
In Vivo Anatomical Research by 3D CT Reconstruction Determines Minimum Acromiohumeral, Coracohumeral, and Glenohumeral Distances in the Human Shoulder: Evaluation of Age and Sex Association in a Sample of the Chinese Population
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Compliance with Ethical Standards
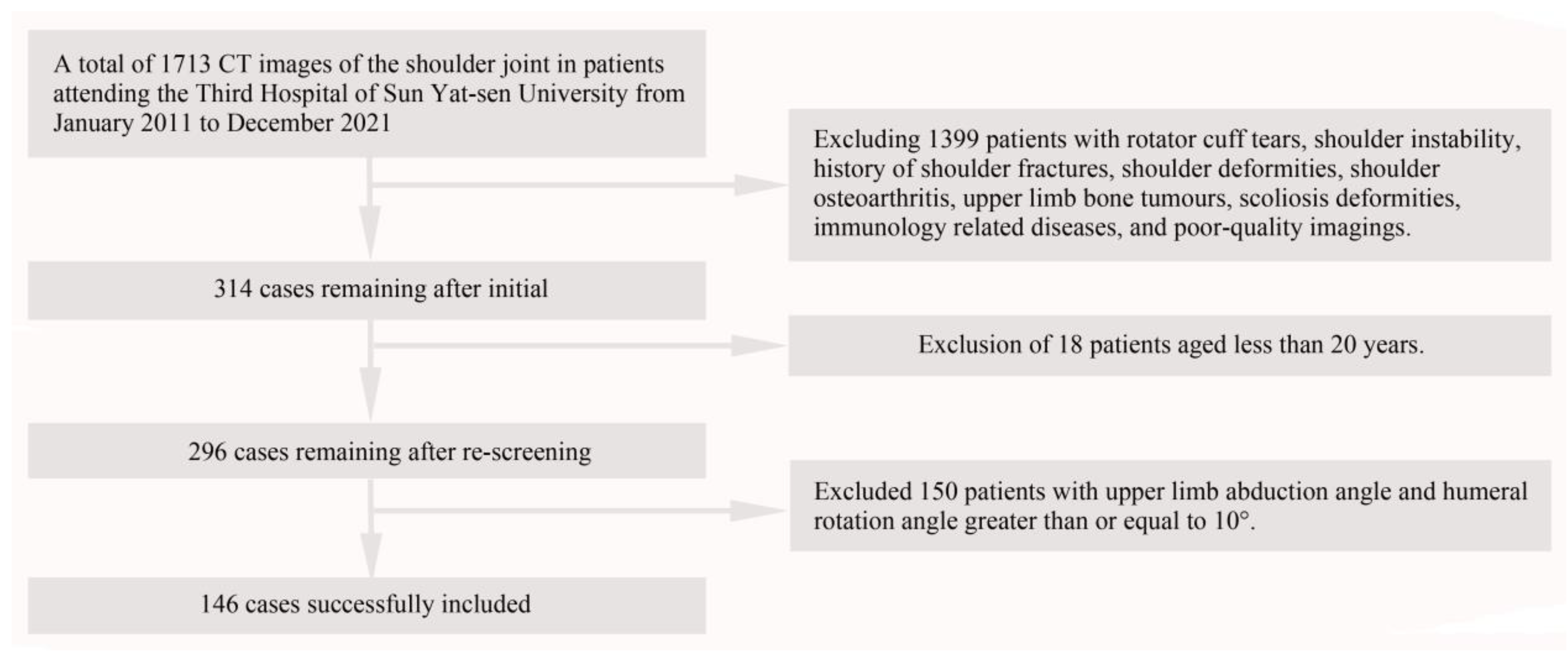
2.2. Patient Data Study
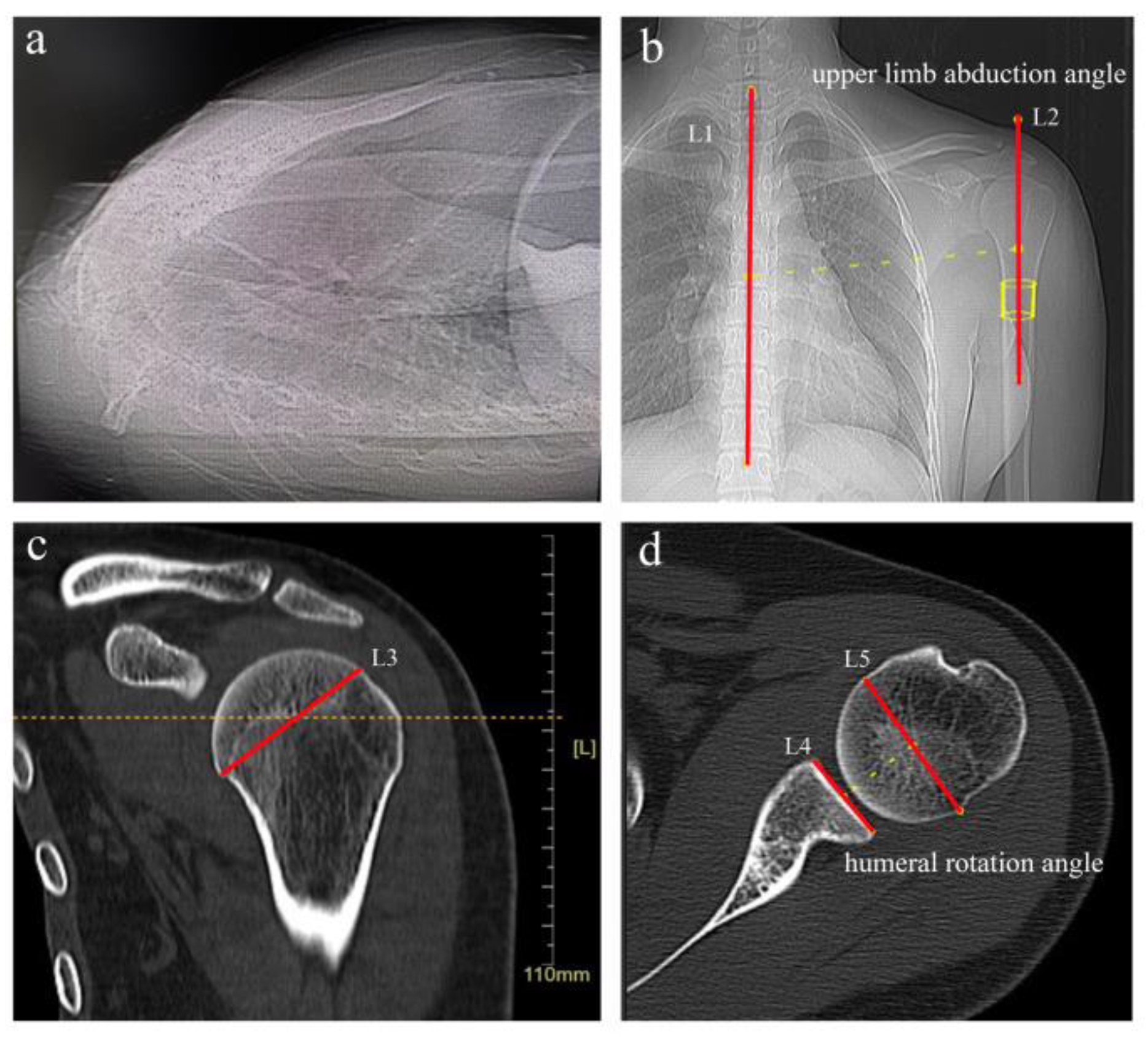
2.3. Evaluation Metrics
2.4. Data Process and Statistical Analysis
3. Results
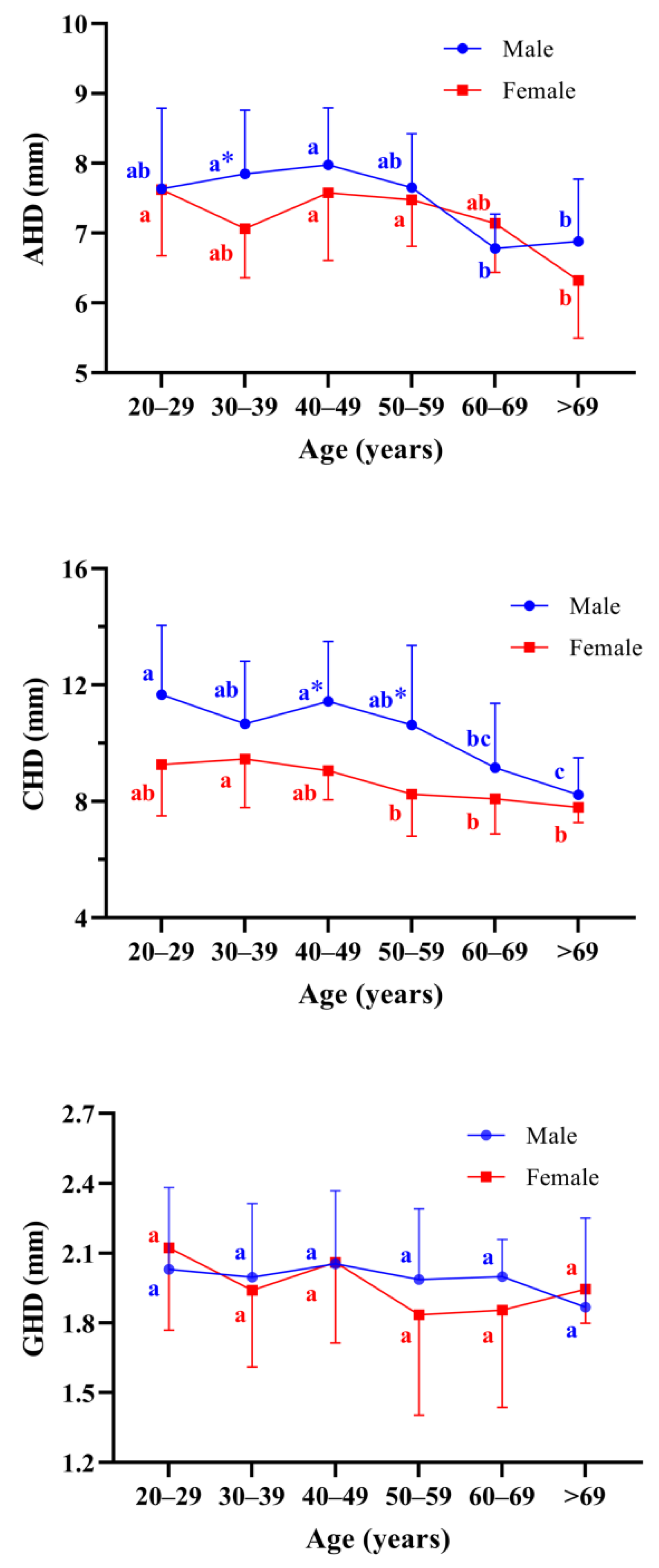
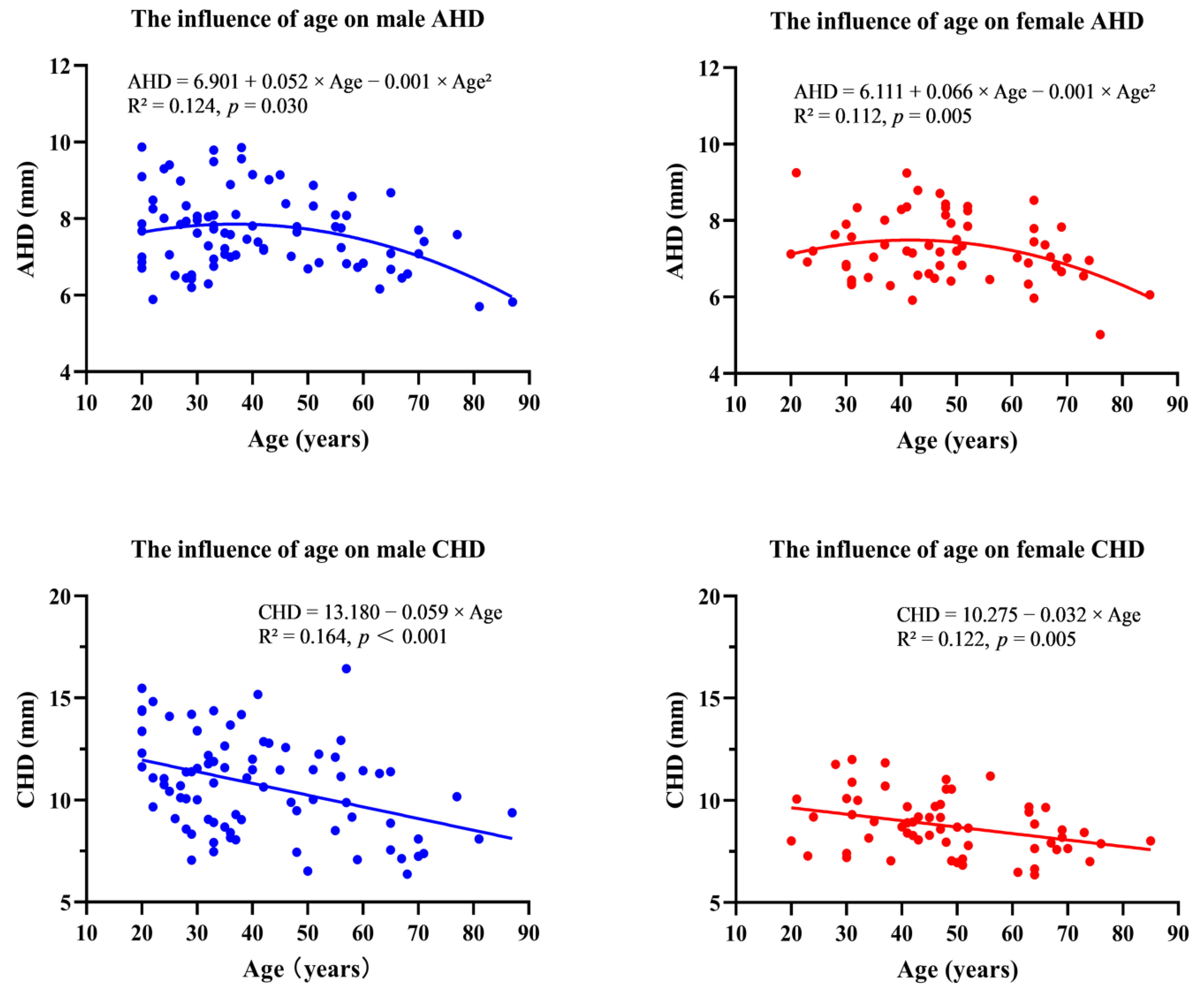
3.1. The Minimum Acromiohumeral Distance
3.2. The Minimum Coracohumeral Distance
3.3. The Minimum Glenohumeral Distances
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Beirer, M.; Imhoff, A.B.; Braun, S. Impingement-Syndrome der Schulter. Der Orthopäde 2017, 46, 373–386. [Google Scholar] [CrossRef] [PubMed]
- Ostor, A.J.; Richards, C.A.; Prevost, A.T.; Speed, C.A.; Hazleman, B.L. Diagnosis and relation to general health of shoulder disorders presenting to primary care. Rheumatology (Oxford) 2005, 44, 800–805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neer, C.N. Anterior acromioplasty for the chronic impingement syndrome in the shoulder: A preliminary report. J. Bone Jt. Surg. Am. 1972, 54, 41–50. [Google Scholar] [CrossRef]
- Gerber, C.; Terrier, F.; Ganz, R. The role of the coracoid process in the chronic impingement syndrome. J. Bone Jt. Surg. Br. 1985, 67, 703–708. [Google Scholar] [CrossRef] [Green Version]
- Medina, G.; Bartolozzi, A.R.; Spencer, J.A.; Morgan, C. The Thrower’s Shoulder. JBJS Rev. 2022, 10, e21.00194. [Google Scholar] [CrossRef]
- Mohammed, H.; Skalski, M.R.; Patel, D.B.; Tomasian, A.; Schein, A.J.; White, E.A.; Hatch, G.R.; Matcuk, G.J. Coracoid Process: The Lighthouse of the Shoulder. Radiographics 2016, 36, 2084–2101. [Google Scholar] [CrossRef] [Green Version]
- van Rijn, R.M.; Huisstede, B.M.; Koes, B.W.; Burdorf, A. Associations between work-related factors and specific disorders of the shoulder—A systematic review of the literature. Scand. J. Work. Environ. Health 2010, 36, 189–201. [Google Scholar] [CrossRef] [Green Version]
