Outpatient Pulmonary Rehabilitation in Patients with Persisting Symptoms after Pulmonary Embolism

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Patient Cohort
2.2. Rehabilitation Procedures
2.3. Outcome Variables
2.4. Long-Term Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Changes in Outcome Variables
3.3. Long-Term Follow-Up
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Konstantinides, S.V. Trends in incidence versus case fatality rates of pulmonary embolism: Good news or bad news? Thromb. Haemost. 2016, 115, 233–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barco, S.; Mahmoudpour, S.H.; Valerio, L.; Klok, F.A.; Münzel, T.; Middeldorp, S.; Ageno, W.; Cohen, A.T.; Hunt, B.J.; Konstantinides, S.V. Trends in mortality related to pulmonary embolism in the European Region, 2000–15: Analysis of vital registration data from the WHO Mortality Database. Lancet Respir. Med. 2020, 8, 277–287. [Google Scholar] [CrossRef]
- Klok, F.A.; van der Hulle, T.; den Exter, P.L.; Lankeit, M.; Huisman, M.V.; Konstantinides, S. The post-PE syndrome: A new concept for chronic complications of pulmonary embolism. Blood Rev. 2014, 28, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Huisman, M.V.; Barco, S.; Cannegieter, S.C.; Le Gal, G.; Konstantinides, S.V.; Reitsma, P.H.; Rodger, M.; Vonk Noordegraaf, A.; Klok, F.A. Pulmonary embolism. Nat. Rev. Dis. Primers 2018, 4, 18028. [Google Scholar] [CrossRef] [PubMed]
- Sista, A.K.; Klok, F.A. Late outcomes of pulmonary embolism: The post-PE syndrome. Thromb. Res. 2018, 164, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Kahn, S.R.; Houweling, A.H.; Granton, J.; Rudski, L.; Dennie, C.; Hirsch, A. Long-term outcomes after pulmonary embolism: Current knowledge and future research. Blood Coagul. Fibrinolysis Int. J. Haemost. Thromb. 2014, 25, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Ende-Verhaar, Y.M.; Cannegieter, S.C.; Vonk Noordegraaf, A.; Delcroix, M.; Pruszczyk, P.; Mairuhu, A.T.; Huisman, M.V.; Klok, F.A. Incidence of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism: A contemporary view of the published literature. Eur. Respir. J. 2017, 49. [Google Scholar] [CrossRef] [PubMed]
