
The Use of Iloprost in the Treatment of Bone Marrow Edema Syndrome of the Proximal Femur: A Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Inclusion Criteria
- -
- Intravenous iloprost therapy alone;
- -
- Localization of the BME at the proximal femur;
- -
- German or English language;
- -
- Documentation of HHS, pain on a VAS, or MRI findings over a period of at least one month;
- -
- If applicable, documentation of surgery rate and conversion to total joint arthroplasty.
2.3. Data-Extraction
- -
- VAS (before and after intervention to form a delta VAS);
- -
- HHS (before and after intervention to form a delta HHS);
- -
- Named as nonresponders or, if not named, failures in terms of subjective or/and MR-tomographic unchanged or worsened condition;
- -
- Follow-up surgery including conversion to total joint arthroplasty.
2.4. Exclusion Criteria
2.5. Risk of Bias Assessment
2.6. Meta Analysis
3. Results
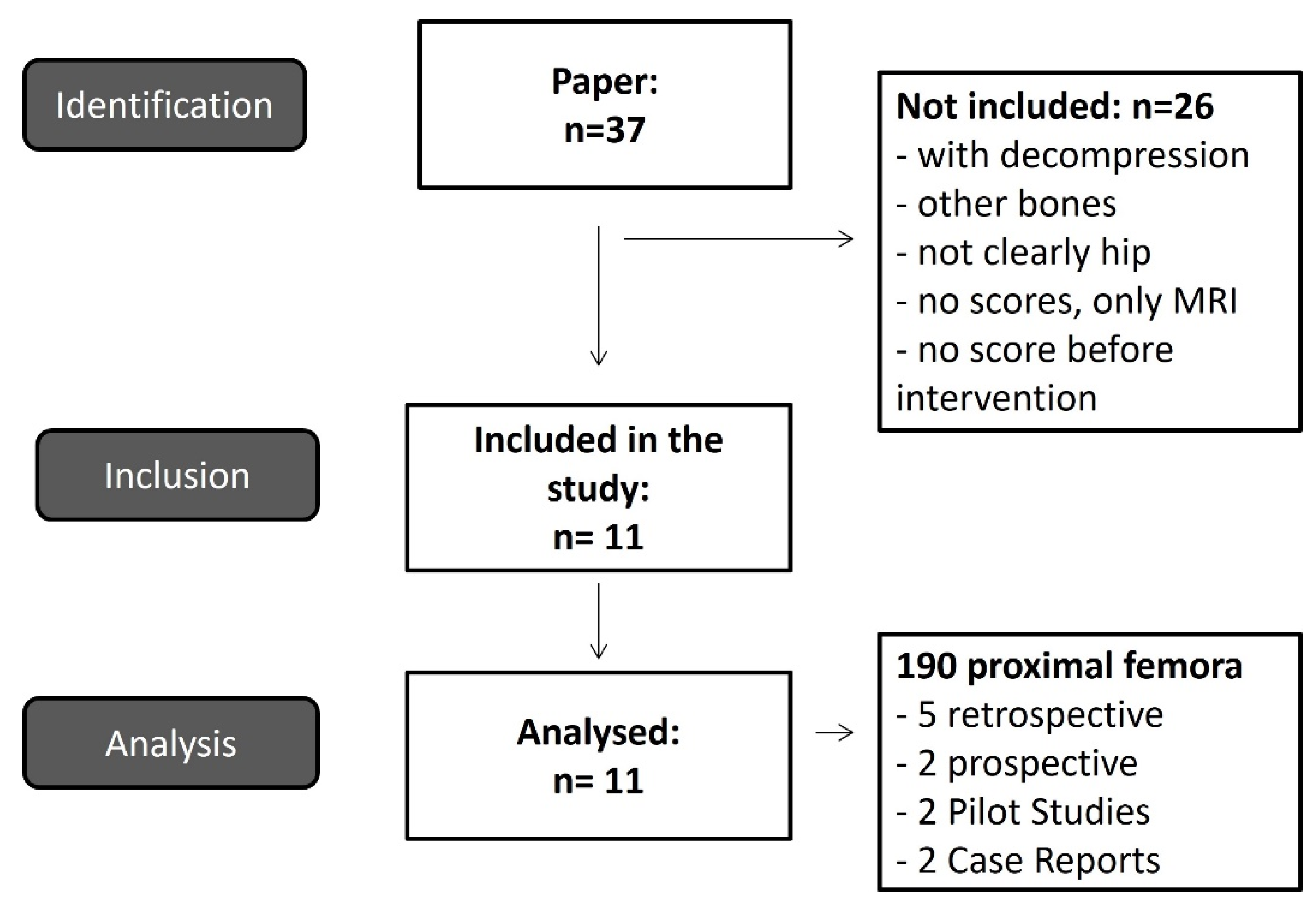
3.1. Identification and Selection of Study Data and Study Characteristics
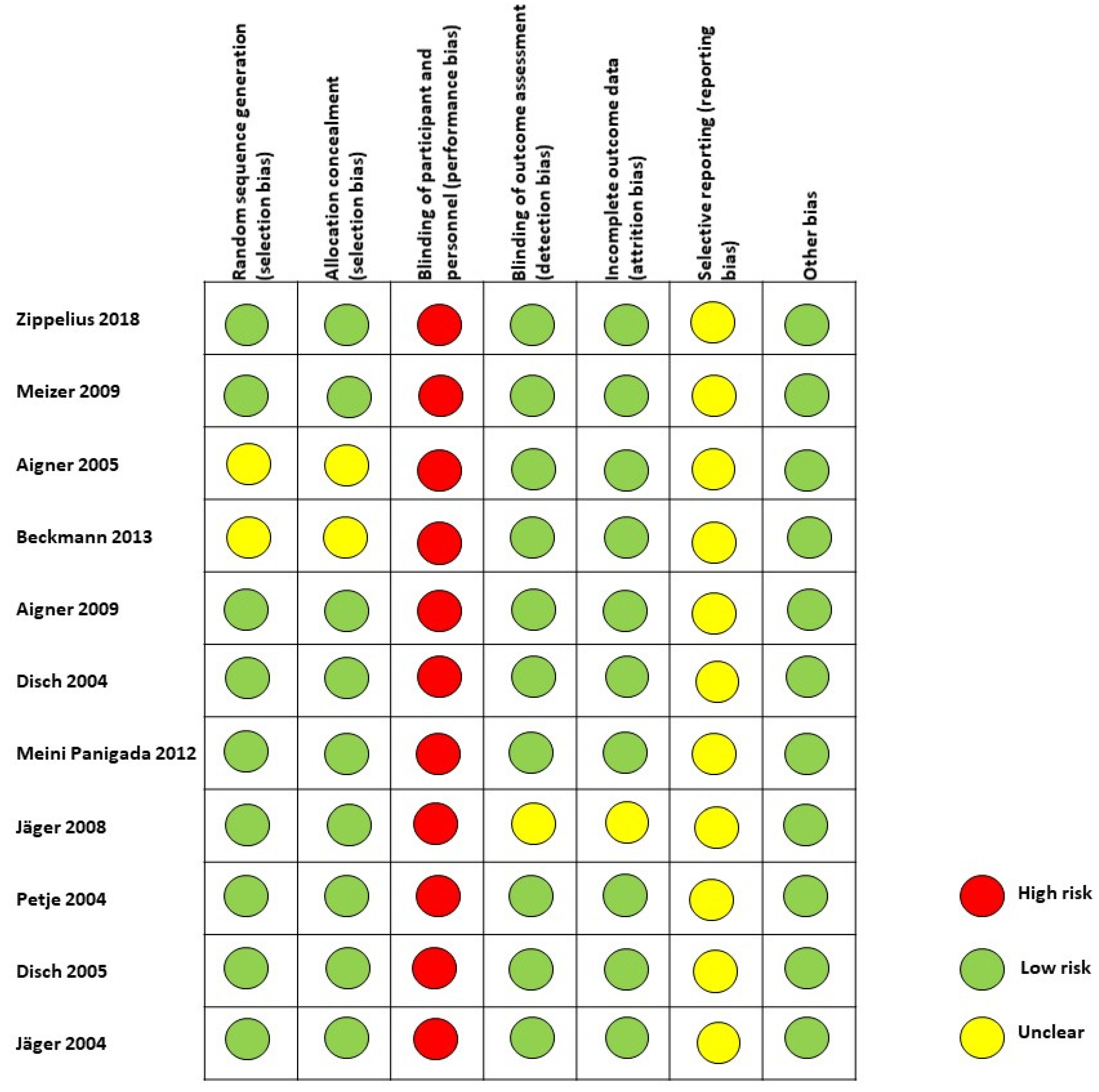
3.2. Risk of Bias
3.3. Heterogeneity of Included Studies
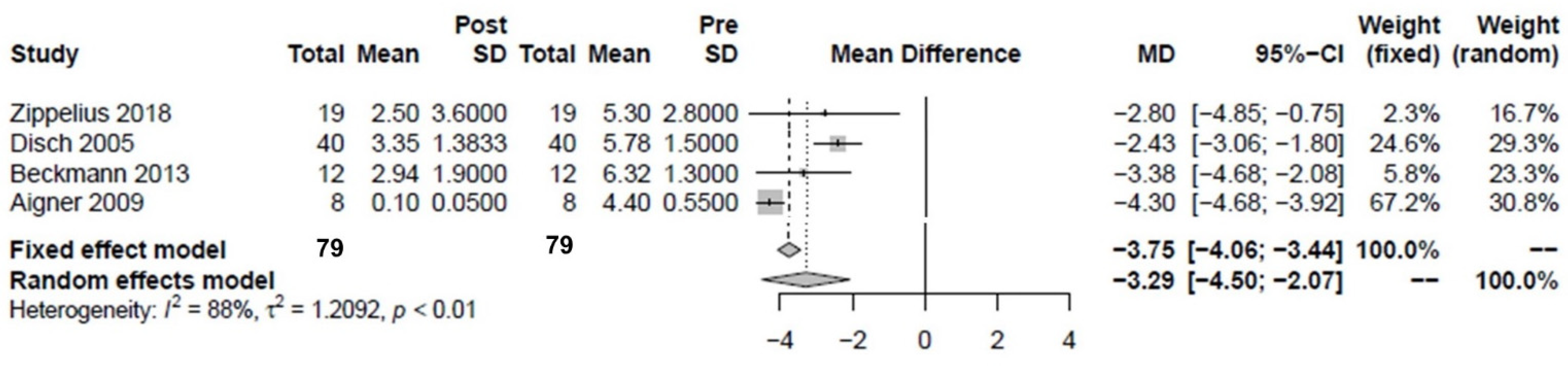
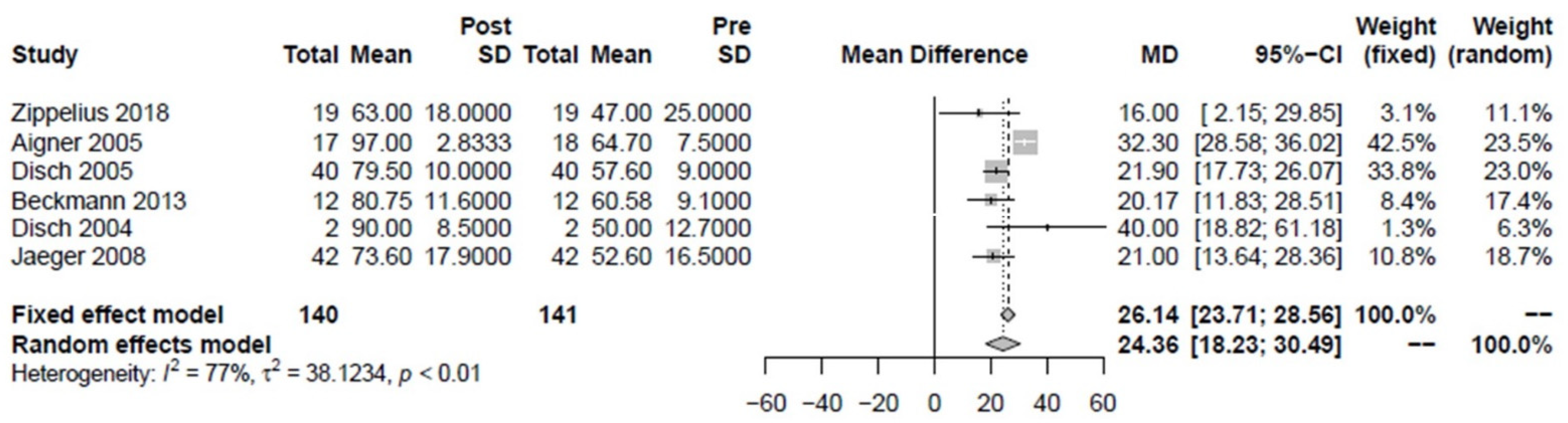
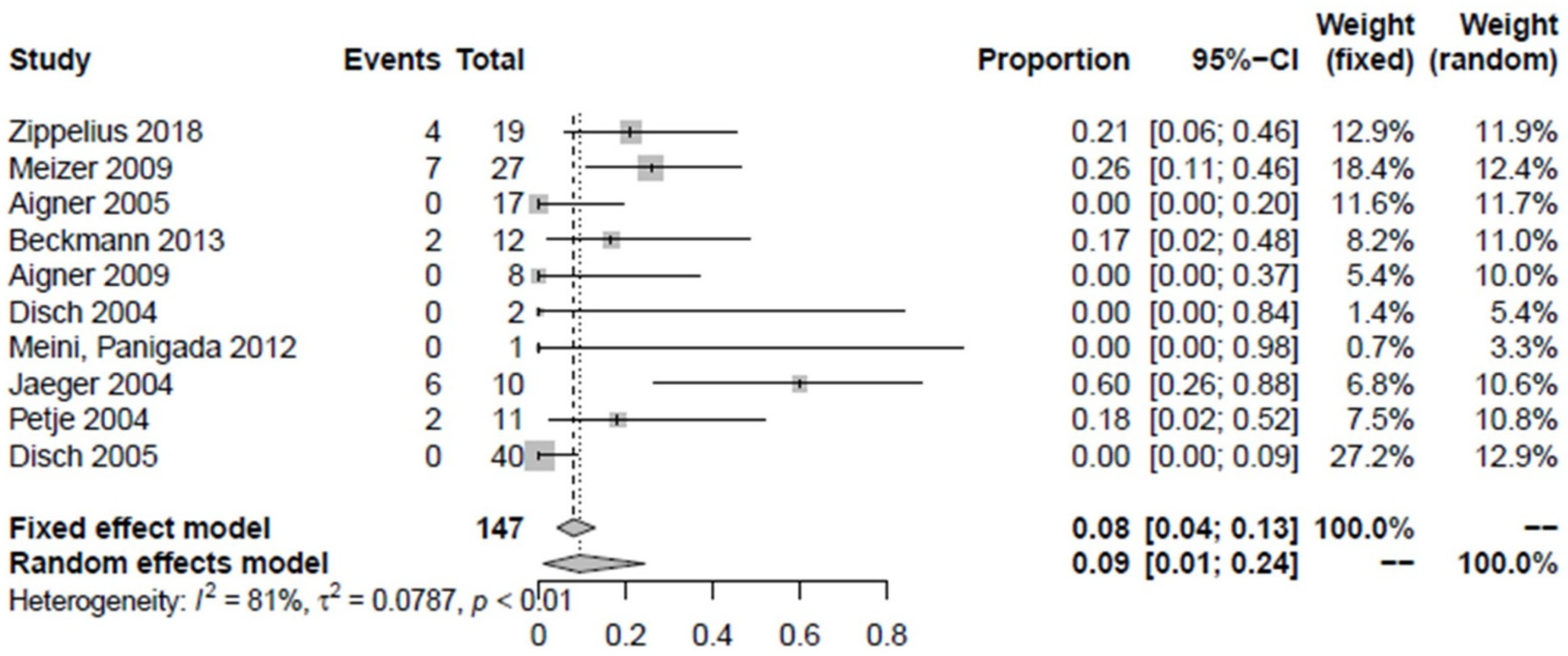
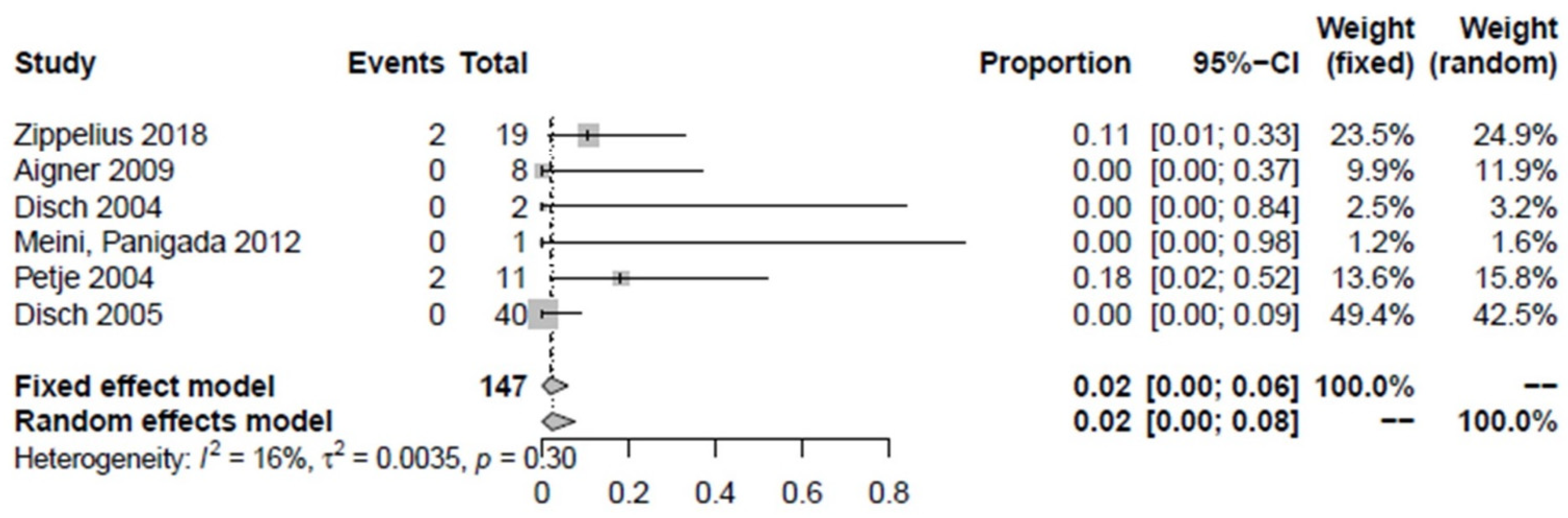
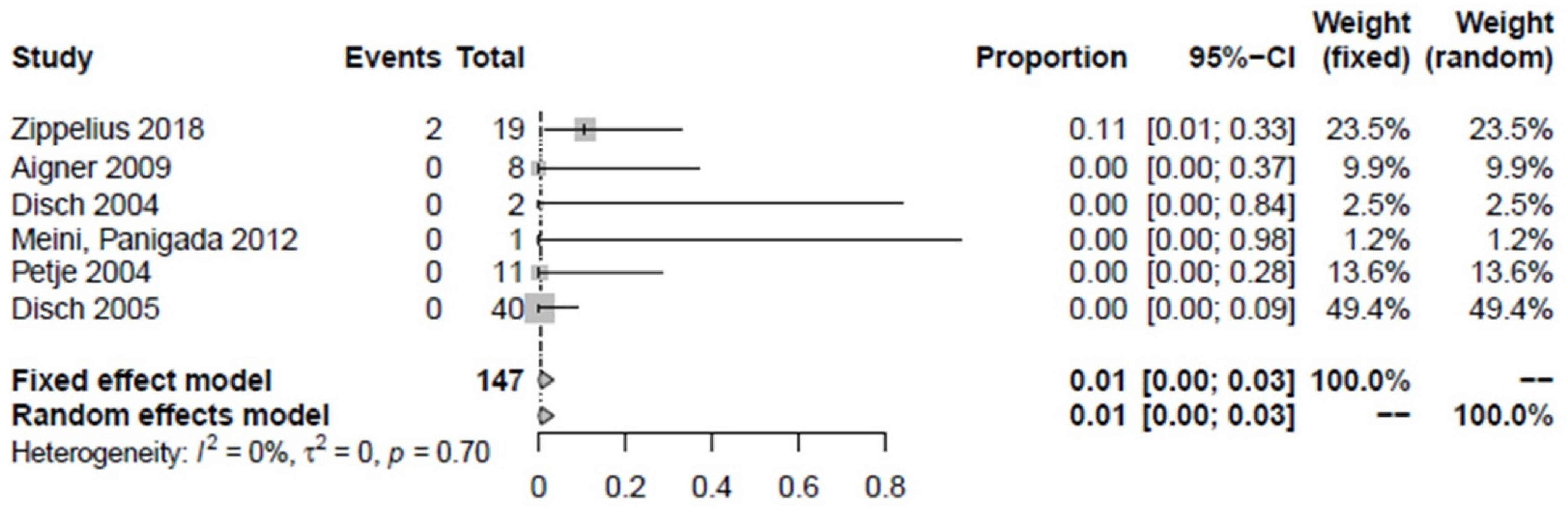
3.4. Therapeutic Effects after Intervention with Iloprost
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pountos, I.; Giannoudis, P.V. The role of Iloprost on bone edema and osteonecrosis: Safety and clinical results. Expert Opin. Drug Saf. 2018, 17, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Zippelius, T.; Perka, C.; Preininger, B.; Matziolis, G.; Strube, P.; Röhner, E. Long-term effects of intravenous iloprost therapy in patients with bone marrow oedema of the hip. Acta Orthop. Belg. 2018, 84, 172–178. [Google Scholar] [PubMed]
- Aigner, N.; Petje, G.; Schneider, W.; Krasny, C.; Grill, F.; Landsiedl, F. Juvenile bone-marrow oedema of the acetabulum treated by iloprost. J. Bone Jt. Surg. Br. Vol. 2002, 84, 1050–1052. [Google Scholar] [CrossRef]
- Aigner, N.; Schneider, W.; Eberl, V.; Knahr, K. Core decompression in early stages of femoral head osteonecrosis—An MRI-controlled study. Int. Orthop. 2002, 26, 31–35. [Google Scholar] [CrossRef] [Green Version]
- Hofmann, S. The painful bone marrow edema syndrome of the hip joint. Wien. Klin. Wochenschr. 2005, 117, 111–120. [Google Scholar] [CrossRef]
- Disch, A.C.; Matziolis, G.; Perka, C. The management of necrosis-associated and idiopathic bone-marrow oedema of the proximal femur by intravenous iloprost. J. Bone Jt. Surg. Br. Vol. 2005, 87, 560–564. [Google Scholar] [CrossRef] [Green Version]
