Safety, Effect and Feasibility of Percutaneous SI-Screw with and without Augmentation—A 15-Year Retrospective Analysis on over 640 Screws

 , , ,
, , ,
Abstract
:1. Introduction
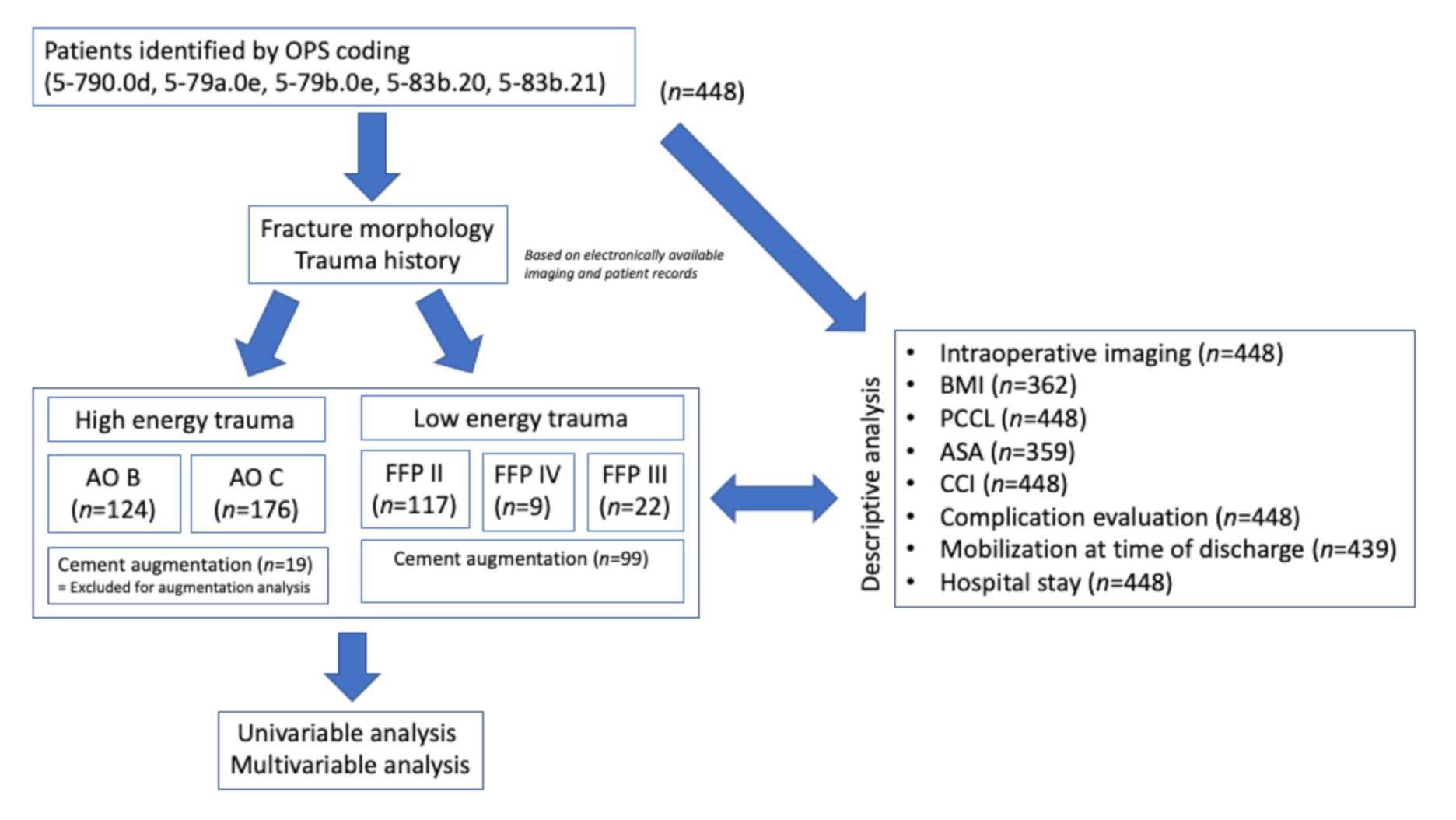
2. Experimental Section
3. Results
3.1. Safety of SI-Screw Insertion
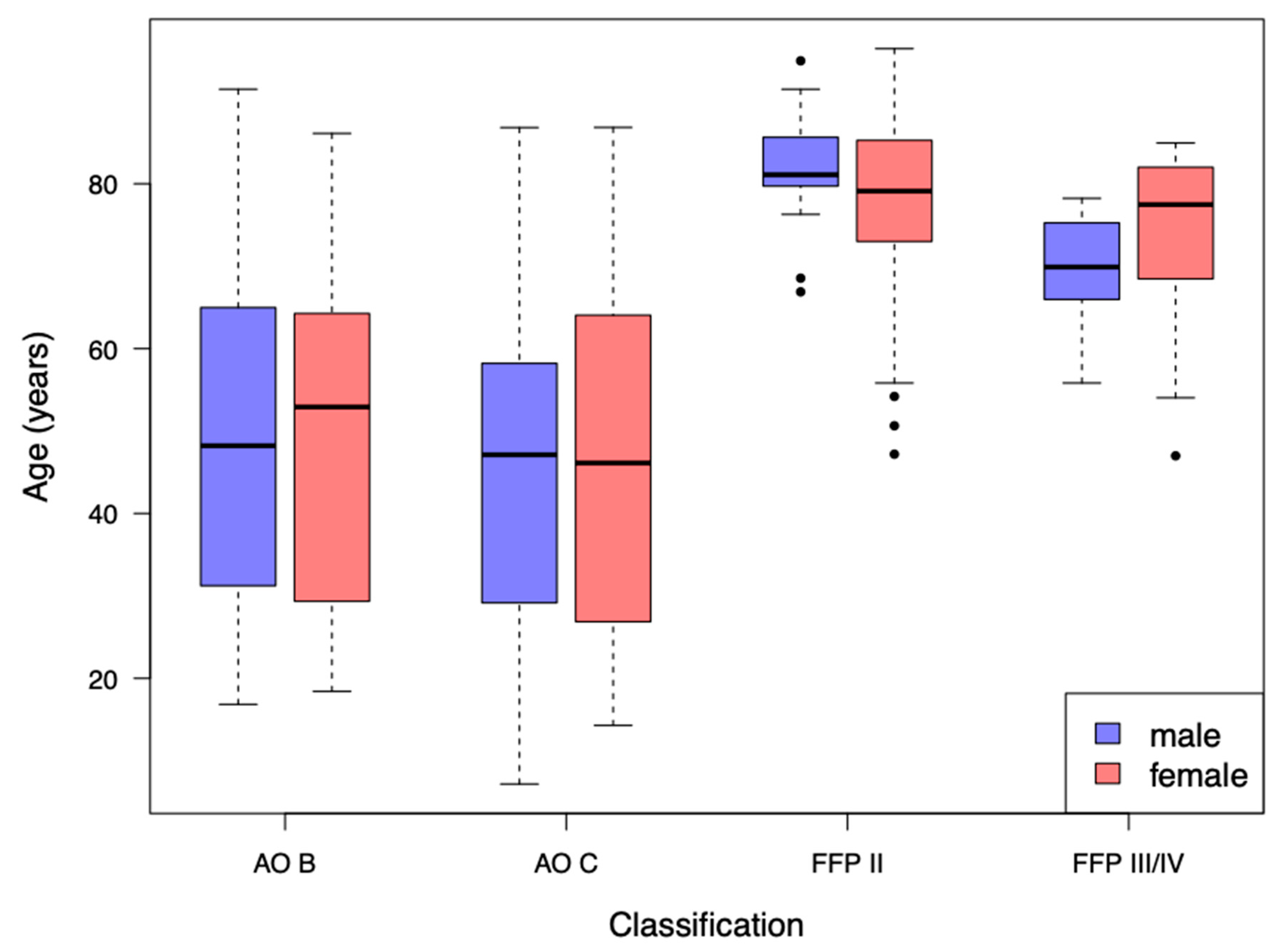
3.2. Analysis of AO-Classified Patients
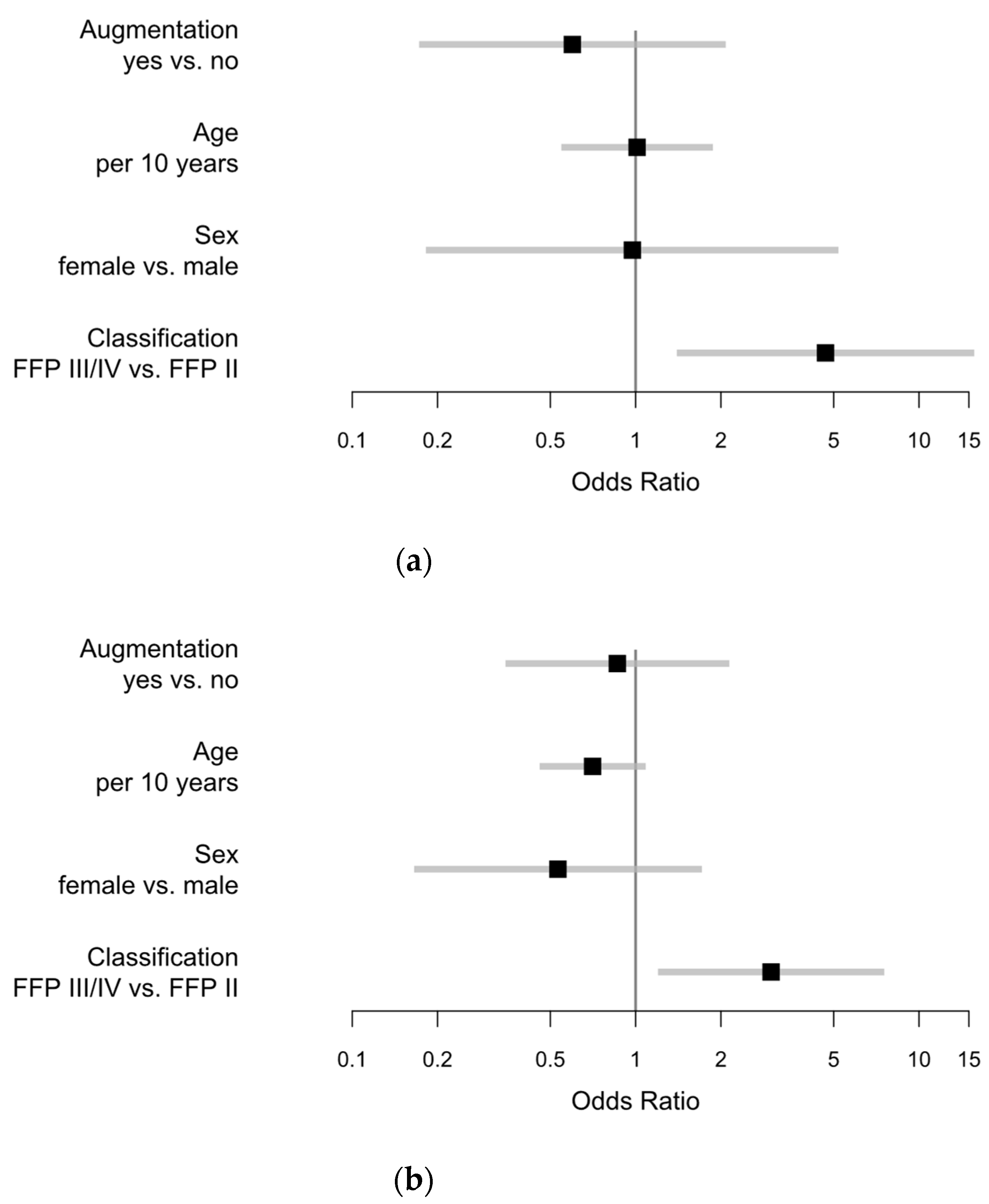
3.3. Analysis of FFP-Classified Patients
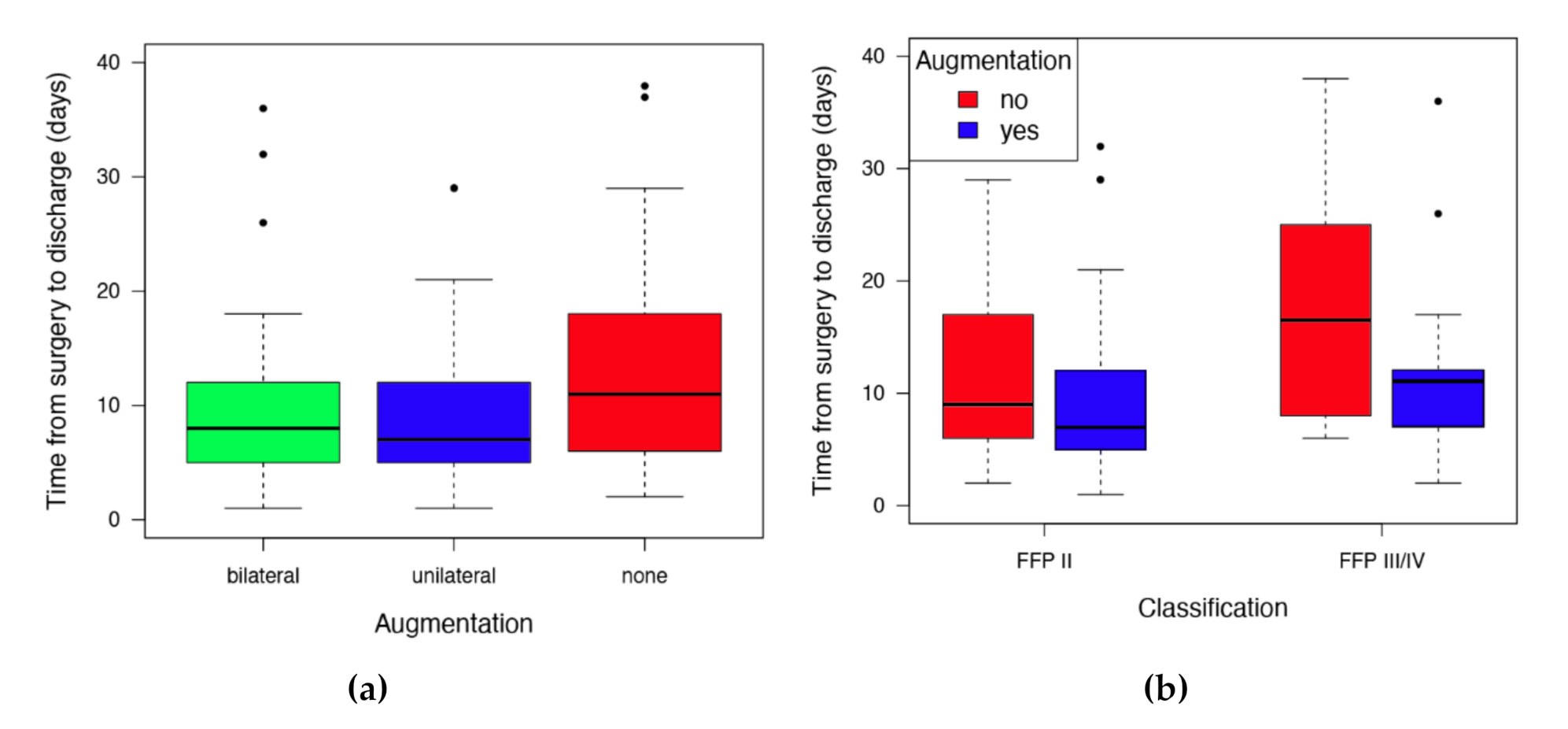
3.4. Effect and Safety of SI-Screw Augmentation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vidal, J.; Allieu, Y.; Fassio, B.; Adrey, J.; Goalard, C. Spondylolisthesis: Reduction with Harrington’s rods. Rev. Chir. Orthop. Reparatrice Appar. Mot. 1973, 59, 21–41. [Google Scholar] [PubMed]
- Iorio, J.A.; Jakoi, A.M.; Rehman, S. Percutaneous Sacroiliac Screw Fixation of the Posterior Pelvic Ring. Orthop. Clin. N. Am. 2015, 46, 511–521. [Google Scholar] [CrossRef]
- Wang, J.-Q.; Wang, Y.; Feng, Y.; Han, W.; Su, Y.-G.; Liu, W.-Y.; Zhang, W.-J.; Wu, X.-B.; Wang, M.-Y.; Fan, Y.-B. Percutaneous Sacroiliac Screw Placement: A Prospective Randomized Comparison of Robot-assisted Navigation Procedures with a Conventional Technique. Chin. Med. J. 2017, 130, 2527–2534. [Google Scholar] [CrossRef]
- Zwingmann, J.; Sudkamp, N.P.; Konig, B.; Culemann, U.; Pohlemann, T.; Aghayev, E.; Schmal, H. Intra-and postoperative complications of navigated and conventional techniques in percutaneous iliosacral screw fixation after pelvic fractures: Results from the German Pelvic Trauma Registry. Injury 2013, 44, 1765–1772. [Google Scholar] [CrossRef] [PubMed]
