Active Smoking Before Liver Transplantation in Patients with Alcohol Use Disorder: Risk Factors and Outcomes

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
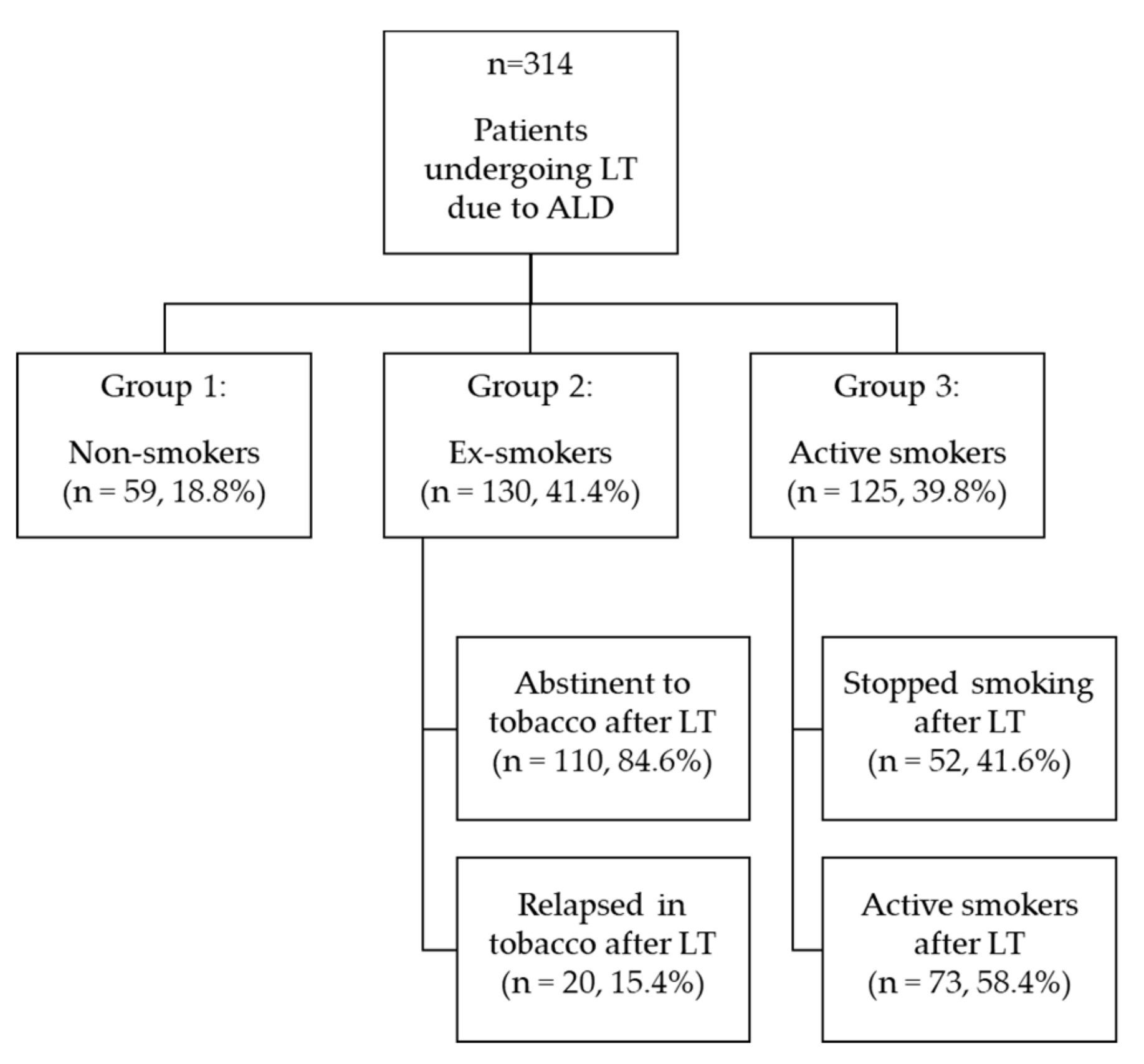
2.1. Participants and Procedure
2.2. Data Analysis
2.3. Ethical Issues
3. Results
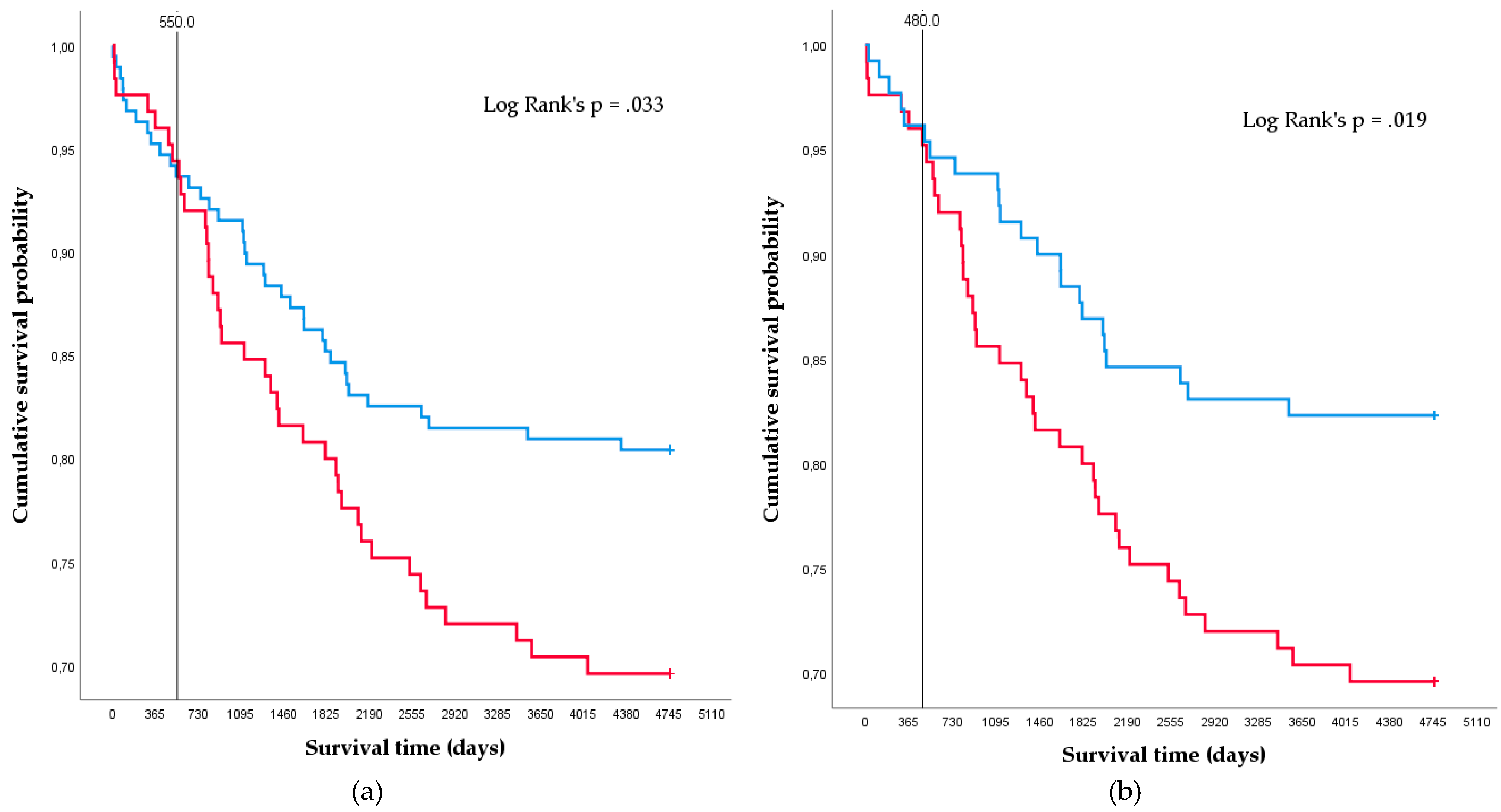
3.1. Smoking Status at LT and Outcomes
3.2. Factors Associated With Active Smoking Before LT
3.3. Factors Associated With Active Smoking After LT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO Tobacco. Available online: https://www.who.int/news-room/fact-sheets/detail/tobacco (accessed on 27 February 2020).
