
Radiomics Analyses to Predict Histopathology in Patients with Metastatic Testicular Germ Cell Tumors before Post-Chemotherapy Retroperitoneal Lymph Node Dissection

 ,
,  , ,
, ,  , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
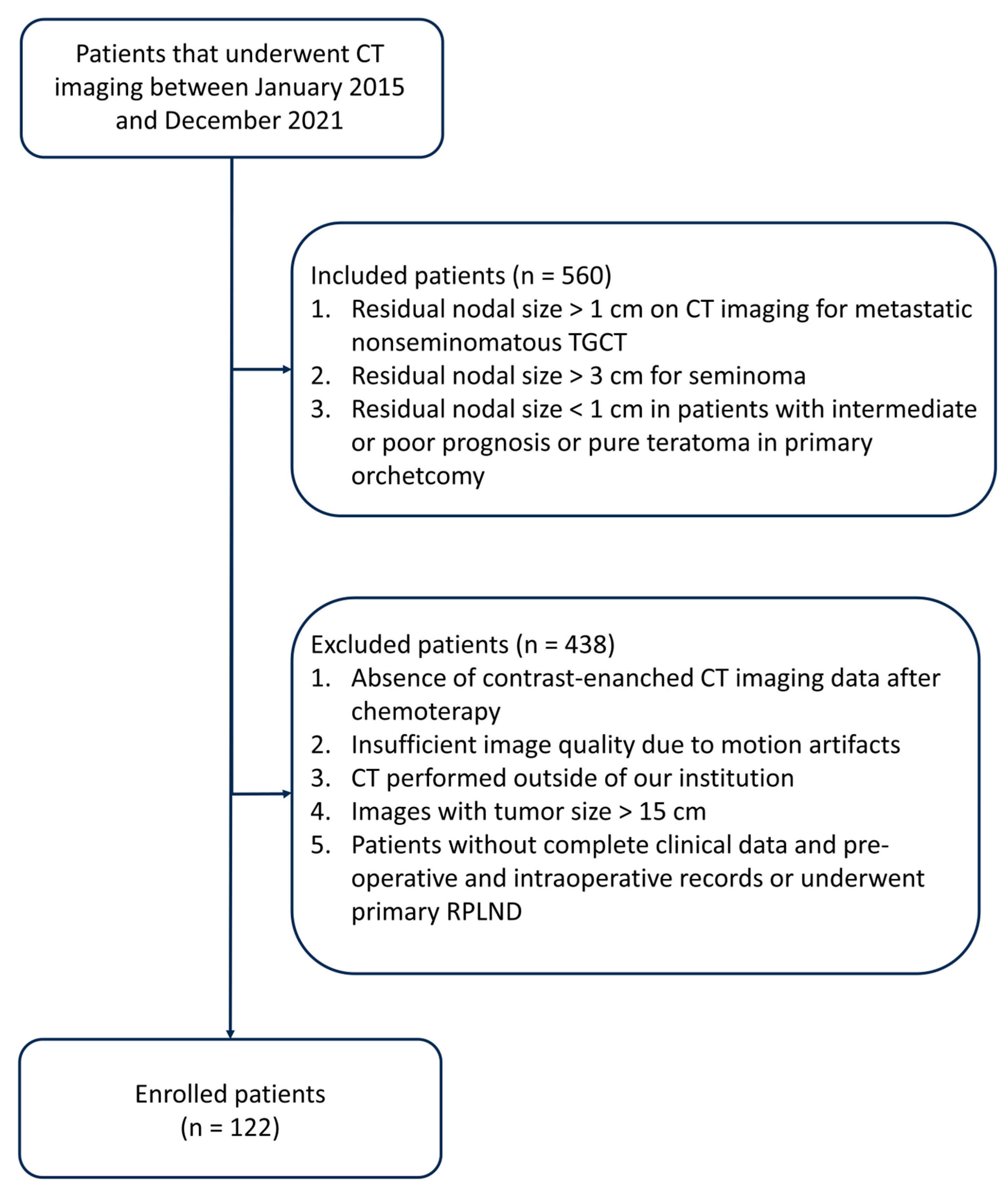
2.1. Study Design
- (a)
- Residual nodal size exceeding 1 cm, as determined through transverse axial dimension on CT imaging, following frontline cisplatin-based chemotherapy for metastatic non-seminomatous TGCT.
- (b)
- Residual nodal size exceeds 3 cm in cases of seminoma.
- (c)
- Residual nodal size measuring less than 1 cm in patients exhibiting intermediate or poor prognosis or pure teratoma in the primary orchiectomy specimen.
- (a)
- Lack of contrast-enhanced CT imaging data post-chemotherapy.
- (b)
- Inadequate image quality is attributable to motion artifacts.
- (c)
- CT scans were conducted at external institutions.
- (d)
- Images displaying a tumor size exceeding 15 cm.
- (e)
- Patients without comprehensive clinical data, pre-operative and intraoperative records, or patients who underwent primary RPLND.