- Tavoly, M.; Wik, H.S.; Sirnes, P.A.; Jelsness-Jorgensen, L.P.; Ghanima, J.P.; Klok, F.A.; Sandset, P.M.; Ghanima, W. The impact of post-pulmonary embolism syndrome and its possible determinants. Thromb. Res. 2018, 171, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Kahn, S.R.; Hirsch, A.M.; Akaberi, A.; Hernandez, P.; Anderson, D.R.; Wells, P.S.; Rodger, M.A.; Solymoss, S.; Kovacs, M.J.; Rudski, L.; et al. Functional and Exercise Limitations After a First Episode of Pulmonary Embolism: Results of the ELOPE Prospective Cohort Study. Chest 2017, 151, 1058–1068. [Google Scholar] [CrossRef] [PubMed]
- Tavoly, M.; Utne, K.K.; Jelsness-Jorgensen, L.P.; Wik, H.S.; Klok, F.A.; Sandset, P.M.; Ghanima, W. Health-related quality of life after pulmonary embolism: A cross-sectional study. BMJ Open 2016, 6, e013086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sista, A.K.; Miller, L.E.; Kahn, S.R.; Kline, J.A. Persistent right ventricular dysfunction, functional capacity limitation, exercise intolerance, and quality of life impairment following pulmonary embolism: Systematic review with meta-analysis. Vasc. Med. (Lond. Engl.) 2017, 22, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Hagan, K.A.; Harrington, L.B.; Kim, J.; Zeleznik, O.; Rimm, E.B.; Grodstein, F.; Kabrhel, C. Reduction in physical function in women after venous thromboembolism. J. Thromb. Haemost. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albaghdadi, M.S.; Dudzinski, D.M.; Giordano, N.; Kabrhel, C.; Ghoshhajra, B.; Jaff, M.R.; Weinberg, I.; Baggish, A. Cardiopulmonary Exercise Testing in Patients Following Massive and Submassive Pulmonary Embolism. J. Am. Heart Assoc. 2018, 7, e006841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2017, 39, 119–177. [Google Scholar] [CrossRef] [Green Version]
- Noack, F.; Schmidt, B.; Amoury, M.; Stoevesandt, D.; Gielen, S.; Pflaumbaum, B.; Girschick, C.; Völler, H.; Schlitt, A. Feasibility and safety of rehabilitation after venous thromboembolism. Vasc. Health Risk Manag. 2015, 11, 397–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amoury, M.; Noack, F.; Kleeberg, K.; Stoevesandt, D.; Lehnigk, B.; Bethge, S.; Heinze, V.; Schlitt, A. Prognosis of patients with pulmonary embolism after rehabilitation. Vasc. Health Risk Manag. 2018, 14, 183–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grünig, E.; Eichstaedt, C.; Barberà, J.-A.; Benjamin, N.; Blanco, I.; Bossone, E.; Cittadini, A.; Coghlan, G.; Corris, P.; D’Alto, M.; et al. ERS statement on exercise training and rehabilitation in patients with severe chronic pulmonary hypertension. Eur. Respir. J. 2019, 53, 1800332. [Google Scholar] [CrossRef] [Green Version]
