
Psoas Muscle Volume as an Opportunistic Diagnostic Tool to Assess Sarcopenia in Patients with Hip Fractures: A Retrospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
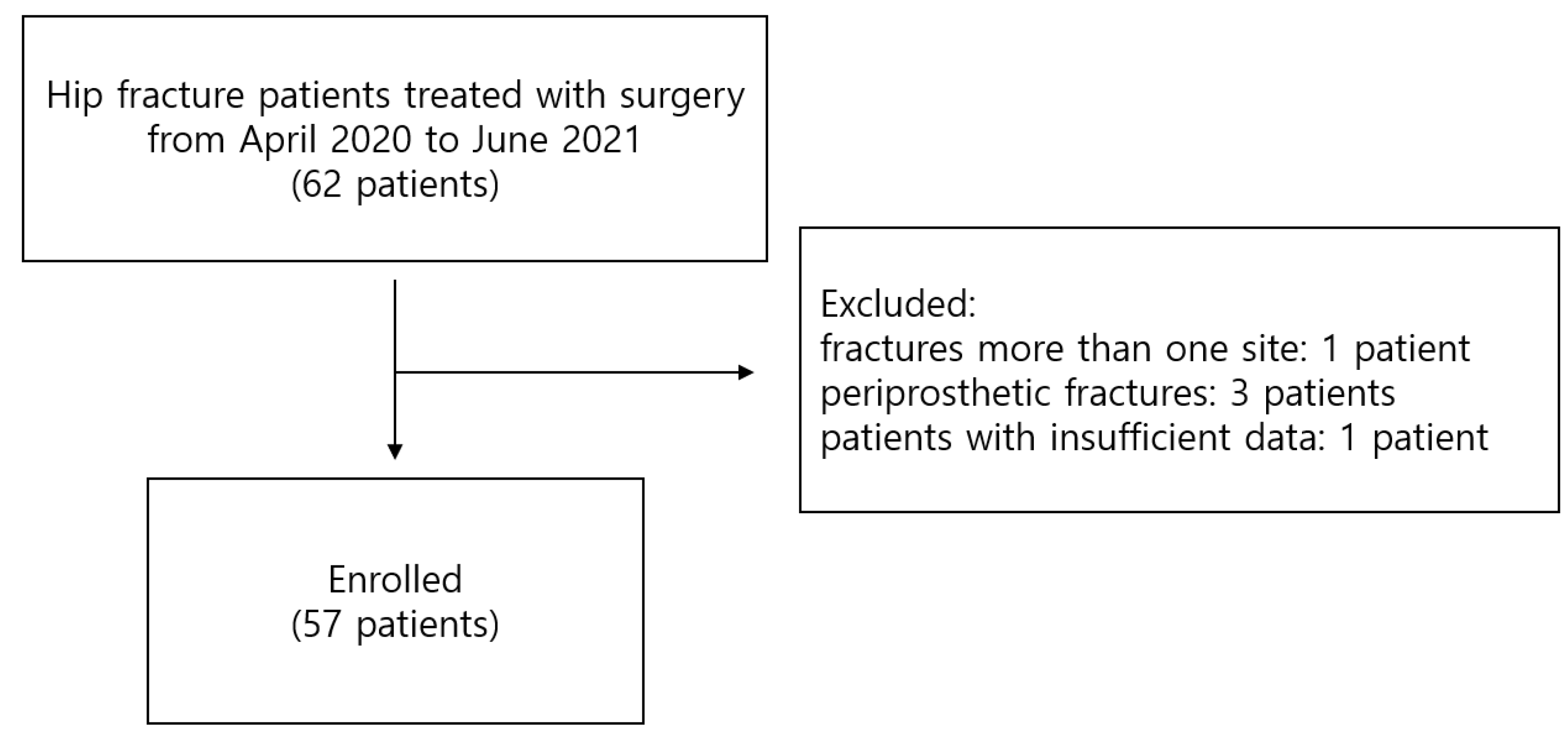
2.1. Study Design and Patient Selection
2.2. Data Collection
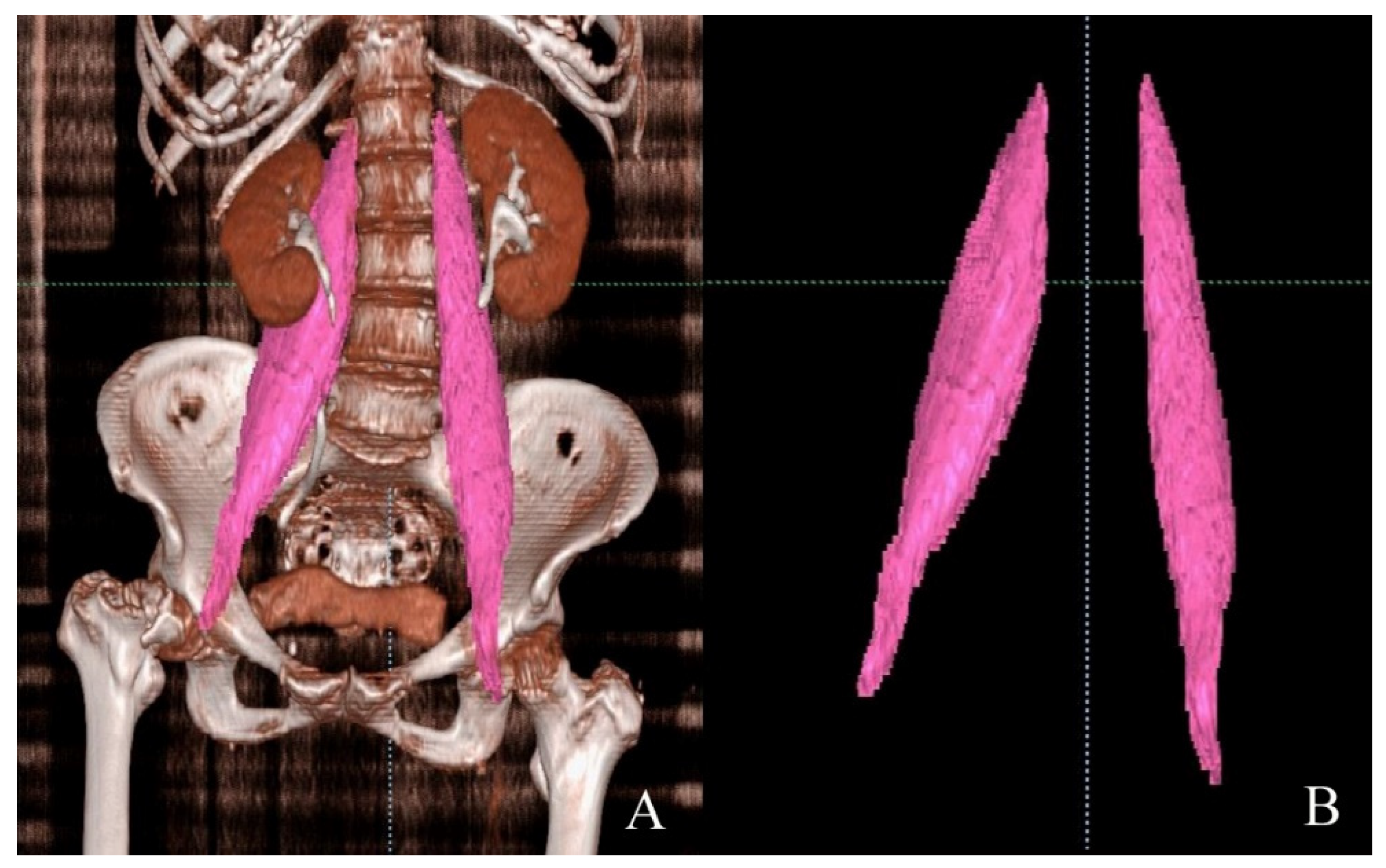
2.2.1. Psoas Muscle Segmentation and Volume Measurement
2.2.2. Measurement of Skeletal Muscle Mass and Handgrip Strength
2.3. Functional Outcomes
2.4. Statistical Analysis
3. Results
3.1. Demographic Variables
3.2. Comparisons of ASM between Psoas Muscle Area and Psoas Muscle Volume
3.3. Comparisons of HGS between Psoas Muscle Area and Psoas Muscle Volume
3.4. Functional Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Landi, F.; Calvani, R.; Ortolani, E.; Salini, S.; Martone, A.M.; Santoro, L.; Santoliquido, A.; Sisto, A.; Picca, A.; Marzetti, E. The association between sarcopenia and functional outcomes among older patients with hip fracture undergoing in-hospital rehabilitation. Osteoporos. Int. 2017, 28, 1569–1576. [Google Scholar] [CrossRef]
- Di Monaco, M.; Castiglioni, C.; De Toma, E.; Gardin, L.; Giordano, S.; Di Monaco, R.; Tappero, R. Presarcopenia and sarcopenia in hip-fracture women: Prevalence and association with ability to function in activities of daily living. Aging Clin. Exp. Res. 2015, 27, 465–472. [Google Scholar] [CrossRef]
- Steihaug, O.M.; Gjesdal, C.G.; Bogen, B.; Kristoffersen, M.H.; Lien, G.; Hufthammer, K.O.; Ranhoff, A.H. Does sarcopenia predict change in mobility after hip fracture? a multicenter observational study with one-year follow-up. BMC Geriatr. 2018, 18, 65. [Google Scholar] [CrossRef]
- Malafarina, V.; Malafarina, C.; Biain Ugarte, A.; Martinez, J.A.; Abete Goñi, I.; Zulet, M.A. Factors Associated with Sarcopenia and 7-Year Mortality in Very Old Patients with Hip Fracture Admitted to Rehabilitation Units: A Pragmatic Study. Nutrients 2019, 11, 2243. [Google Scholar] [CrossRef] [Green Version]
