

Trichoderma spp.-Related Pneumonia: A Case Report in Heart–Lung Transplantation Recipient and a Systematic Literature Review
 , ,
, ,
Abstract
:1. Introduction
The Clinical Case
2. Materials and Methods
2.1. Research Approach
2.2. Eligibility Criteria and Information Sources
2.3. Search Strategy
- Pubmed: (“trichoderma”[MeSH Terms] OR “trichoderma”[All Fields] OR “trichodermas”[All Fields]) AND ((“human s”[All Fields] OR “humans”[MeSH Terms] OR “humans”[All Fields] OR “human”[All Fields]) AND (“infect”[All Fields] OR “infectability”[All Fields] OR “infectable”[All Fields] OR “infectant”[All Fields] OR “infectants”[All Fields] OR “infected”[All Fields] OR “infecteds”[All Fields] OR “infectibility”[All Fields] OR “infectible”[All Fields] OR “infecting”[All Fields] OR “infection s”[All Fields] OR “infections”[MeSH Terms] OR “infections”[All Fields] OR “infection”[All Fields] OR “infective”[All Fields] OR “infectiveness”[All Fields] OR “infectives”[All Fields] OR “infectivities”[All Fields] OR “infects”[All Fields] OR “pathogenicity”[MeSH Subheading] OR “pathogenicity”[All Fields] OR “infectivity”[All Fields]));
- Embase, Scopus, clinicaltrials.gov, and grey literature: (‘trichoderma’/exp OR trichoderma) AND (‘human infection’ OR ((‘human’/exp OR human) AND (‘infection’/exp OR infection))).
2.4. Selection and Data Collection Process
2.5. Data Collection Process and Data Synthesis
2.6. Risk of Bias Assessment
3. Results
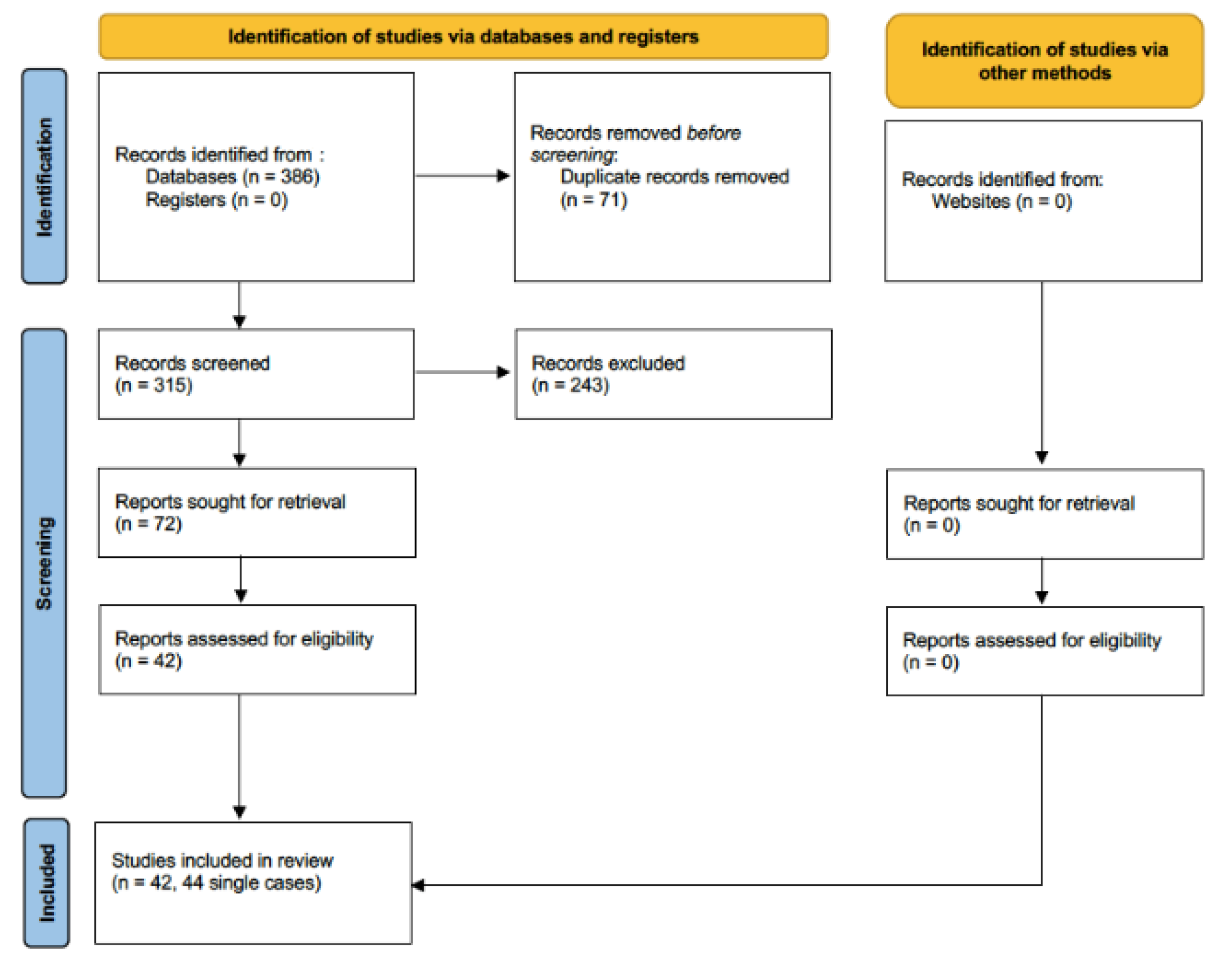
3.1. Search Results
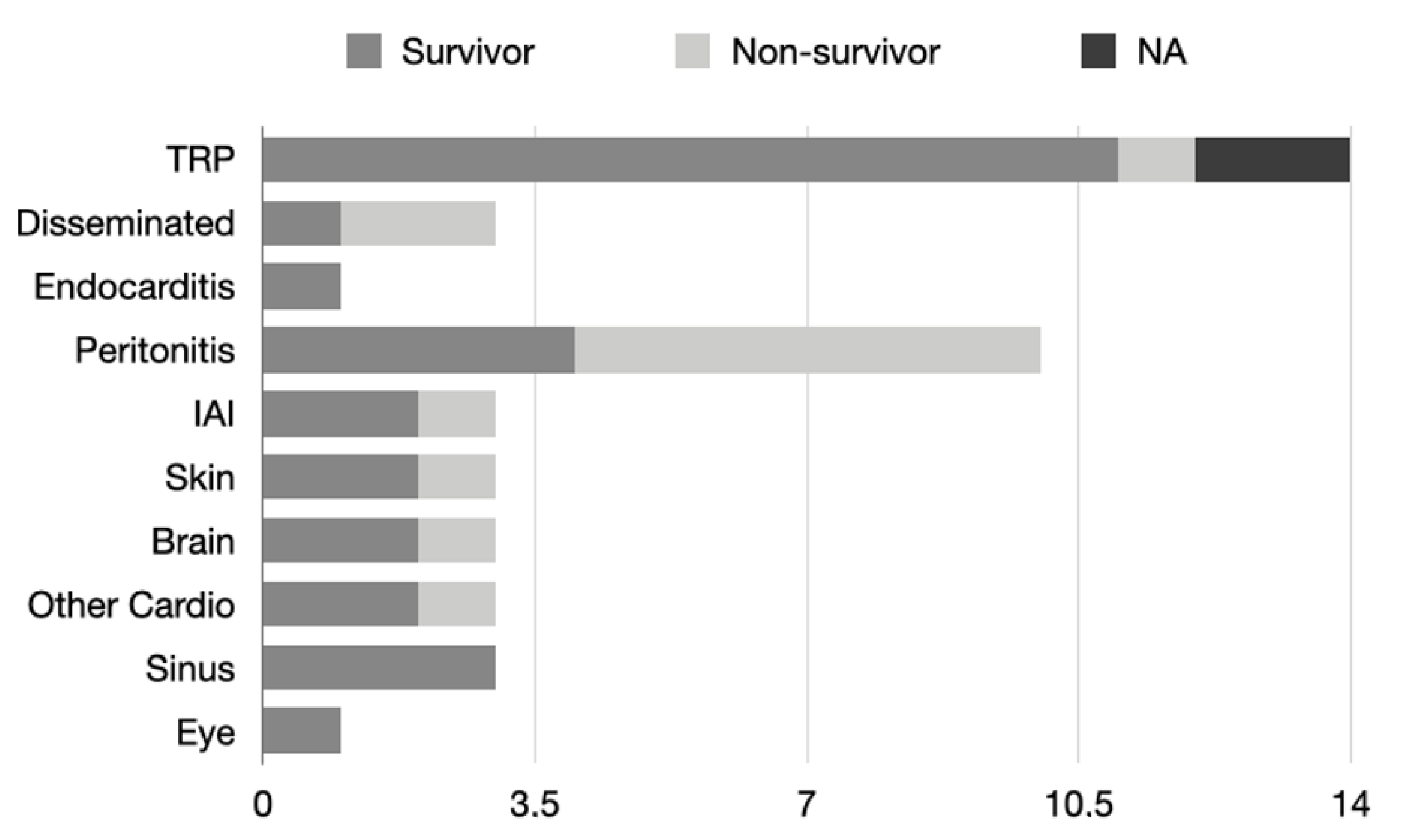
3.2. Trichoderma and the Related Disease
3.3. Diagnostic Tests and Antifungal Susceptibility Testing
3.4. Antifungal Management
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neofytos, D.; Fishman, J.A.; Horn, D.; Anaissie, E.; Chang, C.H.; Olyaei, A.; Pfaller, M.; Steinbach, W.J.; Webster, K.M.; Marr, K.A. Epidemiology and outcome of invasive fungal infections in solid organ transplant recipients. Transpl. Infect. Dis. 2010, 12, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.Z.P.; Schwartz, I.S. Emerging Fungal Infections: New Patients, New Patterns, and New Pathogens. J. Fungi 2019, 5, 67. [Google Scholar] [CrossRef] [PubMed]
- Dellière, S.; Rivero-Menendez, O.; Gautier, C.; Garcia-Hermoso, D.; Alastruey-Izquierdo, A.; Alanio, A. Emerging mould infections: Get prepared to meet unexpected fungi in your patient. Med. Mycol. 2020, 58, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Corcione, S.; Lupia, T.; Raviolo, S.; Montrucchio, G.; Trentalange, A.; Curtoni, A.; Cavallo, R.; De Rosa, F.G. Putative invasive pulmonary aspergillosis within medical wards and intensive care units: A 4-year retrospective, observational, single-centre study. Intern. Emerg. Med. 2021, 16, 1619–1627. [Google Scholar] [CrossRef] [PubMed]
- Martin-Loeches, I.; Antonelli, M.; Cuenca-Estrella, M.; Dimopoulos, G.; Einav, S.; De Waele, J.J.; Garnacho-Montero, J.; Kanj, S.S.; Machado, F.R.; Montravers, P.; et al. ESICM/ESCMID task force on practical management of invasive candidiasis in critically ill patients. Intensive Care Med. 2019, 45, 789–805. [Google Scholar] [CrossRef]
- Montrucchio, G.; Lupia, T.; Lombardo, D.; Stroffolini, G.; Corcione, S.; De Rosa, F.G.; Brazzi, L. Risk factors for invasive aspergillosis in ICU patients with COVID-19: Current insights and new key elements. Ann. Intensive Care 2021, 11, 136. [Google Scholar] [CrossRef]
- Timsit, J.F.; Sonneville, R.; Kalil, A.C.; Bassetti, M.; Ferrer, R.; Jaber, S.; Lanternier, F.; Luyt, C.E.; Machado, F.; Mikulska, M.; et al. Diagnostic and therapeutic approach to infectious diseases in solid organ transplant recipients. Intensive Care Med. 2019, 45, 573–591. [Google Scholar] [CrossRef]