- Mendel, T.; Radetzki, F.; Wohlrab, D.; Stock, K.; Hofmann, G.O.; Noser, H. CT-based 3-D visualisation of secure bone corridors and optimal trajectories for sacroiliac screws. Injury 2013, 44, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Tile, M. Acute Pelvic Fractures: I. Causation and Classification. J. Am. Acad. Orthop. Surg. 1996, 4, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Meinberg, E.G.; Agel, J.; Roberts, C.S.; Karam, M.D.; Kellam, J.F. Fracture and Dislocation Classification Compendium-2018. J. Orthop. Trauma 2018, 32 (Suppl. 1), S1–S170. [Google Scholar] [CrossRef]
- Alvis-Miranda, H.R.; Farid-Escorcia, H.; Alcala-Cerra, G.; Castellar-Leones, S.M.; Moscote-Salazar, L.R. Sacroiliac screw fixation: A mini review of surgical technique. J. Craniovertebral Junction Spine 2014, 5, 110–113. [Google Scholar] [CrossRef]
- König, A.; Oberkircher, L.; Beeres, F.J.P.; Babst, R.; Ruchholtz, S.; Link, B.-C. Cement augmentation of sacroiliac screws in fragility fractures of the pelvic ring-A synopsis and systematic review of the current literature. Injury 2019, 50, 1411–1417. [Google Scholar] [CrossRef]
- Ravindrarajah, R.; Hazra, N.C.; Charlton, J.; Jackson, S.H.D.; Dregan, A.; Gulliford, M.C. Incidence and mortality of fractures by frailty level over 80 years of age: Cohort study using UK electronic health records. BMJ Open 2018, 8, e018836. [Google Scholar] [CrossRef] [Green Version]
- Rommens, P.M.; Wagner, D.; Hofmann, A. Fragility Fractures of the Pelvis. JBJS Rev. 2017, 5. [Google Scholar] [CrossRef] [PubMed]
- Rommens, P.M.; Hofmann, A. Comprehensive classification of fragility fractures of the pelvic ring: Recommendations for surgical treatment. Injury 2013, 44, 1733–1744. [Google Scholar] [CrossRef] [PubMed]
- Pieroh, P.; Hoch, A.; Hohmann, T.; Gras, F.; Mardian, S.; Pflug, A.; Wittenberg, S.; Ihle, C.; Blankenburg, N.; Dallacker-Losensky, K.; et al. Fragility Fractures of the Pelvis Classification: A Multicenter Assessment of the Intra-Rater and Inter-Rater Reliabilities and Percentage of Agreement. J. Bone Jt. Surg. Am. 2019, 101, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, D.O.; Ponsen, K.J.; Fiocco, M.; Amodio, S.; Leenen, L.P.H.; Goslings, J.C. Pelvic fractures in the Netherlands: Epidemiology, characteristics and risk factors for in-hospital mortality in the older and younger population. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Benzinger, P.; Riem, S.; Bauer, J.; Jaensch, A.; Becker, C.; Buchele, G.; Rapp, K. Risk of institutionalization following fragility fractures in older people. Osteoporos. Int. 2019, 30, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Eckardt, H.; Egger, A.; Hasler, R.M.; Zech, C.J.; Vach, W.; Suhm, N.; Morgenstern, M.; Saxer, F. Good functional outcome in patients suffering fragility fractures of the pelvis treated with percutaneous screw stabilisation: Assessment of complications and factors influencing failure. Injury 2017, 48, 2717–2723. [Google Scholar] [CrossRef]
- Muller, F.; Fuchtmeier, B. [Percutaneous cement-augmented screw fixation of bilateral osteoporotic sacral fracture]. Unfallchirurg 2013, 116, 950–954. [Google Scholar] [CrossRef]
- Tjardes, T.; Paffrath, T.; Baethis, H.; Shafizadeh, S.; Steinhausen, E.; Steinbuechel, T.; Rixen, D.; Bouillon, B. Computer assisted percutaneous placement of augmented iliosacral screws: A reasonable alternative to sacroplasty. Spine (Phila. Pa. 1976) 2008, 33, 1497–1500. [Google Scholar] [CrossRef]
- Wahnert, D.; Raschke, M.J.; Fuchs, T. Cement augmentation of the navigated iliosacral screw in the treatment of insufficiency fractures of the sacrum: A new method using modified implants. Int. Orthop. 2013, 37, 1147–1150. [Google Scholar] [CrossRef] [Green Version]
- Hoch, A.; Schimpf, R.; Hammer, N.; Schleifenbaum, S.; Werner, M.; Josten, C.; Bohme, J. Biomechanical analysis of stiffness and fracture displacement after using PMMA-augmented sacroiliac screw fixation for sacrum fractures. Biomed. Tech. (Berl.) 2017, 62, 421–428. [Google Scholar] [CrossRef]