- Byun, S.E.; Kim, S.; Kim, K.H.; Ha, Y.C. Psoas cross-sectional area as a predictor of mortality and a diagnostic tool for sarcopenia in hip fracture patients. J. Bone Miner. Metab. 2019, 37, 871–879. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-P.; Wong, P.-K.; Tsai, M.-J.; Chang, W.-C.; Hsieh, T.-S.; Leu, T.-H.; Jeff Lin, C.-F.; Lee, C.-H.; Kuo, Y.-J.; Lin, C.-Y. The high prevalence of sarcopenia and its associated outcomes following hip surgery in Taiwanese geriatric patients with a hip fracture. J. Formos. Med. Assoc. 2020, 119, 1807–1816. [Google Scholar] [CrossRef]
- Inoue, T.; Maeda, K.; Nagano, A.; Shimizu, A.; Ueshima, J.; Murotani, K.; Sato, K.; Tsubaki, A. Undernutrition, Sarcopenia, and Frailty in Fragility Hip Fracture: Advanced Strategies for Improving Clinical Outcomes. Nutrients 2020, 12, 3743. [Google Scholar] [CrossRef]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef]
- van der Werf, A.; Langius, J.A.E.; de van der Schueren, M.A.E.; Nurmohamed, S.A.; van der Pant, K.; Blauwhoff-Buskermolen, S.; Wierdsma, N.J. Percentiles for skeletal muscle index, area and radiation attenuation based on computed tomography imaging in a healthy Caucasian population. Eur. J. Clin. Nutr. 2018, 72, 288–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derstine, B.A.; Holcombe, S.A.; Ross, B.E.; Wang, N.C.; Su, G.L.; Wang, S.C. Skeletal muscle cutoff values for sarcopenia diagnosis using T10 to L5 measurements in a healthy US population. Sci. Rep. 2018, 8, 11369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mourtzakis, M.; Prado, C.M.; Lieffers, J.R.; Reiman, T.; McCargar, L.J.; Baracos, V.E. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl. Physiol. Nutr. Metab. 2008, 33, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Kim, E.Y.; Kim, Y.S.; Park, I.; Ahn, H.K.; Cho, E.K.; Jeong, Y.M. Prognostic Significance of CT-Determined Sarcopenia in Patients with Small-Cell Lung Cancer. J. Thorac. Oncol. 2015, 10, 1795–1799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baracos, V.; Kazemi-Bajestani, S.M.R. Clinical outcomes related to muscle mass in humans with cancer and catabolic illnesses. Int. J. Biochem. Cell Biol. 2013, 45, 2302–2308. [Google Scholar] [CrossRef]