- Saupe, N.; Pfirrmann, C.W.A.; Schmid, M.R.; Jost, B.; Werner, C.M.L.; Zanetti, M. Association between rotator cuff abnormalities and reduced acromiohumeral distance. Am. J. Roentgenol. 2006, 187, 376–382. [Google Scholar] [CrossRef]
- Giaroli, E.L.; Major, N.M.; Lemley, D.E.; Lee, J. Coracohumeral interval imaging in subcoracoid impingement syndrome on MRI. Am. J. Roentgenol. 2006, 186, 242–246. [Google Scholar] [CrossRef]
- Charbonnier, C.; Chague, S.; Kolo, F.C.; Ladermann, A. Shoulder motion during tennis serve: Dynamic and radiological evaluation based on motion capture and magnetic resonance imaging. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 1289–1297. [Google Scholar] [CrossRef]
- Ruckstuhl, H.; de Bruin, E.D.; Stussi, E.; Vanwanseele, B. Post-traumatic glenohumeral cartilage lesions: A systematic review. BMC Musculoskelet. Disord. 2008, 9, 107. [Google Scholar] [CrossRef] [PubMed]
- Kubicka, A.M.; Stefaniak, J.; Lubiatowski, P.; Dlugosz, J.; Dzianach, M.; Redman, M.; Piontek, J.; Romanowski, L. Reliability of measurements performed on two dimensional and three dimensional computed tomography in glenoid assessment for instability. Int. Orthop. 2016, 40, 2581–2588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefaniak, J.; Kubicka, A.M.; Wawrzyniak, A.; Romanowski, L.; Lubiatowski, P. Reliability of humeral head measurements performed using two- and three-dimensional computed tomography in patients with shoulder instability. Int. Orthop. 2020, 44, 2049–2056. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, Y.; Matsumura, N.; Yamada, Y.; Yamada, M.; Yokoyama, Y.; Matsumoto, M.; Nakamura, M.; Nagura, T.; Jinzaki, M. Evaluation of three-dimensional acromiohumeral distance in the standing position and comparison with its conventional measuring methods. J. Orthop. Surg. Res. 2020, 15, 436. [Google Scholar] [CrossRef]
- Stefaniak, J.; Lubiatowski, P.; Kubicka, A.M.; Wawrzyniak, A.; Wałecka, J.; Romanowski, L. Clinical and radiological examination of bony-mediated shoulder instability. EFORT Open Rev. 2020, 5, 815–827. [Google Scholar] [CrossRef]
