Trends in Diabetes-Related Potentially Preventable Hospitalizations in Adult Population in Spain, 1997–2015: A Nation-Wide Population-Based Study

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Tomlin, A.M.; Tilyard, M.W.; Dovey, S.M.; Dawson, A.G. Hospital admissions in diabetic and non diabetic patients: A case-control study. Diabetes Res. Clin. Pract. 2006, 73, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Lara-Rojas, C.M.; Pérez-Belmonte, L.M.; López-Carmona, M.D.; Guijarro-Merino, R.; Bernal-López, M.R.; Gómez-Huelgas, R. National trends in diabetes mellitus hospitalization in Spain 1997–2010: Analysis of over 5.4 millions of admissions. Eur. J. Intern. Med. 2019, 60, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Imai, K.; Engelgau, M.M.; Geiss, L.S.; Wen, C.; Zhang, P. Secular trends in diabetes-related preventable hospitalizations in the United States, 1998–2006. Diabetes Care 2009, 32, 1213–1217. [Google Scholar] [CrossRef] [PubMed]
- Mata-Cases, M.; Casajuana, M.; Franch-Nadal, J.; Casellas, A.; Castell, C.; Vinagre, I.; Mauricio, D.; Bolíbar, B. Direct medical costs attributable to type 2 diabetes mellitus: A population-based study in Catalonia, Spain. Eur. J. Health Econ. 2016, 17, 1001–1010. [Google Scholar] [CrossRef] [PubMed]
- Joint British Diabetes Societies for Inpatient Care (JBDS–IP). Admissions Avoidance and Diabetes: Guidance for Clinical Commissioning Groups and Clinical Teams. 2013. Available online: https://www.diabetes.org.uk/Documents/Position%20statements/admissions-avoidance-diabetes-0114.pdf (accessed on 25 October 2016).
- Bindman, A.B.; Grumbach, K.; Osmond, D.; Komaromy, M.; Vranizan, K.; Lurie, N.; Billings, J.; Stewart, A. Preventable hospitalizations and access to health care. JAMA 1995, 274, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Purdy, S.; Griffin, T.; Salisbury, C.; Sharp, D. Ambulatory care sensitive conditions: Terminology and disease coding need to be more specific to aid policy makers and clinicians. Public Health 2009, 123, 169–173. [Google Scholar] [CrossRef]
- Billings, J.; Anderson, G.M.; Newman, L.S. Recent findings on preventable hospitalizations. Health Aff. (Millwood) 1996, 15, 239–249. [Google Scholar] [CrossRef]
- Agency for Healthcare Research and Quality. Prevention Quality Indicators Overview. 2016. Available online: http://www.qualityindicators.ahrq.gov/modules/pqi_overview.aspx (accessed on 26 October 2016).
- Rubens, M.; Saxena, A.; Ramamoorthy, V.; Khera, R.; Hong, J.; Veledar, E.; Nasir, K. Trends in Diabetes-Related Preventable Hospitalizations in the U.S., 2005–2014. Diabetes Care 2018, 41, 72–73. [Google Scholar] [CrossRef]
- Lombardo, F.; Maggini, M.; Gruden, G.; Bruno, G. Temporal trend in hospitalizations for acute diabetic complications: A nationwide study, Italy, 2001–2010. PLoS ONE 2013, 8, e63675. [Google Scholar] [CrossRef]
- Manderbacka, K.; Arffman, M.; Lumme, S.; Lehikoinen, M.; Winell, K.; Keskimaki, I. Regional trends in avoidable hospitalizations due to complications among population with diabetes in Finland in 1996–2011: A register-based cohort study. BMJ Open 2016, 6, e011620. [Google Scholar] [CrossRef]
- Abdulrahman, G.O.; Amphlett, B.; Okosieme, O.E. Trends in hospital admissions with diabetic ketoacidosis in Wales, 1999–2010. Diabetes Res. Clin. Pract. 2013, 100, e7–e10. [Google Scholar] [CrossRef]
- Lopez-de-Andres, A.; Martinez-Huedo, M.A.; Carrasco-Garrido, P.; Hernandez-Barrera, V.; Gil-de-Miguel, A.; Jimenez-Garcia, R. Trends in lower-extremity amputations in people with and without diabetes in Spain, 2001–2008. Diabetes Care 2011, 34, 1570–1576. [Google Scholar] [CrossRef]
- Instituto Nacional de Gestión Sanitaria, Ministerio de Sanidad, Servicios Sociales e Igualdad. Conjunto Mínimo Básico de Datos, Hospitales del INSALUD. Available online: http://www.ingesa.msc.es/estadEstudios/documPublica/CMBD-2001.htm (accessed on 14 January 2019).