- Röhner, E.; Zippelius, T.; Steindl, D.; Fussi, J.; Perka, C. Effects of intravenous iloprost therapy in patients with bone marrow oedema of the foot and ankle. Eur. J. Orthop. Surg. Traumatol. 2013, 24, 1609–1616. [Google Scholar] [CrossRef]
- Zippelius, T.; Matziolis, G.; Perka, C.; Putzier, M.; Strube, P.; Röhner, E. Long-Term Effects of Intravenous Iloprost Therapy in Patients with Bone Marrow Oedema of the Knee Joint. Acta Chir. Orthop. Traumatol. Cechoslov. 2018, 85, 17–21. [Google Scholar]
- Starr, A.M.; Wessely, M.A.; Albastaki, U.; Pierre-Jerome, C.; Kettner, N.W. Bone marrow edema: Pathophysiology, differential diagnosis, and imaging. Acta Radiol. 2008, 49, 771–786. [Google Scholar] [CrossRef]
- Hofmann, S.; Kramer, J.; Vakil-Adli, A.; Aigner, N.; Breitenseher, M. Painful bone marrow edema of the knee: Differential diagnosis and therapeutic concepts. Orthop. Clin. N. Am. 2004, 35, 321–333. [Google Scholar] [CrossRef]
- Jones, J. Osteonecrosis and bone marrow edema syndrome: Similar etiology but a different pathogenesis. In Osteonecrosis: Etiology, Diagnosis, and Treatment; Urbaniak, J.R., Jones, J.P., Eds.; American Academy of Orthopaedic Surgeons: Rosemont, IL, USA, 1997; pp. 181–187. [Google Scholar]
- Meizer, R.; Radda, C.; Stolz, G.; Kotsaris, S.; Petje, G.; Krasny, C.; Wlk, M.; Mayetrhöfer, M.; Landsiedl, F.; Aligner, N. MRI-controlled analysis of 104 patients with painful bone marrow edema in different joint localizations treated with the prostacyclin analogue iloprost. Wien. Klin. Wochenschr. 2005, 117, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Breitenseher, M.J.; Kramer, J.; Mayerhoefer, M.E.; Aigner, N.; Hofmann, S. Differential diagnosis of bone marrow edema of the knee joint. Radiologe 2006, 46, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Schmitt-Sody, M.; Kirchhoff, C.; Mayer, W.; Goebel, M.; Jansson, V. Avascular necrosis of the femoral head: Inter- and intraobserver variations of Ficat and ARCO classifications. Int. Orthop. 2008, 32, 283–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmann, S.; Mazières, B. Osteonecrosis: Natural course and conservative therapy. Orthopade 2000, 29, 403–410. [Google Scholar] [PubMed]
- Zippelius, T.; Hoff, P.; Strube, P.; Schiffner, R.; Maslaris, A.; Matziolis, G.; Röhner, E. Effects of iloprost on human mature osteoblasts in vitro. J. Back Musculoskelet. Rehabil. 2019, 32, 897–903. [Google Scholar] [CrossRef]
- Jäger, M.; Zilkens, C.; Bittersohl, B.; Matheney, T.; Kozina, G.; Blondin, D.; Krauspe, R. Efficiency of iloprost treatment for osseous malperfusion. Int. Orthop. 2010, 35, 761–765. [Google Scholar] [CrossRef] [Green Version]
