
Evaluation of 11 DNA Automated Extraction Protocols for the Detection of the 5 Mains Candida Species from Artificially Spiked Blood

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of Artificially Inoculated Blood
2.2. DNA Extraction Methods
2.3. Real Time PCR Assay
2.4. Detection of Inhibitors
2.5. DNA Quantification
2.6. Human Gene Amplification
2.7. Specimen Testing
2.8. Determination of PCR Sensitivity
2.9. Statistical Analysis
3. Results
3.1. Determination of PCR Performances
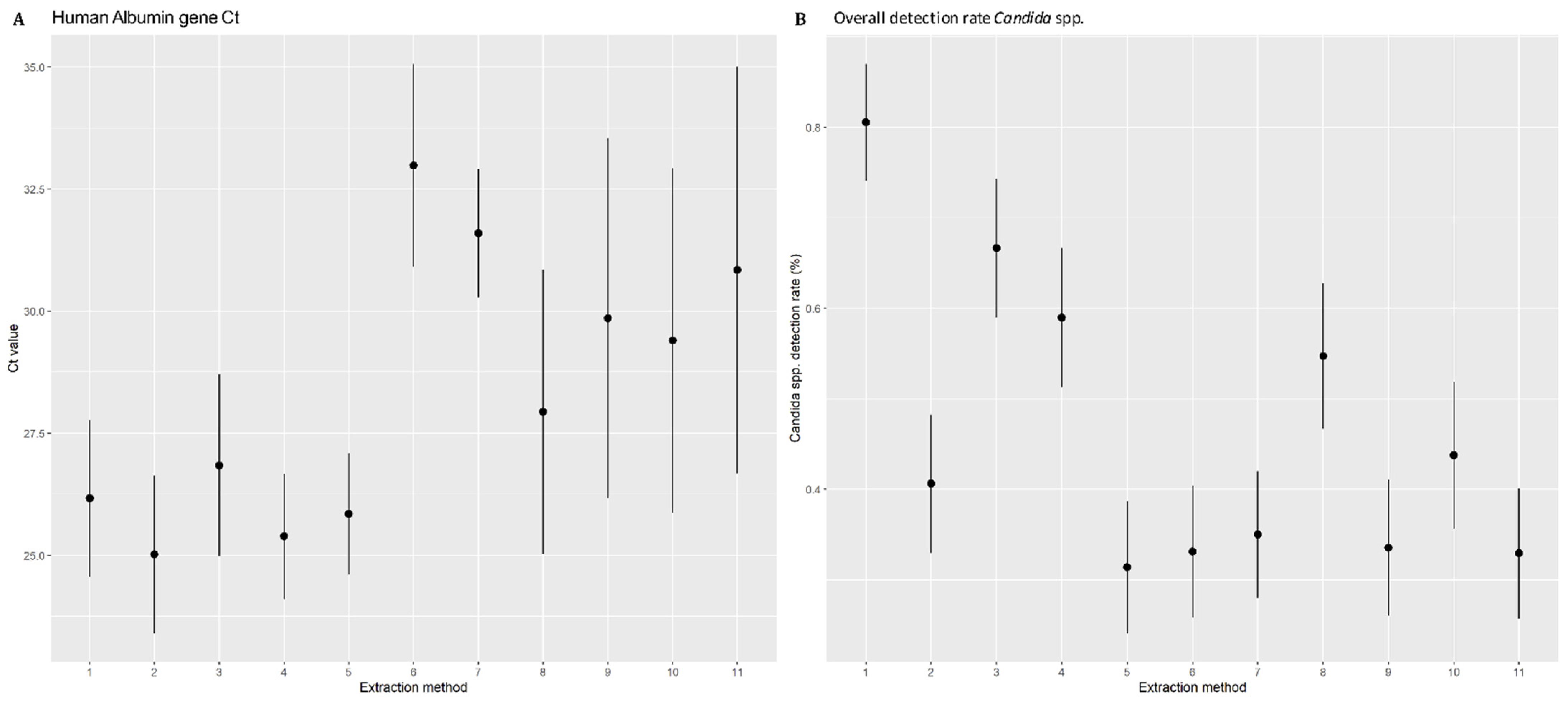
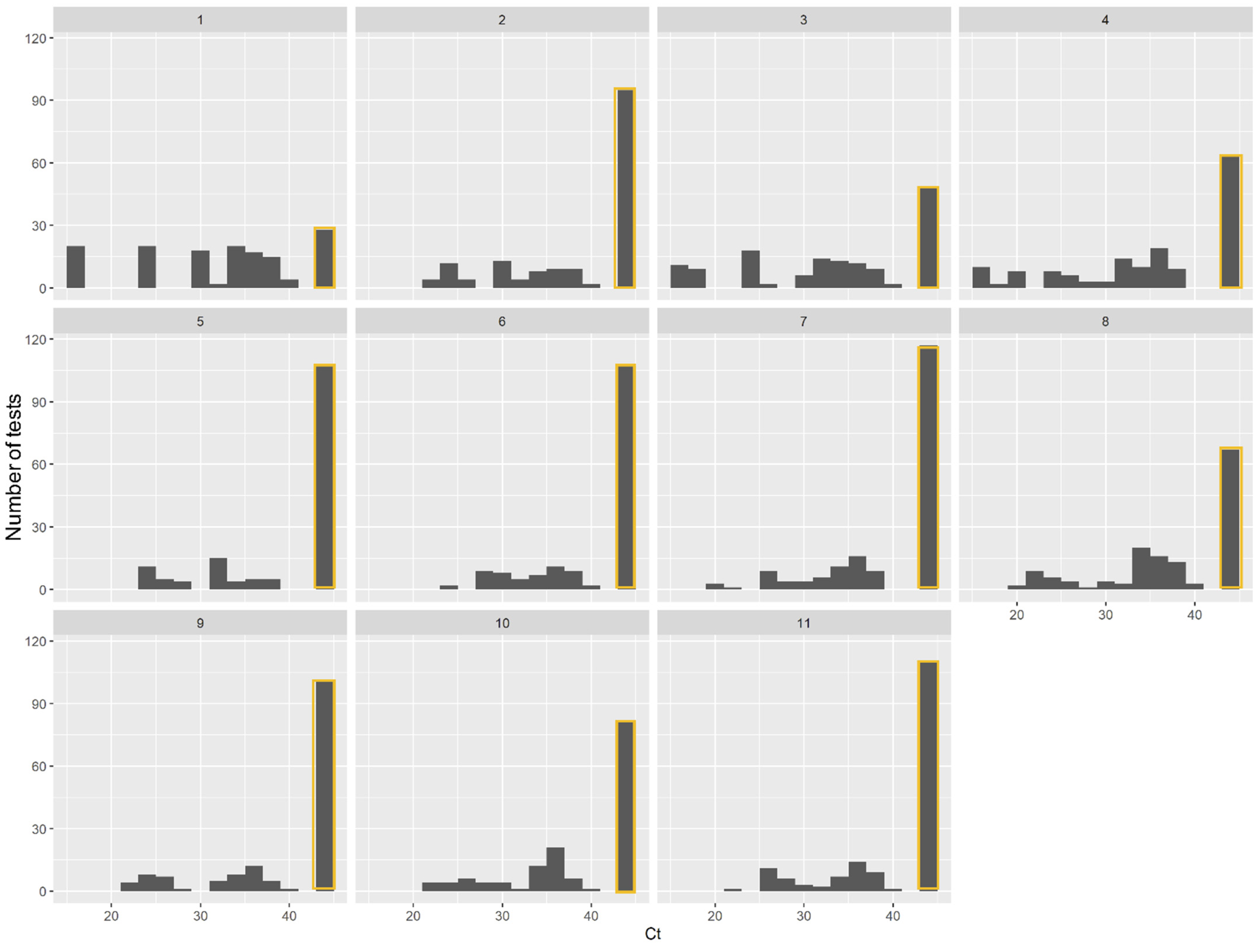
3.2. Human Albumin Gene Amplification and DNA Quantification
3.3. Comparison of DNA Extraction Methods in Isolating Candida DNA from Spiked Blood
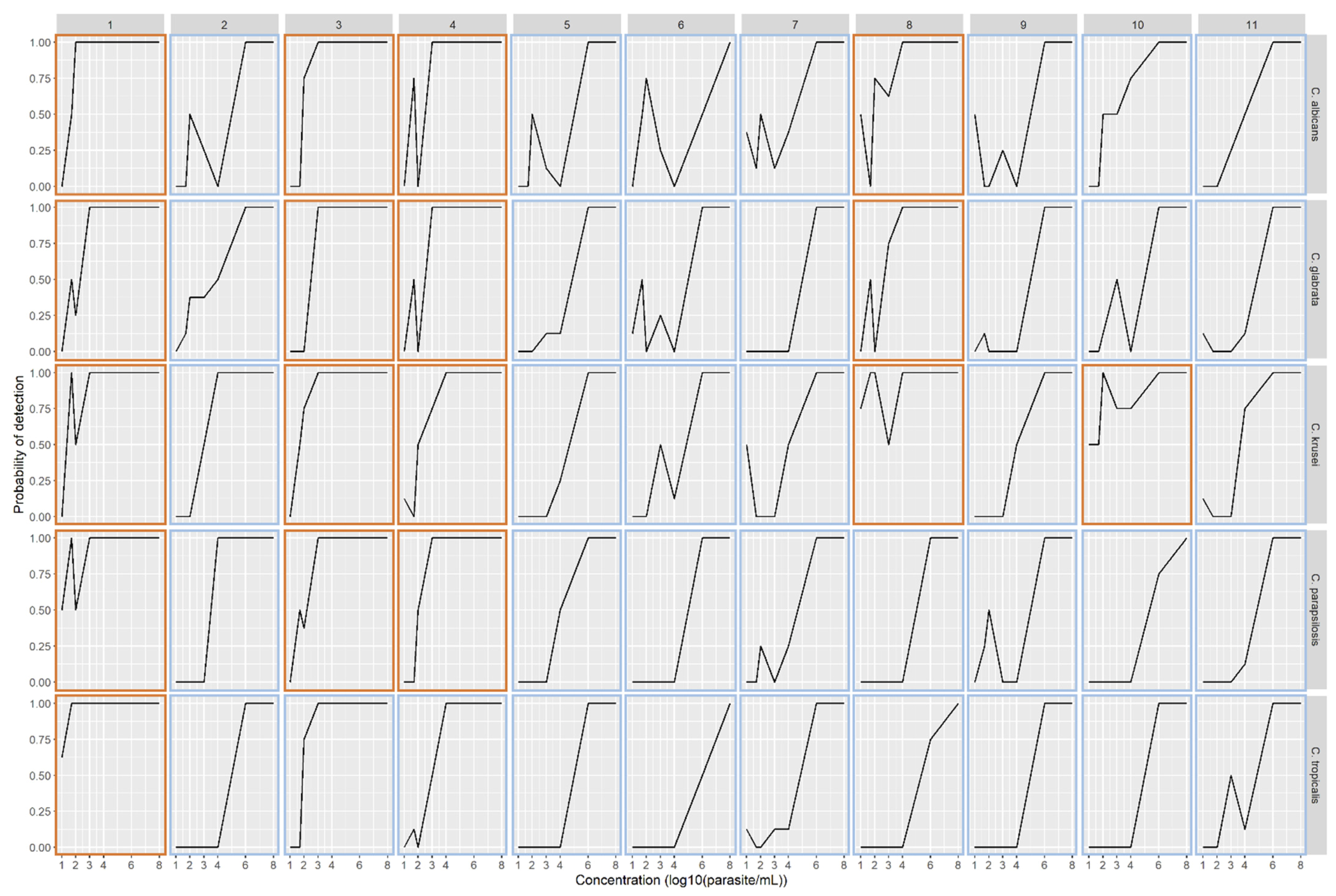
3.4. Performance of DNA Extraction Methods Adjusted for Candida Species and Sample Concentration
3.5. Detection of PCR Inhibitors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Magill, S.S.; O’Leary, E.; Janelle, S.J.; Thompson, D.L.; Dumyati, G.; Nadle, J.; Wilson, L.E.; Kainer, M.A.; Lynfield, R.; Greissman, S.; et