
Pressure- and 3D-Derived Coronary Flow Reserve with Hydrostatic Pressure Correction: Comparison with Intracoronary Doppler Measurements

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Inclusion and Exclusion Criteria
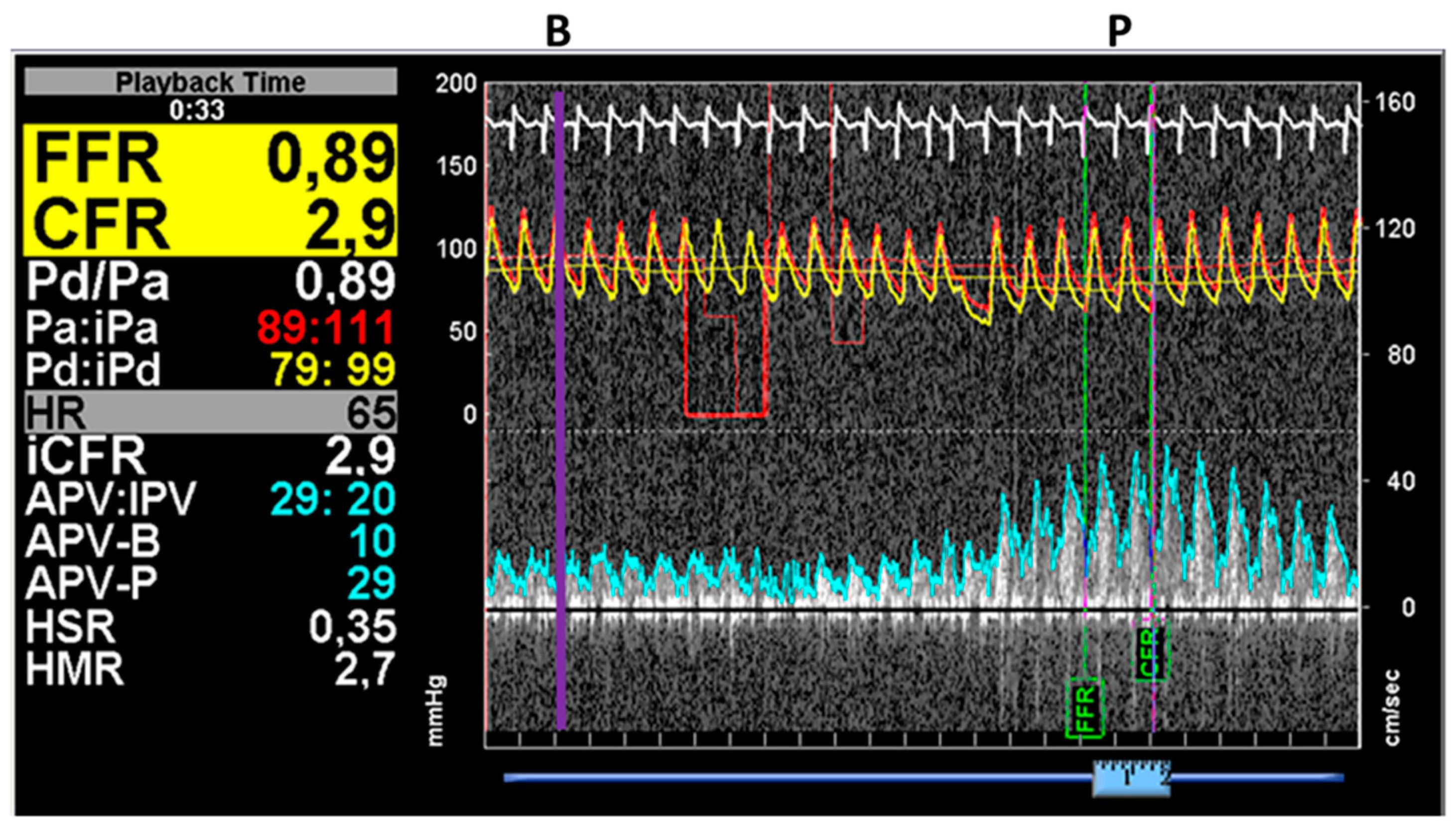
2.2. Invasive Coronary Angiography and Simultaneous Pressure and Flow Measurement by ComboWire
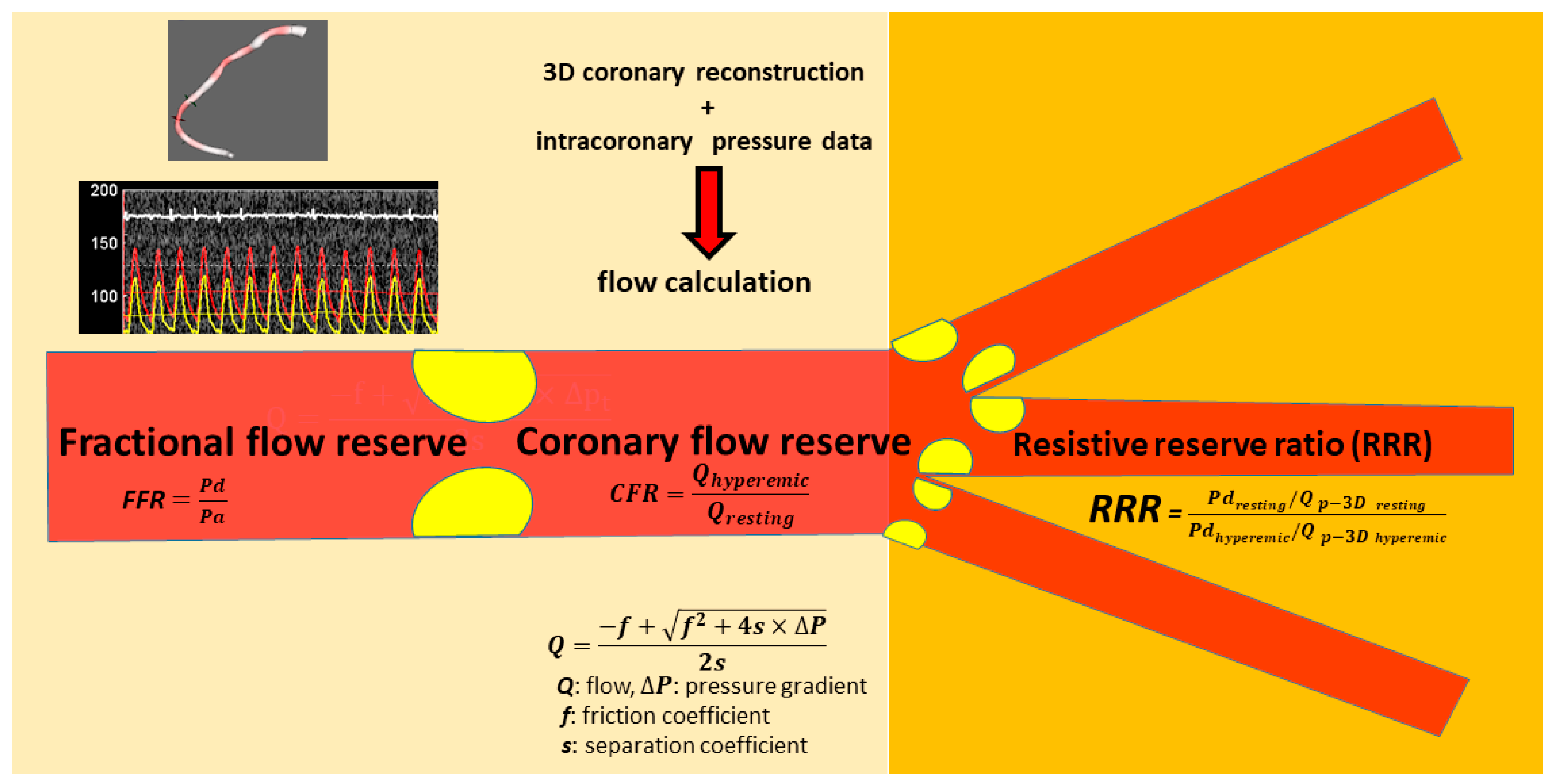
2.3. Three-Dimensional Quantitative Coronary Artery Reconstruction and Hemodynamic Calculations
2.4. Calculation of the Doppler-Derived Indices
2.5. Calculation of the RRRp-3D
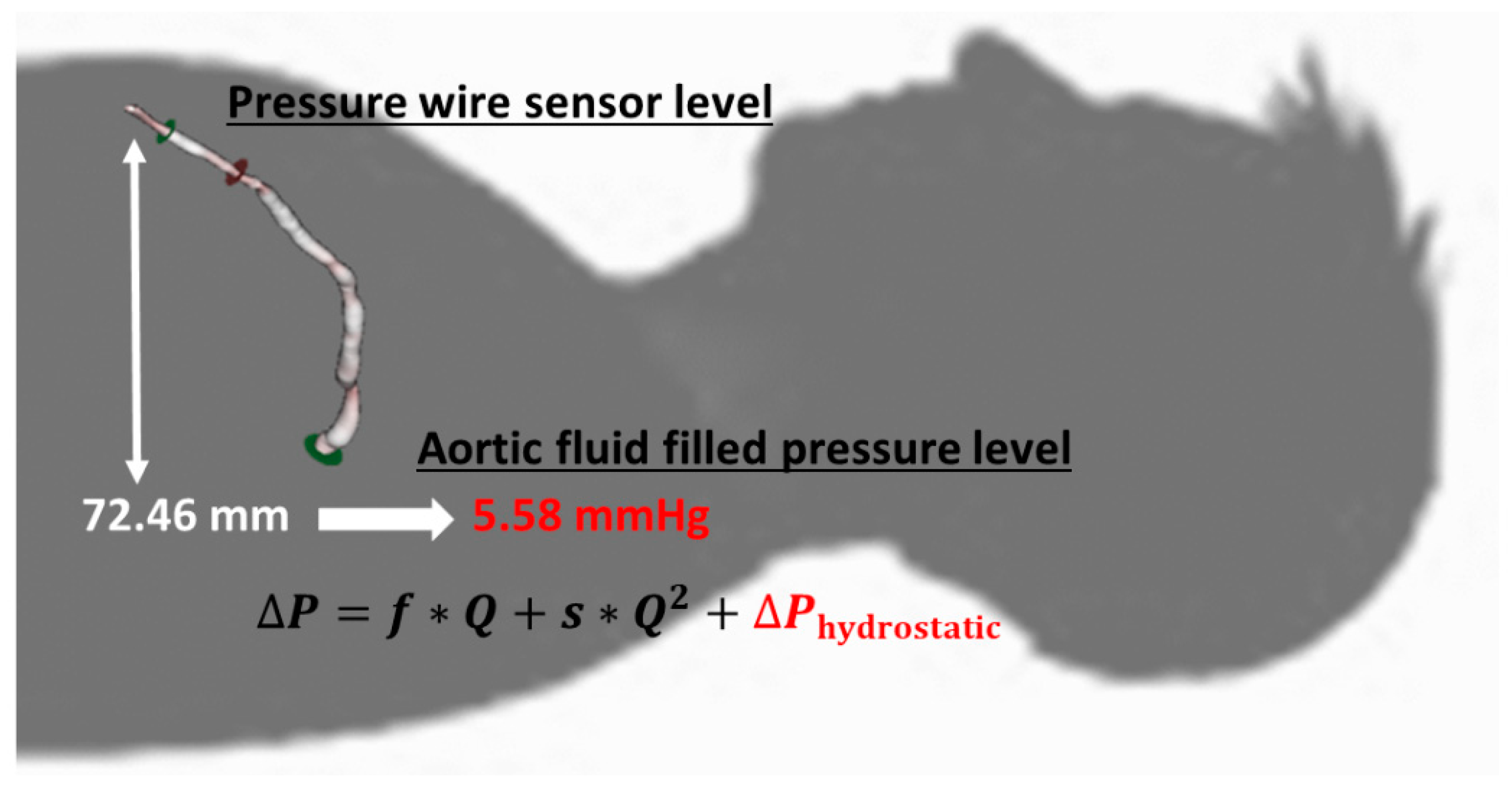
2.6. Correction of the Distal Coronary Pressure for Hydrostatic Pressure
2.7. Statistical Analysis
3. Results
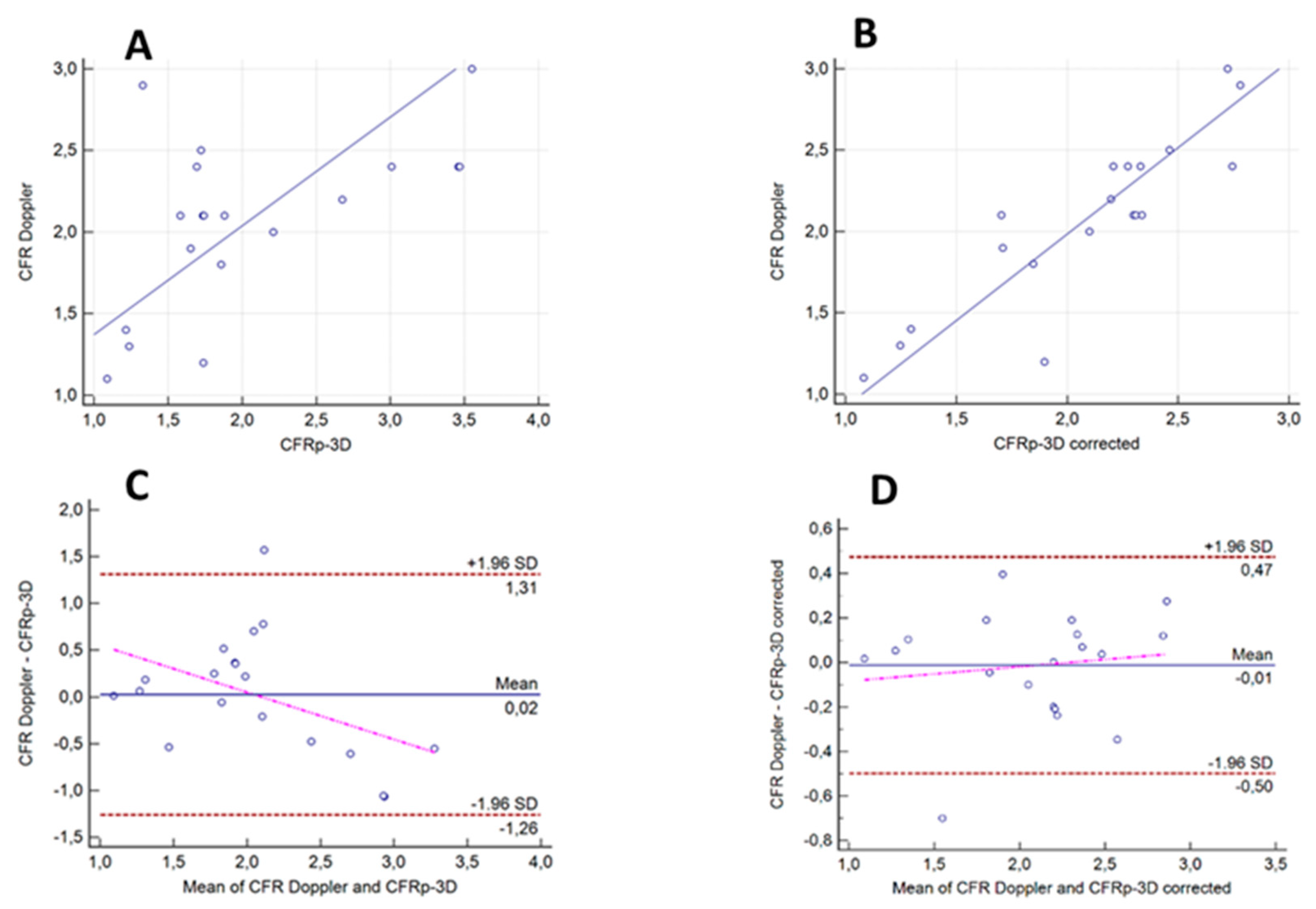
3.1. Correlation and Agreement between the Results of the CFRDoppler Measurements and Calculated CFRp-3D Values without and with the Correction for Hydrostatic Offset
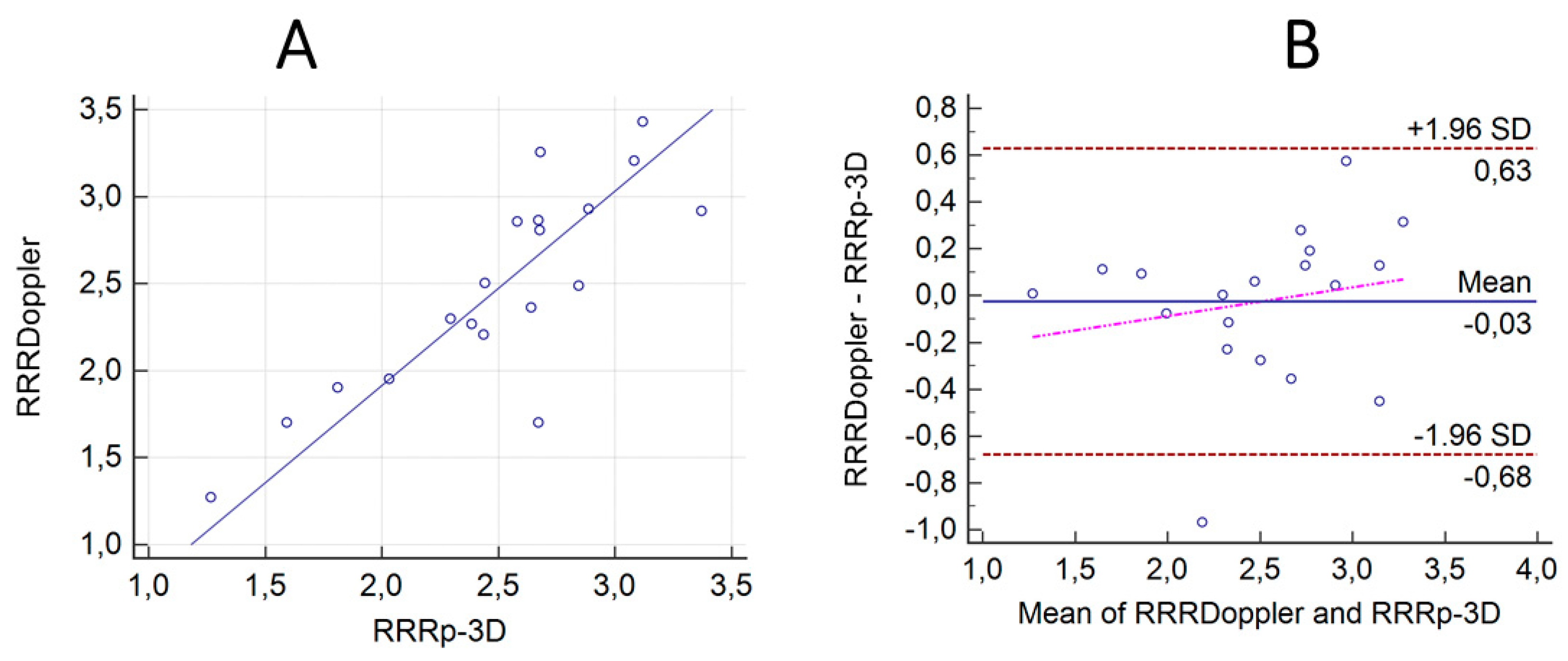
3.2. Correlation and Agreement between the Results of the ComboWire Based RRR Measurements (RRRDoppler) and the Calculated RRRp-3D Values with the Correction for Hydrostatic Offset
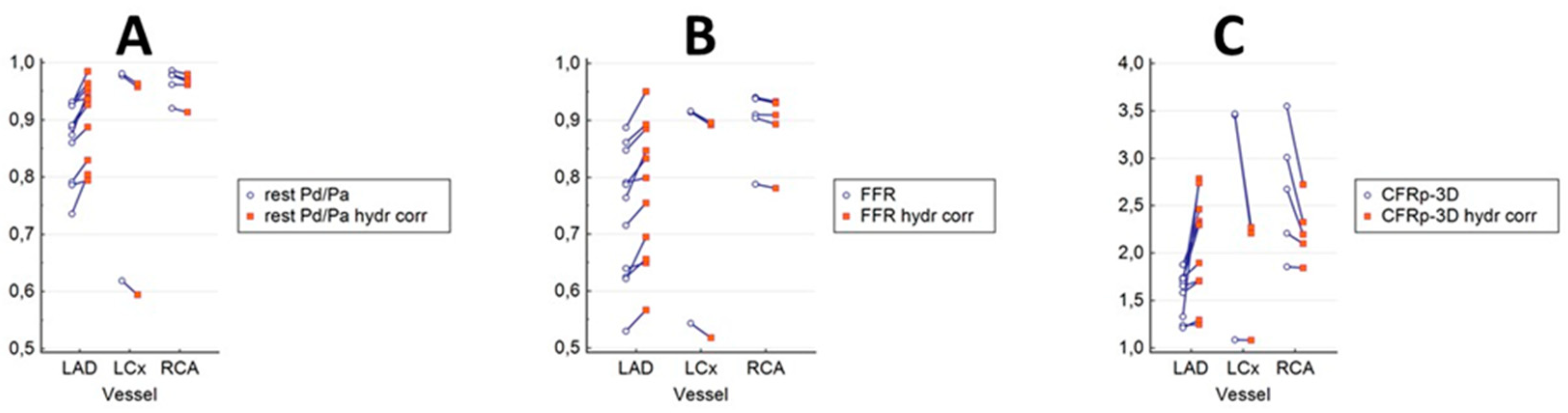
3.3. The Results of Hydrostatic Offset Correction on the Pressure Ratios and the CFRp-3D in the Main Coronary Branches
3.4. Diagnostic Powers of CFRp-3D Calculated from the Distal Pressure without and with Hydrostatic Offset Correction for Identifying CFRDoppler < 2
4. Discussion
5. Limitations of the Study
6. Conclusions
7. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef]
- Sara, J.D.; Widmer, R.J.; Matsuzawa, Y.; Lennon, R.J.; Lerman, L.O.; Lerman, A. Prevalence of coronary microvascular dysfunction among patients with chest pain and nonobstructive coronary artery disease. JACC Cardiovasc. Interv. 2015, 8, 1445–1453. [Google Scholar] [CrossRef]