- Johnson, M.D.; Lewis, R.E.; Ashley, E.S.D.; Ostrosky-Zeichner, L.; Zaoutis, T.; Thompson, G.R.; Andes, D.R.; Walsh, T.J.; Pappas, P.G.; Cornely, O.A.; et al. Core Recommendations for Antifungal Stewardship: A Statement of the Mycoses Study Group Education and Research Consortium. J. Infect. Dis. 2020, 222, S175–S198. [Google Scholar] [CrossRef]
- De Rosa, F.G.; Corcione, S.; Montrucchio, G.; Brazzi, L.; Di Perri, G. Antifungal Treatment Strategies in the ICU: Beyond Meta-analysis. Turk. J. Anaesthesiol. Reanim. 2016, 44, 283–284. [Google Scholar] [CrossRef]
- Martin-Loeches, I.; Nseir, S.; Rodriguez, A.; Azoulay, E. Disease-specific gaps within fungal respiratory tract infections: Clinical features, diagnosis, and management in critically ill patients. Curr. Opin. Pulm. Med. 2022, 28, 218–224. [Google Scholar] [CrossRef]
- Anesi, J.A.; Baddley, J.W. Approach to the Solid Organ Transplant Patient with Suspected Fungal Infection. Infect. Dis. Clin. N. Am. 2016, 30, 277–296. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Guarner, J. Emerging and reemerging fungal infections. Semin. Diagn. Pathol. 2019, 36, 177–181. [Google Scholar] [CrossRef]
- Harman, G.E.; Howell, C.R.; Viterbo, A.; Chet, I.; Lorito, M. Trichoderma species—Opportunistic, avirulent plant symbionts. Nat. Rev. Microbiol. 2004, 2, 43–56. [Google Scholar] [CrossRef]
- Sandoval-Denis, M.; Sutton, D.A.; Cano-Lira, J.F.; Gené, J.; Fothergill, A.W.; Wiederhold, N.P.; Guarro, J. Phylogeny of the clinically relevant species of the emerging fungus Trichoderma and their antifungal susceptibilities. J. Clin. Microbiol. 2014, 52, 2112–2125. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Robertson, M.H. Fungi in fluids—A hazard of intravenous therapy. J. Med. Microbiol. 1970, 3, 99–102. [Google Scholar] [CrossRef]
- Gil, M.R.E.; Corral, E.P.; Muñóz, R.M. Pulmonary mycoma cause by Trichoderma viride. Actas Dermosifiliogr. 1976, 67, 673–680. [Google Scholar]
- Loeppky, C.B.; Sprouse, R.F.; Carlson, J.V.; Everett, E.D. Trichoderma viride peritonitis. South. Med. J. 1983, 76, 798–799. [Google Scholar] [CrossRef]
- Ragnaud, J.M.; Marceau, C.; Roche-Bezian, M.C.; Wone, C. Trichoderma koningii peritonitis in continuous ambulatory peritoneal dialysis. Med. Mal. Infect. 1984, 14, 402–405. [Google Scholar] [CrossRef]
- Jacobs, F.; Byl, B.; Bourgeois, N.; Coremans-Pelseneer, J.; Florquin, S.; Depré, G.; Van de Stadt, J.; Adler, M.; Gelin, M.; Thys, J.P. Trichoderma viride infection in a liver transplant recipient. Mycoses 1992, 35, 301–303. [Google Scholar] [CrossRef]
- Imokawa, S.; Sato, A.; Taniguchi, M.; Imamura, M.; Shirai, T.; Suda, T.; Iwata, M.; Gemma, H. Two cases of acute eosinophilic pneumonia with precipitating antibody against Trichosporon cutaneum and Trichoderma viride. Nihon Kyobu Shikkan Gakkai Zasshi 1993, 31, 352–359. [Google Scholar] [PubMed]
- Tanis, B.C.; van der Pijl, H.; van Ogtrop, M.L.; Kibbelaar, R.E.; Chang, P.C. Fatal fungal peritonitis by Trichoderma longibrachiatum complicating peritoneal dialysis. Nephrol. Dial. Transpl. 1995, 10, 114–116. [Google Scholar]
- Gautheret, A.; Dromer, F.; Bourhis, J.H.; Andremont, A. Trichoderma pseudokoningii as a cause of fatal infection in a bone marrow transplant recipient. Clin. Infect. Dis. 1995, 20, 1063–1064. [Google Scholar] [CrossRef] [PubMed]
- Seguin, P.; Degeilh, B.; Grulois, I.; Gacouin, A.; Maugendre, S.; Dufour, T.; Dupont, B.; Camus, C. Successful treatment of a brain abscess due to Trichoderma longibrachiatum after surgical resection. Eur. J. Clin. Microbiol. Infect. Dis. 1995, 14, 445–448. [Google Scholar] [CrossRef]
- Kawaguchi, H.; Yasuba, H.; Yamashita, K.; Fukuma, H.; Misaki, K.; Sumitomo, S.; Kato, M.; Chihara, J. A case of acute eosinophilic pneumonia: Bronchoalveolar lavage findings before and after steroid treatment. Jpn. J. Thorac. Dis. 1995, 33, 738–744. [Google Scholar]