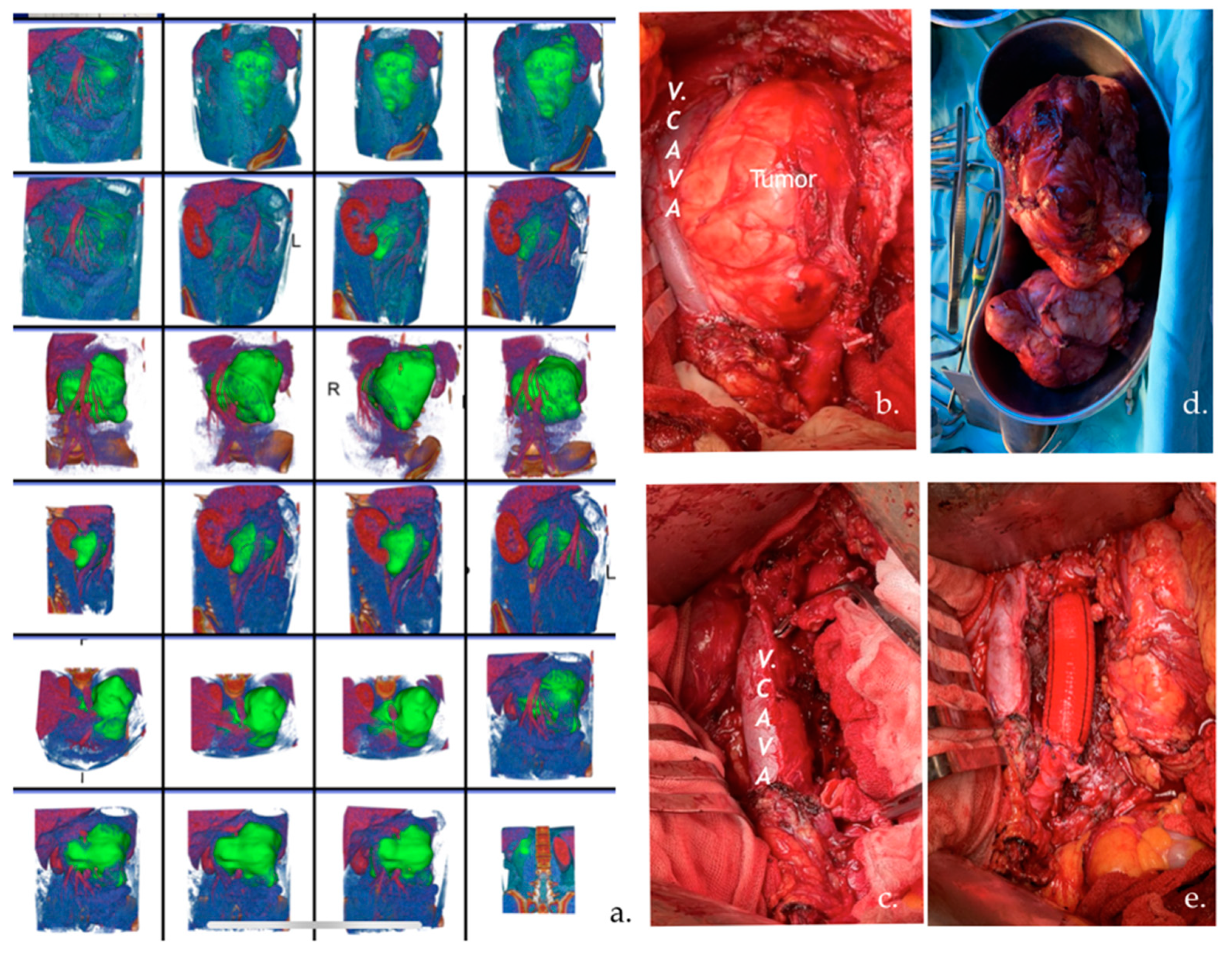
2.2. Segmentation
2.3. Radiomics Feature Extraction
- diagnostics_Configuration_Settings.additionalInfo (True)
- Configuration_Settings.binWidth (25.0)
- Configuration_Settings.distancesforce2Ddimension (0)
- Configuration_Settings.interpolator (sitkBSpline).label (1.0)
- minimumROIDimensions (2)
- minimumROISize (null)
- normalize (false)
- diagnostics_Configuration_Settings.normalizeScale (1)
- diagnostics_Configuration_Settings.padDistance (5)
- diagnostics_Configuration_Settings.preCrop (false)
- diagnostics_Configuration_Settings.removeOutliers (null)
- diagnostics_Configuration_Settings.resampledPixelSpacing (null)
- diagnostics_Configuration_Settings.resegmentRange (null)
- diagnostics_Configuration_Settings.symmetricalGLCM (true)
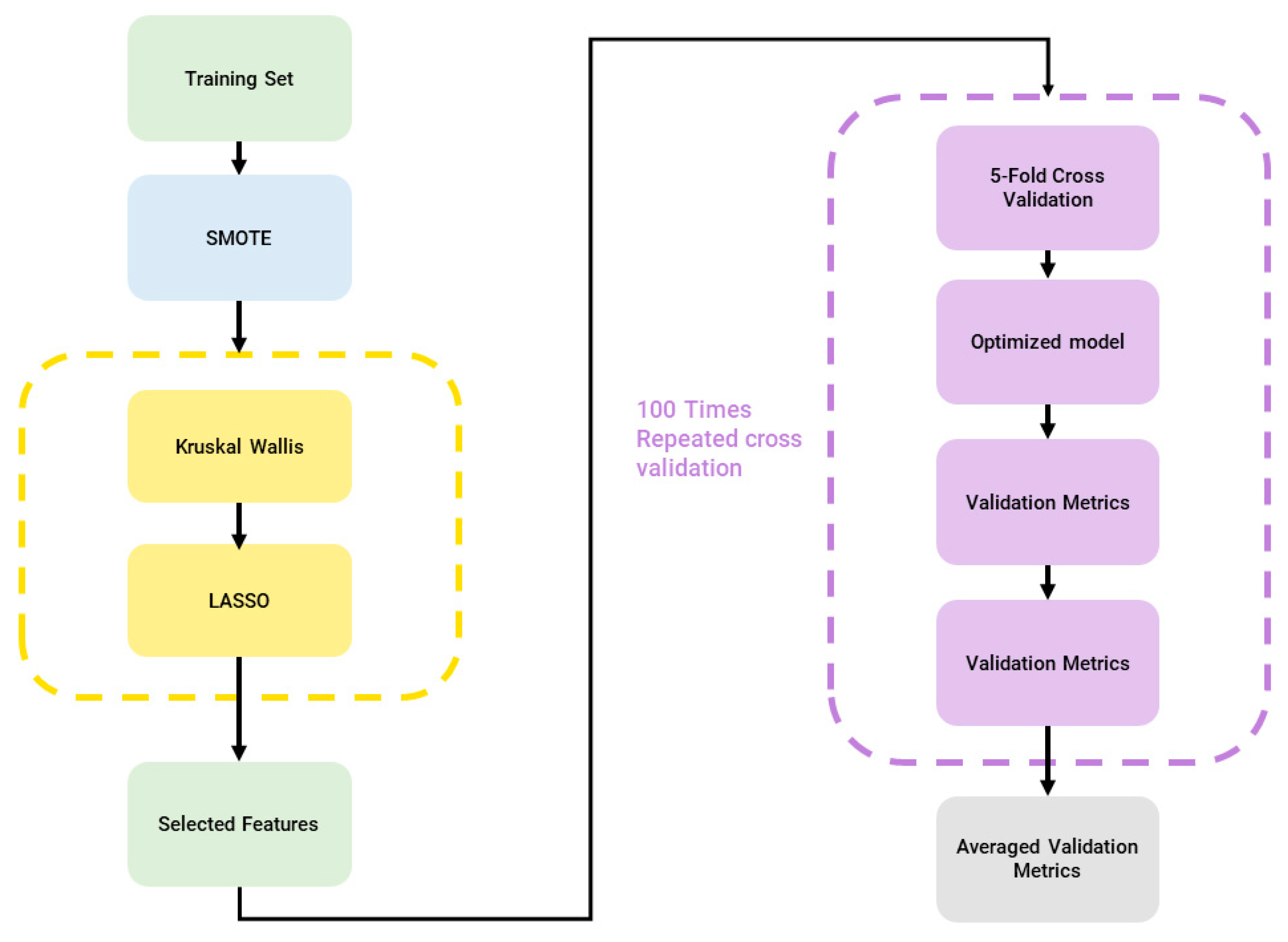
2.4. Machine Learning Pipeline
2.4.1. Minority Classes Oversampling
2.4.2. Feature Reduction and Selection
- In the event that none of the features meet the first threshold (p < 0.005), we elevated the p-value threshold to the second level;
- If the second threshold remains unmet, we escalate the p-value to the third threshold;
- If none of the features satisfied the third threshold, all the features were given as input to the LASSO. The optimal lambda value was determined through a rigorous 10-fold cross-validation process.