- Beckmann, J.; Schmidt, T.; Schaumburger, J.; Rath, B.; Lüring, C.; Tingart, M.; Grifka, J. Infusion, core decompression, or infusion following core decompression in the treatment of bone edema syndrome and early avascular osteonecrosis of the femoral head. Rheumatol. Int. 2012, 33, 1561–1565. [Google Scholar] [CrossRef]
- Roth, A.; Beckmann, J.; Smolenski, U.; Fischer, A.; Jäger, M.; Tingart, M.; Rader, C.; Peters, K.M.; Reppenhagen, S.; Nöth, U.; et al. S3 guideline. Part 2: Non-traumatic avascular femoral head necrosis in adults-untreated course and conservative treatment. Z. Orthop. Unf. 2015, 153, 488–497. [Google Scholar]
- Claßen, T.; Becker, A.; Landgraeber, S.; Haversath, M.; Li, X.; Zilkens, C.; Krauspe, R.; Jäger, M. Long-term clinical results after iloprost treatment for bone marrow edema and avascular necrosis. Orthop. Rev. 2016, 8, 6150. [Google Scholar] [CrossRef] [Green Version]
- Ghasemi, R.A.; Sadeghi, S.; Rahimee, N.; Tahmasebi, M. Technologies in the Treatment of Bone Marrow Edema Syndrome. Orthop. Clin. N. Am. 2018, 50, 131–138. [Google Scholar] [CrossRef]
- Maus, U.; Flechtenmacher, J.; Peters, K.M. Conservative treatment of atraumatic femoral head necrosis. Orthopade 2018, 47, 735–744. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.M.; Goa, K.L. Iloprost. A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic potential in peripheral vascular disease, myocardial ischemia and extracorporeal circulation procedures. Drugs 1992, 43, 889–924. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef] [Green Version]
- Meizer, R.; Meraner, D.; Meizer, E.; Radda, C.; Landsiedl, F.; Aigner, N. Outcome of painful bone marrow edema of the femoral head following treatment with parenteral iloprost. Indian J. Orthop. 2009, 43, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Aigner, N.; Petje, G.; Schneider, W.; Meizer, R.; Wlk, M.; Kotsaris, S.; Knahr, K.; Landsiedl, F. Bone marrow edema syndrome of the femoral head: Treatment with the prostacyclin analogue iloprost vs. core decompression: An MRI-controlled study. Wien. Klin. Wochenschr. 2005, 117, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Aigner, N.; Meizer, R.; Meraner, D.; Becker, S.; Meizer, E.; Landsiedl, F. Bone Marrow Edema Syndrome in Postpartal Women: Treatment with Iloprost. Orthop. Clin. N. Am. 2009, 40, 241–247. [Google Scholar] [CrossRef]
- Disch, A.C.; Matziolis, G.; Reinke, P.; Perka, C. Intravenous Iloprost treatment for severe bone pain caused by sickle cell crisis. Thromb. Haemost. 2004, 91, 1047–1049. [Google Scholar] [PubMed]
- Meini, S.; Panigada, G. Proposal of early retreatment with iloprost in partially responsive patients with bone marrow edema syndrome: A case report. Ital. J. Med. 2012, 6, 332–337. [Google Scholar] [CrossRef]