- Weber, A.E.; Bolia, I.K.; Horn, A.; Villacis, D.; Omid, R.; Tibone, J.E.; White, E.; Hatch, G.F. Glenoid Bone Loss in Shoulder Instability: Superiority of Three-Dimensional Computed Tomography over Two-Dimensional Magnetic Resonance Imaging Using Established Methodology. Clin. Orthop. Surg. 2021, 13, 223–228. [Google Scholar] [CrossRef]
- Werner, C.M.; Conrad, S.J.; Meyer, D.C.; Keller, A.; Hodler, J.; Gerber, C. Intermethod agreement and interobserver correlation of radiologic acromiohumeral distance measurements. J. Shoulder Elb. Surg. 2008, 17, 237–240. [Google Scholar] [CrossRef]
- Cohn, M.R.; Defroda, S.F.; Huddleston, H.P.; Williams, B.T.; Singh, H.; Vadhera, A.; Garrigues, G.E.; Nicholson, G.P.; Yanke, A.B.; Verma, N.N. Does native glenoid anatomy predispose to shoulder instability? An MRI analysis. J. Shoulder Elb. Surg. 2022, 31, S110–S116. [Google Scholar] [CrossRef]
- Balke, M.; Banerjee, M.; Greshake, O.; Hoeher, J.; Bouillon, B.; Liem, D. The Coracohumeral Distance in Shoulders With Traumatic and Degenerative Subscapularis Tendon Tears. Am. J. Sport. Med. 2016, 44, 198–201. [Google Scholar] [CrossRef]
- Richards, D.P.; Burkhart, S.S.; Campbell, S.E. Relation between narrowed coracohumeral distance and subscapularis tears. Arthroscopy 2005, 21, 1223–1228. [Google Scholar] [CrossRef]
- Needell, S.D.; Zlatkin, M.B.; Sher, J.S.; Murphy, B.J.; Uribe, J.W. MR imaging of the rotator cuff: Peritendinous and bone abnormalities in an asymptomatic population. Am. J. Roentgenol. 1996, 166, 863–867. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, K.; Yoshida, A.; Inokuchi, W.; Naniwa, T. Acromial spur: Relationship to aging and morphologic changes in the rotator cuff. J. Shoulder Elb. Surg. 2005, 14, 591–598. [Google Scholar] [CrossRef]
- Zhang, Q.; Shi, L.L.; Ravella, K.C.; Koh, J.L.; Wang, S.; Liu, C.; Li, G.; Wang, J. Distinct Proximal Humeral Geometry in Chinese Population and Clinical Relevance. J. Bone Jt. Surg. 2016, 98, 2071–2081. [Google Scholar] [CrossRef] [PubMed]
