
Association between Fractional Oxygen Extraction from Resting Quadriceps Muscle and Body Composition in Healthy Men
 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Participants
2.3. Evaluations
2.4. Body Composition
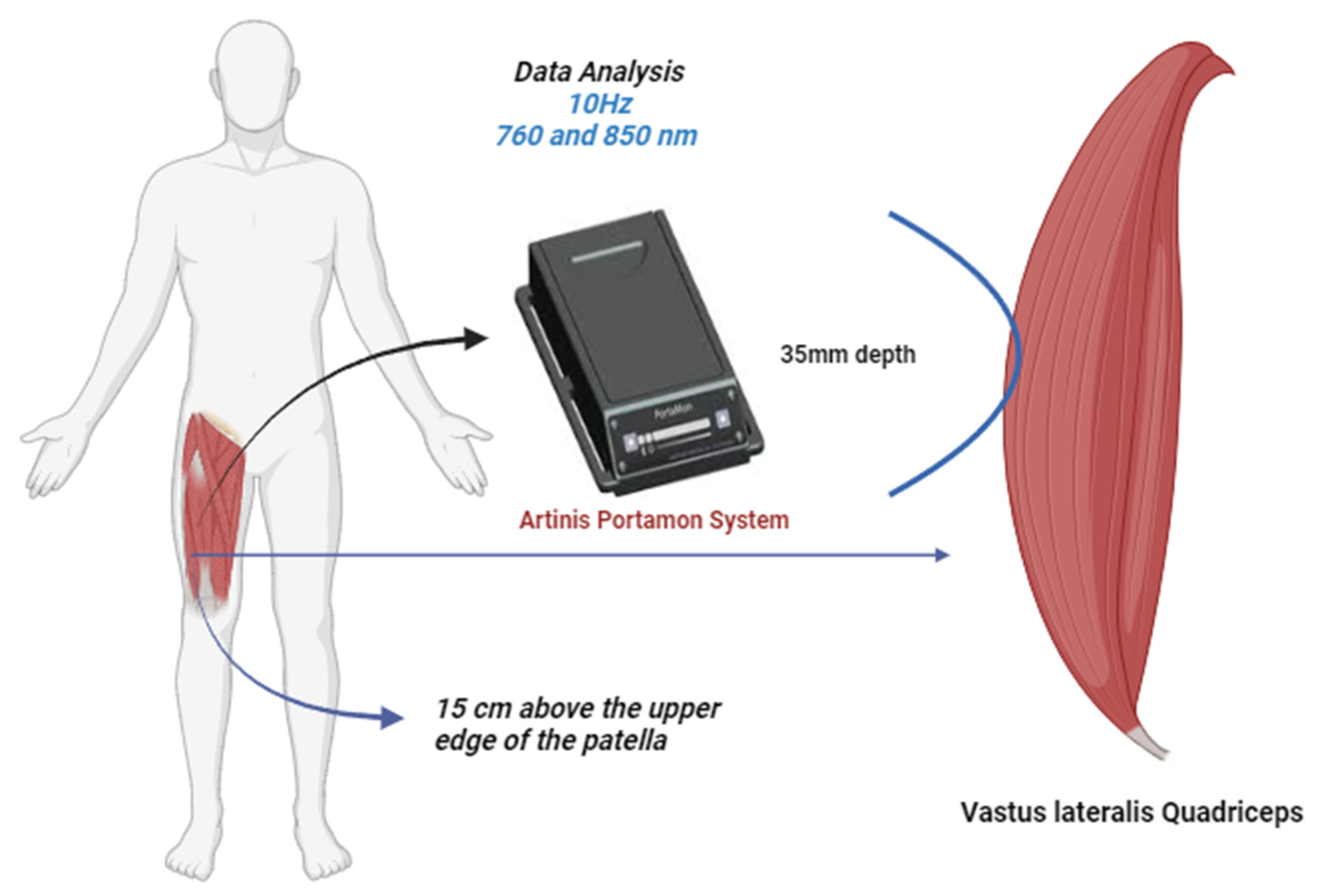
2.5. Muscle Resaturation with NIRS
2.6. Muscle VO2 and the Area above the Curve of HHb
2.7. Data Analysis
2.8. Statistical Analysis
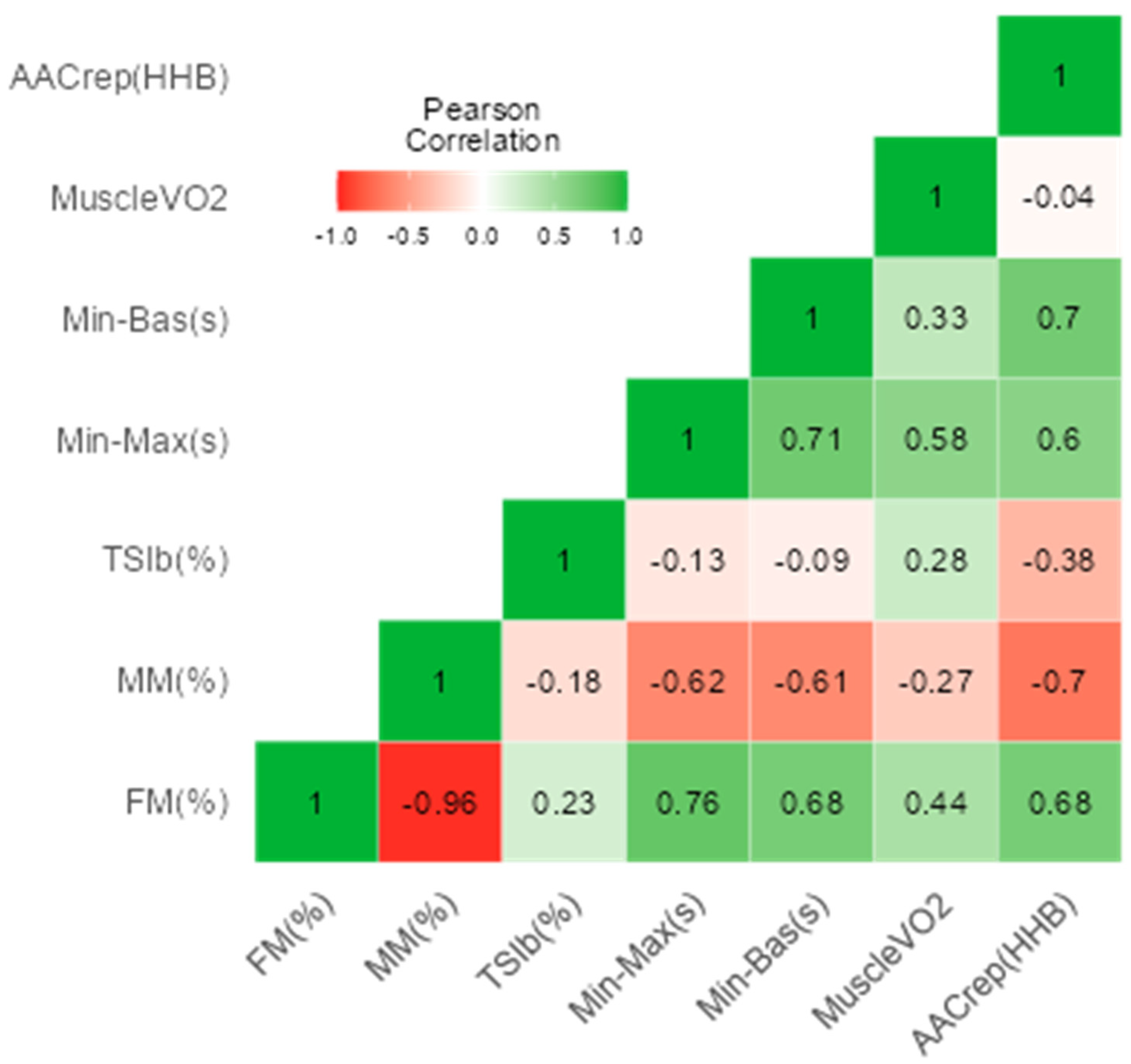
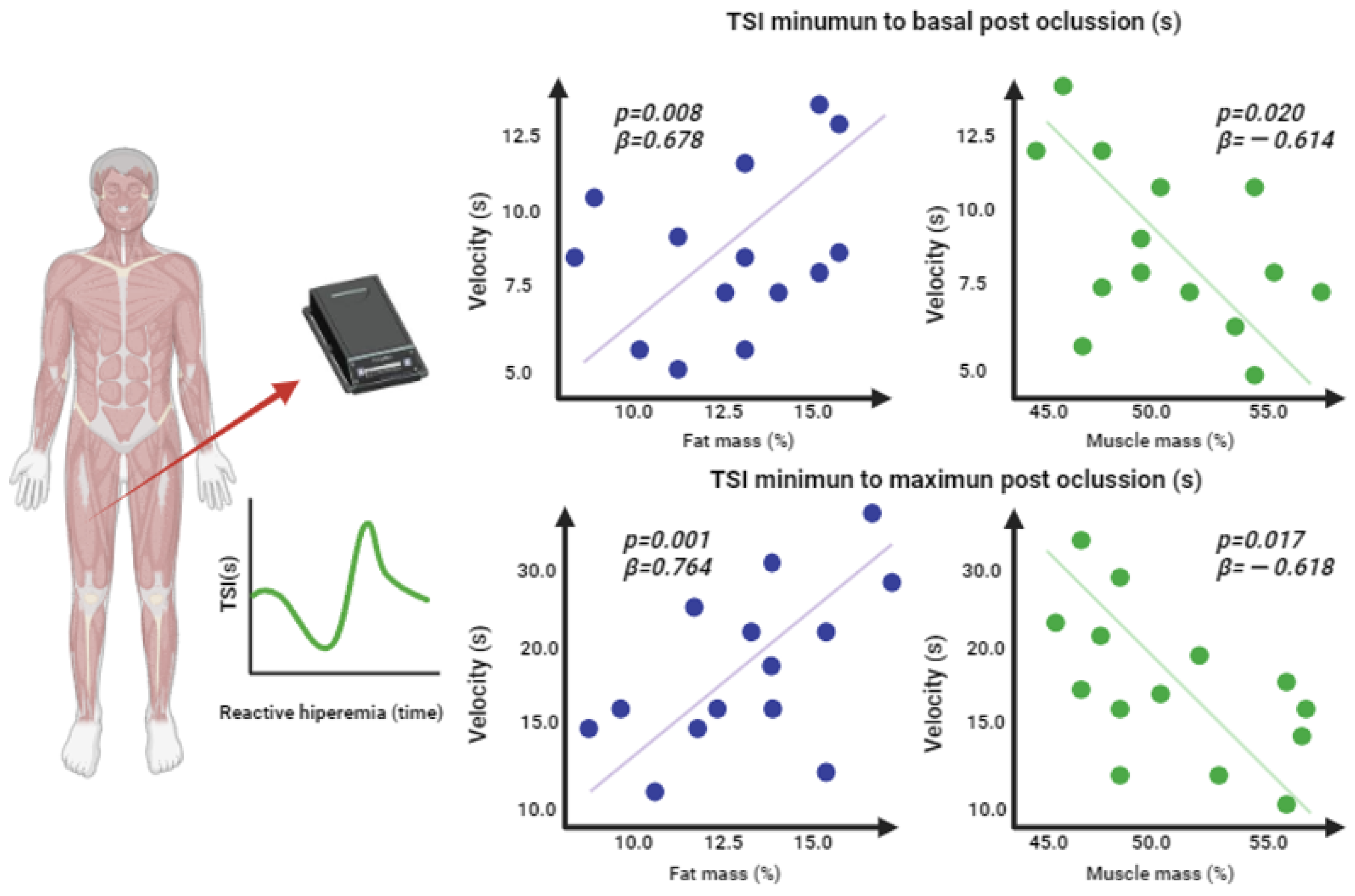
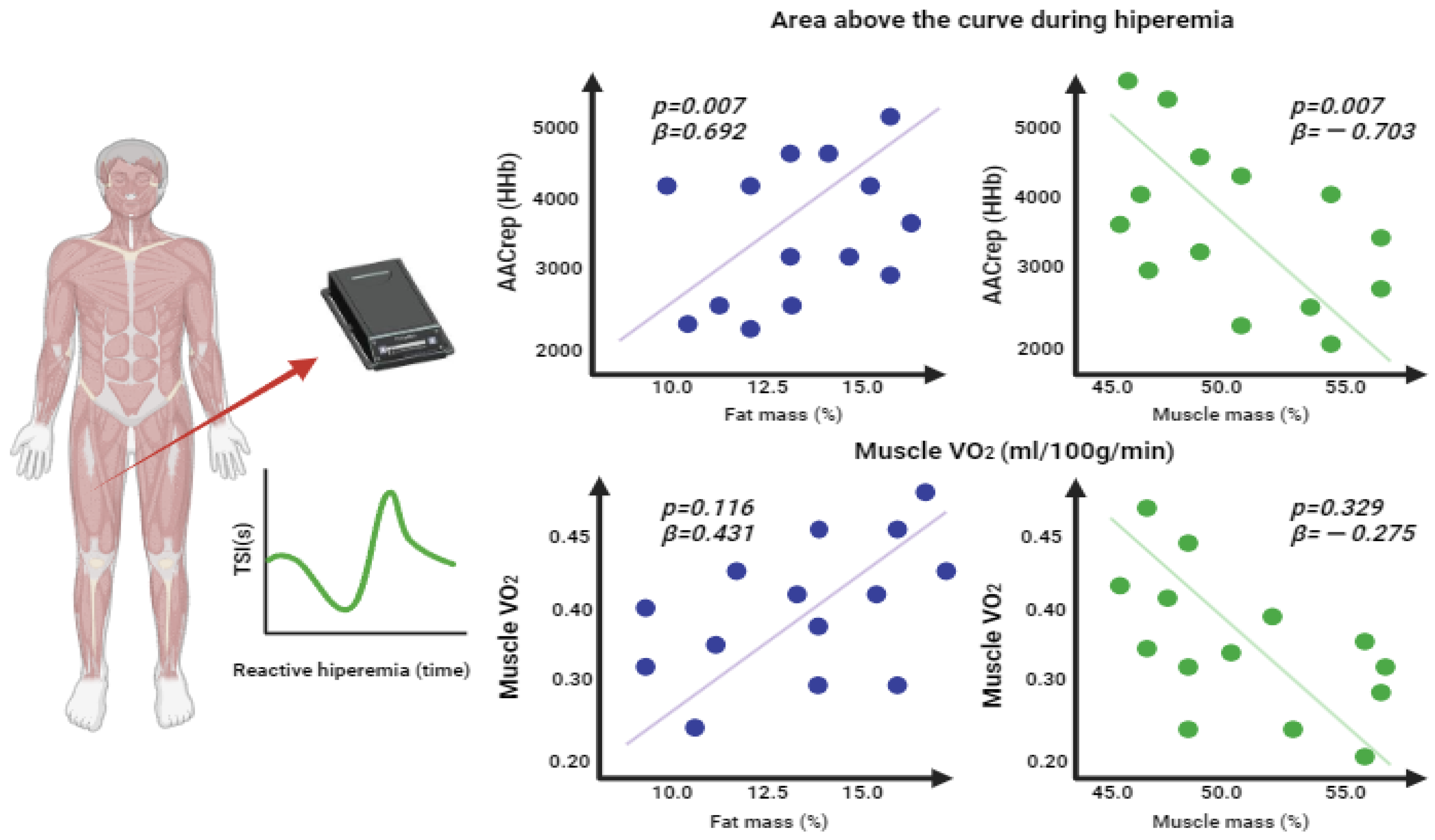
3. Results
4. Discussion
4.1. Hyperemia Reactive Response
4.2. Relationship between Adipose and Muscle Mass with the Hyperemic Response
4.3. Clinical Implications
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pietiläinen, K.H.; Kaprio, J.; Borg, P.; Plasqui, G.; Yki-Järvinen, H.; Kujala, U.M.; Rose, R.J.; Westerterp, K.R.; Rissanen, A. Physical inactivity and obesity: A vicious circle. Obesity 2008, 16, 409–414. [Google Scholar] [PubMed]
- Katzmarzyk, P.; Friedenreich, C.; Shiroma, E.J.; Lee, I. Physical inactivity and non-communicable disease burden in low-income, middle-income and high-income countries. Br. J. Sports Med. 2022, 56, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Widmer, R.; Lerman, A. Endothelial dysfunction and cardiovascular disease. Glob. Cardiol. Sci. Pract. 2014, 2014, 291–308. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, G.; Volino-Souza, M.; Leitão, R.; Pinheiro, V.; Conte-Júnior, C.A.; Alvares, T. Suitability of the muscle O2 resaturation parameters most used for assessing reactive hyperemia: A near-infrared spectroscopy study. J. Vasc. Bras. 2021, 20, e20200143. [Google Scholar] [CrossRef] [PubMed]
- Samolyuk, M.; Grigorieva, N. Evaluation of endothelial dysfunction and the possibility of its correction at the present stage in patients with cardiovascular diseases. Kardiologiia 2019, 59, 4–9. (In Russian) [Google Scholar] [CrossRef]