- Lee, B.K.; Lim, H.S.; Fearon, W.F.; Yong, A.S.; Yamada, R.; Tanaka, S.; Lee, D.P.; Yeung, A.C.; Tremmel, J.A. Invasive evaluation of patients with angina in the absence of obstructive coronary artery disease. Circulation 2015, 131, 1054–1060. [Google Scholar] [CrossRef] [Green Version]
- Ford, T.J.; Stanley, B.; Good, R.; Rocchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; Robertson, K.; et al. Stratified medical therapy using invasive coronary function testing in angina: The CorMicA trial. J. Am. Coll. Cardiol. 2018, 72, 2841–2855. [Google Scholar] [CrossRef]
- Petraco, R.; van de Hoef, T.P.; Nijjer, S.; Sen, S.; van Lavieren, M.A.; Foale, R.A.; Meuwissen, M.; Broyd, C.; Echavarria-Pinto, M.; Foin, N.; et al. Baseline instantaneous wave-free ratio as a pressure-only estimation of underlying coronary flow reserve: Results of the JUSTIFY-CFR study (joined coronary pressure and flow analysis to determine diagnostic characteristics of basal and hyperemic indices of functional lesion severity-coronary flow reserve). Circ. Cardiovasc. Interv. 2014, 7, 492–502. [Google Scholar]
- Serruys, P.W.; Chichareon, P.; Modolo, R.; Leaman, D.M.; Reiber, J.H.C.; Emanuelsson, H.; Di Mario, C.; Pijls, N.H.J.; Morel, M.A.; Valgimigli, M.; et al. The SYNTAX score on its way out or towards artificial intelligence: Part I. EuroIntervention 2020, 16, 44–59. [Google Scholar] [CrossRef]
- Warisawa, T.; Cook, C.M.; Howard, J.P.; Ahmad, Y.; Doi, S.; Nakayama, M.; Goto, S.; Yakuta, Y.; Karube, K.; Shun-Shin, M.J.; et al. Physiological pattern of disease assessed by pressure-wire pullback has an influence on fractional flow reserve/instantaneous wave-free ratio discordance. Circ. Cardiovasc. Interv. 2019, 12, e007494. [Google Scholar] [CrossRef]
- Stegehuis, V.E.; Wijntjens, G.W.; Murai, T.; Piek, J.J.; van de Hoef, T.P. Assessing the haemodynamic impact of coronary artery stenoses: Intracoronary flow versus pressure measurements. Eur. Cardiol. 2018, 13, 46–53. [Google Scholar] [CrossRef]