- Osterhoff, G.; Dodd, A.E.; Unno, F.; Wong, A.; Amiri, S.; Lefaivre, K.A.; Guy, P. Cement Augmentation in Sacroiliac Screw Fixation Offers Modest Biomechanical Advantages in a Cadaver Model. Clin. Orthop. Relat. Res. 2016, 474, 2522–2530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gruneweller, N.; Raschke, M.J.; Zderic, I.; Widmer, D.; Wahnert, D.; Gueorguiev, B.; Richards, R.G.; Fuchs, T.; Windolf, M. Biomechanical comparison of augmented versus non-augmented sacroiliac screws in a novel hemi-pelvis test model. J. Orthop. Res. 2017, 35, 1485–1493. [Google Scholar] [CrossRef] [PubMed]
- Oberkircher, L.; Masaeli, A.; Bliemel, C.; Debus, F.; Ruchholtz, S.; Kruger, A. Primary stability of three different iliosacral screw fixation techniques in osteoporotic cadaver specimens-a biomechanical investigation. Spine J. 2016, 16, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Grechenig, S.; Gänsslen, A.; Gueorguiev, B.; Berner, A.; Müller, M.; Nerlich, M.; Schmitz, P. PMMA-augmented SI screw: A biomechanical analysis of stiffness and pull-out force in a matched paired human cadaveric model. Injury 2015, 46, S125–S128. [Google Scholar] [CrossRef]
- Suero, E.M.; Greiner, A.; Becker, C.A.; Cavalcanti Kußmaul, A.; Weidert, S.; Pfeufer, D.; Woiczinski, M.; Braun, C.; Flatz, W.; Böcker, W.; et al. Biomechanical stability of sacroiliac screw osteosynthesis with and without cement augmentation. Injury 2020. [Google Scholar] [CrossRef]
- Collinge, C.A.; Crist, B.D. Combined Percutaneous Iliosacral Screw Fixation With Sacroplasty Using Resorbable Calcium Phosphate Cement for Osteoporotic Pelvic Fractures Requiring Surgery. J. Orthop. Trauma. 2016, 30, e217–e222. [Google Scholar] [CrossRef]
- Hoch, A.; Pieroh, P.; Henkelmann, R.; Josten, C.; Bohme, J. In-screw polymethylmethacrylate-augmented sacroiliac screw for the treatment of fragility fractures of the pelvis: A prospective, observational study with 1-year follow-up. BMC Surg. 2017, 17, 132. [Google Scholar] [CrossRef] [Green Version]