- Desanlis, J.; Gordon, D.; Calveyrac, C.; Cottin, F.; Gernigon, M. Intra- and Inter-Day Reliability of the NIRS Portamon Device after Three Induced Muscle Ischemias. Sensors 2022, 22, 5165. [Google Scholar] [CrossRef]
- Vasquez-Bonilla, A.; Camacho-Cardeñosa, A.; Timón, R.; Martínez-Guardado, I.; Camacho-Cardeñosa, M.; Olcina, G. Muscle Oxygen Desaturation and Re-Saturation Capacity Limits in Repeated Sprint Ability Performance in Women Soccer Players: A New Physiological Interpretation. Int. J. Environ. Res. Public Health 2021, 18, 3484. [Google Scholar] [CrossRef]
- Hesford, C.; Laing, S.; Cardinale, M.; Cooper, C. Asymmetry of quadriceps muscle oxygenation during elite short-track speed skating. Med. Sci. Sports Exerc. 2012, 44, 501–508. [Google Scholar] [CrossRef]
- Tuesta, M.; Yáñez-Sepúlveda, R.; Verdugo-Marchese, H.; Mateluna, C.; Alvear-Ordenes, I. Near-Infrared Spectroscopy Used to Assess Physiological Muscle Adaptations in Exercise Clinical Trials: A Systematic Review. Biology 2022, 11, 1073. [Google Scholar]
- Grassi, B.; Quaresima, V. Near-infrared spectroscopy and skeletal muscle oxidative function in vivo in health and disease: A review from an exercise physiology perspective. J. Biomed. Optics 2016, 21, 091313. [Google Scholar] [CrossRef]
- Perrey, S.; Ferrari, M. Muscle Oximetry in Sports Science: A Systematic Review. Sports Med. 2018, 48, 597–616. [Google Scholar] [PubMed]
- Rosenberry, R.; Nelson, M. Reactive hyperemia: A review of methods, mechanisms, and considerations. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2020, 318, R605–R618. [Google Scholar] [CrossRef] [PubMed]
- Rosenberry, R.; Munson, M.; Chung, S.; Samuel, T.; Patik, J.; Tucker, W.; Haykowsky, M.; Nelson, M. Age-related microvascular dysfunction: Novel insight from near-infrared spectroscopy. Exp. Physiol. 2018, 103, 190–200. [Google Scholar] [CrossRef]