- Jäger, M.; Tillmann, F.P.; Thornhill, T.S.; Mahmoudi, M.; Blondin, D.; Hetzel, G.R.; Zilkens, C.; Krauspe, R. Rationale for prostaglandin I2 in bone marrow oedema--from theory to application. Arthritis Res. Ther. 2008, 10, R120. [Google Scholar] [CrossRef] [Green Version]
- Petje, G.; Radler, C.; Aigner, N.; Manner, H.; Kriegs-Au, G.; Grill, F. Pharmacological management of aseptic osteonecrosis in children. Expert Opin. Pharmacother. 2004, 5, 1455–1462. [Google Scholar] [CrossRef]
- Jager, M.; Werner, A.; Lentrodt, S.; Modder, U.; Krauspe, R. Pain management in non-juvenile, aseptic osteonecrosis. Schmerz 2004, 18, 481–491. [Google Scholar]
- Aigner, N.; Petje, G.; Steinboeck, G.; Schneider, W.; Krasny, C.; Landsiedl, F. Treatment of bone-marrow oedema of the talus with the prostacyclin analogue iloprost. An MRI-controlled investigation of a new method. J. Bone Jt. Surg. Br. Vol. 2001, 83, 855–858. [Google Scholar] [CrossRef]
- Aigner, N.; Petje, G.; Steinboeck, G.; Schneider, W.; Krasny, C.; Landsiedl, F. Bone Marrow Edema of the Forefoot after Chevron Osteotomy—A Rare Cause of Metatarsalgia: A Case Report. Foot Ankle Int. 2002, 23, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Aigner, N.; Meizer, R.; Stolz, G.; Petje, G.; Krasny, C.; Landsiedl, F.; Steinboeck, G. Iloprost for the treatment of bone marrow edema in the hindfoot. Foot Ankle Clin. 2003, 8, 683–693. [Google Scholar] [CrossRef]
- Aigner, N.; Radda, C.; Meizer, R.; Petje, G.; Kotsaris, S.; Krasny, C.; Landsiedl, F.; Steinboeck, G. Bone marrow edema in the foot—MRI findings after conservative therapy. Foot Ankle Surg. 2005, 11, 87–91. [Google Scholar] [CrossRef]
- Aigner, N.; Meizer, R.; Petje, G.; Meizer, E.; Abdelkafy, A.; Landsiedl, F. Natural course of intra-articular shifting bone marrow edema syndrome of the knee. BMC Musculoskelet. Disord. 2008, 9, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anagnostakos, K.; Orth, P. Role of Serum Lipoprotein at the Site of Iloprost Therapy in the Treatment of Painful Bone Marrow Edema. Orthopedics 2013, 36, e1283–e1289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arazi, M.; Yel, M.; Uguz, B.; Emlik, D. Be aware of bone marrow edema syndrome in ankle arthroscopy: A case successfully treated with iloprost. Arthroscopy 2006, 22, 909.e1–909.e3. [Google Scholar] [CrossRef]
- Arazi, M.; Kiresi, D. Bone marrow edema syndrome of the third metatarsal bone: A rare cause of metatarsalgia treated with Iloprost. Eur. J. Orthop. Surg. Traumatol. 2010, 21, 59–62. [Google Scholar] [CrossRef]