- Mills, E.; Eyawo, O.; Lockhart, I.; Kelly, S.; Wu, P.; Ebbert, J.O. Smoking cessation reduces postoperative complications: A systematic review and meta-analysis. Am. J. Med. 2011, 124, 144–154. [Google Scholar] [CrossRef]
- Liu, B.; Balkwill, A.; Roddam, A.; Brown, A.; Beral, V. Million women study collaborators separate and joint effects of alcohol and smoking on the risks of cirrhosis and gallbladder disease in middle-aged women. Am. J. Epidemiol. 2009, 169, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Dam, M.K.; Flensborg-Madsen, T.; Eliasen, M.; Becker, U.; Tolstrup, J.S. Smoking and risk of liver cirrhosis: A population-based cohort study. Scand. J. Gastroenterol. 2013, 48, 585–591. [Google Scholar] [CrossRef]
- van der Heide, F.; Dijkstra, G.; Porte, R.J.; Kleibeuker, J.H.; Haagsma, E.B. Smoking behavior in liver transplant recipients. Liver transplantation. AASLD 2009, 15, 648–655. [Google Scholar] [CrossRef]
- Lucey, M.R. Alcohol-associated cirrhosis. Clin. Liver Dis. 2019, 23, 115–126. [Google Scholar] [CrossRef]
- Bataller, R.; Cabezas, J.; Aller, R.; Ventura-Cots, M.; Abad, J.; Albillos, A.; Altamirano, J.; Arias-Loste, M.T.; Bañares, R.; Caballería, J.; et al. Alcohol-related liver disease. Clinical practice guidelines. Consensus document sponsored by AEEH. Gastroenterol. Hepatol. 2019, 42, 657–676. [Google Scholar] [CrossRef] [PubMed]
- Daniel, K.E.; Eickhoff, J.; Lucey, M.R. Why do patients die after a liver transplantation? Clin. Transplant. 2017, 31, e12906. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Wang, Y.; Ma, T.; Liu, X.; Wang, B.; Wu, Z.; Lv, Y.; Wu, R. Impact of cigarette smoking on early complications after liver transplantation: A single-center experience and a meta-analysis. PLoS ONE 2017, 12, e0178570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleetwood, V.A.; Hertl, M.; Chan, E.Y. Liver transplantation to the active smoker: Transplant provider opinions and how they have changed: Transplantation in smokers: A survey. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2015, 19, 2223–2227. [Google Scholar] [CrossRef] [PubMed]
- DiMartini, A.; Javed, L.; Russell, S.; Dew, M.A.; Fitzgerald, M.G.; Jain, A.; Fung, J. Tobacco use following liver transplantation for alcoholic liver disease: An underestimated problem. Liver Transplant. 2005, 11, 679–683. [Google Scholar] [CrossRef] [PubMed]
- Ehlers, S.L.; Rodrigue, J.R.; Widows, M.R.; Reed, A.I.; Nelson, D.R. Tobacco use before and after liver transplantation: A single center survey and implications for clinical practice and research. Liver Transplant. 2004, 10, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Lligoña, A.; Freixa, N.; Bataller, R.; Monràs, M.; Rimola, A. Clinical guideline for the evaluation of liver transplant candidates with addictions. Gastroenterol. Hepatol. 