- Guiserix, J.; Ramdane, M.; Finielz, P.; Michault, A.; Rajaonarivelo, P. Trichoderma harzianum peritonitis in peritoneal dialysis. Nephron 1996, 74, 473–474. [Google Scholar] [CrossRef]
- Campos-Herrero, M.I.; Bordes, A.; Perera, A.; Ruiz, M.C.; Fernandez, A. Trichodermia koningii peritonitis in a patient undergoing peritoneal dialysis. Clin. Microbiol. Newsl. 1996, 18, 150–152. [Google Scholar] [CrossRef]
- Munoz, F.M.; Demmler, G.J.; Travis, W.R.; Ogden, A.K.; Rossmann, S.N.; Rinaldi, M.G. Trichoderma longibrachiatum infection in a pediatric patient with aplastic anemia. J. Clin. Microbiol. 1997, 35, 499–503. [Google Scholar] [CrossRef]
- Bren, A. Fungal peritonitis in patients on continuous ambulatory peritoneal dialysis. Eur. J. Clin. Microbiol. Infect. Dis. 1998, 17, 839–843. [Google Scholar] [CrossRef]
- Furukawa, H.; Kusne, S.; Sutton, D.A.; Manez, R.; Carrau, R.; Nichols, L.; Abu-Elmagd, K.; Skedros, D.; Todo, S.; Rinaldi, M.G. Acute invasive sinusitis due to Trichoderma longibrachiatum in a liver and small bowel transplant recipient. Clin. Infect. Dis. 1998, 26, 487–489. [Google Scholar] [CrossRef]
- Richter, S.; Cormican, M.G.; Pfaller, M.A.; Lee, C.K.; Gingrich, R.; Rinaldi, M.G.; Sutton, D.A. Fatal disseminated Trichoderma longibrachiatum infection in an adult bone marrow transplant patient: Species identification and review of the literature. J. Clin. Microbiol. 1999, 37, 1154–1160. [Google Scholar] [CrossRef]
- Guarro, J.; Antolín-Ayala, M.I.; Gené, J.; Gutiérrez-Calzada, J.; Nieves-Díez, C.; Ortoneda, M. Fatal case of Trichoderma harzianum infection in a renal transplant recipient. J. Clin. Microbiol. 1999, 37, 3751–3755. [Google Scholar] [CrossRef]
- Rota, S.; Marchesi, D.; Farina, C.; de Bièvre, C. Trichoderma pseudokoningii peritonitis in automated peritoneal dialysis patient successfully treated by early catheter removal. Perit. Dial. Int. 2000, 20, 91–93. [Google Scholar] [CrossRef]
- Bustamante-Labarta, M.H.; Caramutti, V.; Allende, G.N.; Weinschelbaum, E.; Torino, A.F. Unsuspected embolic fungal endocarditis of an aortic conduit diagnosed by transesophageal echocardiography. J. Am. Soc. Echocardiogr. 2000, 13, 953–954. [Google Scholar] [CrossRef]
- Amato, J.G.; Amato, V.S.; Neto, V.A.; Heins-Vaccari, E.M. An AIDS patient with Trichoderma. Rev. Soc. Bras. Med. Trop. 2002, 35, 269. [Google Scholar] [CrossRef]
- Chouaki, T.; Lavarde, V.; Lachaud, L.; Raccurt, C.P.; Hennequin, C. Invasive infections due to Trichoderma species: Report of 2 cases, findings of in vitro susceptibility testing, and review of the literature. Clin. Infect. Dis. 2002, 35, 1360–1367. [Google Scholar] [CrossRef]
- Myoken, Y.; Sugata, T.; Fujita, Y.; Asaoku, H.; Fujihara, M.; Mikami, Y. Fatal necrotizing stomatitis due to Trichoderma longibrachiatum in a neutropenic patient with malignant lymphoma: A case report. Int. J. Oral Maxillofac. Surg. 2002, 31, 688–691. [Google Scholar] [CrossRef]
- Eşel, D.; Koç, A.N.; Utaş, C.; Karaca, N.; Bozdemir, N. Fatal peritonitis due to Trichoderma sp. in a patient undergoing continuous ambulatory peritoneal dialysis. Mycoses 2003, 46, 71–73. [Google Scholar] [CrossRef]
- De Miguel, D.; Gómez, P.; González, R.; García-Suárez, J.; Cuadros, J.A.; Bañas, M.H.; Romanyk, J.; Burgaleta, C. Nonfatal pulmonary Trichoderma viride infection in an adult patient with acute myeloid leukemia: Report of one case and review of the literature. Diagn. Microbiol. Infect. Dis. 2005, 53, 33–37. [Google Scholar] [CrossRef]
- Alanio, A.; Brethon, B.; de Chauvin, M.F.; de Kerviler, E.; Leblanc, T.; Lacroix, C.; Baruchel, A.; Menotti, J. Invasive pulmonary infection due to Trichoderma longibrachiatum mimicking invasive Aspergillosis in a neutropenic patient successfully treated with voriconazole combined with caspofungin. Clin. Infect. Dis. 2008, 46, e116–e118. [Google Scholar] [CrossRef]