- Vonbank, K.; Zwick, R.H.; Strauss, M.; Lichtenschopf, A.; Puelacher, C.; Budnowski, A.; Possert, G.; Trinker, M. Guidelines for outpatient pulmonary rehabilitation in Austria. Wien. Klin. Wochenschr. 2015, 127, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Enright, P.L. The Six-Minute Walk Test. Respir. Care 2003, 48, 783–785. [Google Scholar] [PubMed]
- ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [CrossRef] [PubMed]
- Bohannon, R.W.; Crouch, R. Minimal clinically important difference for change in 6-minute walk test distance of adults with pathology: A systematic review. J. Eval. Clin. Pract. 2017, 23, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Boon, G.J.A.M.; Barco, S.; Bertoletti, L.; Ghanima, W.; Huisman, M.V.; Kahn, S.R.; Noble, S.; Prandoni, P.; Rosovsky, R.P.; Sista, A.K.; et al. Measuring functional limitations after venous thromboembolism: Optimization of the Post-VTE Functional Status (PVFS) Scale. Thromb. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Ellert, U.; Kurth, B.M. Gesundheitsbezogene Lebensqualität bei Erwachsenen in Deutschland. Bundesgesundheitsblatt Gesundh. Gesundh. 2013, 56, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Enright, P.L.; Sherrill, D.L. Reference equations for the six-minute walk in healthy adults. Am. J. Respir. Crit. Care Med. 1998, 158, 1384–1387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandey, A.; Garg, S.; Khunger, M.; Garg, S.; Kumbhani, D.J.; Chin, K.M.; Berry, J.D. Efficacy and Safety of Exercise Training in Chronic Pulmonary Hypertension: Systematic Review and Meta-Analysis. Circ. Heart Fail. 2015, 8, 1032–1043. [Google Scholar] [CrossRef] [PubMed]
- Mereles, D.; Ehlken, N.; Kreuscher, S.; Ghofrani, S.; Hoeper, M.M.; Halank, M.; Meyer, F.J.; Karger, G.; Buss, J.; Juenger, J.; et al. Exercise and respiratory training improve exercise capacity and quality of life in patients with severe chronic pulmonary hypertension. Circulation 2006, 114, 1482–1489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukui, S.; Ogo, T.; Takaki, H.; Ueda, J.; Tsuji, A.; Morita, Y.; Kumasaka, R.; Arakawa, T.; Nakanishi, M.; Fukuda, T.; et al. Efficacy of cardiac rehabilitation after balloon pulmonary angioplasty for chronic thromboembolic pulmonary hypertension. Heart 2016, 102, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Lakoski, S.G.; Savage, P.D.; Berkman, A.M.; Penalosa, L.; Crocker, A.; Ades, P.A.; Kahn, S.R.; Cushman, M. The safety and efficacy of early-initiation exercise training after acute venous thromboembolism: A randomized clinical trial. J. Thromb. Haemost. 