- Barbato, E.; Aarnoudse, W.; Aengevaeren, W.R.; Werner, G.; Klauss, V.; Bojara, W.; Herzfeld, I.; Oldroyd, K.G.; Pijls, N.H.; de Bruyne, B. Validation of coronary flow reserve measurements by thermodilution in clinical practice. Eur. Heart J. 2004, 25, 219–223. [Google Scholar] [CrossRef] [Green Version]
- Everaars, H.; de Waard, G.A.; Driessen, R.S.; Danad, I.; van de Ven, P.M.; Raijmakers, P.G.; Lammertsma, A.A.; van Rossum, A.C.; Knaapen, P.; van Royen, N. Doppler flow velocity and thermodilution to assess coronary flow reserve: A head-to-head comparison with [15O]H2O PET. JACC Cardiovasc. Interv. 2018, 11, 2044–2054. [Google Scholar] [CrossRef]
- Williams, R.P.; de Waard, G.A.; de Silva, K.; Lumley, M.; Asrress, K.; Arri, S.; Ellis, H.; Mir, A.; Clapp, B.; Chiribiri, A.; et al. Doppler versus thermodilution-derived coronary microvascular resistance to predict coronary microvascular dysfunction in patients with acute myocardial infarction or stable angina pectoris. Am. J. Cardiol. 2018, 121, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.H.; Lee, J.M.; Park, J.; Choi, K.H.; Hwang, D.; Doh, J.H.; Nam, C.W.; Shin, E.S.; Hoshino, M.; Murai, T.; et al. Prognostic implications of resistive reserve ratio in patients with coronary artery disease. J. Am. Heart Assoc. 2020, 9, e015846. [Google Scholar] [CrossRef]
- Van de Hoef, T.P.; de Waard, G.A.; Meuwissen, M.; Voskuil, M.; Chamuleau, S.A.J.; van Royen, N.; Piek, J.J. Invasive coronary physiology: A Dutch tradition. Neth. Heart J. 2020, 28 (Suppl. S1), 99–107. [Google Scholar] [CrossRef]
- De Bruyne, B.; Pijls, N.H.J.; Gallinoro, E.; Candreva, A.; Fournier, S.; Keulards, D.C.J.; Sonck, J.; Van’t Veer, M.; Barbato, E.; Bartunek, J.; et al. Microvascular resistance reserve for assessment of coronary microvascular function: JACC technology corner. J. Am. Coll. Cardiol. 2021, 78, 1541–1549. [Google Scholar] [CrossRef]