- Baier, C.; Schaumburger, J.; Götz, J.; Heers, G.; Schmidt, T.; Grifka, J.; Beckmann, J. Bisphosphonates or prostacyclin in the treatment of bone-marrow oedema syndrome of the knee and foot. Rheumatol. Int. 2012, 33, 1397–1402. [Google Scholar] [CrossRef]
- Hörterer, H.; Baumbach, S.F.; Gregersen, J.; Kriegelstein, S.; Gottschalk, O.; Szeimies, U.; Walther, M. Treatment of Bone Marrow Edema of the Foot and Ankle With the Prostacyclin Analog Iloprost. Foot Ankle Int. 2018, 39, 1183–1191. [Google Scholar] [CrossRef]
- Huang, Y.-G.; Chia, W.K.; Jin, D.; Gao, Y.; Sheng, J.; Zhang, C. Bone marrow lesion on magnetic resonance imaging indicates the last chance for hip osteonecrosis treated with vascularized fibular grafting before collapse. Int. Orthop. 2020, 44, 2529–2536. [Google Scholar] [CrossRef] [PubMed]
- Jäger, M.; Zilkens, C.; Westhoff, B.; Jelinek, E.M.; Kozina, G.; Krauspe, R. Efficiency of iloprost treatment for chemotherapy-associated osteonecrosis after childhood cancer. Anticancer Res. 2009, 29, 3433–3440. [Google Scholar] [PubMed]
- Lackner, H.; Benesch, M.; Moser, A.; Smolle-Jüttner, F.; Linhart, W.; Raith, J.; Urban, C. Aseptic osteonecrosis in children and adolescents treated for hemato-oncologic diseases: A 13-year longitudinal observational study. J. Pediatr. Hematol. Oncol. 2005, 27, 259–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmoudi, M. Therapie der Nicht-Juvenilen, Aseptischen Osteonekrose und des Symptomatischen Knochenmarködems mit dem Prostazyklin-Analogon Iloprost: Eie MRT-Kontrollierte Klinische. Ph.D. Thesis, Heinrich Heine University Düsseldorf, Düsseldorf, Germany, 2009. [Google Scholar]
- Mayerhoefer, M.E.; Kramer, J.; Breitenseher, M.J.; Norden, C.; Vakil-Adli, A.; Hofmann, S.; Meizer, R.; Siedentop, H.; Landsiedl, F.; Aigner, N. Short-term outcome of painful bone marrow oedema of the knee following oral treatment with iloprost or tramadol: Results of an exploratory phase II study of 41 patients. Rheumatology 2007, 46, 1460–1465. [Google Scholar] [CrossRef] [Green Version]
- Mayerhoefer, M.E.; Kramer, J.; Breitenseher, M.J.; Norden, C.; Vakil-Adli, A.; Hofmann, S.; Meizer, R.; Siedentop, H.; Landsiedl, F.; Aigner, N. MRI-demonstrated outcome of subchondral stress fractures of the knee after treatment with iloprost or tramadol: Observations in 14 patients. Clin. J. Sport Med. 2008, 18, 358–362. [Google Scholar] [CrossRef] [PubMed]
- Petje, G.; Radler, C.; Aigner, N.; Kriegs-Au, G.; Ganger, R.; Grill, F. Aseptic osteonecrosis in childhood: Diagnosis and treatment. Orthopade 2002, 31, 1027–1038. [Google Scholar] [CrossRef]