2.4.3. Classification
2.4.4. Statistical Analyses
- Accuracy ((TP + TN)/(TP + TN + FP + FN))
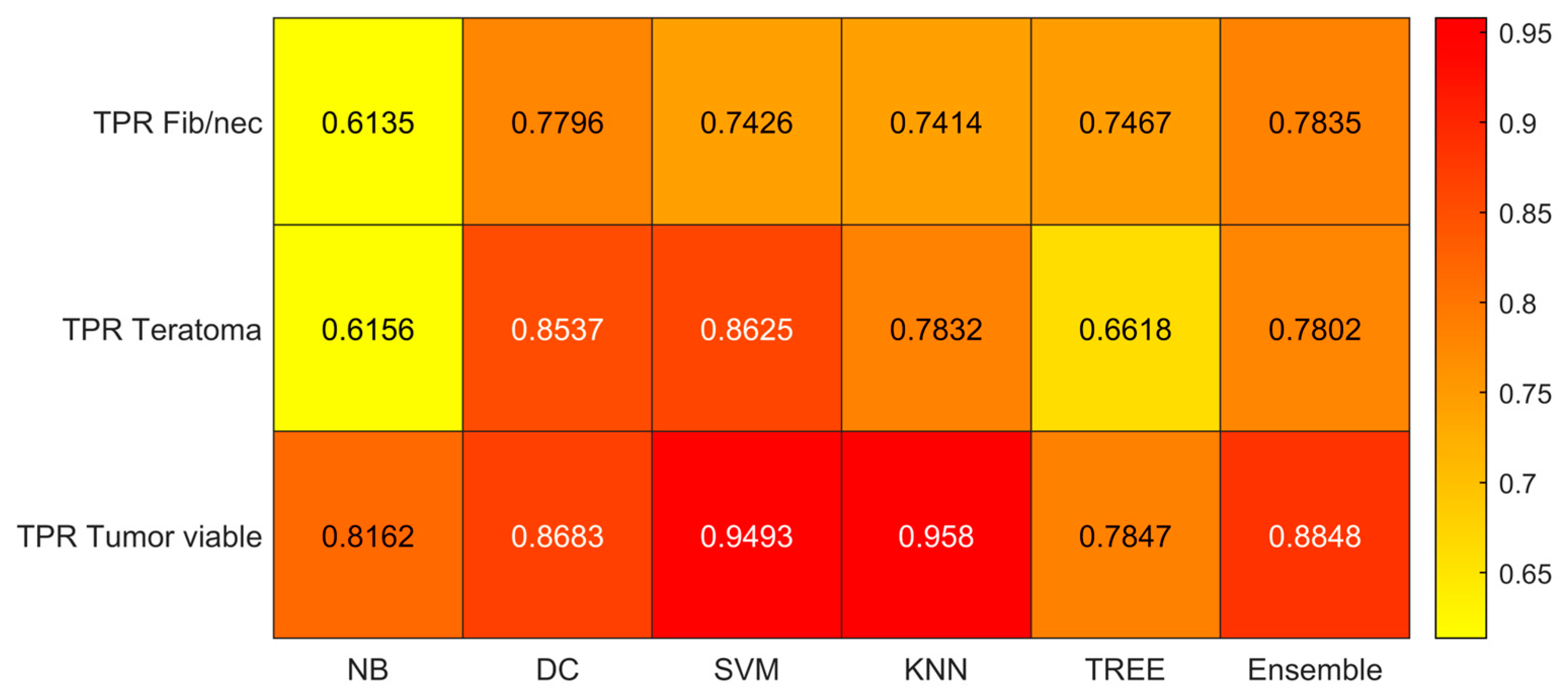
- True Positive Rate (TPR) or sensitivity (TP/(TP + FN))
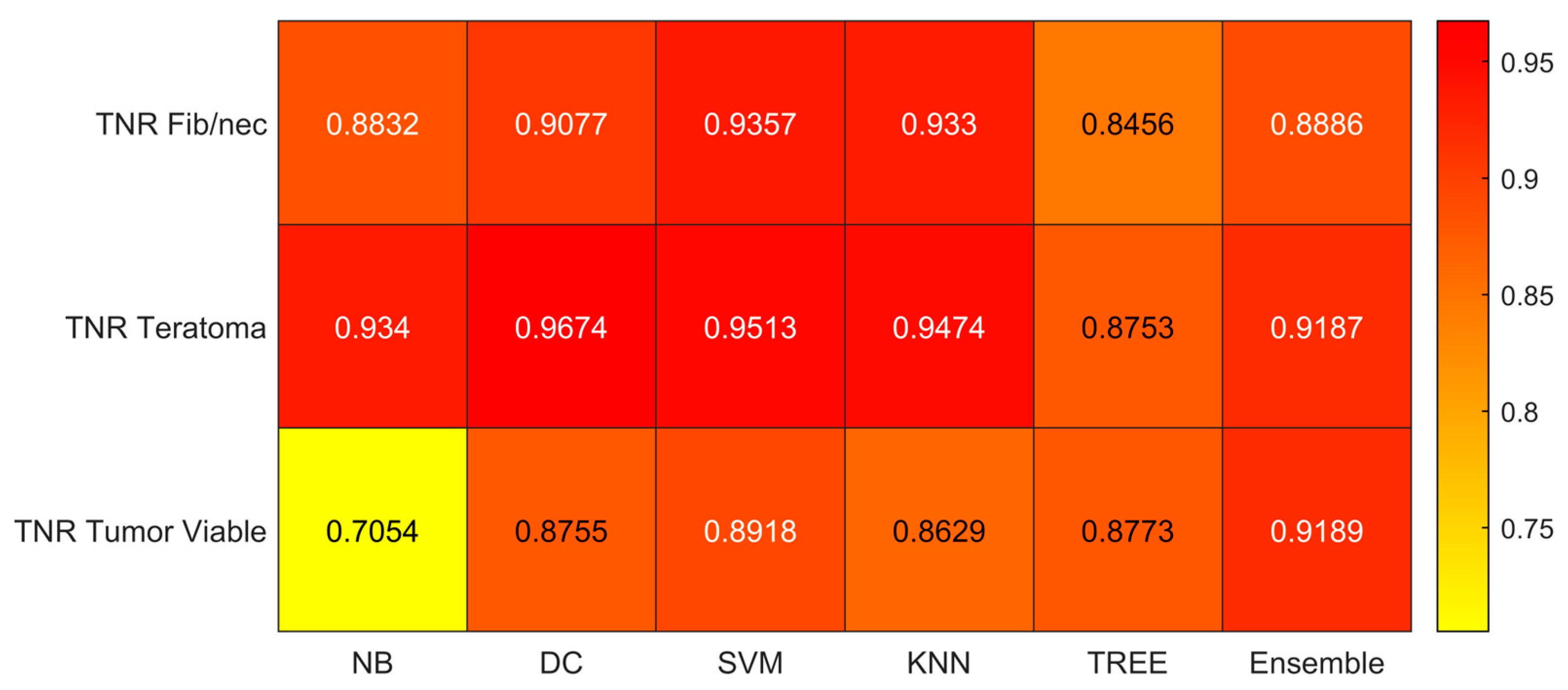
- True Negative Rate (TNR) or specificity (TN/(TN + FP))
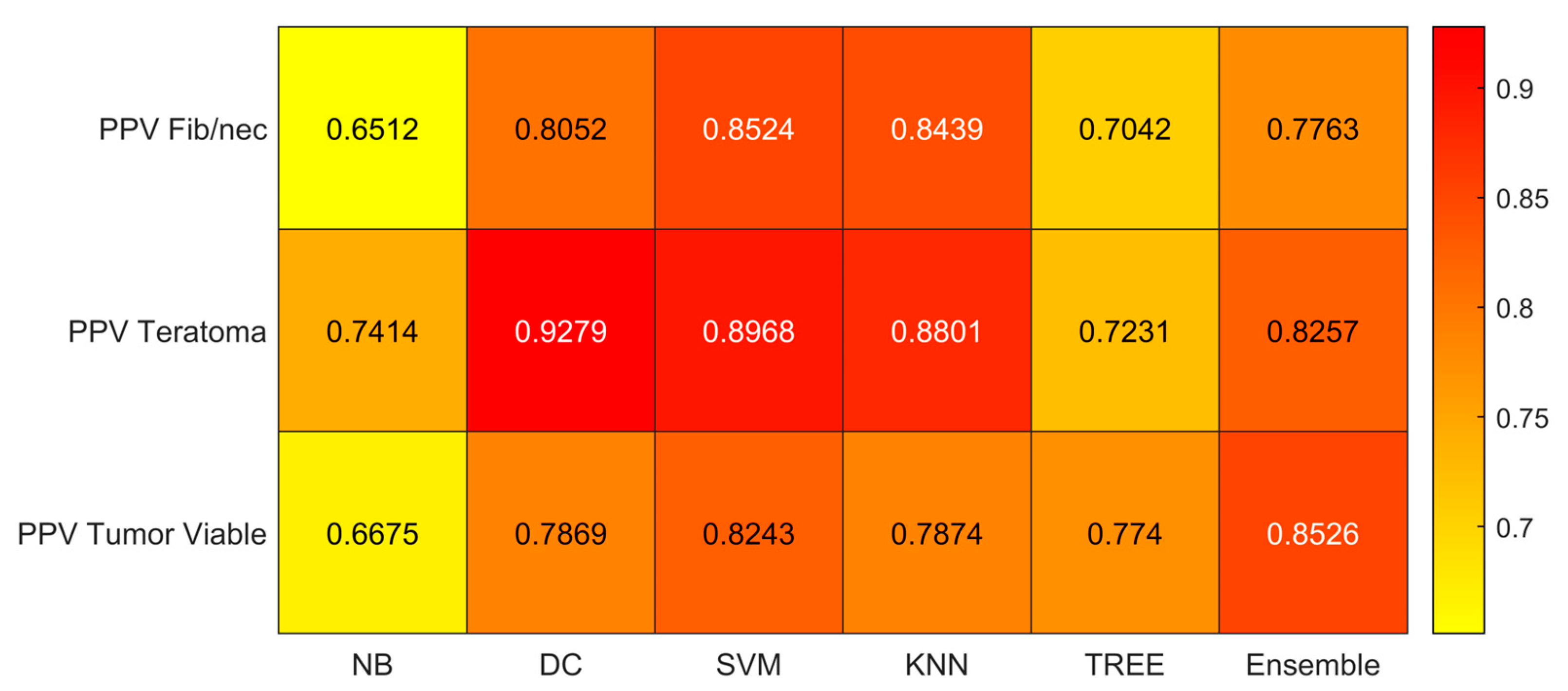
- Positive Predicted Value (PPV) or precision (TP/(TP + FP))
- The area under the receiver operating characteristic curve (AUC)
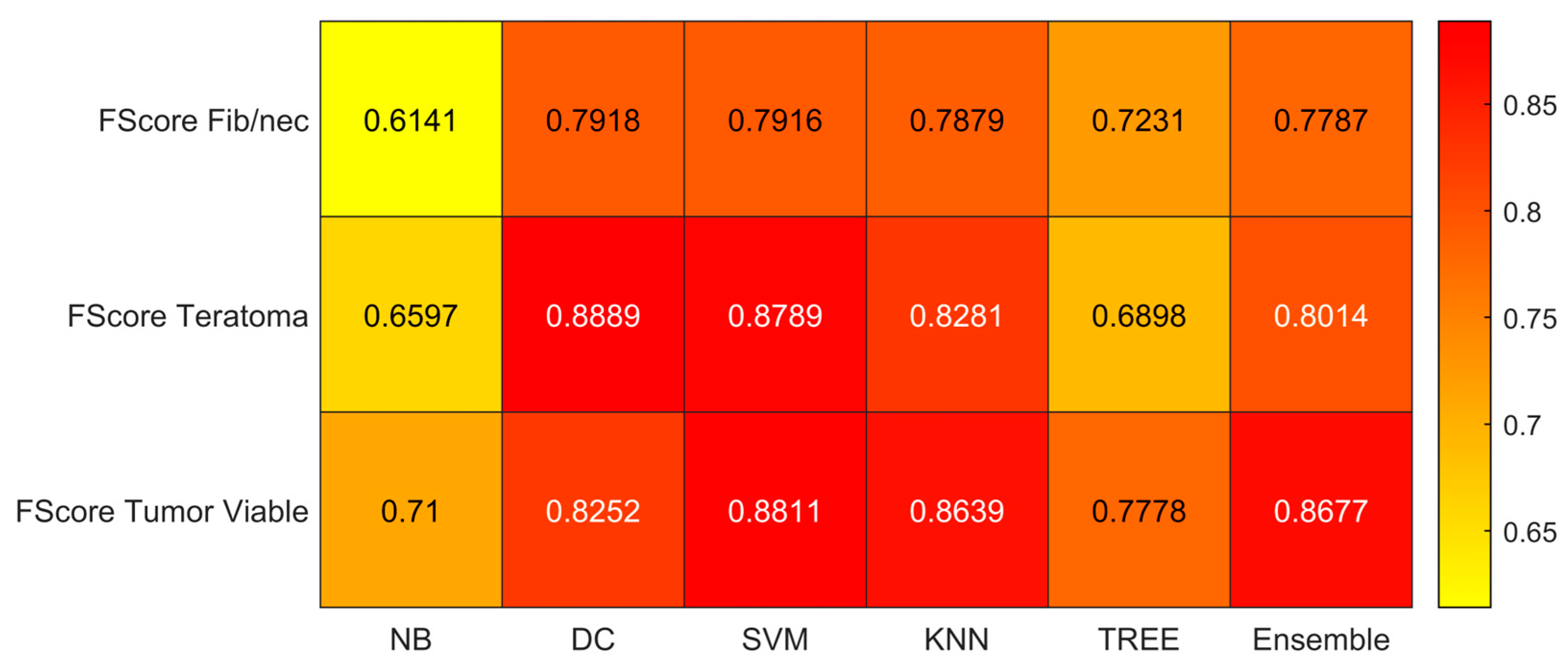
- F-score
3. Results
3.1. Clinical Data
3.2. Feature Reduction and Selection
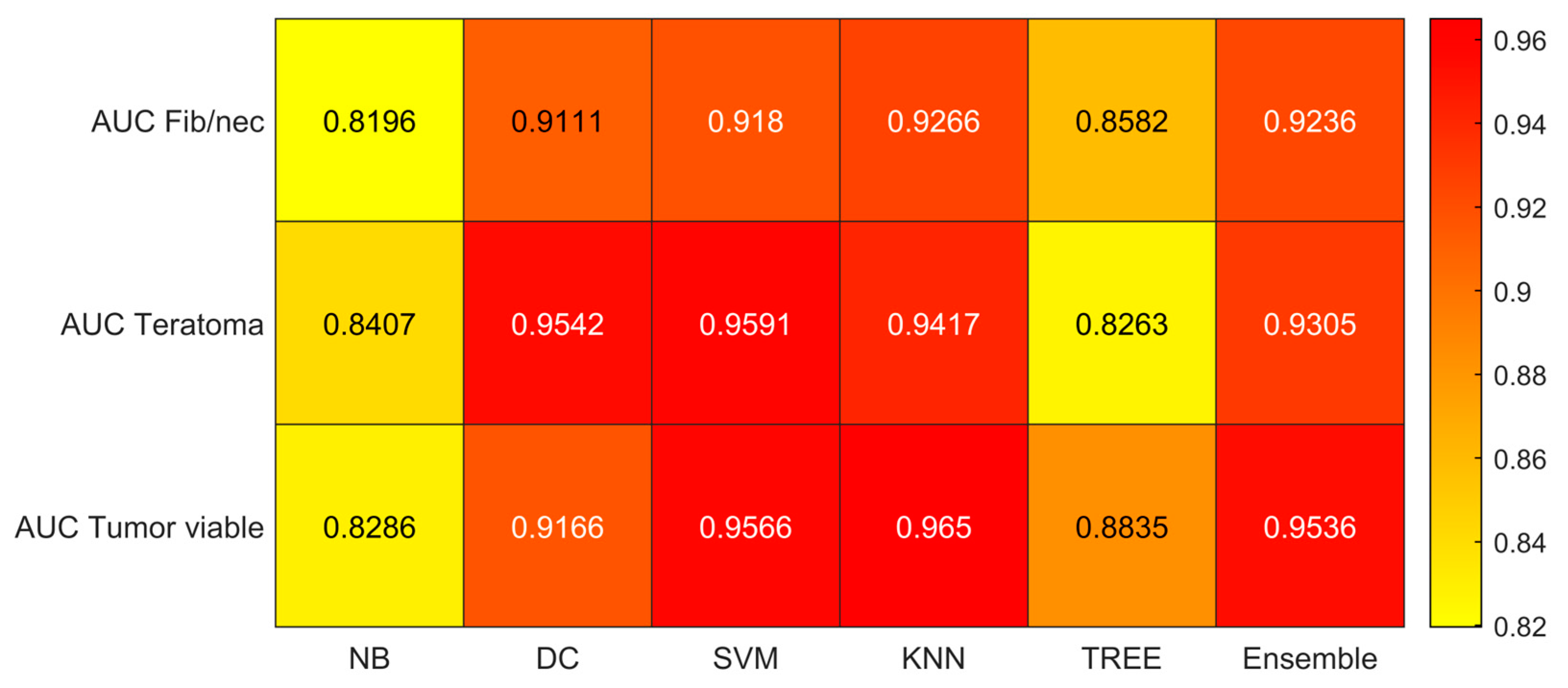
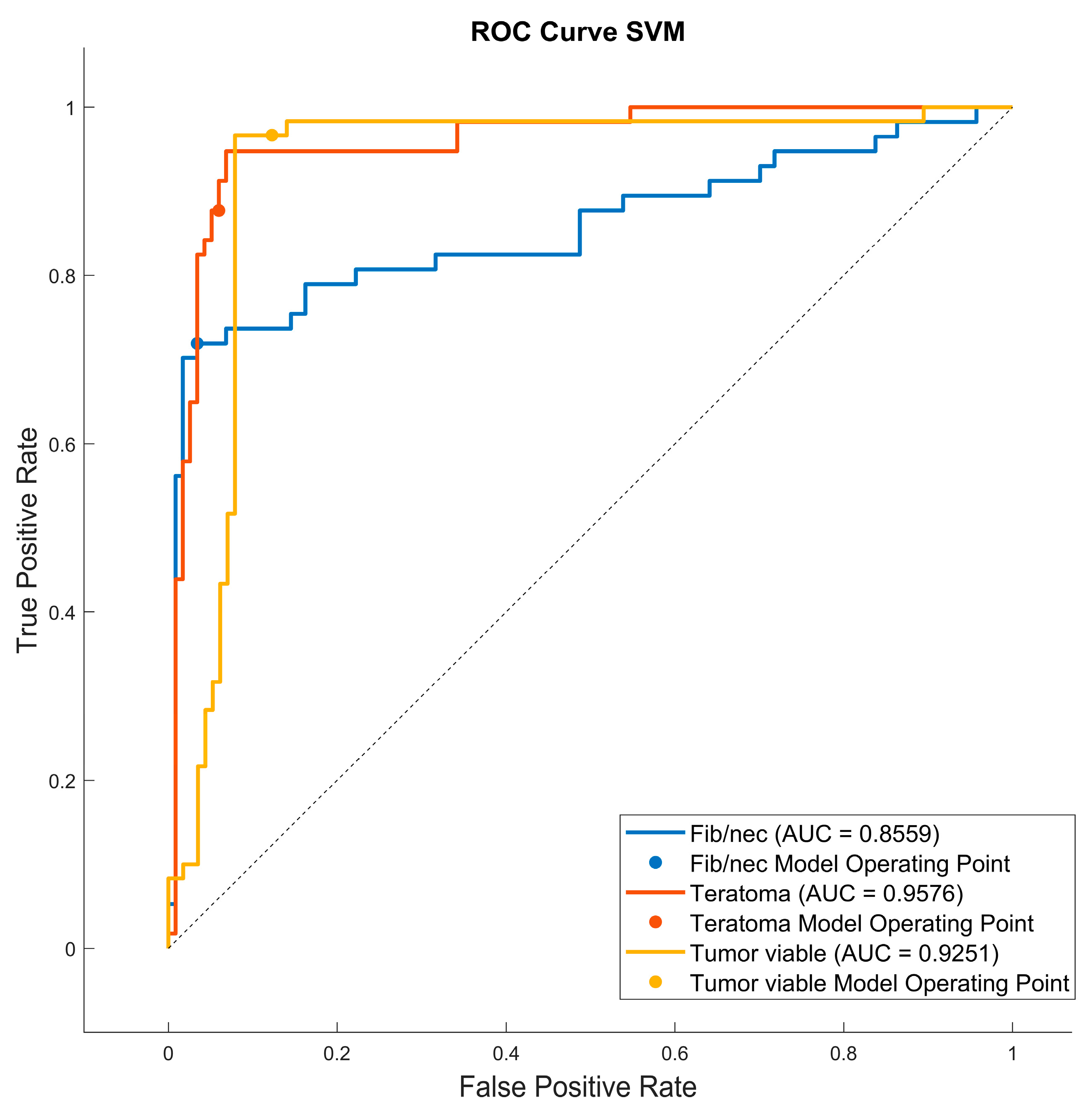
3.3. Classification
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Park, J.S.; Kim, J.; Elghiaty, A.; Ham, W.S. Recent Global Trends in Testicular Cancer Incidence and Mortality. Medicine 2018, 97, e12390. [Google Scholar] [CrossRef]
- Yazici, S.; Del Biondo, D.; Napodano, G.; Grillo, M.; Calace, F.P.; Prezioso, D.; Crocetto, F.; Barone, B. Risk Factors for Testicular Cancer: Environment, Genes and Infections—Is It All? Medicina 2023, 59, 724. [Google Scholar] [CrossRef] [PubMed]
- Scavuzzo, A.; Figueroa-Rodriguez, P.; Stefano, A.; Jimenez Guedulain, N.; Muruato Araiza, S.; de Cendejas Gomez, J.J.; Quiroz Compeaán, A.; Victorio Vargas, D.O.; Jiménez-Ríos, M.A. CT Rendering and Radiomic Analysis in Post-Chemotherapy Retroperitoneal Lymph Node Dissection for Testicular Cancer to Anticipate Difficulties for Young Surgeons. J. Imaging 2023, 9, 71. [Google Scholar] [CrossRef] [PubMed]
- Laguna, M.P.; Pizzocaro, G.; Klepp, O.; Algaba, F.; Kisbenedek, L.; Leiva, O. EAU Guidelines on Testicular Cancer. Eur. Urol. 2001, 40, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Lisson, C.S.; Manoj, S.; Wolf, D.; Schrader, J.; Schmidt, S.A.; Beer, M.; Goetz, M.; Zengerling, F.; Lisson, C.G.S. CT Radiomics and Clinical Feature Model to Predict Lymph Node Metastases in Early-Stage Testicular Cancer. Onco 2023, 3, 65–80. [Google Scholar] [CrossRef]
- Benfante, V.; Stefano, A.; Comelli, A.; Giaccone, P.; Cammarata, F.P.; Richiusa, S.; Scopelliti, F.; Pometti, M.; Ficarra, M.; Cosentino, S.; et al. A New Preclinical Decision Support System Based on PET Radiomics: A Preliminary Study on the Evaluation of an Innovative 64Cu-Labeled Chelator in Mouse Models. J. Imaging 2022, 8, 92. [Google Scholar] [CrossRef]
- Castiglioni, I.; Gilardi, M.C. Radiomics: Is It Time to Compose the Puzzle? Clin. Transl. Imaging 2018, 6, 411–413. [Google Scholar] [CrossRef]