- Gallinoro, E.; Candreva, A.; Colaiori, I.; Kodeboina, M.; Fournier, S.; Nelis, O.; di Gioia, G.; Sonck, J.; Van’t Veer, M.; Pijls, N.H.J.; et al. Thermodilution-derived volumetric resting coronary blood flow measurement in humans. EuroIntervention 2021, 17, e672–e679. [Google Scholar] [CrossRef]
- Härle, T.; Luz, M.; Meyer, S.; Kronberg, K.; Nickau, B.; Escaned, J.; Davies, J.; Elsässer, A. Effect of coronary anatomy and hydrostatic pressure on intracoronary indices of stenosis severity. JACC Cardiovasc. Interv. 2017, 10, 764–773. [Google Scholar] [CrossRef]
- Kawaguchi, Y.; Ito, K.; Kin, H.; Shirai, Y.; Okazaki, A.; Miyajima, K.; Watanabe, T.; Tatsuguchi, M.; Wakabayashi, Y.; Maekawa, Y. Impact of hydrostatic pressure variations caused by height differences in supine and prone positions on fractional flow reserve values in the coronary circulation. J. Interv. Cardiol. 2019, 2019, 4532862. [Google Scholar] [CrossRef]
- Üveges, Á.; Tar, B.; Jenei, C.; Czuriga, D.; Papp, Z.; Csanádi, Z.; Kőszegi, Z. The impact of hydrostatic pressure on the result of physiological measurements in various coronary segments. Int. J. Cardiovasc. Imaging 2021, 37, 5–14. [Google Scholar] [CrossRef]
- Tar, B.; Jenei, C.; Dezsi, C.A.; Bakk, S.; Beres, Z.; Santa, J.; Svab, M.; Szentes, V.; Polgar, P.; Bujaky, C.; et al. Less invasive fractional flow reserve measurement from 3-dimensional quantitative coronary angiography and classic fluid dynamic equations. EuroIntervention 2018, 14, 942–950. [Google Scholar] [CrossRef] [Green Version]
- Csippa, B.; Üveges, Á.; Gyürki, D.; Jenei, C.; Tar, B.; Bugarin-Horváth, B.; Szabó, G.T.; Komócsi, A.; Paál, G.; Kőszegi, Z. Simplified coronary flow reserve calculations based on three-dimensional coronary reconstruction and intracoronary pressure data. Cardiol. J. 2021. epub ahead of print. [Google Scholar] [CrossRef]