- Kviliute, R.; Paskevicius, A.; Gulbinovic, J.; Stulpinas, R.; Griskevicius, L. Nonfatal Trichoderma citrinoviride pneumonia in an acute myeloid leukemia patient. Ann. Hematol. 2008, 87, 501–502. [Google Scholar] [CrossRef] [PubMed]
- Lagrange-Xélot, M.; Schlemmer, F.; Gallien, S.; Lacroix, C.; Molina, J.M. Trichoderma fungaemia in a neutropenic patient with pulmonary cancer and human immunodeficiency virus infection. Clin. Microbiol. Infect. 2008, 14, 1190–1192. [Google Scholar] [CrossRef] [PubMed]
- Trabelsi, S.; Hariga, D.; Khaled, S. First case of Trichoderma longibrachiatum infection in a renal transplant recipient in Tunisia and review of the literature. Tunis. Med. 2010, 88, 52–57. [Google Scholar] [PubMed]
- Salas, C.F.S.; Joshi, A.Y.; Dhiman, N.; Banerjee, R.; Huskins, W.C.; Wengenack, N.L.; Henry, N.K. Fatal post-operative Trichoderma longibrachiatum mediastinitis and peritonitis in a paediatric patient with complex congenital cardiac disease on peritoneal dialysis. J. Med. Microbiol. 2011, 60, 1869–1871. [Google Scholar] [CrossRef] [PubMed]
- Peralta, L.I.R.; Vera, M.R.M.; Delgado, M.J.G.; de la Cruz, A.J.P. Endocarditis caused by Trichoderma longibrachiatumin a patient receiving home parenteral nutrition. Nutr. Hosp. 2013, 28, 961–964. [Google Scholar] [CrossRef]
- Molnár-Gábor, E.; Dóczi, I.; Hatvani, L.; Vágvölgyi, C.; Kredics, L. Isolated sinusitis sphenoidalis caused by Trichoderma longibrachiatum in an immunocompetent patient with headache. J. Med. Microbiol. 2013, 62, 1249–1252. [Google Scholar] [CrossRef]
- Festuccia, M.; Giaccone, L.; Gay, F.; Brunello, L.; Maffini, E.; Ferrando, F.; Talamo, E.; Boccadoro, M.; Serra, R.; Barbui, A.; et al. Trichoderma species fungemia after high-dose chemotherapy and autologous stem cell transplantation: A case report. Transpl. Infect. Dis. 2014, 16, 653–657. [Google Scholar] [CrossRef]
- Tascini, C.; Cardinali, G.; Barletta, V.; Di Paolo, A.; Leonildi, A.; Zucchelli, G.; Corte, L.; Colabella, C.; Roscini, L.; Consorte, A.; et al. First Case of Trichoderma longibrachiatum CIED (Cardiac Implantable Electronic Device)-Associated Endocarditis in a Non-immunocompromised Host: Biofilm Removal and Diagnostic Problems in the Light of the Current Literature. Mycopathologia 2016, 181, 297–303. [Google Scholar] [CrossRef]
- Akagi, T.; Kawamura, C.; Terasawa, N.; Yamaguchi, K.; Kubo, K. Suspected Pulmonary Infection with Trichoderma longibrachiatum after Allogeneic Stem Cell Transplantation. Intern. Med. 2017, 56, 215–219. [Google Scholar] [CrossRef]
- Carlson, J.; Staiano, P.P.; James, L.R. A rare presentation of an unusual fungus: Trichoderma peritonitis. J. Am. Soc. Nephrol. 2018, 29, 586. [Google Scholar]
- Román-Soto, S.; Álvarez-Rojas, E.; García-Rodríguez, J. Skin infection due to Trichoderma longibrachiatum in a haematological paediatric patient. Clin. Microbiol. Infect. 2019, 25, 1383–1384. [Google Scholar] [CrossRef]
- Sautour, M.; Chrétien, M.L.; Valot, S.; Lafon, I.; Basmaciyan, L.; Legouge, C.; Verrier, T.; Gonssaud, B.; Abou-Hanna, H.; Dalle, F.; et al. First case of proven invasive pulmonary infection due to Trichoderma longibrachiatum in a neutropenic patient with acute leukemia. J. Mycol. Med. 2018, 28, 659–662. [Google Scholar] [CrossRef]
- Recio, R.; Meléndez-Carmona, M.; Martín-Higuera, M.C.; Pérez, V.; López, E.; López-Medrano, F.; Pérez-Ayala, A. Trichoderma longibrachiatum: An unusual pathogen of fungal pericarditis. Clin. Microbiol. Infect. 2019, 25, 586–587. [Google Scholar] [CrossRef]
- Bachu, R.; Hemmings, S.C.; Siddamreddy, S. A rare case of Trichoderma-related peritonitis in a patient on peritoneal dialysis. J. Am. Soc. Nephrol. 2020, 31, 424. [Google Scholar] [CrossRef]