- Dellinger, J.R.; Figueroa, A.; Gonzales, J. Reactive hyperemia half-time response is associated with skeletal muscle oxygen saturation changes during cycling exercise. Microvasc. Res. 2023, 149, 104569. [Google Scholar] [CrossRef]
- Paine, N.; Hinderliter, A.; Blumenthal, J.; Adams, K.F.; Sueta, C., Jr.; Chang, P.; O’Connor, C.; Sherwood, A. Reactive hyperemia is associated with adverse clinical outcomes in heart failure. Am. Heart J. 2016, 178, 108–114. [Google Scholar] [CrossRef]
- Townsend, D.; Deysher, D.; Wu, E.; Barstow, T. Reduced insulin sensitivity in young, normoglycaemic subjects alters microvascular tissue oxygenation during postocclusive reactive hyperaemia. Exp. Physiol. 2019, 104, 967–974. [Google Scholar] [CrossRef]
- Soares, R.; George, M.; Proctor, D.; Murias, J. Differences in vascular function between trained and untrained limbs assessed by near-infrared spectroscopy. Eur. J. Appl. Physiol. 2018, 118, 2241–2248. [Google Scholar] [CrossRef]
- Jones, S.; Tillin, T.; Williams, S.; Rapala, A.; Chaturvedi, N.; Hughes, A. Skeletal Muscle Tissue Saturation Changes Measured Using Near Infrared Spectroscopy During Exercise Are Associated with Post-Occlusive Reactive Hyperaemia. Front. Physiol. 2022, 13, 919754. [Google Scholar] [CrossRef]
- Shivgulam, M.; Liu, H.; Schwartz, B.; Langley, J.; Bray, N.; Kimmerly, D.; O’Brien, M. Impact of Exercise Training Interventions on Flow-Mediated Dilation in Adults: An Umbrella Review. Sports Med. 2023, 53, 1161–1174. [Google Scholar]
- Song, B.; Azhar, L.; Koo, G.; Marzolini, S.; Gallagher, D.; Swardfager, W.; Chen, C.; Ba, J.; Herrmann, N.; Lanctôt, K. The effect of exercise on blood concentrations of angiogenesis markers in older adults: A systematic review and meta-analysis. Res. Sq. 2023. [Google Scholar] [CrossRef]