- Agency for Healthcare Research and Quality. Prevention Quality Indicators Technical Specifications Updates—Version 6.0 (ICD-9). 2016. Available online: http://www.qualityindicators.ahrq.gov/Modules/PQI_TechSpec_ICD09_v60.aspx (accessed on 27 October 2016).
- Kruzikas, D.T.; Jiang, H.J.; Remus, D.; Barrett, M.L.; Coffey, R.M.; Andrews, R. Preventable Hospitalizations: A Window into Primary and Preventive Care, 2000; HCUP Fact Book No. 5; AHRQ Publ. No. 04-0056; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2004.
- Lopez-de-Andres, A.; Jiménez-García, R.; Aragón-Sánchez, J.; Jiménez-Trujillo, I.; Hernández-Barrera, V.; Méndez-Bailón, M.; de Miguel-Yanes, J.M.; Perez-Farinos, N.; Carrasco-Garrido, P. National trends in incidence and outcomes in lower extremity amputations in people with and without diabetes in Spain, 2001–2012. Diabetes Res. Clin. Pract. 2015, 108, 499–507. [Google Scholar] [CrossRef]
- Alexander, G.C.; Sehgal, N.L.; Moloney, R.M.; Stafford, R.S. National trends in treatment of type 2 diabetes mellitus, 1994–2007. Arch. Intern. Med. 2008, 168, 2088–2094. [Google Scholar] [CrossRef]
- Ford, E.S.; Li, C.; Little, R.R.; Mokdad, A.H. Trends in A1C concentrations among U.S. adults with diagnosed diabetes from 1999 to 2004. Diabetes Care 2008, 31, 102–104. [Google Scholar] [CrossRef]
- Vinagre, I.; Mata-Cases, M.; Hermosilla, E.; Morros, R.; Fina, F.; Rosell, M.; Castell, C.; Franch-Nadal, J.; Bolíbar, B.; Mauricio, D. Control of glycemia and cardiovascular risk factors in patients with type 2 diabetes in primary care in Catalonia (Spain). Diabetes Care 2012, 35, 774–779. [Google Scholar] [CrossRef]
- Franch Nadal, J.; Artola Menéndez, S.; Diez Espino, J.; Mata Cases, M. The evolution of quality care indicators of patients with type 2 diabetes in the Spanish primary care (1996–2007). The RedGEDAPS quality of care program. Med. Clin. (Barc.) 2010, 135, 600–607. [Google Scholar] [CrossRef]
- Martínez-González, N.A.; Berchtold, P.; Ullman, K.; Busato, A.; Egger, M. Integrated care programmes for adults with chronic conditions: A meta-review. Int. J. Qual. Health Care 2014, 26, 561–570. [Google Scholar] [CrossRef]
- Russell, A.; Baxter, K.; Askew, D.; Tsai, J.; Ware, R.S.; Jackson, C.L. Model of care for the management of complex Type 2 diabetes managed in the community by primary care physicians with specialist support: An open controlled trial. Diabet. Med. 2013, 30, 1112–1121. [Google Scholar] [CrossRef]