- Zhou, Y.B.; Zhang, G.J.; Song, Y.G.; Sun, L.N.; Chen, Y.H.; Sun, T.T.; Li, R.Y.; Liu, W.; Li, D.M. Application of laser capture microdissection and polymerase chain reaction in the diagnosis of Trichoderma longibrachiatum infection: A promising diagnostic tool for ‘fungal contaminants’ infection. Med. Mycol. 2020, 58, 315–321. [Google Scholar] [CrossRef]
- Georgakopoulou, V.E.; Melemeni, D.; Mantzouranis, K.; Damaskos, C.; Gkoufa, A.; Chlapoutakis, S.; Garmpis, N.; Garmpi, A.; Sklapani, P.; Trakas, N.; et al. Firstcase of pneumonia-parapneumonic effusion due to Trichoderma longibrachiatum. IDCases 2021, 25, e01239. [Google Scholar] [CrossRef]
- Al-Shehri, A.; Aljohani, S.; Semidey, V.A. Bilateral endogenous Trichoderma endophthalmitis in an immunocompromised host. Am. J. Ophthalmol. Case Rep. 2021, 24, 101234. [Google Scholar] [CrossRef]
- Fisher, M.C.; Hawkins, N.J.; Sanglard, D.; Gurr, S.J. Worldwide emergence of resistance to antifungal drugs challenges human health and food security. Science 2018, 360, 739–742. [Google Scholar] [CrossRef]
- Lamoth, F.; Kontoyiannis, D.P. Therapeutic Challenges of Non-Aspergillus Invasive Mold Infections in Immunosuppressed Patients. Antimicrob. Agents Chemother. 2019, 63, e01244-19. [Google Scholar] [CrossRef]
- Shoham, S. Emerging fungal infections in solid organ transplant recipients. Infect. Dis. Clin. N. Am. 2013, 27, 305–316. [Google Scholar] [CrossRef]
- Husain, S.; Camargo, J.F. Invasive Aspergillosis in solid-organ transplant recipients: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13544. [Google Scholar] [CrossRef] [PubMed]
- Ascioglu, S.; Rex, J.H.; de Pauw, B.; Bennett, J.E.; Bille, J.; Crokaert, F.; Denning, D.W.; Donnelly, J.P.; Edwards, J.E.; Erjavec, Z.; et al. Defining opportunistic invasive fungal infections in immunocompromised patients with cancer and hematopoietic stem cell transplants: An international consensus. Clin. Infect. Dis. 2002, 34, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Giacobbe, D.R.; Cortegiani, A.; Karaiskos, I.; Mercier, T.; Tejada, S.; Peghin, M.; Grecchi, C.; Rebuffi, C.; Asperges, E.; Zuccaro, V.; et al. Performance of Existing Definitions and Tests for the Diagnosis of Invasive Fungal Diseases other than Invasive Candidiasis and Invasive Aspergillosis in Critically Ill, Adult Patients: A Systematic Review with Qualitative Evidence Synthesis. J. Fungi 2021, 7, 176. [Google Scholar] [CrossRef] [PubMed]
- Cornely, O.A.; Arikan-Akdagli, S.; Dannaoui, E.; Groll, A.H.; Lagrou, K.; Chakrabarti, A.; Lanternier, F.; Pagano, L.; Skiada, A.; Akova, M.; et al. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of mucormycosis 2013. Clin. Microbiol. Infect. 2014, 20 (Suppl. S3), 5–26. [Google Scholar] [CrossRef] [Green Version]
- Tortorano, A.M.; Richardson, M.; Roilides, E.; van Diepeningen, A.; Caira, M.; Munoz, P.; Johnson, E.; Meletiadis, J.; Pana, Z.D.; Lackner, M.; et al. ESCMID and ECMM joint guidelines on diagnosis and management of hyalohyphomycosis: Fusarium spp., Scedosporium spp. and others. Clin. Microbiol. Infect. 2014, 20 (Suppl. S3), 27–46. [Google Scholar] [CrossRef]
- Kidd, S.E.; Crawford, L.C.; Halliday, C.L. Antifungal Susceptibility Testing and Identification. Infect. Dis. Clin. N. Am. 2021, 35, 313–339. [Google Scholar] [CrossRef]
- Husain, B.; Kirchberger, M.C.; Erdmann, M.; Schüpferling, S.; Abolhassani, A.R.; Fröhlich, W.; Berking, C.; Heinzerling, L. Inflammatory markers in autoimmunity induced by checkpoint inhibitors. J. Cancer Res. Clin. Oncol. 2021, 147, 1623–1630. [Google Scholar] [CrossRef]
- Ashbee, H.R.; Barnes, R.A.; Johnson, E.M.; Richardson, M.D.; Gorton, R.; Hope, W.W. Therapeutic drug monitoring (TDM) of antifungal agents: Guidelines from the British Society for Medical Mycology. J. Antimicrob. Chemother. 2014, 69, 1162–1176. [Google Scholar] [CrossRef]