- Lim, A.; Chen, Y.; Hsu, C.; Fu, T.; Wang, J. The Effects of Exercise Training on Mitochondrial Function in Cardiovascular Diseases: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2022, 23, 12559. [Google Scholar] [CrossRef] [PubMed]
- Niebauer, J.; Cooke, J. Cardiovascular effects of exercise: Role of endothelial shear stress. J. Am. Coll. Cardiol. 1996, 28, 1652–1660. [Google Scholar] [PubMed]
- Kajikawa, M.; Higashi, Y. Obesity and Endothelial Function. Biomedicines 2022, 10, 1745. [Google Scholar]
- Dvoretskiy, S.; Lieblein-Boff, J.; Jonnalagadda, S.; Atherton, P.; Phillips, B.; Pereira, S. Exploring the Association between Vascular Dysfunction and Skeletal Muscle Mass, Strength and Function in Healthy Adults: A Systematic Review. Nutrients 2020, 12, 715. [Google Scholar] [CrossRef]
- Ren, Z.; Fu, L.; Feng, Z.; Song, Z.; Liu, Y.; Zhang, T.; Wu, N. Skeletal muscle mass is a strong predictor of cardiorespiratory fitness in the Chinese population with obesity. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 1407–1414. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Med. A 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Aandstad, A.; Holtberget, K.; Hageberg, R.; Holme, I.; Anderssen, S. Validity and reliability of bioelectrical impedance analysis and skinfold thickness in predicting body fat in military personnel. Mil. Med. 2014, 179, 208–217. [Google Scholar] [CrossRef]
- Sanni, A.; McCully, K. Interpretation of Near-Infrared Spectroscopy (NIRS) Signals in Skeletal Muscle. J. Funct. Morphol. Kinesiol. 2019, 4, 28. [Google Scholar] [CrossRef]
- Paradis-Deschênes, P.; Joanisse, D.; Mauriège, P.; Billaut, F. Ischemic Preconditioning Enhances Aerobic Adaptations to Sprint-Interval Training in Athletes Without Altering Systemic Hypoxic Signaling and Immune Function. Front. Sports Act. Living 2020, 2, 41. [Google Scholar] [CrossRef]