- Young, D.F.; Cholvin, N.R.; Roth, A.C. Pressure drop across artificially induced stenoses in the femoral arteries of dogs. Circ. Res. 1975, 36, 735–743. [Google Scholar] [CrossRef] [Green Version]
- Morris, P.D.; Ryan, D.; Morton, A.C.; Lycett, R.; Lawford, P.V.; Hose, D.R.; Gunn, J.P. Virtual fractional flow reserve from coronary angiography: Modeling the significance of coronary lesions: Results from the VIRTU-1 (VIRTUal fractional flow reserve from coronary angiography) study. JACC Cardiovasc. Interv. 2013, 6, 149–157. [Google Scholar] [CrossRef] [Green Version]
- Tu, S.; Barbato, E.; Köszegi, Z.; Yang, J.; Sun, Z.; Holm, N.R.; Tar, B.; Li, Y.; Rusinaru, D.; Wijns, W.; et al. Fractional flow reserve calculation from 3-dimensional quantitative coronary angiography and TIMI frame count: A fast computer model to quantify the functional significance of moderately obstructed coronary arteries. JACC Cardiovasc. Interv. 2014, 7, 768–777. [Google Scholar] [CrossRef] [Green Version]
- Kousera, C.A.; Nijjer, S.; Torii, R.; Petraco, R.; Sen, S.; Foin, N.; Hughes, A.D.; Francis, D.P.; Xu, X.Y.; Davies, J.E. Patient-specific coronary stenoses can be modeled using a combination of OCT and flow velocities to accurately predict hyperemic pressure gradients. IEEE Trans. Biomed. Eng. 2014, 61, 1902–1913. [Google Scholar] [CrossRef]
- Ahn, J.M.; Zimmermann, F.M.; Johnson, N.P.; Shin, E.S.; Koo, B.K.; Lee, P.H.; Park, D.W.; Kang, S.J.; Lee, S.W.; Kim, Y.H.; et al. Fractional flow reserve and pressure-bounded coronary flow reserve to predict outcomes in coronary artery disease. Eur. Heart J. 2017, 38, 1980–1989. [Google Scholar] [CrossRef]
- Zimmermann, F.M.; Pijls, N.H.J.; de Bruyne, B.; Bech, G.J.; van Schaardenburgh, P.; Kirkeeide, R.L.; Gould, K.L.; Johnson, N.P. What can intracoronary pressure measurements tell us about flow reserve? Pressure-bounded coronary flow reserve and an example application to the randomized DEFER trial. Catheter. Cardiovasc. Interv. 2017, 90, 917–925. [Google Scholar] [CrossRef]