2015, 13, 1238–1244. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A.; Pitta, F.; Garvey, C.; ZuWallack, R.L.; Roberts, C.M.; Collins, E.G.; Goldstein, R.; McNamara, R.; Surpas, P.; Atsuyoshi, K.; et al. Differences in content and organisational aspects of pulmonary rehabilitation programmes. Eur. Respir. J. 2014, 43, 1326–1337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lacasse, Y.; Martin, S.; Lasserson, T.J.; Goldstein, R.S. Meta-analysis of respiratory rehabilitation in chronic obstructive pulmonary disease. A Cochrane systematic review. Eura Med. 2007, 43, 475–485. [Google Scholar]
- Kaminsky, L.A.; Imboden, M.T.; Arena, R.; Myers, J. Reference Standards for Cardiorespiratory Fitness Measured With Cardiopulmonary Exercise Testing Using Cycle Ergometry: Data From the Fitness Registry and the Importance of Exercise National Database (FRIEND) Registry. Mayo Clin. Proc. 2017, 92, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Pessoa, I.M.B.S.; Parreira, V.F.; Fregonezi, G.A.F.; Sheel, A.W.; Chung, F.; Reid, W.D. Reference Values for Maximal Inspiratory Pressure: A Systematic Review. Can. Respir. J. 2014, 21, 982374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klok, F.A.; van Kralingen, K.W.; van Dijk, A.P.; Heyning, F.H.; Vliegen, H.W.; Kaptein, A.A.; Huisman, M.V. Quality of life in long-term survivors of acute pulmonary embolism. Chest 2010, 138, 1432–1440. [Google Scholar] [CrossRef] [PubMed]
- van Es, J.; den Exter, P.L.; Kaptein, A.A.; Andela, C.D.; Erkens, P.M.G.; Klok, F.A.; Douma, R.A.; Mos, I.C.M.; Cohn, D.M.; Kamphuisen, P.W.; et al. Quality of life after pulmonary embolism as assessed with SF-36 and PEmb-QoL. Thromb. Res. 2013, 132, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Investigators, E.-P.; Buller, H.R.; Prins, M.H.; Lensin, A.W.; Decousus, H.; Jacobson, B.F.; Minar, E.; Chlumsky, J.; Verhamme, P.; Wells, P.; et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N. Engl. J. Med. 2012, 366, 1287–1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Couturaud, F.; Sanchez, O.; Pernod, G.; Mismetti, P.; Jego, P.; Duhamel, E.; Provost, K.; dit Sollier, C.B.; Presles, E.; Castellant, P.; et al. Six Months vs Extended Oral Anticoagulation After a