al. Changes in Prevalence of Health Care-Associated Infections in U.S. Hospitals. N. Engl. J. Med. 2018, 379, 1732–1744. [Google Scholar] [CrossRef]
- Lortholary, O.; Renaudat, C.; Sitbon, K.; Desnos-Ollivier, M.; Bretagne, S.; Dromer, F.; French Mycoses Study Group. The Risk and Clinical Outcome of Candidemia Depending on Underlying Malignancy. Intensiv. Care Med. 2017, 43, 652–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keighley, C.L.; Pope, A.; Marriott, D.J.E.; Chapman, B.; Bak, N.; Daveson, K.; Hajkowicz, K.; Halliday, C.; Kennedy, K.; Kidd, S.; et al. Risk Factors for Candidaemia: A Prospective Multi-Centre Case-Control Study. Mycoses 2020. [Google Scholar] [CrossRef]
- Rajendran, R.; Sherry, L.; Deshpande, A.; Johnson, E.M.; Hanson, M.F.; Williams, C.; Munro, C.A.; Jones, B.L.; Ramage, G. A Prospective Surveillance Study of Candidaemia: Epidemiology, Risk Factors, Antifungal Treatment and Outcome in Hospitalized Patients. Front. Microbiol. 2016, 7. [Google Scholar] [CrossRef] [Green Version]