- Wijntjens, G.W.M.; van Lavieren, M.A.; van de Hoef, T.P.; Echavarría-Pinto, M.; Meuwissen, M.; Stegehuis, V.E.; Murai, T.; Escaned, J.; Piek, J.J. Pressure-derived estimations of coronary flow reserve are inferior to flow-derived coronary flow reserve as diagnostic and risk stratification tools. Int. J. Cardiol. 2019, 279, 6–11. [Google Scholar] [CrossRef]
- Morris, P.D.; Gosling, R.; Zwierzak, I.; Evans, H.; Aubiniere-Robb, L.; Czechowicz, K.; Evans, P.C.; Hose, D.R.; Lawford, P.V.; Narracott, A.; et al. A novel method for measuring absolute coronary blood flow & microvascular resistance in patients with ischaemic heart disease. Cardiovasc. Res. 2020, 117, 1567–1577. [Google Scholar]
- Gosling, R.C.; Sturdy, J.; Morris, P.D.; Fossan, F.E.; Hellevik, L.R.; Lawford, P.; Hose, D.R.; Gunn, J. Effect of side branch flow upon physiological indices in coronary artery disease. J. Biomech. 2020, 103, 109698. [Google Scholar] [CrossRef]
- Johnson, N.P.; Oldroyd, K.G. Flow, pressure, anatomy: An eternal golden braid. Cardiovasc. Res. 2021, 117, 1426–1427. [Google Scholar] [CrossRef] [PubMed]
- Szabó, G.T.; Üveges, Á.; Tar, B.; Ágoston, A.; Dorj, A.; Jenei, C.; Kolozsvári, R.; Csippa, B.; Czuriga, D.; Kőszegi, Z. The holistic coronary physiology display: Calculation of the flow separation index in vessel-specific individual flow range during fractional flow reserve measurement using 3D coronary reconstruction. J. Clin. Med. 2021, 10, 1910. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient No. | Age | Gender | Target Vessel | Hypertension | DM | Dyslipidaemia | Hyperuricaemia | Chronic Renal Failure | Aorta Stenosis | DVT | CCS (prev) | PCI (prev) | PAD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 62 | f | RCA | √ | √ | χ | χ | χ | χ | √ | √ | √ | χ |
| 2 | 51 | m | CX | χ | χ | χ | χ | χ | χ | χ | √ | √ | χ |