- Malagoni, A.M.; Felisatti, M.; Mandini, S.; Mascoli, F.; Manfredini, R.; Basaglia, N.; Zamboni, P.; Manfredini, F. Resting muscle oxygen consumption by near-infrared spectroscopy in peripheral arterial disease: A parameter to be considered in a clinical setting? Angiology 2010, 61, 530–536. [Google Scholar] [CrossRef]
- Soares, R.N.; McLay, K.M.; George, M.A.; Murias, J.M. Differences in oxidative metabolism modulation induced by ischemia/reperfusion between trained and untrained individuals assessed by NIRS. Physiol. Rep. 2017, 5, e13384. [Google Scholar] [CrossRef]
- Barstow, T. Understanding near infrared spectroscopy and its application to skeletal muscle research. J. Appl. Physiol. 2019, 126, 1360–1376. [Google Scholar] [CrossRef]
- Hopkins, W.; Marshall, S.; Batterham, A.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef]
- Pinheiro, V.; da Silva Tavares, A.; Volino-Souza, M.; de Oliveira, G.; Alvares, T. Association between Femoral Artery Flow-Mediated Dilation and Muscle Oxygen Saturation Parameters in Healthy, Young Individuals. J. Cardiovasc. Dev. 2023, 10, 63. [Google Scholar] [CrossRef]
- De Boer, M.; Sern, E.; Smulders, Y.; Eringa, E.; Meijer, R. Phenotyping the microcirculation with contrast-enhanced ultrasound. Hypertension 2012, 60, e38. [Google Scholar] [CrossRef]
- Alvares, T.; Oliveira, G.; Soares, R.; Murias, J. Near-infrared spectroscopy-derived total haemoglobin as an indicator of changes in muscle blood flow during exercise-induced hyperaemia. J. Sports Sci. 2020, 38, 751–758. [Google Scholar] [CrossRef]
- Zuccarelli, L.; do Nascimento Salvador, P.; Del Torto, A.; Fiorentino, R.; Grassi, B. Skeletal muscle o2 kinetics by the NIRS repeated occlusions method during the recovery from cycle ergometer exercise. J. Appl. Physiol. 2020, 128, 534–544. [Google Scholar] [CrossRef]
