CrossRef] [Green Version]
- Mählmann, L.; Röcke, C.; Brand, A.; Hafen, E.; Vayena, E. Attitudes towards personal genomics among older Swiss adults: An exploratory study. Appl. Transl. Genom. 2016, 8, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Patel, H.N.; Ursan, I.D.; Zueger, P.M.; Cavallari, L.; Pickard, S.A. Stakeholder views on pharmacogenetic testing. Pharmacotherapy 2014, 34, 151–165. [Google Scholar] [CrossRef]
- Eurobarometer, S. Responsible Research and Innovation, Science and Technology. Report to the European Commission, Directorate-General for Communication; European Commission: Brussels, Belgium, 2013. [Google Scholar]
- Nielsen, J.B.; Leppin, A.; Gyrd-Hansen, D.; Ejg Jarbøl, D.; Søndergaard, J.; Larsen, P.V. Barriers to lifestyle changes for prevention of cardiovascular disease—A survey among 40-60-year-old Danes. BMC Cardiovasc. Disord. 2017, 17, 245–252. [Google Scholar] [CrossRef] [Green Version]
- Smit, C.; De Hoogd, S.; Brüggemann, R.J.M.; Knibbe, C.A. Obesity and drug pharmacology: A review of the influence of obesity on pharmacokinetic and pharmacodynamic parameters. Expert Opin. Drug Metab. Toxicol. 2018, 14, 275–285. [Google Scholar] [CrossRef]
- Meng, L.; Holubar, M.K.; Deresinksi, M.C. Comprehensive guidance for antibiotic dosage in obese adults. Pharmacotherapy 2017, 3, 1415–1431. [Google Scholar] [CrossRef] [PubMed]
- Akinyemi, R.O.; Sarfo, F.S.; Akinyemi, J.; Singh, A.; Onoja, A.M.; Akpalu, A.; Ovbiagele, B. Knowledge, attitudes and practices of West Africans on genetic studies of stroke: Evidence from the SIREN Study. Int. J. Stroke 2019, 14, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Allen, C.G.; Roberts, M.; Guan, Y. Exploring predictors of genetic counseling and testing for hereditary breast and ovarian cancer: Findings from the 2015 US National Health Interview Study. J. Pers. Med. 2019, 9, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sweeny, K.; Ghane, A.; Legg, A.M.; Huynh, H.P.; Andrews, S.E. Predictors of genetic testing decisions: A systematic review and critique of the literature. J. Genet. Couns. 2014, 23, 263–288. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.E.; Crocker, J. Schematic bases of social information processing. In Social Cognition. The Ontario Symposium on Personality and Social Psychology; Higgins, E.T., Herman, C.A., Zanna, M.P., Eds.; Erlbaum: Hillsdale, NJ, USA, 1981; pp. 89–134. [Google Scholar]
- Kahneman, D.; Tversky, A. Subjective probability: A judgement of representativeness. Cogn. Psychol 1972, 3, 430–454. [Google Scholar] [CrossRef]
- Blouin-Bougie, J.; Amara, N.; Bouchard, K.; Simard, J.; Dorval, M. Disentangling the determinants of interest and willingness to pay for breast cancer susceptibility testing in the general population: A cross-sectional web-based survey among women of Québec (Canada). BMJ Open 2018, 8, e016662. [Google Scholar] [CrossRef]