| 3 | 60 | m | RCA | √ | χ | √ | χ | χ | √ | χ | √ | χ | √ |
| 4 | 66 | m | LAD | √ | χ | √ | χ | χ | χ | χ | √ | √ | χ |
| 5 | 65 | m | LAD | χ | √ | √ | χ | χ | χ | χ | √ | √ | χ |
| 6 | 55 | m | LAD | √ | χ | √ | χ | χ | χ | χ | √ | χ | χ |
| 7 | 64 | m | RCA | √ | χ | χ | χ | √ | χ | χ | √ | √ | χ |
| 8 | 55 | m | LAD | √ | √ | √ | χ | √ | χ | χ | √ | χ | χ |
| 9 | 69 | m | LAD | √ | √ | χ | χ | χ | χ | χ | √ | √ | χ |
| 10 | 43 | m | RCA | √ | χ | √ | √ | χ | χ | χ | √ | √ | χ |
| 11 | 56 | m | LAD | √ | √ | χ | χ | χ | χ | χ | √ | √ | χ |
| 12 | 52 | m | LAD | χ | χ | √ | χ | χ | χ | χ | √ | √ | χ |
| 13 | 66 | m | CX-OM | √ | √ | √ | χ | χ | χ | χ | √ | √ | √ |
| 14 | 60 | f | CX-OM | √ | √ | χ | χ | χ | χ | χ | √ | χ | χ |
| 15 | 63 | m | LAD | √ | χ | √ | χ | χ | χ | χ | √ | χ | χ |
| 16 | 66 | m | LAD | √ | √ | χ | √ | χ | √ | χ | √ | χ | χ |
| Case No. | Vessel Segment | Hydrostatic Pressure Difference (mmHg) ** | Pd/Pa Rest | FFR | CFRp-3D | CFRp-3D Corrected *** | APV-B (cm/s) | APV-P (cm/s) | CFR Doppler | RRRp-3D Corrected *** | RRRDoppler Corrected *** |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | RCA med | 0.46 | 0.99 | 0.94 | 3.55 | 2.72 | 14 | 42 | 3 | 3.12 | 3.43 |
| 2 | LCx dist | 1.99 | 0.98 | 0.92 | 3.47 | 2.21 | 19 | 45 | 2.4 | 2.67 | 2.86 |
| 3 | RCA med | 0.05 | 0.96 | 0.91 | 1.86 | 1.85 | 18 | 32 | 1.8 | 2.03 | 1.95 |
| 4 | LAD prox | −2.93 | 0.92 | 0.86 | 1.74 | 2.3 | 24 | 50 | 2.1 | 2.44 | 2.21 |
| 5 | LAD med | −2.5 | 0.86 | 0.63 | 1.58 | 1.7 | 14 | 29 | 2.1 | 2.68 | 3.26 |
| 6 | LAD prox | −0.69 | 0.79 | 0.64 | 1.24 | 1.25 | 32 | 42 | 1.3 | 1.81 | 1.91 |
| 7 * | RCA med | 0.76 | 0.92 | 0.79 | 2.21 | 2.1 | 15 | 30 | 2 | 2.39 | 2.27 |
| 8 | RCA med (post stent) | 0.77 | 0.98 | 0.94 | 2.68 | 2.2 | 15 | 33 | 2.2 | 2.29 | 2.3 |
| 9 | LAD prox | −0.71 | 0.93 | 0.79 | 1.65 | 1.71 | 19 | 36 | 1.9 | 2.58 | 2.86 |