- Russo, G.; Stefano, A.; Alongi, P.; Comelli, A.; Catalfamo, B.; Mantarro, C.; Longo, C.; Altieri, R.; Certo, F.; Cosentino, S.; et al. Feasibility on the Use of Radiomics Features of 11[C]-MET PET/CT in Central Nervous System Tumours: Preliminary Results on Potential Grading Discrimination Using a Machine Learning Model. Curr. Oncol. 2021, 28, 5318–5331. [Google Scholar] [CrossRef]
- Barone, S.; Cannella, R.; Comelli, A.; Pellegrino, A.; Salvaggio, G.; Stefano, A.; Vernuccio, F. Hybrid Descriptive-Inferential Method for Key Feature Selection in Prostate Cancer Radiomics. Appl. Stoch. Models Bus. Ind. 2021, 37, 961–972. [Google Scholar] [CrossRef]
- Pasini, G.; Bini, F.; Russo, G.; Comelli, A.; Marinozzi, F.; Stefano, A. MatRadiomics: A Novel and Complete Radiomics Framework, from Image Visualization to Predictive Model. J. Imaging 2022, 8, 221. [Google Scholar] [CrossRef]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic Minority over-Sampling Technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Pasini, G.; Stefano, A.; Russo, G.; Comelli, A.; Marinozzi, F.; Bini, F. Phenotyping the Histopathological Subtypes of Non-Small-Cell Lung Carcinoma: How Beneficial Is Radiomics? Diagnostics 2023, 13, 1167. [Google Scholar] [CrossRef] [PubMed]
- Tharwat, A.; Gaber, T.; Ibrahim, A.; Hassanien, A.E. Linear Discriminant Analysis: A Detailed Tutorial. AI Commun. 2017, 30, 169–190. [Google Scholar] [CrossRef]
- Naseri, H.; Skamene, S.; Tolba, M.; Faye, M.D.; Ramia, P.; Khriguian, J.; Patrick, H.; Andrade Hernandez, A.X.; David, M.; Kildea, J. Radiomics-Based Machine Learning Models to Distinguish between Metastatic and Healthy Bone Using Lesion-Center-Based Geometric Regions of Interest. Sci. Rep. 2022, 12, 9866. [Google Scholar] [CrossRef] [PubMed]
- Soltaninejad, S.; Keshani, M.; Tajeripour, F. Lung Nodule Detection by KNN Classifier and Active Contour Modelling and 3D Visualization. In Proceedings of the 16th CSI International Symposium on Artificial Intelligence and Signal Processing (AISP 2012), Shiraz, Iran, 2–3 May 2012; pp. 440–445. [Google Scholar] [CrossRef]
- Keshani, M.; Azimifar, Z.; Tajeripour, F.; Boostani, R. Lung Nodule Segmentation and Recognition Using SVM Classifier and Active Contour Modeling: A Complete Intelligent System. Comput. Biol. Med. 2013, 43, 287–300. [Google Scholar] [CrossRef]
- Comelli, A.; Stefano, A.; Bignardi, S.; Coronnello, C.; Russo, G.; Sabini, M.G.; Ippolito, M.; Yezzi, A. Tissue Classification to Support Local Active Delineation of Brain Tumors; Springer International Publishing: Cham, Switzerland, 2020; Volume 1065, ISBN 9783030393427. [Google Scholar]