- Sahu, D.; Joshi, M.; Rathod, V.; Nathani, P.; Valavi, A.S.; Jagiasi, J.D. Geometric analysis of the humeral head and glenoid in the Indian population and its clinical significance. JSES Int. 2020, 4, 992–1001. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, N.; Oki, S.; Ogawa, K.; Iwamoto, T.; Ochi, K.; Sato, K.; Nagura, T. Three-dimensional anthropometric analysis of the glenohumeral joint in a normal Japanese population. J. Shoulder Elb. Surg. 2016, 25, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Mäkelä, M.; Heliövaara, M.; Sainio, P.; Knekt, P.; Impivaara, O.; Aromaa, A. Shoulder joint impairment among Finns aged 30 years or over: Prevalence, risk factors and co-morbidity. Rheumatology (Oxford) 1999, 38, 656–662. [Google Scholar] [CrossRef] [Green Version]
- Jim, Y.F.; Chang, C.Y.; Wu, J.J.; Chang, T. Shoulder impingement syndrome: Impingement view and arthrography study based on 100 cases. Skelet. Radiol. 1992, 21, 449–451. [Google Scholar] [CrossRef]
- Flatow, E.L.; Soslowsky, L.J.; Ticker, J.B.; Pawluk, R.J.; Hepler, M.; Ark, J.; Bigliani, L.U. Excursion of the Rotator Cuff Under the Acromion. Am. J. Sport. Med. 1994, 22, 779–788. [Google Scholar] [CrossRef]
- Hufeland, M.; Brusis, C.; Kubo, H.; Grassmann, J.; Latz, D.; Patzer, T. The acromiohumeral distance in the MRI should not be used as a decision criterion to assess subacromial space width in shoulders with an intact rotator cuff. Knee Surg. Sport. Traumatol. Arthrosc. 2021, 29, 2085–2089. [Google Scholar] [CrossRef]
- Friedman, R.J.; Bonutti, P.M.; Genez, B. Cine magnetic resonance imaging of the subcoracoid region. Orthopedics 1998, 21, 545–548. [Google Scholar]
- Petersson, C.J.; Redlund-Johnell, I. Joint Space in Normal Gleno-Humeral Radiographs. Acta Orthop. Scand. 1983, 54, 274–276. [Google Scholar] [CrossRef] [PubMed]