- Lamoth, F.; Lewis, R.E.; Kontoyiannis, D.P. Role and Interpretation of Antifungal Susceptibility Testing for the Management of Invasive Fungal Infections. J. Fungi 2020, 7, 17. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author | Year | Country | Fungal Species | Main Pathology | Clinical Manifestation | Treatment of Choice | Outcome |
|---|---|---|---|---|---|---|---|
| Robertson et al. [16] | 1969 | UK | Trichoderma spp. | Disseminated | AmB | Infection resolution | |
| Escudero Gil et al. [17] | 1976 | Spain | T. viride | Acute myeloid leukemia | Pulmonary infection | Surgery | Infection resolution |
| Escudero Gil et al. [17] | 1976 | Spain | T. viride | Acute myeloid leukemia | Pulmonary infection | AmB + VOR + CASP | Infection resolution |
| Loeppky et al. [18] | 1983 | USA | T. viride | Renal failure secondary to amyloidosis | Peritonitis | Peritoneal catheter removal + AmB | Infection resolution |
| Ragnaud et al. [19] | 1984 | France | T. koningii | CAPD | Peritonitis | Peritoneal catheter removal + miconazole | Infection resolution |
| Jacobs et al. [20] | 1992 | Belgium | T. viride | Liver transplantation | Perihepatic hematoma and peritoneal fluid | AmB + FLU | Death |
| Imokawa et al. [21] | 1993 | Japan | Trichoderma spp. | Not stated | Pulmonary infection | NK | NK |
| Tanis et al. [22] | 1995 | The Netherlands | T. longibrachiatum | Renal transplantation | Peritonitis | AmB | Death |
| Gautheret et al. [23] | 1995 | France | T. pseudokoningii | Bone marow transplantation | Disseminated | AmB + 5-FC | Death |
| Seguin et al. [24] | 1995 | France | T. longibrachiatum | Leukemia | Brain abscess | AmB, ITR + surgery | Infection resolution |
| Kawaguchi et al. [25] | 1995 | Japan | T. viride | Pulmonary infection | NK | NK | |
| Guiserix et al. [26] | 1996 | France | T. harzianum | CAPD | Peritonitis | Peritoneal catheter removal + KET | Death |
| Campos-Herrero et al. [27] | 1996 | Spain | T. koningii | CAPD | Peritonitis | KET | Death |
| Munoz et al. [28] | 1997 | USA | T. longibrachiatum | Aplastic anemia | Skin infection | AmB | Infection resolution |
| Bren et al. [29] | 1998 | Slovenia | Trichoderma spp. | End-stage renal failure and CAPD | Peritonitis | KET | Infection resolution |
| Furukawa et al. [30] | 1998 | USA | T. longibrachiatum | Small-bowel and liver transplantation | Invasive sinusitis | AmB + ITR, surgery | Infection resolution |
| Richter et al. [31] | 1999 | USA | T. longibrachiatum | Allo-HSCT | Disseminated | AmB, ITR | Death |
| Guarro et al. [32] | 1999 | Spain | T. harzianum | Renal transplantation | Brain abscess | None | Death |
| Rota et al. [33] | 2000 | Italy | T. pseudokoningii | CAPD | Peritonitis | Peritoneal catheter removal + AmB | Infection resolution |
| Bustamante-Labarta et al. [34] | 2000 | Argentina | Trichoderma spp. | Aorta surgery | Endocarditis | Antifungal, graft replaced | Infection resolution |
| Amato et al. [35] | 2002 | Portugal | Trichoderma spp. | AIDS | Encephalitis | AmB | Infection resolution |
| Chouaki et al. [36] | 2002 | France | T. longibrachiatum | Liver transplantation | Perihepatic hematoma | Surgery | Infection resolution |
| Chouaki et al. [36] | 2002 | France | T. longibrachiatum | Lung transplantation | Pulmonary infection | Amb | Death |
| Myoken et al. [37] | 2002 | Japan | T. longibrachiatum | Lymphoma | Necrotizing stomatitis | AmB, ITR | Death |
| Esel et al. [38] | 2003 | Turkey | Trichoderma spp. | CAPD | peritonitis | AmB | Death |
| De Miguel et al. [39] | 2005 | Spain | T. viride | Acute myeloid leukemia | Pulmonary infection | AmB and VOR | Infection resolution |
| Alanio et al. [40] | 2008 | France | T. longibrachiatum | Hematologic malignancy | Pulmonary infection | VOR and CASP | Infection resolution |