- Park, Y.W.; Eom, J.; Kim, S.; Kim, H.; Ahn, S.S.; Ku, C.R.; Kim, E.H.; Lee, E.J.; Kim, S.H.; Lee, S.K. Radiomics With Ensemble Machine Learning Predicts Dopamine Agonist Response in Patients With Prolactinoma. J. Clin. Endocrinol. Metab. 2021, 106, e3069–e3077. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Keizer, H.J.; Fosså, S.D.; Sleijfer, D.T.; Toner, G.C.; Schraffordt Koops, H.; Mulders, P.F.; Messemer, J.E.; Ney, K.; Donohue, J.P. Prediction of Residual Retroperitoneal Mass Histology after Chemotherapy for Metastatic Nonseminomatous Germ Cell Tumor: Multivariate Analysis of Individual Patient Data from Six Study Groups. J. Clin. Oncol. 1995, 13, 1177–1187. [Google Scholar] [CrossRef]
- Vergouwe, Y.; Steyerberg, E.W.; Foster, R.S.; Sleijfer, D.T.; Fosså, S.D.; Gerl, A.; de Wit, R.; Roberts, J.T.; Habbema, J.D.F. Predicting Retroperitoneal Histology in Postchemotherapy Testicular Germ Cell Cancer: A Model Update and Multicentre Validation with More Than 1000 Patients. Eur. Urol. 2007, 51, 424–432. [Google Scholar] [CrossRef]
- Punjani, N.; Power, N.; Vanhie, J.J.; Winquist, E. Validation of a Prediction Model for Avoiding Post-Chemotherapy Retroperitoneal Lymphadenectomy in Patients with Metastatic Nonseminomatous Germ Cell Cancer. Can. Urol. Assoc. J. 2016, 10, 260–263. [Google Scholar] [CrossRef]
- Baessler, B.; Nestler, T.; Pinto dos Santos, D.; Paffenholz, P.; Zeuch, V.; Pfister, D.; Maintz, D.; Heidenreich, A. Radiomics Allows for Detection of Benign and Malignant Histopathology in Patients with Metastatic Testicular Germ Cell Tumors Prior to Post-Chemotherapy Retroperitoneal Lymph Node Dissection. Eur. Radiol. 2020, 30, 2334–2345. [Google Scholar] [CrossRef]
- Harrell, F.E., Jr.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Venishetty, N.; Taylor, J.; Xi, Y.; Howard, J.M.; Ng, Y.S.; Wong, D.; Woldu, S.L.; De Leon, A.D.; Pedrosa, I.; Margulis, V.; et al. Testicular Radiomics To Predict Pathology At Time of Postchemotherapy Retroperitoneal Lymph Node Dissection for Nonseminomatous Germ Cell Tumor. Clin. Genitourin. Cancer 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Lewin, J.; Dufort, P.; Halankar, J.; O’Malley, M.; Jewett, M.A.S.; Hamilton, R.J.; Gupta, A.; Lorenzo, A.; Traubici, J.; Nayan, M.; et al. Applying Radiomics to Predict Pathology of Postchemotherapy Retroperitoneal Nodal Masses in Germ Cell Tumors. JCO Clin. Cancer Inf. 2018, 2, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Winter, C.; Pfister, D.; Busch, J.; Bingöl, C.; Ranft, U.; Schrader, M.; Dieckmann, K.P.; Heidenreich, A.; Albers, P. Residual Tumor Size and IGCCCG Risk Classification Predict Additional Vascular Procedures in Patients with Germ Cell Tumors and Residual Tumor Resection: A Multicenter Analysis of the German Testicular Cancer Study Group. Eur. Urol. 2012, 61, 403–409. [Google Scholar] [CrossRef]