2009, 32, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Lombardo-Quezada, J.; Colmenero, J.; López-Pelayo, H.; Gavotti, C.; Lopez, A.; Crespo, G.; Lopez, E.; Gual, A.; Lligoña, A.; Navasa, M. Prediction of alcohol relapse among liver transplant candidates with less than 6 months of abstinence using the high-risk alcoholism relapse score. Liver Transplant. Off. Publ. Am. Assoc. Study Liver Dis. Int. Liver Transplant. Soc. 2019, 25, 1142–1154. [Google Scholar] [CrossRef]
- Carrión, J.A.; Navasa, M.; Bosch, J.; Bruguera, M.; Gilabert, R.; Forns, X. Transient elastography for diagnosis of advanced fibrosis and portal hypertension in patients with hepatitis C recurrence after liver transplantation. Liver Transplant. 2006, 12, 1791–1798. [Google Scholar] [CrossRef] [PubMed]
- Ursic-Bedoya, J.; Donnadieu-Rigole, H.; Faure, S.; Pageaux, G.P. Alcohol use and smoking after liver transplantation; complications and prevention. Best Pract. Res. Clin. Gastroenterol. 2017, 31, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Mangus, R.S.; Fridell, J.A.; Kubal, C.A.; Loeffler, A.L.; Krause, A.A.; Bell, J.A.; Tiwari, S.; Tector, J. Worse long-term patient survival and higher cancer rates in liver transplant recipients with a history of smoking. Transplantation 2015, 99, 1862–1868. [Google Scholar] [CrossRef]
- Leithead, J.A.; Ferguson, J.W.; Hayes, P.C. Smoking-related morbidity and mortality following liver transplantation. Liver Transplant. 2008, 14, 1159–1164. [Google Scholar] [CrossRef]
- Lee, D.S.; Mathur, A.K.; Acker, W.B.; Al-Holou, S.N.; Ehrlichman, L.K.; Lewin, S.A.; Nguyen, C.K.B.; Peterson, S.F.; Ranney, D.N.; Sell, K.; et al. Effects of Smoking on survival for patients with end-stage liver disease. J. Am. Coll. Surg. 2009, 208, 1077–1084. [Google Scholar] [CrossRef]
- Renaud, L.; Hilleret, M.N.; Thimonier, E.; Guillaud, O.; Arbib, F.; Ferretti, G.; Jankowski, A.; Chambon-Augoyard, C.; Erard-Poinsot, D.; Decaens, T.; et al. De novo malignancies screening after liver transplantation for alcoholic liver disease: A comparative opportunistic study. Liver Transplant. 2018, 24, 1690–1698. [Google Scholar] [CrossRef] [Green Version]
- Watt, K.D.S.; Pedersen, R.A.; Kremers, W.K.; Heimbach, J.K.; Sanchez, W.; Gores, G.J. Long-term probability of and mortality from de novo malignancy after liver transplantation. Gastroenterology 2009, 137, 2010–2017. [Google Scholar] [CrossRef] [Green Version]
- Rademacher, S.; Seehofer, D.; Eurich, D.; Schoening, W.; Neuhaus, R.; Oellinger, R.; Denecke, T.; Pascher, A.; Schott, E.; Sinn, M.; et al. The 28-year incidence of de novo malignancies after liver transplantation: A single-center analysis of risk factors and mortality in 1616 patients. Liver Transplant. 2017, 23, 1404–1414. [Google Scholar] [CrossRef] [PubMed]