- Kullberg, B.J.; Arendrup, M.C. Invasive Candidiasis. N. Engl. J. Med. 2015, 373, 1445–1456. [Google Scholar] [CrossRef] [Green Version]
- Clancy, C.J.; Nguyen, M.H. Finding the “Missing 50%” of Invasive Candidiasis: How Nonculture Diagnostics Will Improve Understanding of Disease Spectrum and Transform Patient Care. Clin. Infect. Dis. 2013, 56, 1284–1292. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, C.D.; Samsa, G.P.; Schell, W.A.; Reller, L.B.; Perfect, J.R.; Alexander, B.D. Quantitation of Candida CFU in Initial Positive Blood Cultures. J. Clin. Microbiol. 2011, 49, 2879–2883. [Google Scholar] [CrossRef] [Green Version]
- Clancy, C.J.; Nguyen, M.H. Diagnosing Invasive Candidiasis. J. Clin. Microbiol. 2018, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taieb, F.; Méchaï, F.; Lefort, A.; Lanternier, F.; Bougnoux, M.-E.; Lortholary, O. Management of candidemia and invasive candidiasis. Rev. Med. Interne 2011, 32, 173–180. [Google Scholar] [CrossRef]
- Camp, I.; Spettel, K.; Willinger, B. Molecular Methods for the Diagnosis of Invasive Candidiasis. J. Fungi 2020, 6, 101. [Google Scholar] [CrossRef]
- Avni, T.; Leibovici, L.; Paul, M. PCR Diagnosis of Invasive Candidiasis: Systematic Review and Meta-Analysis. J. Clin. Microbiol. 2011, 49, 665–670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuchs, S.; Lass-Flörl, C.; Posch, W. Diagnostic Performance of a Novel Multiplex PCR Assay for Candidemia among ICU Patients. J. Fungi 2019, 5, 86. [Google Scholar] [CrossRef] [Green Version]
- Denina, M.; Scolfaro, C.; Colombo, S.; Calitri, C.; Garazzino, S.; Barbui Anna, A.; Brossa, S.; Regina Margherita Children’s Hospital Bloodstream Infections Study Group Participants; Tovo, P.-A. Magicplex(TM) Sepsis Real-Time Test to Improve Bloodstream Infection Diagnostics in Children. Eur. J. Pediatr. 2016, 175, 1107–1111. [Google Scholar] [CrossRef] [Green Version]
- Bretagne, S.; Costa, J.M. Towards a Molecular Diagnosis of Invasive Aspergillosis and Disseminated Candidosis. Available online: https://pubmed.ncbi.nlm.nih.gov/16054349/ (accessed on 30 January 2021).