- Guidelines with Evidence Blocks. Available online: https://www.nccn.org/guidelines/guidelines-with-evidence-blocks (accessed on 21 August 2023).
- Patrikidou, A.; Cazzaniga, W.; Berney, D.; Boormans, J.; de Angst, I.; Di Nardo, D.; Fankhauser, C.; Fischer, S.; Gravina, C.; Gremmels, H.; et al. European Association of Urology Guidelines on Testicular Cancer: 2023 Update. Eur. Urol. 2023, 84, 289–301. [Google Scholar] [CrossRef]
- Wakileh, G.A.; Ruf, C.; Heidenreich, A.; Dieckmann, K.P.; Lisson, C.; Prasad, V.; Bolenz, C.; Zengerling, F. Contemporary Options and Future Perspectives: Three Examples Highlighting the Challenges in Testicular Cancer Imaging. World J. Urol. 2022, 40, 307–315. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; De Jong, E.E.C.; Van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The Bridge between Medical Imaging and Personalized Medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef]
- Ruf, C.G.; Krampe, S.; Matthies, C.; Anheuser, P.; Nestler, T.; Simon, J.; Isbarn, H.; Dieckmann, K.P. Major Complications of Post-Chemotherapy Retroperitoneal Lymph Node Dissection in a Contemporary Cohort of Patients with Testicular Cancer and a Review of the Literature. World J. Surg. Oncol. 2020, 18, 253. [Google Scholar] [CrossRef]
- Akinci D’Antonoli, T.; Cuocolo, R.; Baessler, B.; Pinto dos Santos, D. Towards Reproducible Radiomics Research: Introduction of a Database for Radiomics Studies. Eur. Radiol. 2023, 1, 1–8. [Google Scholar] [CrossRef]
- Stefano, A.; Vitabile, S.; Russo, G.; Ippolito, M.; Marletta, F.; D’Arrigo, C.; D’Urso, D.; Gambino, O.; Pirrone, R.; Ardizzone, E.; et al. A Fully Automatic Method for Biological Target Volume Segmentation of Brain Metastases. Int. J. Imaging Syst. Technol. 2016, 26, 29–37. [Google Scholar] [CrossRef]
- Castiglioni, I.; Gallivanone, F.; Soda, P.; Avanzo, M.; Stancanello, J.; Aiello, M.; Interlenghi, M.; Salvatore, M. AI-Based Applications in Hybrid Imaging: How to Build Smart and Truly Multi-Parametric Decision Models for Radiomics. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2673–2699. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fibrosis/Necrosis | Teratoma | Viable Tumor | |
|---|---|---|---|