- Pilge, H.; Bittersohl, B.; Schneppendahl, J.; Hesper, T.; Zilkens, C.; Ruppert, M.; Krauspe, R.; Jäger, M. Bone marrow aspirate concentrate in combination with intravenous iloprost increases bone healing in patients with avascular necrosis of the femoral head: A matched pair analysis. Orthop. Rev. 2016, 8, 6902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tillmann, F.P.; Jager, M.; Blondin, D.; Schooldermann, D.; Voiculescu, A.; Sucker, C.; Grabensee, B.; Krauspe, R.; Hetzel, G.R. Intravenous iloprost: A new therapeutic option for patients with post-transplant distal limb syndrome (PTDLS). Am. J. Transplant 2007, 7, 667–671. [Google Scholar] [CrossRef] [PubMed]
- Tosun, H.B.; Uludağ, A.; Demir, S.; Serbest, S.; Yasar, M.M.; Öznam, K. Effectiveness of Iloprost in the Treatment of Bone Marrow Edema. Cureus 2020, 12, e10547. [Google Scholar] [CrossRef] [PubMed]
- Der Simonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Study Design | Number of Proximal Femora | Gender | Dose | MRI Result | Failure | Control Group | Control after | Follow-Up | Partial Load | Besonderheit | VAS | HHS |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Zippelius [2] | 2018 | retrospective | 19 | 7 women, 12 men | 0.5 ng/kg/min over 6 h over 5 days | After 3 months: 15/19 complete edema regression | 4 surgeries (2× cannulation, 2× TEP) | / | 3, approx. 29 months | 29 ± 11 months | 6 weeks | X only after 29 months | X only after 29 months | |
| Meizer [25] | 2009 | retrospective | 27 | 8 women, 19 men | 50–20 μg over 6 h for 5 days; start with 50, reduce if needed | After 4 months: 20/27 improved on MRI, unchanged, 3 worsened | 7 nonresponders (named) | / | 4 months | 4 months | 3 weeks | 81% less pain at rest, 63% less activity pain | Other score | - |
| Aigner [26] | 2005 | retrospective | 18 | 4 women, 13 men | 20 μg over 6 h for 5 days | After 3 months: Complete edema regression in all femora | / | Core decompression group | 3, 12 months | 11 months | Partial (for 5 patients for 3 weeks) | In the iloprost group, one patient had to discontinue treatment due to severe headache (n post: 17 femora) | - | X after 3 months |
| Beckmann [18] | 2013 | retrospective | 12 | 3 women, 9 men | 20–40 μg over 6 h for 5 days, day 1 20 μg, day 2 30 μg, day 3–5 40 μg | After 3 months: Reduction from BME, not from ON | 2 nonresponders by pain indication (named) | Core decompression, core decompression with ilomedin | 3, 12 months | 13 months (11–16) (all groups) | 6 weeks | The combination of iloprost and tapping shows the best results | X after 3 months | X after 3 months |
| Aigner [27] | 2009 | prospective | 8 | 6 women | 20 μg over 6 h for 5 days, start 10 days after birth | After 3 months: Complete remission in 5, subtotal in 1 pat (all BME.) No progression at last follow-up | / | / | 1, 3 months | 31 months (14–43) | unknown | All six subjects improved immediately during the first 2 weeks after initiation of intravenous therapy | X after 3 months at rest | - |