- d’El-Rei, J.; Cunha, M.; Mattos, S.; Marques, B.; Menezes, V.; Cunha, A.; França, É.; Oigman, W.; Neves, M. Microvascular Reactivity in Hypertensive Patients with High Body Adiposity. Estudo da Reatividade Microvascular em Pacientes Hipertensos com Adiposidade Corporal Elevada. Arq. Bras. Cardiol. 2020, 115, 896–904. [Google Scholar] [CrossRef]
- Gu, P.; Xu, A. Interplay between adipose tissue and blood vessels in obesity and vascular dysfunction. Rev. Endocr. Metab. Disord. 2013, 14, 49–58. [Google Scholar]
- Mirza, I.; Mohamed, A.; Deen, H.; Balaji, S.; Elsabbahi, D.; Munasser, A.; Naquiallah, D.; Abdulbaseer, U.; Hassan, C.; Masrur, M.; et al. Obesity-Associated Vitamin D Deficiency Correlates with Adipose Tissue DNA Hypomethylation, Inflammation, and Vascular Dysfunction. Int. J. Mol. Sci. 2022, 23, 14377. [Google Scholar] [CrossRef]
- Vasquez-Bonilla, A.; Brazo-Sayavera, J.; Timon, R.; Olcina, G. Measurement of resting muscle oxygenation and the relationship with countermovement jumps and body composition in soccer players. Cult. Cienc. Deporte 2021, 16, 215–223. [Google Scholar]
- Keller, J.; Traylor, M.; Gray, S.; Hill, E.; Weir, J. Sex differences in NIRS-derived values of reactive hyperemia persist after experimentally controlling for the ischemic vasodilatory stimulus. J. Appl. Phys. 2023, 135, 3–14. [Google Scholar] [CrossRef]
- van Beekvelt, M.; Borghuis, M.; van Engelen, B.; Wevers, R.; Colier, W. Adipose tissue thickness affects in vivo quantitative near-IR spectroscopy in human skeletal muscle. Clin. Sci. 2001, 101, 21–28. [Google Scholar] [CrossRef]
- McManus, C.; Collison, J.; Cooper, C. Performance comparison of the MOXY and PortaMon near-infrared spectroscopy muscle oximeters at rest and during exercise. J. Biomed. Opt. 2018, 23, 015007. [Google Scholar] [CrossRef]
- Vasquez-Bonilla, A.; Tomas-Carus, P.; Brazo-Sayavera, J.; Malta, J.; Folgado, H.; Olcina, G. Muscle oxygenation is associated with bilateral strength asymmetry during isokinetic testing in sport teams. Sci. Sports 2023, 38, 426.e1–426.e9. [Google Scholar] [CrossRef]