- Müller, F.-M.C.; Werner, K.E.; Kasai, M.; Francesconi, A.; Chanock, S.J.; Walsh, T.J. Rapid Extraction of Genomic DNA from Medically Important Yeasts and Filamentous Fungi by High-Speed Cell Disruption. J. Clin. Microbiol. 1998, 36, 1625–1629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paul, R.; Ostermann, E.; Wei, Q. Advances in Point-of-Care Nucleic Acid Extraction Technologies for Rapid Diagnosis of Human and Plant Diseases. Biosens. Bioelectron. 2020, 169, 112592. [Google Scholar] [CrossRef] [PubMed]
- Colman, R.E.; Suresh, A.; Dolinger, D.L.; Muñoz, T.; Denkinger, C.M.; Rodwell, T.C. Review of Automated DNA Extraction Systems for Sequencing-Based Solutions for Drug-Resistant Tuberculosis Detection. Diagn. Microbiol. Infect. Dis. 2020, 98, 115096. [Google Scholar] [CrossRef]
- Jeddi, F.; Piarroux, R.; Mary, C. Application of the NucliSENS EasyMAG System for Nucleic Acid Extraction: Optimization of DNA Extraction for Molecular Diagnosis of Parasitic and Fungal Diseases. Parasite 2013, 20. [Google Scholar] [CrossRef]
- Zhang, J.; Hung, G.-C.; Nagamine, K.; Li, B.; Tsai, S.; Lo, S.-C. Development of Candida-Specific Real-Time PCR Assays for the Detection and Identification of Eight Medically Important Candida Species. Microbiol. Insights 2016, 9, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis, 2nd ed.; Use R! Springer International Publishing: Berlin/Heidelberg, Germany, 2016; ISBN 978-3-319-24275-0. [Google Scholar]
- Zeller, I.; Schabereiter-Gurtner, C.; Mihalits, V.; Selitsch, B.; Barousch, W.; Hirschl, A.M.; Makristathis, A.; Willinger, B. Detection of Fungal Pathogens by a New Broad Range Real-Time PCR Assay Targeting the Fungal ITS2 Region. J. Med. Microbiol. 2017, 66, 1383–1392. [Google Scholar] [CrossRef]
- Camp, I.; Manhart, G.; Schabereiter-Gurtner, C.; Spettel, K.; Selitsch, B.; Willinger, B. Clinical Evaluation of an In-House Panfungal Real-Time PCR Assay for the Detection of Fungal Pathogens. Infection 2020, 48, 345–355. [Google Scholar] [CrossRef] [Green Version]
- Lau, A.; Halliday, C.; Chen, S.C.-A.; Playford, E.G.; Stanley, K.; Sorrell, T.C. Comparison of Whole Blood, Serum, and Plasma for Early Detection of Candidemia by Multiplex-Tandem PCR. J. Clin. Microbiol. 2010, 48, 811–816. [Google Scholar] [CrossRef] [Green Version]
- Metwally, L.; Fairley, D.J.; Coyle, P.V.; Hay, R.J.; Hedderwick, S.; McCloskey, B.; O’Neill, H.J.; Webb, C.H.; Elbaz, W.; McMullan, R. Improving Molecular Detection of Candida DNA in Whole Blood: Comparison of Seven Fungal DNA Extraction Protocols Using Real-Time PCR. J. Med. Microbiol. 2008, 57, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Bastien, P.; Procop, G.W.; Reischl, U. Quantitative Real-Time PCR Is Not More Sensitive than “Conventional” PCR. J. Clin. Microbiol. 2008, 46, 1897–1900. [Google Scholar] [CrossRef] [Green Version]
- Löffler, J.; Hebart, H.; Schumacher, U.; Reitze, H.; Einsele, H. Comparison of Different Methods for Extraction of DNA of Fungal Pathogens from Cultures and Blood. J. Clin. Microbiol. 1997, 35, 3311–3312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, P.; Pandey, P.; Harishankar, A.; Chandy, M.; Bhattacharya, S. A High Yield DNA Extraction Method for Medically Important Candida Species: A Comparison of Manual versus QIAcube-Based Automated System. Indian J. Med. Microbiol. 2016, 34, 533–535. [Google Scholar] [CrossRef] [PubMed]
- Scharf, S.; Bartels, A.; Kondakci, M.; Pfeffer, K.; Henrich, B.; Haas, R. Introduction of a Bead Beating Step Improves Fungal DNA Extraction from Selected Patient Specimens. Int. J. Med. Microbiol. 2020, 310, 151443. [Google Scholar] [CrossRef]