- Mukthinuthalapati, P.K.; Gotur, R.; Ghabril, M. Incidence, risk factors and outcomes of de novo malignancies post liver transplantation. World J. Hepatol. 2016, 8, 533–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, N.C.; Chen, Y.L.; Tsai, K.Y. Head and neck cancer in living donor liver transplant recipients: Single center retrospective study. Medicine 2019, 98, e16701. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.J. Failure to treat tobacco use in mental health and addiction treatment settings: A form of harm reduction? Drug Alcohol Depend. 2010, 110, 177–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cote, D.R.; Chirichella, T.J.; Noon, K.A.; Shafran, D.M.; Augustine, J.J.; Schulak, J.A.; Sanchez, E.Q.; Woodside, K.J. Abdominal organ transplant center tobacco use policies vary by organ program type. Transplant. Proc. 2016, 48, 1920–1926. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total (n = 314) | Group 1: Non-Smokers (n = 59) | Group 2: Ex-Smokers (n = 130) | Group 3: Active Smokers (n = 125) | p | |
|---|---|---|---|---|---|
| Male | 283 (90.1%) | 50 (17.7%) | 119 (42.0%) | 114 (40.3%) | 0.30 |
| Age, Years (SD) | 55.48 (7.47) | 56.31 (7.53) | 57.50 (6.67) | 53.00 (7.59) | 0.00 |
| MELD (SD) | 16.89 (6.50) | 18.05 (7.15) | 15.83 (6.03) | 17.43 (6.54) | 0.04 |
| Liver-Kidney | 11 (3.6%) | 2 (18.2%) | 8 (72.7%) | 1 (9.1%) | 0.07 |
| HCV | 127 (40.4%) | 17 (13.4%) | 43 (33.9%) | 67 (52.8%) | 0.00 |
| HBV | 13 (4.1%) | 2 (15.4%) | 5 (38.5%) | 6 (46.2%) | 0.88 |
| HCC | 130 (41.4%) | 21 (16.2%) | 58 (44.6%) | 51 (39.2%) | 0.49 |
| HIV | 12 (3.8%) | 2 (16.7%) | 6 (50.0%) | 4 (33.3%) | 0.83 |
| Good Family Support | 261 (86.1%) | 54 (20.7%) | 115 (44.1%) | 92 (35.2%) | 0.02 |
| Unstable Family Support | 41 (13.6%) | 4 (9.8%) | 14 (34.1%) | 23 (56.1%) | 0.03 |
| Living Donor | 22 (7.1%) | 4 (18.2%) | 9 (40.9%) | 9 (40.9%) | 0.99 |
| Alcohol Abstinence Before LT 1–C6 Months | 60 (19.1%) | 12 (20.0%) | 21 (35.0%) | 27 (45.0%) | 0.52 |
| Alcohol Abstinence Before LT 7–12 Months | 88 (28.0%) | 20 (22.7%) | 33 (37.5%) | 35 (39.8%) | 0.48 |
| Alcohol Abstinence Before LT >12 Months | 166 (52.9%) | 27 (16.3%) | 76 (45.8%) | 63 (38.0%) | 0.21 |
| DHD > 25 Years | 107 (34.3%) | 16 (15.0%) | 51 (47.7%) | 40 (37.4%) | 0.18 |
| DHD 11–25 Years | 161 (51.6%) | 32 (19.9%) | 65 (39.8%) | 64 (40.4%) | 0.90 |
| DHD < 11 Years | 44 (14.1%) | 11 (25.0%) | 12 (27.3%) | 21 (47.7%) | 0.13 |
| SDU < 11 | 144 (46.3%) | 36 (25.0%) | 54 (37.5%) | 54 (37.5%) | 0.04 |
| SDU 11–20 | 125 (40.2%) | 16 (12.8%) | 60 (48.0%) | 49 (39.2%) | 0.04 |
| SDU > 20 | 42 (13.5%) | 7 (16.7%) | 14 (33.3%) | 21 (50.0%) | 0.35 |
| 0 Alcoholism Treatment | 268 (85.4%) | 49 (18.3%) | 111 (41.4%) | 108 (40.3%) | 0.83 |
| 1 Alcoholism Treatment | 37 (11.8%) | 9 (24.3%) | 18 (48.6%) | 10 (27.0%) | 0.23 |
| 2 Alcoholism Treatments | 9 (2.9%) | 1 (11.1%) | 1 (11.1%) | 7 (77.8%) | 0.05 |
| HRAR Score >3 | 107 (34.4%) | 16 (15.0%) | 48 (44.9%) | 43 (40.2%) | 0.36 |