- Salminen, S.; Pihlajamäki, H.; Avikainen, V.; Kyrö, A.; Böstman, O. Specific features associated with femoral shaft fractures caused by low-energy trauma. J. Trauma 1997, 43, 117–122. [Google Scholar] [CrossRef]
- Clavien, P.A.; Sanabria, J.R.; Strasberg, S.M. Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery 1992, 111, 518–526. [Google Scholar]
- Koval, K.J.; Zuckerman, J.D. Functional recovery after fracture of the hip. J. Bone Jt. Surg. Am. 1994, 76, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. Pitfalls in the measurement of muscle mass: A need for a reference standard. J. Cachexia Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Masanés, F.; Rojano, I.L.X.; Salvà, A.; Serra-Rexach, J.A.; Artaza, I.; Formiga, F.; Cuesta, F.; López Soto, A.; Ruiz, D.; Cruz-Jentoft, A.J. Cut-off Points for Muscle Mass—Not Grip Strength or Gait Speed—Determine Variations in Sarcopenia Prevalence. J. Nutr. Health Aging 2017, 21, 825–829. [Google Scholar] [CrossRef] [PubMed]
- Hull, H.; He, Q.; Thornton, J.; Javed, F.; Allen, L.; Wang, J.; Pierson, R.N., Jr.; Gallagher, D. iDXA, Prodigy, and DPXL dual-energy X-ray absorptiometry whole-body scans: A cross-calibration study. J. Clin. Densitom. 2009, 12, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Sergi, G.; De Rui, M.; Veronese, N.; Bolzetta, F.; Berton, L.; Carraro, S.; Bano, G.; Coin, A.; Manzato, E.; Perissinotto, E. Assessing appendicular skeletal muscle mass with bioelectrical impedance analysis in free-living Caucasian older adults. Clin. Nutr. 2015, 34, 667–673. [Google Scholar] [CrossRef]
- Yu, S.C.; Powell, A.; Khow, K.S.; Visvanathan, R. The Performance of Five Bioelectrical Impedance Analysis Prediction Equations against Dual X-ray Absorptiometry in Estimating Appendicular Skeletal Muscle Mass in an Adult Australian Population. Nutrients 2016, 8, 189. [Google Scholar] [CrossRef] [Green Version]