- Bosompra, K.; Ashikaga, T.; Flynn, B.S.; Worden, J.K.; Solomon, L.J. Psychosocial factors associated with the public’s willingness to pay for genetic testing for cancer risk: A structural equation model. Health Educ. Res. 2001, 16, 157–172. [Google Scholar] [CrossRef] [Green Version]
- Bunn, J.Y.; Bosompra, K.; Ashikaga, T.; Flynn, B.S.; Worden, J.K. Factors influencing intention to obtain a genetic test for colon cancer risk: A population-based study. Prev. Med. 2002, 34, 567–577. [Google Scholar] [CrossRef]
- Botham, J.; Shilling, V.; Jones, J. Patient and public understanding of the concept of ’personalized medicine’ in relation to cancer treatment: A systematic review. Future Healthc. J. 2021, 8, 1–6. [Google Scholar]
- Waters, E.A.; Ball, L.; Gehlert, S. “I don’t believe it”. Acceptance and skepticism of genetic health information among African American and White smokers. Soc. Sc. Med. 2017, 184, 153e160. [Google Scholar]
- Haga, S.B.; Barry, W.T.; Mills, R.; Ginsburg, G.S.; Svetkey, L.; Sullivan, J.; Willard, H.F. Public knowledge of and attitudes toward genetics and genetic testing. Genet Test Mol Biomarkers 2013, 17, 327–335. [Google Scholar] [CrossRef]
- Nielsen, J.B.; Berg-Beckhoff, G.; Leppin, A. To do or not to do—A survey study on factors associated with participating in the Danish screening program for colorectal cancer. BMC Health Serv. Res. 2021, 21, 43–53. [Google Scholar] [CrossRef]
- Najafzadeh, M.; Johnston, K.M.; Peacock, S.J.; Connors, J.M.; Marra, M.A.; Lynd, L.D.; Marra, C.A. Genomic testing to determine drug response: Measuring preferences of the public and patients using discrete choice experiment (DCE). BMC Health Serv. Res. 2013, 13, 454–465. [Google Scholar]


{kind=link}
| Study Sample (n = 6695) (%) | Gross Sample 1 (n = 6807) (%) | DK Population (50–80 Years) (n = 2,054,477) (%) | ||
|---|---|---|---|---|
| Sex | Female | 52.1 | 52.5 | 50.9 |
| Age | 50–60 | 38.8 | 38.8 | 42.3 |
| 61–70 | 36.6 | 36.6 | 32.1 | |
| 71–80 | 24.5 | 24.6 | 25.6 | |
| Education | Less than 11 years school education | 18.8 | 18.9 | 27.3 |
| 11–13 years school education | 44.1 | 44.0 | 43.8 | |
| >13 years school education | 37.1 | 37.1 | 28.9 | |
| Personal income | <27.000 € | 34.9 | 42.3 | |
| 27.000–40.000 € | 32.7 | 30.6 | ||
| >40.000 € | 32.4 | 27.1 | ||
| Work status | Working | 51.7 | 48.3 | |
| Birthplace | Denmark | 94.9 | 92.0 | |
| Residence in DK | Capital (Copenhagen) | 28.7 | 28.3 | |
| Zealand | 16.1 | 16.3 | ||
| Jutland & Funen | 55.2 | 55.3 |
| Characteristics | Willing to Be Tested | Not Willing to Be Tested | Total | ||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | p-Value | |
| Overall (row/%) | 5331 | 79.6 | 1364 | 20.4 | 6695 | 100.00 | |
| Sex | |||||||