| Concomitant Substance Abuse | 92 (29.3%) | 5 (5.4%) | 31 (33.7%) | 56 (60.9%) | 0.00 |
| Benzodiazepines | 14 (4.5%) | 1 (7.1%) | 5 (35.7%) | 8 (57.1%) | 0.32 |
| Cannabis | 49 (15.6%) | 3 (6.1%) | 17 (34.7%) | 29 (59.2%) | 0.00 |
| Heroin | 28 (8.9%) | 3 (10.7%) | 11 (39.3%) | 14 (50.0%) | 0.39 |
| Cocaine | 51 (16.2%) | 3 (5.9%) | 15 (29.4%) | 33 (64.7%) | 0.00 |
| Other | 5 (1.6%) | 0 (0.0%) | 1 (20.0%) | 4 (80.0%) | 0.17 |
| Toxicity Awareness | 264 (84.1%) | 53 (20.1%) | 114 (43.2%) | 97 (36.7%) | 0.04 |
| Dependency Awareness | 165 (59.1%) | 31 (18.8%) | 66 (40.0%) | 68 (41.2%) | 0.91 |
| Psychiatric Pathology | 46 (14.6%) | 8 (17.4%) | 17 (37.0%) | 21 (45.7%) | 0.68 |
| HADS Depression (Positive) | 21 (10.8%) | 2 (9.5%) | 7 (33.3%) | 12 (57.1%) | 0.16 |
| HADS Anxiety (Positive) | 36 (18.5%) | 4 (11.1%) | 19 (52.8%) | 13 (36.1%) | 0.68 |
| Maladaptive Personality Traits | 25 (8.1%) | 5 (20.0%) | 8 (32.0%) | 12 (48.0%) | 0.56 |
| Group 1: Non-Smokers (n = 59) | Group 2: Ex-Smokers (n = 130) | Group 3: Active Smokers (n = 125) | p | |
|---|---|---|---|---|
| Alcohol Use Relapse | 10 | 25 | 35 | 0.13 |
| Substance Use Relapse | 1 | 0 | 8 | 0.02 |
| Graft Cirrhosis | 10 | 17 | 18 | 0.77 |
| Biopsy-Proven Alcoholic Steatohepatitis | 2 | 2 | 1 | 0.52 |
| HCC Recurrence | 3 | 3 | 6 | 0.33 |
| Skin Cancer | 2 | 4 | 3 | 0.92 |
| Non–Skin Cancer | 2 | 14 | 18 | 0.04 |
| OR (95% CI) | p | |
|---|---|---|
| Higher Risk of Being an Active Smoker Until LT | ||
| Age | 0.94 (0.89–0.99) | 0.01 |
| MELD | 1.06 (1.01–1.12) | 0.03 |
| Comorbid Substance Use Disorder | 2.35 (1.11–4.96) | 0.03 |
| Higher Risk of Being an Active Smoker After LT | ||
| Abstinence Period Of 6 Months or Less | 3.23 (1.19–8.78) | 0.02 |
| Comorbid Substance Use Disorder | 4.87 (2.17–10.96) | 0.00 |
| Alcohol Dependency Awareness | 0.43 (0.19–0.97) | 0.04 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Lazcano, A.I.; Gual, A.; Colmenero, J.; Caballería, E.; Lligoña, A.; Navasa, M.; Crespo, G.; López, E.; López-Pelayo, H. Active Smoking Before Liver Transplantation in Patients with Alcohol Use Disorder: Risk Factors and Outcomes. J. Clin. Med. 2020, 9, 2710. https://doi.org/10.3390/jcm9092710
López-Lazcano AI, Gual A, Colmenero J, Caballería E, Lligoña A, Navasa M, Crespo G, López E, López-Pelayo H. Active Smoking Before Liver Transplantation in Patients with Alcohol Use Disorder: Risk Factors and Outcomes. Journal of Clinical Medicine. 2020; 9(9):2710. https://doi.org/10.3390/jcm9092710
Chicago/Turabian StyleLópez-Lazcano, Ana Isabel, Antoni Gual, Jordi Colmenero, Elsa Caballería, Anna Lligoña, Miquel Navasa, Gonzalo Crespo, Eva López, and Hugo López-Pelayo. 2020. "Active Smoking Before Liver Transplantation in Patients with Alcohol Use Disorder: Risk Factors and Outcomes" Journal of Clinical Medicine 9, no. 9: 2710. https://doi.org/10.3390/jcm9092710