- Konig, M.A.; Hediger, S.; Schmitt, J.W.; Jentzsch, T.; Sprengel, K.; Werner, C.M.L. In-screw cement augmentation for iliosacral screw fixation in posterior ring pathologies with insufficient bone stock. Eur. J. Trauma Emerg. Surg. 2018, 44, 203–210. [Google Scholar] [CrossRef]
- Sandmann, G.H.; Stockle, U.; Freude, T.; Stuby, F.M. Balloon Guided Cement Augmentation of Iliosacral Screws in the Treatment of Insufficiency Fractures of the Sacrum—Description of a New Method and Preliminary Results. Acta Chir. Orthop. Traumatol. Cech. 2018, 85, 85–88. [Google Scholar]
- Franz, D.; Kaufmann, M.; Siebert, C.H.; Windolf, J.; Roeder, N. Orthopedic and trauma surgery in the German DRG System 2007. Unfallchirurg 2007, 110, 270–280. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pishnamaz, M.; Dienstknecht, T.; Hoppe, B.; Garving, C.; Lange, H.; Hildebrand, F.; Kobbe, P.; Pape, H.C. Assessment of pelvic injuries treated with ilio-sacral screws: Injury severity and accuracy of screw positioning. Int. Orthop. 2016, 40, 1495–1501. [Google Scholar] [CrossRef] [PubMed]
- Grossterlinden, L.; Rueger, J.; Catala-Lehnen, P.; Rupprecht, M.; Lehmann, W.; Rucker, A.; Briem, D. Factors influencing the accuracy of iliosacral screw placement in trauma patients. Int. Orthop. 2011, 35, 1391–1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghisla, S.; Napoli, F.; Lehoczky, G.; Delcogliano, M.; Habib, N.; Arigoni, M.; Filardo, G.; Candrian, C. Posterior pelvic ring fractures: Intraoperative 3D-CT guided navigation for accurate positioning of sacro-iliac screws. Orthop. Traumatol. Surg. Res. 2018, 104, 1063–1067. [Google Scholar] [CrossRef]
- Thakkar, S.C.; Thakkar, R.S.; Sirisreetreerux, N.; Carrino, J.A.; Shafiq, B.; Hasenboehler, E.A. 2D versus 3D fluoroscopy-based navigation in posterior pelvic fixation: Review of the literature on current technology. Int. J. Comput. Assist. Radiol. Surg. 2017, 12, 69–76. [Google Scholar] [CrossRef]