- Amini, N.; Spolverato, G.; Gupta, R.; Margonis, G.A.; Kim, Y.; Wagner, D.; Rezaee, N.; Weiss, M.J.; Wolfgang, C.L.; Makary, M.M.; et al. Impact Total Psoas Volume on Short- and Long-Term Outcomes in Patients Undergoing Curative Resection for Pancreatic Adenocarcinoma: A New Tool to Assess Sarcopenia. J. Gastrointest. Surg. 2015, 19, 1593–1602. [Google Scholar] [CrossRef] [PubMed]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Beaudart, C.; McCloskey, E.; Bruyère, O.; Cesari, M.; Rolland, Y.; Rizzoli, R.; Araujo de Carvalho, I.; Amuthavalli Thiyagarajan, J.; Bautmans, I.; Bertiere, M.C.; et al. Sarcopenia in daily practice: Assessment and management. BMC Geriatr. 2016, 16, 170. [Google Scholar] [CrossRef]
- Kleczynski, P.; Tokarek, T.; Dziewierz, A.; Sorysz, D.; Bagienski, M.; Rzeszutko, L.; Dudek, D. Usefulness of Psoas Muscle Area and Volume and Frailty Scoring to Predict Outcomes After Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2018, 122, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Karvellas, C.J.; Baracos, V.; Williams, D.C.; Khadaroo, R.G.; Acute Care and Emergency Surgery (ACES) Group. Sarcopenia is a predictor of outcomes in very elderly patients undergoing emergency surgery. Surgery 2014, 156, 521–527. [Google Scholar] [CrossRef]
- Deren, M.E.; Babu, J.; Cohen, E.M.; Machan, J.; Born, C.T.; Hayda, R. Increased Mortality in Elderly Patients with Sarcopenia and Acetabular Fractures. J. Bone Jt. Surg. Am. 2017, 99, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.-K.; Lee, S.Y.; Beom, J.; Lim, J.-Y. Comparative outcomes of inpatient fragility fracture intensive rehabilitation management (FIRM) after hip fracture in sarcopenic and non-sarcopenic patients: A prospective observational study. Eur. Geriatr. Med. 2018, 9, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Jang, G.; Park, J.W.; Lee, Y.-K.; Koo, K.-H. Vitamin D Deficiency and Sarcopenia in Hip Fracture Patients. J. Bone Metab. 2021, 28, 79–83. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value (n = 57) |
|---|---|
| Mean age (y) | 79.5 (range, 59–93) |
| BMI (kg/m2) | 21.8 (95% CI, 20.8–22.7) |
| ASM (kg/m2) | 5.4 (95% CI, 5.1–5.7) |
| TPV1 (cc) | 173.2 (95% CI, 159.9–186.4) |
| TPV2 (cc/m) | 112.3 (95% CI, 104.2–120.4) |
| TPV3 (cc/m2) | 72.9 (95% CI, 67.8–78.0) |
| TPV4 (cc/m3) | 47.4 (95% CI, 44.1–50.8) |
| PA-L3 (mm2/m2) | 439.8 (95% CI, 402.2–477.3) |
| PA-L4 (mm2/m2) | 550.6 (95% CI, 514.1–587.1) |