| Disch [28] | 2004 | Case Report | 2 | 1 man (with sickle cell anemia) | 0.5–1.0 μg/kg/min over 6 h/d for 5 days; day 1 0.5 μg, day 2 0.75 μg, day 3–5 1 μg | After 3 months: Significant reduction of edema in both femora | / | / | 1, 3 months | 3 months | unknown | Already after the 3rd day less pain. Further improvement in the next 4 weeks regarding ROM | - | X after 1 month |
| Meini, Panigada [29] | 2012 | Case Report | 1 | 1 woman | 2 ng/kg/min over 6 h for 5 days, after 4 weeks repeat with 1.5 ng/kg/min over 6 h for 5 days | After 4 weeks, reduction of edema, then iloprost again. Then, after 4 weeks, further reduction; after three more months, control/complete remission | / | / | 1, 2, 5 months after first treatment | 5 months after first treatment | unknown | During treatment with iloprost from the third day significant reduction of pain and joint dysfunction | X after second therapy | X after second therapy |
| Jäger [30] 1 | 2008 | prospective | 42 | 28 women, 22 men (total 117 bones) | 0.5–1.0 ng/kg/min over 6 h for 5 days | Significant reduction of edema after 3 and 6 months. After 6 months, complete regression in 65 of 117 bones. Advanced ARCO stages (III, IV) were not affected by iloprost | Not exactly named. However, ARCO III and IV unchanged (total 15 joints) | / | 5 days, 3, 6 months | unknown | X VAS in all bones | X after 3 months | ||
| Petje [31] | 2004 | Long-term pilot study | 11 | 3 women, 4 men | 2 ng/kg/min over 6 h for 5 days | ON progression in 2 patients | 2 Perthes children with Salter surgery and femoral varization osteotomy | / | / | 32 months (12–48) all bones (45 patients) | unknown | - | - | |
| Disch [6] | 2005 | prospective, case-controlled | 40 | 7 women, 26 men | 0.5–1.0 μg/kg/min over 6 h/d for 5 days; day 1 0.5 μg, day 2 0.75, day 3–5 1 μg | Edema reduction in all patients after 3 months | / | 1,3, and approx. 25 months | 25 months (11–37) | unknown | Group I: 16 isolated BME (ARCO I), Group II: 17 ON (ARCO II, III) | X after 3 months | X after 3 months | |
| Jäger [32] | 2004 | prospective | 10 | 2 women, 5 men (total 20 bones) | Unknown dose for 5 days | After 3 months, reduction in 4 proximal femora, no change in another 4, and in 2 (the latter already previously ARCO III & IV) | 6 after MRI | 3 months | 3 months | unknown | unknown | Yes, but all joints at VAS | - |
| Author | Year | Reason for Exclusion |
|---|---|---|
| Aigner [33] | 2001 | Location (talus) |
| Aigner [34] | 2002 | Location (forefoot) |