| Patient age at diagnosis (years) | 26.03 ± 6.46 | 23.94 ± 5.95 | 28.81 ± 11.66 |
| Clinical stage (initial) | |||
| I | 2/57 (3.51%) | 7/48 (14.6%) | 9/17 (52.9%) |
| II | 20/57 (35.1%) | 16/48 (33.3%) | 6/17 (35.3%) |
| III | 35/57 (61.4%) | 25/48 (52.1%) | 2/17 (11.7%) |
| IGCCCG (initial) | |||
| Good | 14/57 (24.6%) | 15/48 (31.2%) | 5/17 (29.4%) |
| Intermediate | 26/57 (45.6%) | 19/48 (39.6%) | 7/17 (41.2%) |
| Poor | 13/57 (22.8%) | 12/48 (25.0%) | 5/17 (29.4%) |
| Missing information | 4/57 (7.0%) | 2/48 (4.2%) | 0/17 (0%) |
| Serum Marker initial | |||
| AFP | 2278 ± 7246 | 3639 ± 8481 | 5401 ± 9912 |
| hCG | 3596 ± 12,899 | 13,436 ± 40,984 | 925 ± 1331 |
| LDH | 1334 ± 2202 | 475 ± 384 | 546 ± 431 |
| Primary histopathology | |||
| Seminoma | 13/57 (22.8%) | 1/48 (0.021%) | 1/17 (0.059%) |
| Non-seminoma | 44/57 (77.2%) | 47/48 (97.9%) | 16/17 (94.12%) |
| Containing teratoma | 1/57 (0.017%) | 2/48 (0.042%) | 6/17 (35.3%) |
| Without teratoma | 56/57 (98.2%) | 46/48 (95.8%) | 11/17 (64.7%) |
| Type of pcRPLND | |||
| Primary | 2/57 (3.5%) | 0/48 (0%) | 2/17 (11.8%) |
| Standard | 8/57 (14.0%) | 10/48 (20.8%) | 0/17 (0%) |
| Salvation | 41/57 (71.9%) | 28/48 (58.3%) | 6/17 (35.3%) |
| Desperation | 5/57 (8.8%) | 9/48 (18.8%) | 5/17 (29.4%) |
| Redo | 1/57 (1.8%) | 1/48 (2.1%) | 4/17 (23.5%) |
| Serum marker prior pcRPLN | |||
| AFP | 4.0 ± 3.5 | 6.6 ± 11.8 | 56.4 ± 91.2 |
| hCG | 3.1 ± 18.5 | 5.3 ± 30.0 | 21.7 ± 83.8 |
| LDH | 195 ± 105 | 247.7 ± 170.1 | 631.3 ± 1461.3 |
| Side of orchiectomy | |||
| Left | 31/57 (54.4%) | 30/48 (62.5%) | 7/17 (41.2%) |
| Right | 19/57 (33.3%) | 16/48 (33.3%) | 9/17 (52.9%) |
| Bilateral | 2/57 (3.5%) | 1/48 (2.1%) | 1/17 (5.9%) |
| Extragonadal | 1/57 (1.8%) | 1/48 (2.1%) | 0/17 (0%) |
| Deferred | 4/57 (7%) | 0/48 (0%) | 0/17 (0%) |
| Damage to organs | |||
| Yes | 4/57 (7%) | 2/48 (4.2%) | 1/17 (5.9%) |
| No | 53/57 (93%) | 46/48 (95.8%) | 16/17 (94.1%) |
| Vascular damage | |||
| Yes | 4/57 (7%) | 7/48 (14.6%) | 2/17 (11.8%) |
| No | 53/57 (93%) | 41/48 (85.4%) | 15/17 (88.2%) |
| Volume (cm3) | 65.8 ± 132.4 | 505.4 ± 744.6 | 1156.6 ± 1689.3 |
| Selected Features | p-Value |
|---|---|
| original_firstorder_Median | <<0.005 |
| wavelet_LLH_glcm_MCC | <<0.005 |
| original_firstorder_90Percentile | <<0.005 |
| wavelet_LLL_glcm_Idmn | <<0.005 |
| wavelet_LLL_firstorder_RootMeanSquared | <<0.005 |
| wavelet_HHH_glszm_LargeAreaEmphasis | <<0.005 |
| wavelet_HLH_glszm_SmallAreaEmphasis | <<0.005 |
| wavelet_HHH_glszm_LargeAreaHighGrayLevelEmphasis | <<0.005 |
| wavelet_HHH_firstorder_Median | <<0.005 |