First Episode of Pulmonary Embolism: The PADIS-PE Randomized Clinical Trial. JAMA 2015, 314, 31–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, G.; Vicaut, E.; Danays, T.; Agnelli, G.; Becattini, C.; Beyer-Westendorf, J.; Bluhmki, E.; Bouvaist, H.; Brenner, B.; Couturaud, F.; et al. Fibrinolysis for Patients with Intermediate-Risk Pulmonary Embolism. N. Engl. J. Med. 2014, 370, 1402–1411. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.-J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur. Heart J. 2019. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Patients with Data/Total Number of Patients | Median [IQR] or Count (%) |
|---|---|---|
| Demographics | ||
| Age (years) | 22/22 | 47.5 [42.5–54.3] |
| Female | 22/22 | 7 (31.8%) |
| BMI (kg/m²) | 22/22 | 32.4 [27.8–37.4] |
| Weight (kg) | 22/22 | 102.5 [87.5–114.8] |
| PE characteristics † | ||
| DVT present at index event | 21/22 | 12 (57.1%) |
| Triggering events/risk factors | ||
| --Unprovoked | 22/22 | 13 (59.1%) |
| --Oestrogen use | 22/22 | 4 (18.2%) |
| --Recent surgery (major/minor) | 22/22 | 3 (13.6%) |
| --Long travel (>4 h, past 30 days) | 22/22 | 1 (4.5%) |
| --Benign tumor | 22/22 | 1 (4.5%) |
| Site of PE | ||
| --Unilateral | 20/22 | 2 (10%) |
| --Bilateral | 20/22 | 18 (90%) |
| Location of PE | ||
| --Central | 16/22 | 9 (56.3%) |
| --Lobar | 16/22 | 2 (12.5%) |
| --Segmental | 16/22 | 5 (31.3%) |
| History of VTE | ||
| Previous DVT | 22/22 | 4 (18.2%) |
| Previous PE | 22/22 | 3 (13.6%) |
| Comorbidities | ||
| Charlson Comorbidity Index (CCI) | 22/22 | 0.55 (0–0) |
| Chronic obstructive pulmonary disease | 22/22 | 2 (9%) |
| History of acute lymphatic leukemia | 22/22 | 1 (4.5%) |
| Arterial hypertension | 22/22 | 10 (45.5%) |
| Active smoker | 20/22 | 3 (15%) |
| History of smoking | 20/22 | 9 (45%) |
| Timeline | ||
| Time between PE diagnosis and start of rehabilitation (weeks) * | 22/22 | 19 [14–37.25] |
| Duration of rehabilitation (weeks) | 22/22 | 6 [6–10.50] |
| Assessment (Measurement) | Patients with Data/Total Number of Patients | Admission | Discharge | Difference (Percent) | p-Value |
|---|---|---|---|---|---|
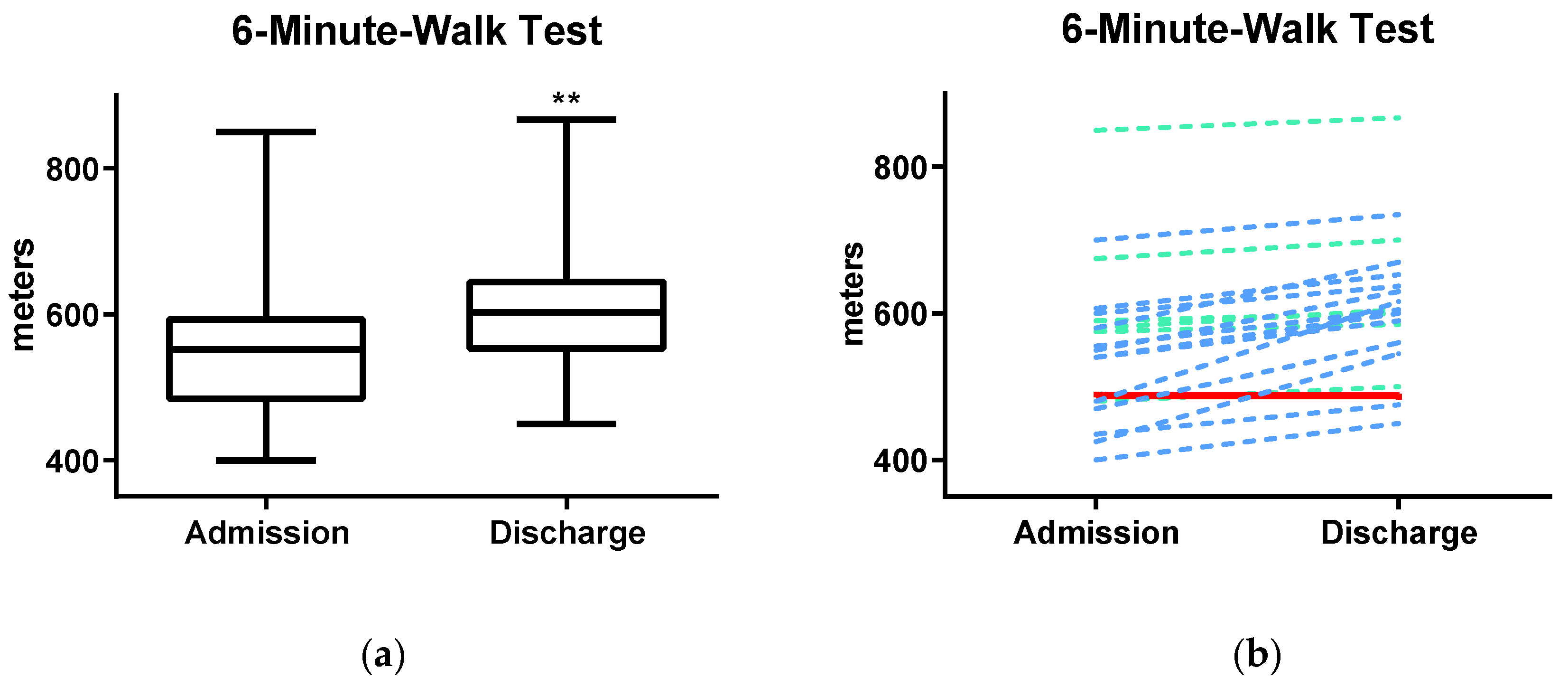
| 6MWT (m) | 20/22 | 556.1 (±104.8) | 605.5 (±96.0) | +49.4 (9%) | <0.001 |
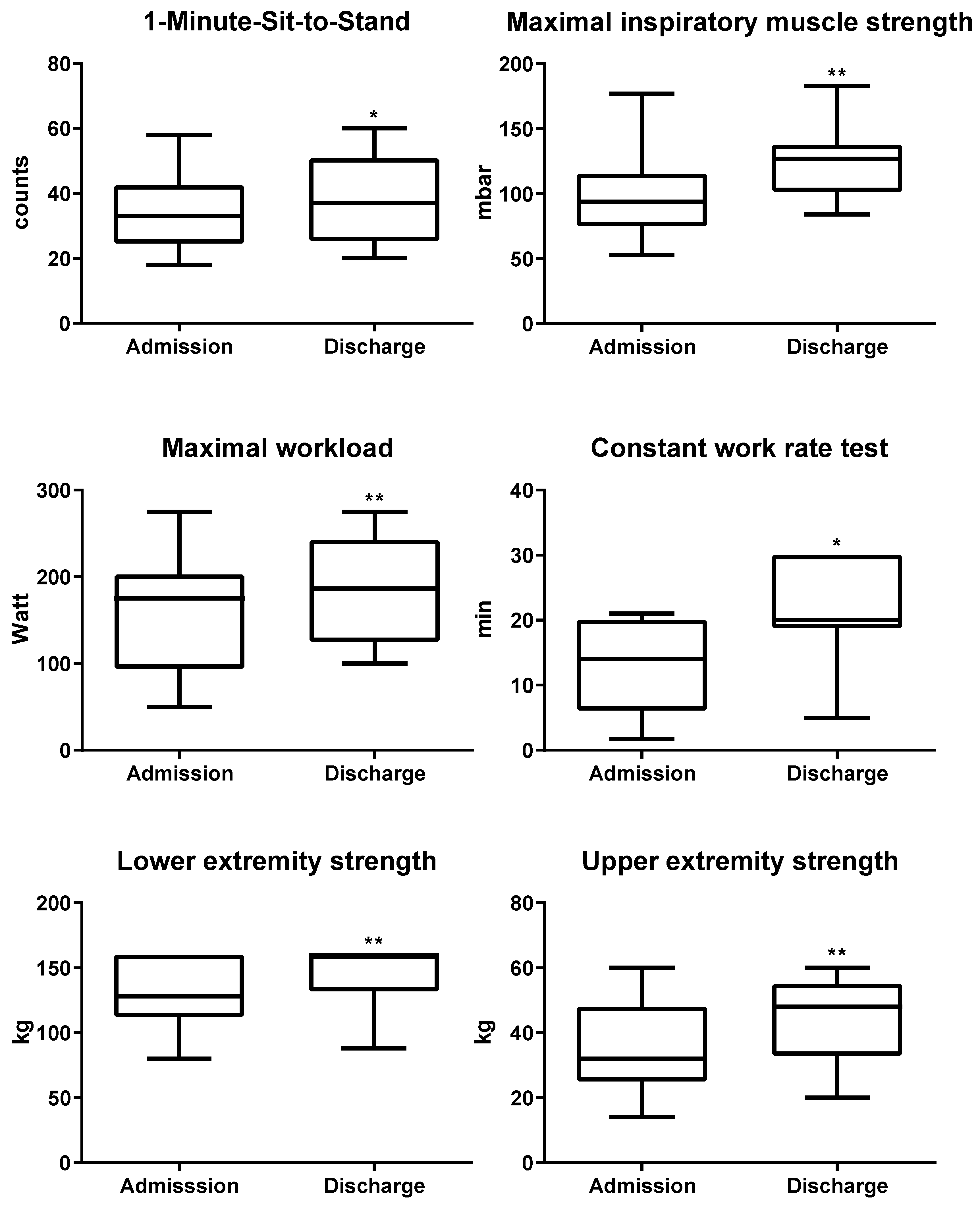
| 1-MSTST | 14/22 | 35.1 (±12.6) | 39.0(±14.3) | +3.9 (11%) | 0.034 |
| Pimax (mbar) | 22/22 | 94.7 (±30.4) | 125.2 (±27.0) | +30.5 (32%) | <0.001 |