| 10 | LAD med | −5.58 | 0.93 | 0.89 | 1.33 | 2.78 | 10 | 29 | 2.9 | 3.08 | 3.21 |
| 11 | RCA med | 1.05 | 0.98 | 0.9 | 3.01 | 2.33 | 36 | 86 | 2.4 | 2.44 | 2.5 |
| 12 * | LAD dist | −4.51 | 0.89 | 0.72 | 1.88 | 2.34 | 22 | 45 | 2.1 | 2.84 | 2.49 |
| 13 | LAD dist (post stent) | −3.93 | 0.93 | 0.85 | 1.72 | 2.46 | 22 | 55 | 2.5 | 2.89 | 2.93 |
| 14 | LAD prox | −3.65 | 0.79 | 0.53 | 1.74 | 1.9 | 38 | 46 | 1.2 | 2.67 | 1.7 |
| 15 | LCx dist (OM) | 2.6 | 0.62 | 0.54 | 1.09 | 1.08 | 33 | 36 | 1.1 | 1.27 | 1.27 |
| 16 | LCx dist (OM) | 1.84 | 0.98 | 0.91 | 3.46 | 2.27 | 26 | 62 | 2.4 | 2.68 | 2.81 |
| 17 | LAD prox | −5 | 0.89 | 0.79 | 1.74 | 2.31 | 15 | 31 | 2.1 | 2.64 | 2.37 |
| 18 * | LAD med | −6 | 0.74 | 0.62 | 1.21 | 1.3 | 31 | 43 | 1.4 | 1.59 | 1.7 |
| 19 | LAD med (post stent) | −6 | 0.87 | 0.76 | 1.69 | 2.74 | 24 | 57 | 2.4 | 3.37 | 2.92 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tar, B.; Ágoston, A.; Üveges, Á.; Szabó, G.T.; Szűk, T.; Komócsi, A.; Czuriga, D.; Csippa, B.; Paál, G.; Kőszegi, Z. Pressure- and 3D-Derived Coronary Flow Reserve with Hydrostatic Pressure Correction: Comparison with Intracoronary Doppler Measurements. J. Pers. Med. 2022, 12, 780. https://doi.org/10.3390/jpm12050780
Tar B, Ágoston A, Üveges Á, Szabó GT, Szűk T, Komócsi A, Czuriga D, Csippa B, Paál G, Kőszegi Z. Pressure- and 3D-Derived Coronary Flow Reserve with Hydrostatic Pressure Correction: Comparison with Intracoronary Doppler Measurements. Journal of Personalized Medicine. 2022; 12(5):780. https://doi.org/10.3390/jpm12050780
Chicago/Turabian StyleTar, Balázs, András Ágoston, Áron Üveges, Gábor Tamás Szabó, Tibor Szűk, András Komócsi, Dániel Czuriga, Benjamin Csippa, György Paál, and Zsolt Kőszegi. 2022. "Pressure- and 3D-Derived Coronary Flow Reserve with Hydrostatic Pressure Correction: Comparison with Intracoronary Doppler Measurements" Journal of Personalized Medicine 12, no. 5: 780. https://doi.org/10.3390/jpm12050780