| Male | 2675 | 83.4 | 531 | 16.6 | 3206 | 47.9 | |
| Female | 2656 | 76.1 | 833 | 23.9 | 3489 | 52.1 | <0.001 |
| Age | |||||||
| 50–60 | 2139 | 82.3 | 461 | 17.7 | 2600 | 38.8 | |
| 61–70 | 1946 | 79.4 | 506 | 20.6 | 2452 | 36.6 | |
| 71–80 | 1246 | 75.8 | 397 | 24.2 | 1643 | 24.5 | <0.001 |
| Education | |||||||
| <11 years | 1011 | 80.1 | 251 | 19.9 | 1262 | 18.8 | |
| 11–13 years | 2406 | 81.5 | 546 | 18.5 | 2952 | 44.1 | |
| >13 years | 1914 | 77.1 | 567 | 22.9 | 2481 | 37.1 | <0.001 |
| Income in € p.a.1 | |||||||
| <33.333 | 1993 | 77.5 | 577 | 22.5 | 2570 | 38.4 | |
| 33.333–46.666 | 1606 | 80.7 | 384 | 19.3 | 1990 | 29.7 | |
| >46.666 | 1732 | 81.1 | 403 | 18.9 | 2135 | 31.9 | =0.004 |
| Smoking status | |||||||
| Smoker | 770 | 78.6 | 210 | 21.4 | 980 | 14.6 | |
| Quit smoking | 1467 | 81.3 | 337 | 18.7 | 1804 | 26.9 | |
| Never smoker | 3094 | 79.1 | 817 | 20.9 | 3911 | 58.4 | =0.105 |
| Alcohol consumption | |||||||
| 0–7 (women)/0–14 (men) units | 4297 | 79.5 | 1108 | 20.5 | 5405 | 80.7 | |
| >7 (women)/>14 (men) units | 1034 | 80.2 | 256 | 19.8 | 1290 | 19.3 | =0.315 |
| Physical activity | |||||||
| Never to 4 times a week | 4580 | 80.0 | 1147 | 20.0 | 5727 | 85.6 | |
| 5 times a week or more | 749 | 77.7 | 215 | 22.3 | 964 | 14.4 | =0.058 |
| Body mass index | |||||||
| <25.0 | 2120 | 77.3 | 623 | 22.7 | 2743 | 41.8 | |
| 25.0–<30.0 | 2053 | 80.5 | 498 | 19.5 | 2551 | 38.8 | |
| 30.0+ | 1069 | 83.8 | 207 | 16.2 | 1276 | 19.4 | <0.001 |
| Daily medication intake | |||||||
| No | 2136 | 79.0 | 568 | 21.0 | 2704 | 40.4 | |
| Yes | 3192 | 80.1 | 792 | 19.9 | 3984 | 59.6 | =0.137 |
| Satisfaction with health | |||||||
| Low | 536 | 84.4 | 99 | 15.6 | 635 | 9.5 | |
| Medium | 1063 | 81.5 | 242 | 18.5 | 1305 | 19.5 | |
| High | 3730 | 78.5 | 1023 | 21.5 | 4753 | 71.0 | <0.001 |
| Genetic vulnerability | |||||||
| No | 2312 | 76.2 | 723 | 23.8 | 3035 | 45.3 | |
| Don’t know | 2065 | 81.0 | 483 | 19.0 | 2548 | 38.1 | <0.001 |
| Yes | 954 | 85.8 | 158 | 14.2 | 1112 | 16.6 | |
| Internal health locus of control | |||||||
| Low | 2837 | 78.2 | 790 | 21.8 | 3627 | 54.6 | |
| High | 2457 | 81.3 | 564 | 18.7 | 3021 | 45.4 | =0.002 |
| Health-related risk taking | |||||||
| None | 1191 | 78.0 | 335 | 22.0 | 1526 | 22.8 | |
| Low | 2775 | 79.6 | 710 | 20.4 | 3485 | 52.1 | |
| Medium-High | 1360 | 81.2 | 315 | 18.8 | 1675 | 25.1 | =0.087 |
| Prior awareness about personalized medicine | |||||||
| No | 2137 | 85.2 | 371 | 14.8 | 2508 | 37.5 | |
| Yes | 3183 | 76.3 | 990 | 23.7 | 4173 | 62.5 | <0.001 |
| Characteristics | Crude OR | 95% CI | Adjusted OR | 95% CI |
|---|---|---|---|---|
| Sex | ||||
| Female | 0.63 | 0.56–0.72 | 0.67 | 0.59–0.77 |
| Age group | ||||
| 50–60 | 1 | Ref | 1 | Ref |
| 61–70 | 0.83 | 0.72–0.95 | 0.88 | 0.76–1.02 |
| 71–80 | 0.68 | 0.58–0.79 | 0.72 | 0.61–0.86 |