- Koutlas, A.; Smilios, I.; Kokkinou, E.; Myrkos, A.; Kounoupis, A.; Dipla, K.; Zafeiridis, A. NIRS-Derived Muscle-Deoxygenation and Microvascular Reactivity During Occlusion-Reperfusion at Rest Are Associated with Whole-Body Aerobic Fitness. Res. Q. Exerc. Sport 2023, 1–13. [Google Scholar] [CrossRef]
- Ryan, T.E.; Erickson, M.L.; Brizendine, J.T.; Young, H.J.; McCully, K.K. Noninvasive evaluation of skeletal muscle mitochondrial capacity with near-infrared spectroscopy: Correcting for blood volume changes. J. Appl. Physiol. 2012, 113, 175–183. [Google Scholar] [CrossRef]
- Soares, R.N.; Reimer, R.A.; Doyle-Baker, P.K.; Murias, J.M. Metabolic inflexibility in individuals with obesity assessed by near-infrared spectroscopy. Diabetes Vasc. Dis. Res. 2017, 14, 502–509. [Google Scholar] [CrossRef]
- Tryfonos, A.; Tzanis, G.; Pitsolis, T.; Karatzanos, E.; Koutsilieris, M.; Nanas, S.; Philippou, A. Exercise Training Enhances Angiogenesis-Related Gene Responses in Skeletal Muscle of Patients with Chronic Heart Failure. Cells 2021, 10, 1915. [Google Scholar] [CrossRef]
- Gorski, T.; De Bock, K. Metabolic regulation of exercise-induced angiogenesis. Vasc. Biol. 2019, 1, H1–H8. [Google Scholar]
- Green, D.J.; Jones, H.; Thijssen, D.; Cable, N.T.; Atkinson, G. Flow-mediated dilation and cardiovascular event prediction: Does nitric oxide matter? Hypertension 2011, 57, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Kim, J.H. Impact of Skeletal Muscle Mass on Metabolic Health. Endocrinol. Metab. 2020, 35, 1–6. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean | SD | 95% CI | ||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Age (years) | 26.9 | ± | 2.4 | 25.4 | 28.3 |
| Weight (kg) | 74.8 | ± | 5.9 | 71.3 | 78.2 |
| Height (m) | 1.74 | ± | 0.05 | 1.70 | 1.77 |
| BMI (weight/height2) | 24.83 | ± | 1.74 | 23.83 | 25.83 |