| Aigner [3] | 2002 | Location (acetabulum) |
| Aigner [35] | 2003 | Location (hindfoot) |
| Aigner [36] | 2005 | Location (foot) |
| Aigner [37] | 2008 | Location (knee) |
| Anagnostakos [38] | 2013 | No clear differentiation of results regarding the proximal femur (21 bones) |
| Arazi [39] | 2006 | Location (ankle) |
| Arazi [40] | 2011 | Location (os metatarsale) |
| Baier [41] | 2013 | Location (knee, foot) |
| Claßen [20] | 2016 | No clear differentiation of results regarding the proximal femur (136 bones) |
| Hörterer [42] | 2018 | Location (foot, ankle) |
| Huang [43] | 2020 | No treatment with iloprost |
| Jäger [44] | 2009 | 3 out of 8 patients had a core decompression, no clear differentiation |
| Jäger [17] | 2011 | No clear differentiation of results regarding the proximal femur (20 bones) |
| Lackner [45] | 2005 | Observational Study: 3 out of 9 patients with iloprost without a clear differentiation |
| Mahmoudi (dissertation) [46] | 2009 | Most likely the same cohort as Jäger 2008, co-author |
| Mayerhoefer [47] | 2007 | Location (knee) |
| Mayerhoefer [48] | 2008 | Location (knee) |
| Meizer [12] | 2005 | No clear differentiation of results regarding the proximal femur (104 bones) |
| Petje [49] | 2002 | No scores, no clear differentiation |
| Pilge [50] | 2016 | Ilomedin therapy with core decompression and bone marrow aspirate |
| Röhner [7] | 2014 | Location (foot, ankle) |
| Tillmann [51] | 2007 | Location (knee, foot) |
| Tosun [52] | 2020 | No clear differentiation of results regarding the proximal femur (23 bones) |
| Zippelius [8] | 2018 | Location (knee) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zippelius, T.; Strube, P.; Rohe, S.; Schlattmann, P.; Dobrindt, O.; Caffard, T.; Awan Malik, H.; Lindemann, C.; Matziolis, G.; Böhle, S. The Use of Iloprost in the Treatment of Bone Marrow Edema Syndrome of the Proximal Femur: A Review and Meta-Analysis. J. Pers. Med. 2022, 12, 1757. https://doi.org/10.3390/jpm12111757
Zippelius T, Strube P, Rohe S, Schlattmann P, Dobrindt O, Caffard T, Awan Malik H, Lindemann C, Matziolis G, Böhle S. The Use of Iloprost in the Treatment of Bone Marrow Edema Syndrome of the Proximal Femur: A Review and Meta-Analysis. Journal of Personalized Medicine. 2022; 12(11):1757. https://doi.org/10.3390/jpm12111757
Chicago/Turabian StyleZippelius, Timo, Patrick Strube, Sebastian Rohe, Peter Schlattmann, Oliver Dobrindt, Thomas Caffard, Hassan Awan Malik, Chris Lindemann, Georg Matziolis, and Sabrina Böhle. 2022. "The Use of Iloprost in the Treatment of Bone Marrow Edema Syndrome of the Proximal Femur: A Review and Meta-Analysis" Journal of Personalized Medicine 12, no. 11: 1757. https://doi.org/10.3390/jpm12111757