| Kviliute et al. [41] | 2008 | Lithuania | T. citrinoviride | Acute myeloid leukemia | Pulmonary infection | AmB | Infection resolution |
| Lagrange-Xélot et al. [42] | 2008 | France | Trichoderma longibrachiatum | AIDS | Pulmonary infection | AmB and VOR | Infection resolution |
| Trabelsi et al. [43] | 2010 | Tunisia | Trichoderma spp. | Renal transplantation | Skin abscess and intertrigo | VOR | Infection resolution |
| Santillan Salas et al. [44] | 2011 | USA | T. longibrachiatum | Cardiac pediatric surgery | Mediastinitis and peritonitis | CASP and subsequently VOR and intraperitoneal AmB | Infection resolution |
| Rodríguez Peralta et al. [45] | 2013 | Spain | T. longibrachiatum | Home parenteral nutrition patient | Endocarditis | CASP | Infection resolution |
| Molnár-Gábor et al. [46] | 2013 | Hungary | T. longibrachiatum | Immunocompetent patient | Sinusitis | Topical AmB + surgical debridement | Infection resolution |
| Festuccia et al. [47] | 2014 | Italy | Trichoderma spp. | Auto-HSCT | Pulmonary infection | VOR | Infection resolution |
| Tascini et al. [48] | 2016 | Italy | T. longibrachiatum | ICD implantation complicated by PNX | Endocarditis | VOR and subsequently AmB | Infection resolution |
| Akagi et al. [49] | 2017 | Japan | T. longibrachiatum | Aplastic anemia | Pulmonary infection | AmB | Infection resolution |
| Carlson et al. [50] | 2018 | USA | Trichoderma spp. | Capd | Peritonitis | AmB and VOR | Infection resolution |
| Román-Soto et al. [51] | 2019 | Spain | T. longibrachiatum | Allo-HSCT | Necrotic ulcers | VOR, CASP + ulcer debridment | Infection resolution |
| Sautour et al. [52] | 2019 | France | T. longibrachiatum | Acute myeloid leukemia | Pulmonary infection | VOR + CASP | Infection resolution |
| Recio et al. [53] | 2019 | Spain | T. longibrachiatum | Pericardiectomy after lung transplant | Pericarditis | ANID and subsequently isavuconazole | Death |
| Bachu et al. [54] | 2020 | Turkey | Trichoderma spp. | Capd | Peritonitis | ANID and subsequently AmB | Death |
| Zhou [55] | 2020 | China | T. longibrachiatum | Lung cancer | Pulmonary infection | VOR | Infection resolution |
| Georgakopoulou et al. [56] | 2021 | Greece | T. longibrachiatum | Diabetes mellitus | Pulmonary infection | AmB | Infection resolution |
| Al-Shehri et al. [57] | 2021 | Saudi Arabia | Trichoderma spp. | Acute myeloid leukemia | Endophthalmitis | AmB + surgery | Infection resolution |
| Author | Clinical Manifestation | Specimen | Immunosuppression | Chemotherapy | Time from SOT/ CT | AST | Amb | Vor MIC | Casp | ITR | FLC | KET |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MIC | (mcg/mL) | MIC | MIC | MIC | MIC | |||||||
| (mcg/mL) | (mcg/mL) | (mcg/mL) | (mcg/mL) | (mcg/mL) | ||||||||
| Robertson et al. [16] | Disseminated | NA | No | No | NA | No | ||||||
| Escudero Gil et al. [17] | TRP | BAL | NA | NA | NA | No | ||||||
| Escudero Gil et al. [17] | TRP | BAL | NA | NA | NA | No | ||||||
| Loeppky et al. [18] | Peritonitis | Peritoneal fluid | No | No | Yes | 0.78 | 1.56 | |||||
| Ragnaud et al. [19] | Peritonitis | Peritoneal fluid | No | No | Yes | R | S | S | ||||
| Jacobs et al. [20] | Peritonitis | Surgical debridement | Yes | No | 21 days | Yes | 3.1 | 1.6 | 25 | 0.8 | ||
| Imokawa et al. [21] | TRP | BAL | No | No | No | |||||||
| Tanis et al. [22] | Peritonitis | Peritoneal fluid | No | No | 6 years | No | ||||||
| Gautheret et al. [23] | Disseminated | BAL, skin biopsy | Yes | No | 1 year | Yes | 0.09 | 0.18 | 25 | |||
| Seguin et al. [24] | Brain abscess | Brain specimen | Yes | No | 102 days | Yes | 2.5 | 1.25 | 12.5 | S | ||
| Kawaguchi et al. [25] | TRP | BAL | Yes | No | NA | No | ||||||