| Volume | Cross-Sectional Area | |||||
|---|---|---|---|---|---|---|
| ASM (n = 57) | TPV1 | TPV2 | TPV3 | TPV4 | PA–L3 | PA–L4 |
| Correlation coefficient | 0.375 | 0.392 | 0.396 | 0.385 | 0.326 | 0.292 |
| p-value | <0.01 | <0.01 | <0.01 | <0.01 | 0.01 | 0.03 |
| Volume | Cross-Sectional Area | ||||||
|---|---|---|---|---|---|---|---|
| Handgrip Strength (n = 46) | ASM | TPV1 | TPV2 | TPV3 | TPV4 | PA–L3 | PA–L4 |
| Correlation coefficient | 0.316 | 0.320 | 0.333 | 0.336 | 0.327 | 0.071 | 0.228 |
| p-value | 0.03 | 0.03 | 0.02 | 0.02 | 0.03 | 0.64 | 0.13 |
| Grade of Complication (n = 57) | Length of Stay (n = 57) | ASA Grade (n = 57) | Koval Score (n = 57) | |||||
|---|---|---|---|---|---|---|---|---|
| Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | |
| ASM | −0.028 | 0.84 | −0.049 | 0.74 | 0.057 | 0.67 | −0.028 | 0.84 |
| TPV1 | −0.125 | 0.36 | −0.057 | 0.70 | −0.107 | 0.43 | −0.041 | 0.76 |
| TPV2 | −0.090 | 0.51 | −0.058 | 0.70 | −0.099 | 0.46 | −0.033 | 0.81 |
| TPV3 | −0.047 | 0.73 | −0.056 | 0.71 | −0.062 | 0.65 | −0.013 | 0.92 |
| TPV4 | −0.029 | 0.83 | −0.052 | 0.73 | −0.043 | 0.75 | 0.011 | 0.94 |
| PA-L3 | −0.043 | 0.75 | 0.034 | 0.82 | 0.032 | 0.81 | −0.091 | 0.50 |
| PA-L4 | −0.041 | 0.76 | 0.070 | 0.64 | 0.136 | 0.31 | −0.095 | 0.48 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
So, S.-P.; Lee, B.-S.; Kim, J.-W. Psoas Muscle Volume as an Opportunistic Diagnostic Tool to Assess Sarcopenia in Patients with Hip Fractures: A Retrospective Cohort Study. J. Pers. Med. 2021, 11, 1338. https://doi.org/10.3390/jpm11121338
So S-P, Lee B-S, Kim J-W. Psoas Muscle Volume as an Opportunistic Diagnostic Tool to Assess Sarcopenia in Patients with Hip Fractures: A Retrospective Cohort Study. Journal of Personalized Medicine. 2021; 11(12):1338. https://doi.org/10.3390/jpm11121338
Chicago/Turabian StyleSo, Sang-Pil, Bum-Sik Lee, and Ji-Wan Kim. 2021. "Psoas Muscle Volume as an Opportunistic Diagnostic Tool to Assess Sarcopenia in Patients with Hip Fractures: A Retrospective Cohort Study" Journal of Personalized Medicine 11, no. 12: 1338. https://doi.org/10.3390/jpm11121338