| wavelet_HLH_glrlm_RunLengthNonUniformityNormalized | <<0.005 |
| wavelet_LHL_glrlm_RunLengthNonUniformityNormalized | <<0.005 |
| wavelet_LLH_glcm_InverseVariance | <<0.005 |
| wavelet_LLH_gldm_SmallDependenceEmphasis | <<0.005 |
| wavelet_LLH_glszm_ZoneVariance | <<0.005 |
| wavelet_LLL_firstorder_10Percentile | <<0.005 |
| wavelet_HLH_glszm_LargeAreaEmphasis | <<0.005 |
| wavelet_HHL_firstorder_Minimum | <<0.005 |
| wavelet_LHL_glszm_SmallAreaHighGrayLevelEmphasis | <<0.005 |
| wavelet_LHH_firstorder_Range | <<0.005 |
| wavelet_LHH_glrlm_LongRunHighGrayLevelEmphasis | 0.0011 |
| wavelet_LLH_firstorder_Minimum | 0.0017 |
| wavelet_HHL_glszm_SizeZoneNonUniformityNormalized | 0.0018 |
| wavelet_HHL_glrlm_RunLengthNonUniformityNormalized | 0.0021 |
| wavelet_LLH_firstorder_Kurtosis | 0.0022 |
| wavelet_LHH_ngtdm_Complexity | 0.0028 |
| wavelet_HLH_glcm_MCC | 0.0040 |
| original_glszm_LargeAreaEmphasis | 0.0041 |
| wavelet_LHH_gldm_DependenceNonUniformity | 0.0042 |
| wavelet_HLL_firstorder_10Percentile | 0.0045 |
| wavelet_HHL_gldm_HighGrayLevelEmphasis | 0.0048 |
| Image Type | Class | Number of Features |
|---|---|---|
| Original | Shape | 0 |
| Original | First Order | 2 |
| Original | Texture | 1 |
| Wavelet | Shape | 0 |
| Wavelet | First Order | 10 |
| Wavelet | Texture | 17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scavuzzo, A.; Pasini, G.; Crescio, E.; Jimenez-Rios, M.A.; Figueroa-Rodriguez, P.; Comelli, A.; Russo, G.; Vazquez, I.C.; Araiza, S.M.; Ortiz, D.G.; et al. Radiomics Analyses to Predict Histopathology in Patients with Metastatic Testicular Germ Cell Tumors before Post-Chemotherapy Retroperitoneal Lymph Node Dissection. J. Imaging 2023, 9, 213. https://doi.org/10.3390/jimaging9100213
Scavuzzo A, Pasini G, Crescio E, Jimenez-Rios MA, Figueroa-Rodriguez P, Comelli A, Russo G, Vazquez IC, Araiza SM, Ortiz DG, et al. Radiomics Analyses to Predict Histopathology in Patients with Metastatic Testicular Germ Cell Tumors before Post-Chemotherapy Retroperitoneal Lymph Node Dissection. Journal of Imaging. 2023; 9(10):213. https://doi.org/10.3390/jimaging9100213
Chicago/Turabian StyleScavuzzo, Anna, Giovanni Pasini, Elisabetta Crescio, Miguel Angel Jimenez-Rios, Pavel Figueroa-Rodriguez, Albert Comelli, Giorgio Russo, Ivan Calvo Vazquez, Sebastian Muruato Araiza, David Gomez Ortiz, and et al. 2023. "Radiomics Analyses to Predict Histopathology in Patients with Metastatic Testicular Germ Cell Tumors before Post-Chemotherapy Retroperitoneal Lymph Node Dissection" Journal of Imaging 9, no. 10: 213. https://doi.org/10.3390/jimaging9100213