| Guiserix et al. [26] | Peritonitis | Peritoneal fluid | No | No | No | |||||||
| Campos-Herrero et al. [27] | Peritonitis | Peritoneal fluid | No | No | Yes | 4.0 | 1.28 | 1.0 | ||||
| Munoz et al. [28] | Skin infection | Biopsy | Yes | No | 8 mo | Yes | 2.0 | 2.0 | ≥64 | |||
| Bren et al. [29] | Peritonitis | Peritoneal fluid | No | No | No | |||||||
| Furukawa et al. [30] | Sinusitis | Biopsy | Yes | No | 6 mo | Yes | 0.58 | 0.035 | 40 | |||
| Richter et al. [31] | Disseminated | Biopsy | Yes | No | 28 days | Yes | 2.0 | 1.0 | ||||
| Guarro et al. [32] | Brain abscess | Biopsy | Yes | No | 1 mo | Yes | 2.0 | 32 | 128 | 8 | ||
| Rota et al. [33] | Peritonitis | Peritoneal fluid | No | No | No | |||||||
| Bustamante-Labarta et al. [34] | Endocarditis | Biopsy | No | No | No | |||||||
| Amato et al. [35] | Encephalitis | CSF | Yes | No | NA | No | ||||||
| Chouaki et al. [36] | Perihepatic hematoma | Abscess aspirate | Yes | No | 9 mo | Yes | >1 | 0.25 | 16 | |||
| Chouaki et al. [36] | TRP | BAL | Yes | No | few days | No | ||||||
| Myoken et al. [37] | Stomatitis | Biopsy | Yes | No | 27 days | Yes | 0.5 | 0.5 | ≥32 | ≥64 | ||
| Esel et al. [38] | Peritonitis | Peritoneal fluid | No | No | Yes | 0.5 | 1.5 | 2 | 1.5 | |||
| De Miguel et al. [39] | TRP | BAL | Yes | No | 12 days | Yes | 0.25 | 2 | 8 | |||
| Alanio et al. [40] | TRP | BAL | Yes | No | 4 days | Yes | 0.5 | 1 | 0.5 | |||
| Kviliute et al. [41] | TRP | BAL | Yes | No | 27 days | Yes | >32 | 4 | 0.125 | >32 | ||
| Lagrange-Xélot et al. [42] | TRP | BAL | Yes | No | 2 mo | Yes | 1 | 0.5 | 0.5 | 2 | >64 | |
| Trabelsi et al. [43] | Skin infection | Byopsy | NA | No | Yes | 1 | 0.5 | 0.5 | ||||
| Santillan Salas et al. [44] | Peritonitis | Biopsy | No | No | Yes | ≥1 | ≤0.5 | |||||
| Rodríguez Peralta et al. [45] | Endocarditis | Peritoneal fluid | No | No | No | |||||||
| Molnár-Gábor et al. [46] | Sinusitis | Biopsy | No | No | Yes | 0,5 | 0.5 | 0.25 | ||||
| Festuccia et al. [47] | TRP | BAL | Yes | No | 10 days | Yes | 0.125 | 0.047 | >256 | >32 | ||
| Tascini et al. [48] | Endocarditis | Catheter tip | No | No | Yes | 2 | 0.5 | 1 | ||||
| Akagi et al. [49] | TRP | BAL | Yes | No | 151 days | No | ||||||
| Carlson et al. [50] | Peritonitis | Peritoneal fluid | No | No | No | |||||||
| Román-Soto et al. [51] | Necrotic ulcers | Skin biopsy | Yes | No | NA | Yes | 1.5 | 0.23 | 0.047 | 0.23 | ||
| Sautour et al. [52] | TRP | BAL | Yes | No | 11 days | Yes | 2 | 0.19 | 0.064 | >32 | ||
| Recio et al. [53] | Pericarditis | BAL | Yes | No | 2 mo | Yes | 1 | 2 | 1 | |||
| Bachu et al. [54] | Peritonitis | NA | No | No | No | |||||||
| Zhou [55] | TRP | Biopsy | Yes | No | 0 days | Yes | 4 | 1 | ≤0.03 | >16 | >64 | |
| Georgakopoulou et al. [56] | TRP | Pleural fluid | No | No | Yes | S | R | R | R | R | ||
| Al-Shehri et al. [57] | Endophthalmitis | Vitreous tap | Yes | No | 2 weeks | Yes | 0.5 | 16 | 0.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burzio, C.; Balzani, E.; Montrucchio, G.; Trompeo, A.C.; Corcione, S.; Brazzi, L. Trichoderma spp.-Related Pneumonia: A Case Report in Heart–Lung Transplantation Recipient and a Systematic Literature Review. J. Fungi 2023, 9, 195. https://doi.org/10.3390/jof9020195
Burzio C, Balzani E, Montrucchio G, Trompeo AC, Corcione S, Brazzi L. Trichoderma spp.-Related Pneumonia: A Case Report in Heart–Lung Transplantation Recipient and a Systematic Literature Review. Journal of Fungi. 2023; 9(2):195. https://doi.org/10.3390/jof9020195
Chicago/Turabian StyleBurzio, Carlo, Eleonora Balzani, Giorgia Montrucchio, Anna Chiara Trompeo, Silvia Corcione, and Luca Brazzi. 2023. "Trichoderma spp.-Related Pneumonia: A Case Report in Heart–Lung Transplantation Recipient and a Systematic Literature Review" Journal of Fungi 9, no. 2: 195. https://doi.org/10.3390/jof9020195