- Aktas, E.; Sahin, B.; Arikan, M.; Ciledag, N.; Buyukcam, F.; Tokgoz, O.; Caglar, E.; Aribas, B.K. MRI analysis of coracohumeral interval width and its relation to rotator cuff tear. Eur. J. Orthop. Surg. Traumatol. 2015, 25, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Ekizoglu, O.; Inci, E.; Ors, S.; Kacmaz, I.E.; Basa, C.D.; Can, I.O.; Kranioti, E.F. Applicability of T1-weighted MRI in the assessment of forensic age based on the epiphyseal closure of the humeral head. Int. J. Leg. Med. 2019, 133, 241–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harput, G.; Guney-Deniz, H.; Düzgün, İ.; Toprak, U.; Michener, L.A.; Powers, C.M. Active Scapular Retraction and Acromiohumeral Distance at Various Degrees of Shoulder Abduction. J. Athl. Train. 2018, 53, 584–589. [Google Scholar] [CrossRef] [Green Version]
- De Wilde, L.F.; Berghs, B.M.; Vandevyver, F.; Schepens, A.; Verdonk, R.C. Glenohumeral relationship in the transverse plane of the body. J. Shoulder Elb. Surg. 2003, 12, 260–267. [Google Scholar] [CrossRef]
- Jacxsens, M.M.; Van Tongel, A.M.P.; Henninger, H.B.P.; De Coninck, B.M.; Mueller, A.M.M.; De Wilde, L.M.P. A three-dimensional comparative study on the scapulohumeral relationship in normal and osteoarthritic shoulders. J. Shoulder Elb. Surg. 2016, 25, 1607–1615. [Google Scholar] [CrossRef]
- Budoff, J.E.; Nirschl, R.P.; Guidi, E.J. Debridement of partial-thickness tears of the rotator cuff without acromioplasty. Long-term follow-up and review of the literature. J. Bone Jt. Surg. 1998, 80, 733–748. [Google Scholar] [CrossRef] [Green Version]
- Fremerey, R.; Bastian, L.; Siebert, W.E. The coracoacromial ligament: Anatomical and biomechanical properties with respect to age and rotator cuff disease. Knee Surg. Sport. Traumatol. Arthrosc. 2000, 8, 309–313. [Google Scholar] [CrossRef]
- Rothenberg, A.; Gasbarro, G.; Chlebeck, J.; Lin, A. The Coracoacromial Ligament: Anatomy, Function, and Clinical Significance. Orthop. J. Sport. Med. 2017, 5, 2325967117703398. [Google Scholar] [CrossRef] [Green Version]
- Vahakari, M.; Leppilahti, J.; Hyvonen, P.; Ristiniemi, J.; Paivansalo, M.; Jalovaara, P. Acromial shape in asymptomatic subjects: A study of 305 shoulders in different age groups. Acta Radiol. 2010, 51, 202–206. [Google Scholar] [CrossRef]