- Falzarano, G.; Rollo, G.; Bisaccia, M.; Pace, V.; Lanzetti, R.M.; Garcia-Prieto, E.; Pichierri, P.; Meccariello, L. Percutaneous screws CT guided to fix sacroiliac joint in tile C pelvic injury. Outcomes at 5 years of follow-up. SICOT-J. 2018, 4, 52. [Google Scholar] [CrossRef]
- Rommens, P.M.; Wagner, D.; Hofmann, A. Do We Need a Separate Classification for Fragility Fractures of the Pelvis? J. Orthop. Trauma 2019, 33 (Suppl. 2), S55–S60. [Google Scholar] [CrossRef]
- Schoenfeld, A.J.; Reamer, E.N.; Wynkoop, E.I.; Choi, H.; Bono, C.M. Does Patient Sex Affect the Rate of Mortality and Complications After Spine Surgery? A Systematic Review. Clin. Orthop. Relat. Res. 2015, 473, 2479–2486. [Google Scholar] [CrossRef] [Green Version]
- Hermans, E.; Biert, J.; Edwards, M.J.R. Epidemiology of Pelvic Ring Fractures in a Level 1 Trauma Center in the Netherlands. Hip Pelvis 2017, 29, 253–261. [Google Scholar] [CrossRef] [Green Version]
- Falzarano, G.; Medici, A.; Carta, S.; Grubor, P.; Fortina, M.; Meccariello, L.; Ferrata, P. The orthopedic damage control in pelvic ring fractures: When and why-a multicenter experience of 10 years’ treatment. J. Acute Dis. 2014, 3, 201–206. [Google Scholar] [CrossRef] [Green Version]
- Ueda, Y.; Inui, T.; Kurata, Y.; Tsuji, H.; Saito, J.; Shitan, Y. Prolonged pain in patients with fragility fractures of the pelvis may be due to fracture progression. Eur. J. Trauma Emerg. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Rommens, P.M.; Arand, C.; Hopf, J.C.; Mehling, I.; Dietz, S.O.; Wagner, D. Progress of instability in fragility fractures of the pelvis: An observational study. Injury 2019, 50, 1966–1973. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Fan, P.; Xie, X.; Wang, Y. Risk Factors for Cement Leakage and Adjacent Vertebral Fractures in Kyphoplasty for Osteoporotic Vertebral Fractures. Clin. Spine Surg. 2020. [Google Scholar] [CrossRef]