| Wmax (watt) | 18/22 | 156.8 (±63.6) | 188.5 (±57.1) | +31.7 (20%) | <0.001 |
| CWR70% (min) * | 14/22 | 12.7 (±6.7) | 21.2 (±7.7) | +8.5 (67%) | 0.002 |
| LE strength (kg) # | 11/22 | 117 (±17.9) | 146.9 (±16.5) | +29.9 (26%) | <0.001 |
| UE strength (kg) | 16/22 | 34.9 (±12.6) | 44.5 (±11.7) | +9.6 (28%) | <0.001 |
| Vital Parameters and FEV1 | Patients with Data/Total Number of Patients | Admission | Discharge | Mean Difference [95% CI] |
|---|---|---|---|---|
| HR at rest | 20/22 | 89.6 (±19.0) | 83.8 (±14.4) | −5.8 [−12.5, 0.9] |
| HR at max | 20/22 | 142.5 (±18.1) | 144.9 (±18.4) | 2.4 [−4.1, 8.8] |
| sysBP at rest (mmHg) | 17/22 | 132.7 (±16.0) | 130.8 (±11.2) | −1.9 [−10.4, 6.7] |
| diaBP at rest (mmHg) | 17/22 | 82.7 (±68.8) | 82.9 (±48.9) | 0.2 [−4.5, 4.9] |
| sysBP at max (mmHg) | 15/22 | 190.8 (±39.5) | 193.2 (±32.7) | 2.4 [−14.7, 19.5] |
| diaBP at max (mmHg) | 15/22 | 85.3 (±18.4) | 86.1 (±19.4) | 0.8 [−10.9, 12.5] |
| Weight (kg) | 22/22 | 99.9 (±19.8) | 99.4 (±19.8) | −0.5 [−1.6, 0.6] |
| FEV1 (liter) | 20/22 | 3.03 (±0.6) | 3.07 (±0.6) | 0.04 [−0.2, 0,3] |
| PR Cohort (n = 18) | Reference Population Norm Age 40–49 [25] | |
|---|---|---|
| Physical functioning (PF) | 76.7 (±17.2) * | 89.5 |
| Role physical (RP) | 68.1 (±39.1) | 85.5 |
| Role emotional (RE) | 72.2 (±40.0) | 86.8 |
| Vitality (VT) | 50.3 (±19.1) * | 60.7 |
| Mental health (MH) | 69.6 (±14.8) | 72.8 |
| Social functioning (SF) | 75.0 (±26.8) | 85.6 |
| Bodily Pain (BP) | 71.9 (±23.1) | 75.3 |
| General health (GH) | 50.0 (±23.2) * | 69.9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nopp, S.; Klok, F.A.; Moik, F.; Petrovic, M.; Derka, I.; Ay, C.; Zwick, R.H. Outpatient Pulmonary Rehabilitation in Patients with Persisting Symptoms after Pulmonary Embolism. J. Clin. Med. 2020, 9, 1811. https://doi.org/10.3390/jcm9061811
Nopp S, Klok FA, Moik F, Petrovic M, Derka I, Ay C, Zwick RH. Outpatient Pulmonary Rehabilitation in Patients with Persisting Symptoms after Pulmonary Embolism. Journal of Clinical Medicine. 2020; 9(6):1811. https://doi.org/10.3390/jcm9061811
Chicago/Turabian StyleNopp, Stephan, Frederikus A. Klok, Florian Moik, Milos Petrovic, Irmgard Derka, Cihan Ay, and Ralf Harun Zwick. 2020. "Outpatient Pulmonary Rehabilitation in Patients with Persisting Symptoms after Pulmonary Embolism" Journal of Clinical Medicine 9, no. 6: 1811. https://doi.org/10.3390/jcm9061811