- Kumari, A.; Mankotia, S.; Chaubey, B.; Luthra, M.; Singh, R. Role of Biofilm Morphology, Matrix Content and Surface Hydrophobicity in the Biofilm-Forming Capacity of Various Candida Species. J. Med. Microbiol. 2018, 67, 889–892. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Method | Kit | Company | Automate | Validated Sample | Validated Material | Nucleic Acids | Pretreatment | Sample Volume | Expected Elution Volume | Observed Elution Volume | Elution Appearance | DNA Quantification (ng/µL) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C | M | E | ||||||||||||
| 1 | NucliSENSTM EasyMAGTM | BioMérieux | NucliSENS EasyMAG | Human | Whole blood, serum, plasma, stools, respiratory samples and other body fluids. | DNA/RNA | LB | CB | - | 200 µL | 110 µL | 110 µL | Clear | 27.0 (±6.6) |
| 2 | EZ1TM DNA Blood 200 µL Kit | Qiagen | EZ1 | Human | Whole blood | DNA | - | - | - | 200 µL | 100 µL | 100 µL | Clear | 30.5 (±5.5) |
| 3 | EZ1TM DNA Blood 200 µL Kit + pretreatment | Qiagen | EZ1 | Human | Whole blood | DNA | LB | CB | - | 200 µL | 100 µL | 100 µL | Clear | 10.4 (±2.7) |
| 4 | EZ1TM DNA Tissue Kit + pretreatment | Qiagen | EZ1 | Human | Whole dried blood, tissue, buccal cells, cultured cells, Paraffin-Embedded Tissue | DNA | - | - | Ly | 200 µL | 100 µL | 100 µL | Clear | 30.3 (±3.3) |
| 5 | QIAamp 96 DNA QIAcube HT Kit | Qiagen | QIAcube | Human | Whole blood, tissue, cells | DNA | - | - | PK | 200 µL | 120 µL | 120 µL | Red tinted | 30.2 (±6.6) |
| 6 | Macherey-Nagel™ Pathogène NucleoMag™ | Fisher Scientific | KingFisher | Human | Whole blood, serum, plasma; tissue (e.g., ear notches); feces; swab wash solution | DNA/RNA | - | - | PK | 150 µL | 80 µL | 80 µL | Clear | 30.2 (±7.9) |
| 7 | Mag-BindTM Viral DNA/RNA | Omega Bio-tek | KingFisher | Human | Whole blood, serum, plasma, saliva, and other body fluids. | DNA/RNA | - | - | PK | 200 µL | 100 µL | 100 µL | Clear | 84.5 (±29.0) |
| 8 | MagMAX™ Viral/Pathogen Nucleic Acid Isolation Kit | Applied Biosystems | MGISP-960 | Human | Whole blood, swabs, urine, and viral transport media | DNA/RNA | - | - | PK | 400 µL | 100 µL | 100 µL | Red tinted | 32.2 (±35.3) |
| 9 | Chemagic Viral DNA/RNA 300 kit H96 | PerkinElmer | Chemagic 360 | Human | Serum, plasma, saliva, nasal or oral swab, BALF | DNA/RNA | - | - | PK | 300 µL | 100 µL | 100 µL | Red tinted | 17.8 (±19.5) |
| 10 | Virus DNA/RNA Extraction kit | MGI | MGISP-960 | Human | Serum, plasma, saliva, virus culture medium, throat swabs, BALF, sputum | DNA/RNA | - | - | PK | 200 µL | 100 µL | 25 µL | Clear | 61.3 (±42.6) |
| 11 | BioextractTM SuperballTM | Biosellal | KingFisher | Veterinary | Whole blood, milk, serum, organs | DNA/RNA | - | - | PK | 200 µL | 100 µL | 100 µL | Clear | 13.9 (±2.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menu, E.; Landier, J.; Prudent, E.; Ranque, S.; L’Ollivier, C. Evaluation of 11 DNA Automated Extraction Protocols for the Detection of the 5 Mains Candida Species from Artificially Spiked Blood. J. Fungi 2021, 7, 228. https://doi.org/10.3390/jof7030228
Menu E, Landier J, Prudent E, Ranque S, L’Ollivier C. Evaluation of 11 DNA Automated Extraction Protocols for the Detection of the 5 Mains Candida Species from Artificially Spiked Blood. Journal of Fungi. 2021; 7(3):228. https://doi.org/10.3390/jof7030228
Chicago/Turabian StyleMenu, Estelle, Jordi Landier, Elsa Prudent, Stéphane Ranque, and Coralie L’Ollivier. 2021. "Evaluation of 11 DNA Automated Extraction Protocols for the Detection of the 5 Mains Candida Species from Artificially Spiked Blood" Journal of Fungi 7, no. 3: 228. https://doi.org/10.3390/jof7030228