- Gianakos, A.L.; George, N.; Pinninti, A.; Kwan, S.; Laporte, D.; Mulcahey, M.K. Sex- and Gender-specific Analysis in Orthopaedic Studies. Clin. Orthop. Relat. Res. 2020, 478, 1482–1488. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Zhang, Q.; Zhu, Y.; Jiang, C. Is radiofrequency treatment effective for shoulder impingement syndrome? A prospective randomized controlled study. J. Shoulder Elb. Surg. 2013, 22, 1488–1494. [Google Scholar] [CrossRef] [PubMed]
- Lavoie-Gagne, O.; Farah, G.; Lu, Y.; Mehta, N.; Parvaresh, K.C.; Forsythe, B. Physical Therapy Combined With Subacromial Cortisone Injection Is a First-Line Treatment Whereas Acromioplasty With Physical Therapy Is Best if Nonoperative Interventions Fail for the Management of Subacromial Impingement: A Systematic Review and Network Meta-Analysis. Arthroscopy 2022, 38, 2511–2524. [Google Scholar] [CrossRef]
- Kragh, J.J.; Doukas, W.C.; Basamania, C.J. Primary coracoid impingement syndrome. Am. J. Orthop. 2004, 33, 229–232. [Google Scholar]
- Burkhart, S.S.; De Beer, J.F. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy 2000, 16, 677–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habermeyer, P.; Ebert, T. Current status and perspectives of shoulder replacement. Unfallchirurg 1999, 102, 668–683. [Google Scholar] [CrossRef]
- Gregory, T.; Hansen, U.; Emery, R.J.; Augereau, B.; Amis, A.A. Developments in shoulder arthroplasty. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2007, 221, 87–96. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Age (Years) | Total | |||||
|---|---|---|---|---|---|---|---|
| 20–29 | 30–39 | 40–49 | 50–59 | 60–69 | >69 | ||
| Male | 24 | 24 | 11 | 12 | 7 | 6 | 84 |
| Female | 5 | 13 | 19 | 8 | 12 | 5 | 62 |
| Total | 29 | 37 | 30 | 20 | 19 | 11 | 146 |
| Characteristic | All | Male | Female | p Value (Sex Difference) |
|---|---|---|---|---|
| Age (years) | 43.97 ± 16.25 (n = 146) | 41.08 ± 16.42 (n = 84) | 47.89 ± 15.28 (n = 62) | 0.012 |
| Outreach angles (°) | 4.75 ± 3.32 (n = 146) | 4.49 ± 3.30 (n = 84) | 5.09 ± 3.34 (n = 62) | 0.288 |
| Internal rotation angles (°) | 5.96 ± 2.87 (n = 71) | 6.15 ± 2.89 (n = 48) | 5.55 ± 2.83 (n = 23) | 0.409 |