- Van Dijk, W.A.; Poeze, M.; Van Helden, S.H.; Brink, P.R.; Verbruggen, J.P. Ten-year mortality among hospitalised patients with fractures of the pubic rami. Injury 2010, 41, 411–414. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Minor Compilation | Major Complication |
|---|---|
| • Hypertensive derailment | • Inguinal hernia incarcerated postoperatively |
| • Delayed wound healing | • Cerebral hemorrhage postoperatively |
| • Infections (UTIs 1, pneumonia, other infections without severe clinical impact) | • Postoperative fracture dislocation |
| • Intraoperative resuscitation | |
| • Postoperative atrial fibrillation | • Death |
| • Postoperative anemia | • Implant failure requiring revision surgery |
| • Pain described to be the reason of delayed discharge | • Heavy intraoperative bleeding 2 |
| • Superficial wound infections | • Acute kidney failure (AKIN) |
| • Hematoma (without revision) | • Persistent postoperative neurological impairment until discharge 3 |
| • Temporary neurological impairment 1 | • Postoperative cerebral insult |
| • Postoperative angioedema | • Wound infection requires revision surgery |
| • New diagnosis of restless leg syndrome | • Postoperative pulmonary artery embolism |
| • Early loosening of external supraacetabular fixator | • Postoperative wound-related hemorrhage |
| • Pain beyond a period of about 6 months | • Postoperative severe hematoma with revision surgery |
| • Postoperative positive Trendelenburg sign |
| Free Mobilization | Rollator/Walking Frame | Wheelchair | Crutches/Walking Stick | Bedridden | No Information | |
|---|---|---|---|---|---|---|
| Median age (years) | 86.17 | 80.16 | 75.45 | 76.53 | 84.72 | – |
| Q 25% | 56.48 | 75.46 | 66.48 | 64.81 | 69.01 | – |
| Q 75% | 87.80 | 84.14 | 84.95 | 83.96 | 85.65 | – |
| FFP II | 2 (1.71%) | 60 (51.28%) | 7 (5.98%) | 37 (31.62%) | 9 (7.69%) | 2 (1.71%) |