| Education | ||||
| <11 years | 1 | Ref | 1 | Ref |
| 11–13 years | 1.09 | 0.93–1.29 | 1.04 | 0.87–1.24 |
| >13 years | 0.84 | 0.71–0.99 | 0.84 | 0.70–1.02 |
| Income per year (€) 1 | ||||
| <33,000 | 1 | Ref | 1 | Ref |
| 33.000–47.000 | 1.21 | 1.05–1.40 | 1.23 | 1.05–1.44 |
| >47.000 | 1.24 | 1.08–1.44 | 1.29 | 1.09–1.52 |
| Smoking status | ||||
| Smoker | 1 | Ref | 1 | Ref |
| Quit smoking | 1.19 | 0.98–1.44 | 1.25 | 1.02–1.54 |
| Never smoked | 1.03 | 0.87–1.23 | 1.19 | 0.99–1.43 |
| Alcohol consumption over recommended levels | ||||
| >7 (women)/>14 units (men) | 1.04 | 0.90–1.21 | 1.09 | 0.93–1.28 |
| Sufficient physical activity | ||||
| 5 days a week or more | 0.87 | 0.74–1.03 | 0.95 | 0.80–1.13 |
| BMI | ||||
| <25.0 | 1 | Ref | 1 | Ref |
| 25.0–29.9 | 1.21 | 1.06–1.38 | 1.05 | 0.92–1.21 |
| =>30.0 | 1.52 | 1.28–1.81 | 1.24 | 1.03–1.49 |
| Daily medication intake | 1.07 | 0.95–1.21 | 1.03 | 0.89–1.18 |
| Satisfaction with health status | 1 | Ref | 1 | Ref |
| Low | 0.81 | 0.63–1.05 | 0.73 | 0.56–0.96 |
| Medium | 0.81 | 0.63–1.05 | 0.73 | 0.56–0.96 |
| High | 0.67 | 0.54–0.84 | 0.64 | 0.49–0.82 |
| Perceived genetic vulnerability | ||||
| No | 1 | Ref | 1 | Ref |
| Don’t know | 1.34 | 1.17–1.52 | 1.38 | 1.20–1.58 |
| Yes | 1.89 | 1.57–2.28 | 1.91 | 1.57–2.34 |
| Internal health locus of control | 1.21 | 1.08–1.37 | 1.21 | 1.06–1.38 |
| Health-related risk taking | ||||
| None | 1 | Ref | 1 | Ref |
| Low | 1.10 | 0.95–1.27 | 1.00 | 0.85–1.17 |
| Medium-High | 1.21 | 1.02–1.44 | 1.02 | 0.85–1.23 |
| Prior awareness about | ||||
| personalized medicine | 0.56 | 0.49–0.64 | 0.58 | 0.50–0.66 |
| Extraversion (1–7) | 1.05 | 1.01–1.09 | 1.08 | 1.03–1.14 |
| Openness (1–7) | 0.99 | 0.94–1.04 | 0.98 | 0.93–1.04 |
| Emotional Stability (1–7) | 1.06 | 1.01–1.11 | 1.06 | 1.01–1.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leppin, A.; Nielsen, J.B. Readiness to Accept Genetic Testing for Personalized Medicine: Survey Findings on the Role of Socio-Demographic Characteristics, Health Vulnerabilities, Perceived Genetic Risk and Personality Factors. J. Pers. Med. 2022, 12, 1836. https://doi.org/10.3390/jpm12111836
Leppin A, Nielsen JB. Readiness to Accept Genetic Testing for Personalized Medicine: Survey Findings on the Role of Socio-Demographic Characteristics, Health Vulnerabilities, Perceived Genetic Risk and Personality Factors. Journal of Personalized Medicine. 2022; 12(11):1836. https://doi.org/10.3390/jpm12111836
Chicago/Turabian StyleLeppin, Anja, and Jesper Bo Nielsen. 2022. "Readiness to Accept Genetic Testing for Personalized Medicine: Survey Findings on the Role of Socio-Demographic Characteristics, Health Vulnerabilities, Perceived Genetic Risk and Personality Factors" Journal of Personalized Medicine 12, no. 11: 1836. https://doi.org/10.3390/jpm12111836