| External rotation angles (°) | 6.03 ± 2.89 (n = 75) | 5.73 ± 2.91 (n = 36) | 6.30 ± 2.88 (n = 39) | 0.392 |
| Left shoulder (cases) | 73 | 40 | 33 | |
| Right shoulder (cases) | 73 | 44 | 29 | |
| AHD (mm) | 7.47 ± 0.94 (n = 146) | 7.62 ± 0.98 (n = 84) | 7.27 ± 0.86 (n = 62) | 0.046 |
| CHD (mm) | 9.90 ± 2.25 (n = 146) | 10.75 ± 2.40 (n = 84) | 8.76 ± 1.38 (n = 62) | <0.001 |
| GHD (mm) | 1.98 ± 0.33 (n = 146) | 2.00 ± 0.31 (n = 84) | 1.96 ± 0.36 (n = 62) | 0.598 |
| Variable | Age (Years) | p Value | |||||
|---|---|---|---|---|---|---|---|
| 20–29 | 30–39 | 40–49 | 50–59 | 60–69 | >69 | ||
| AHD (mm) | |||||||
| Male | 7.63 ± 1.15 (5.89 – 9.87) | 7.85 ± 0.91 (6.30 – 9.79) | 7.98 ± 0.81 (7.02 – 9.15) | 7.65 ± 0.77 (6.69 – 8.87) | 6.78 ± 0.49 (6.16 – 7.68) | 6.88 ± 0.89 (5.70 – 7.70) | 0.039 |
| Female | 7.62 ± 0.95 (6.92 – 9.25) | 7.06 ± 0.71 (6.30 – 8.34) | 7.58 ± 0.96 (5.92 – 9.24) | 7.48 ± 0.67 (6.46 – 8.37) | 7.14 ± 0.70 (5.97 – 8.53) | 6.32 ± 0.82 (5.02 – 7.02) | 0.048 |
| p Value | 0.889 | 0.011 | 0.250 | 0.734 | 0.261 | 0.247 | |
| CHD (mm) | |||||||
| Male | 11.66 ± 2.38 (7.06 – 15.47) | 10.67 ± 2.14 (7.47 – 14.37) | 11.44 ± 2.06 (7.44 – 15.17) | 10.63 ± 2.73 (6.52 – 16.43) | 9.15 ± 2.21 (6.37 – 11.44) | 8.23 ± 1.27 (7.10 – 10.17) | 0.011 |
| Female | 9.26 ± 1.76 (7.28 – 11.77) | 9.46 ± 1.67 (7.05 – 12.01) | 9.06 ± 1.00 (7.05 – 11.03) | 8.24 ± 1.44 (6.83 – 11.20) | 8.08 ± 1.20 (6.36 – 9.68) | 7.80 ± 0.52 (7.01 – 8.43) | 0.039 |
| p Value | 0.051 | 0.124 | 0.001 | 0.047 | 0.432 | 0.792 | |
| GHD (mm) | |||||||
| Male | 2.03 ± 0.35 (1.47 – 2.75) | 2.00 ± 0.32 (1.47 – 2.75) | 2.05 ± 0.31 (1.66 – 2.65) | 1.99 ± 0.30 (1.52 – 2.67) | 2.00 ± 0.16 (1.74 – 2.17) | 1.87 ± 0.38 (1.41 – 2.40) | 0.903 |
| Female | 2.12 ± 0.35 (1.65 – 2.57) | 1.94 ± 0.33 (1.41 – 2.43) | 2.06 ± 0.35 (1.44 – 2.63) | 1.84 ± 0.43 (1.28 – 2.56) | 1.86 ± 0.42 (1.24 – 2.42) | 1.94 ± 0.15 (1.77 – 2.09) | 0.489 |
| p Value | 0.518 | 0.649 | 0.966 | 0.384 | 0.773 | 0.792 | |
| Parameter/Population | Previous Studies | Current Study | p Value † | |||||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Sample Size | Imaging Method | Mean ± SD | Sample Size | Imaging Method | |||