| FFP III | – | 1 (11.11%) | 1 (11.11%) | 6 (66.67%) | – | 1 (11.11%) |
| FFP IV | 1 (4.55%) | 16 (72.73%) | 3 (13.64%) | 1 (4.55%) | 1 (4.55%) | – |
| PCCL | ||||||
|---|---|---|---|---|---|---|
| 0–1 | 2 | 3 | 4 | 5–6 | Total | |
| n | 33 | 18 | 50 | 37 | 10 | 148 |
| Median (d) | 9 | 5.5 | 8 | 9 | 25 | 8 |
| Q 25% | 5 | 4 | 5 | 6 | 16 | 5 |
| Q 75% | 12 | 8 | 11.5 | 15 | 32 | 13.5 |
| Free Mobilization | Crutches/Walking Stick | Rollator/Walking Frame | Wheelchair | Bedridden | No Information | |
|---|---|---|---|---|---|---|
| Unilateral augmentation | 2 (6.06%) | 10 (30.30%) | 18 (54.55%) | 1 (3.03%) | 2 (6.06%) | – |
| Bilateral augmentation | – | 12 (18.18%) | 39 (59.09%) | 7 (10.61%) | 6 (9.09%) | 2 (3.03%) |
| No augmentation | 1 (2.04%) | 22 (44.9%) | 20 (40.82%) | 3 (6.12%) | 2 (4.08%) | 1 (2.04%) |
| In 3 cases, no information about mobilization could be found. | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hartensuer, R.; Lodde, M.F.; Keller, J.; Eveslage, M.; Stolberg-Stolberg, J.; Riesenbeck, O.; Raschke, M.J. Safety, Effect and Feasibility of Percutaneous SI-Screw with and without Augmentation—A 15-Year Retrospective Analysis on over 640 Screws. J. Clin. Med. 2020, 9, 2660. https://doi.org/10.3390/jcm9082660
Hartensuer R, Lodde MF, Keller J, Eveslage M, Stolberg-Stolberg J, Riesenbeck O, Raschke MJ. Safety, Effect and Feasibility of Percutaneous SI-Screw with and without Augmentation—A 15-Year Retrospective Analysis on over 640 Screws. Journal of Clinical Medicine. 2020; 9(8):2660. https://doi.org/10.3390/jcm9082660
Chicago/Turabian StyleHartensuer, René, Moritz F. Lodde, Jonas Keller, Maria Eveslage, Josef Stolberg-Stolberg, Oliver Riesenbeck, and Michael J. Raschke. 2020. "Safety, Effect and Feasibility of Percutaneous SI-Screw with and without Augmentation—A 15-Year Retrospective Analysis on over 640 Screws" Journal of Clinical Medicine 9, no. 8: 2660. https://doi.org/10.3390/jcm9082660