| Fat mass (%) | 12.16 | ± | 4.09 | 9.79 | 14.52 |
| Muscle mass (%) | 50.25 | ± | 2.83 | 48.61 | 51.89 |
| Fat mass, right leg (kg) | 1.87 | ± | 0.42 | 1.63 | 2.11 |
| Muscle mass, right leg (kg) | 11.15 | ± | 1.15 | 10.48 | 11.82 |
| Heart rate (bpm) | 53.2 | ± | 6.3 | 49.5 | 56.9 |
| Systolic pressure (mmHg) | 126.00 | ± | 10.66 | 119.84 | 132.16 |
| Diastolic pressure (mmHg) | 73.93 | ± | 7.80 | 69.42 | 78.43 |
| TSI Baseline (%) | 68.5 | ± | 2.91 | 66.9 | 70.2 |
| MuscleVO2 (mL/100 g/min) | 0.30 | ± | 0.08 | 0.26 | 0.35 |
| Minimum to maximum post-occlusion time (s) | 18.54 | ± | 5.01 | 15.65 | 21.43 |
| Minimum to baseline post-occlusion time (s) | 8.31 | ± | 3.08 | 6.53 | 10.09 |
| AACrep (HHb) | 3842 | ± | 979 | 3276 | 4407 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yáñez-Sepúlveda, R.; Olivares-Arancibia, J.; Cortés-Roco, G.; Vasquez-Bonilla, A.; Monsalves-Álvarez, M.; Alvear-Órdenes, I.; Tuesta, M. Association between Fractional Oxygen Extraction from Resting Quadriceps Muscle and Body Composition in Healthy Men. J. Funct. Morphol. Kinesiol. 2023, 8, 149. https://doi.org/10.3390/jfmk8040149
Yáñez-Sepúlveda R, Olivares-Arancibia J, Cortés-Roco G, Vasquez-Bonilla A, Monsalves-Álvarez M, Alvear-Órdenes I, Tuesta M. Association between Fractional Oxygen Extraction from Resting Quadriceps Muscle and Body Composition in Healthy Men. Journal of Functional Morphology and Kinesiology. 2023; 8(4):149. https://doi.org/10.3390/jfmk8040149
Chicago/Turabian StyleYáñez-Sepúlveda, Rodrigo, Jorge Olivares-Arancibia, Guillermo Cortés-Roco, Aldo Vasquez-Bonilla, Matías Monsalves-Álvarez, Ildefonso Alvear-Órdenes, and Marcelo Tuesta. 2023. "Association between Fractional Oxygen Extraction from Resting Quadriceps Muscle and Body Composition in Healthy Men" Journal of Functional Morphology and Kinesiology 8, no. 4: 149. https://doi.org/10.3390/jfmk8040149