| AHD (mm) | ||||||||
| Chinese | Not Found | 7.47 ± 0.94 | 146 | CT | ||||
| Japanese | 8.1 ± 1.2 | 166 [14] | Radio-graphy | <0.001 | ||||
| Japanese | 6.6 ± 1.2 | 166 [14] | CT | <0.001 | ||||
| German | 10.4 ± 2.4 | 234 [29] | Radio-graphy | <0.001 | ||||
| German | 9.2 ± 1.8 | 234 [29] | MRI | <0.001 | ||||
| American | †† | 11.1 ± 1.4 | 8 [28] | Radio-graphy | <0.001 | |||
| CHD (mm) | ||||||||
| Chinese | Not Found | 9.90 ± 2.25 | 146 | CT | ||||
| Turkish | 9.35 ± 2.52 | 58 [32] | MRI | 0.151 | ||||
| American | 10.00 ± 1.33 | 35 [20] | MRI | 0.733 | ||||
| American | †† | 11.00 ± 0.43 | 50 [30] | MRI | <0.001 | |||
| GHD (mm) | ||||||||
| Chinese | Not Found | 1.98 ± 0.33 | 146 | CT | ||||
| Swedish | †† | 4.68 ± 0.35 | 175 [31] | Radio-graphy | <0.001 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, X.; Liu, C.; Liang, T.; Ren, J.; Su, S.; Li, P.; Zhu, S.; Chen, Y.; Peng, Y.; He, W.; et al. In Vivo Anatomical Research by 3D CT Reconstruction Determines Minimum Acromiohumeral, Coracohumeral, and Glenohumeral Distances in the Human Shoulder: Evaluation of Age and Sex Association in a Sample of the Chinese Population. J. Pers. Med. 2022, 12, 1804. https://doi.org/10.3390/jpm12111804
Chen X, Liu C, Liang T, Ren J, Su S, Li P, Zhu S, Chen Y, Peng Y, He W, et al. In Vivo Anatomical Research by 3D CT Reconstruction Determines Minimum Acromiohumeral, Coracohumeral, and Glenohumeral Distances in the Human Shoulder: Evaluation of Age and Sex Association in a Sample of the Chinese Population. Journal of Personalized Medicine. 2022; 12(11):1804. https://doi.org/10.3390/jpm12111804
Chicago/Turabian StyleChen, Xi, Chang Liu, Tangzhao Liang, Jianhua Ren, Shouwen Su, Ping Li, Shaoshen Zhu, Yanbin Chen, You Peng, Weiping He, and et al. 2022. "In Vivo Anatomical Research by 3D CT Reconstruction Determines Minimum Acromiohumeral, Coracohumeral, and Glenohumeral Distances in the Human Shoulder: Evaluation of Age and Sex Association in a Sample of the Chinese Population" Journal of Personalized Medicine 12, no. 11: 1804. https://doi.org/10.3390/jpm12111804