- Hepworth, J.; Askew, D.; Jackson, C.; Russell, A. ‘Working with the team’: An exploratory study of improved type 2 diabetes management in a new model of integrated primary/secondary care. Aust. J. Prim. Health 2013, 19, 207–212. [Google Scholar] [CrossRef]
- Zhang, J.; Donald, M.; Baxter, K.A.; Ware, R.S.; Burridge, L.; Russell, A.W.; Jackson, C.L. Impact of an integrated model of care on potentially preventable hospitalizations for people with Type 2 diabetes mellitus. Diabet. Med. 2015, 32, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Booth, G.L.; Hux, J.E.; Fang, J.; Chan, B.T. Time trends and geographic disparities in acute complications of diabetes in Ontario, Canada. Diabetes Care 2005, 28, 1045–1050. [Google Scholar] [CrossRef] [PubMed]
- Sumner, W., 2nd; Hagen, M.D. Variation over time in preventable hospitalization rates across counties. J. Am. Board Fam. Med. 2011, 24, 639–646. [Google Scholar] [CrossRef]
- Balogh, R.S.; Lake, J.K.; Lin, E.; Wilton, A.; Lunsky, Y. Disparities in diabetes prevalence and preventable hospitalizations in people with intellectual and developmental disability: A population-based study. Diabet. Med. 2015, 32, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.F.; Chen, N.W.; Baillargeon, J.; Raji, M.A.; Goodwin, J.S. Potentially Preventable Hospitalizations in Medicare Patients With Diabetes: A Comparison of Primary Care Provided by Nurse Practitioners Versus Physicians. Med. Care 2015, 53, 776–783. [Google Scholar] [CrossRef]
- Moy, E.; Mau, M.K.; Raetzman, S.; Barrett, M.; Miyamura, J.B.; Chaves, K.H.; Andrews, R. Ethnic differences in potentially preventable hospitalizations among Asian Americans, Native Hawaiians, and other Pacific Islanders: Implications for reducing health care disparities. Ethn. Dis. 2013, 23, 6–11. [Google Scholar] [PubMed]
- Chen, P.C.; Tsai, C.Y.; Woung, L.C.; Lee, Y.C. Socioeconomic disparities in preventable hospitalization among adults with diabetes in Taiwan: A multilevel modelling approach. Int. J. Equity Health 2015, 14, 31. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| AAPC | 95%CI | p-Value (Trend) | |
|---|---|---|---|
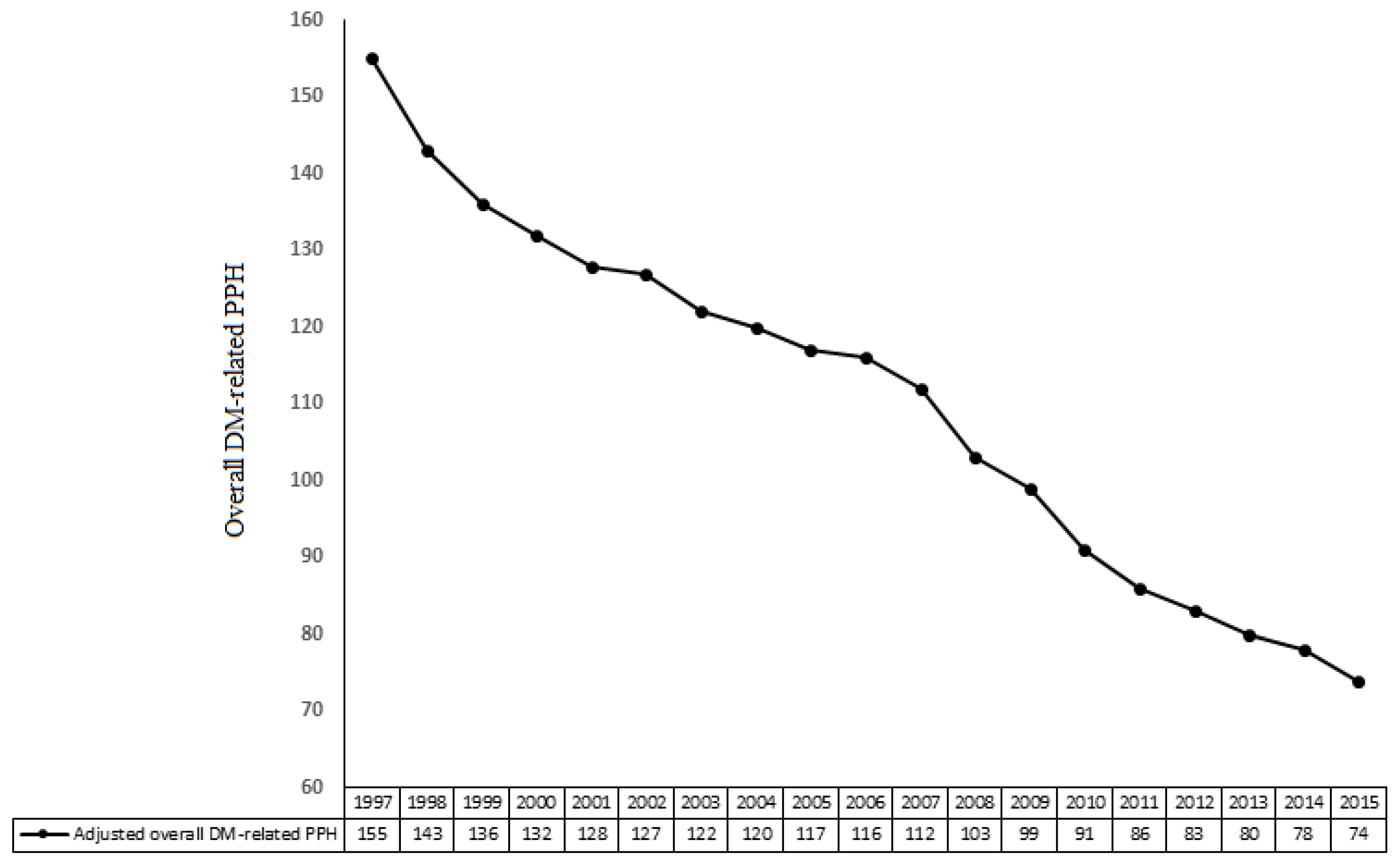
| Overall DM-related PPH | |||
| 18–44 years | −1.9 | −2.6 to −1.2 | <0.01 |
| 45–64 years | −3.4 | −4.2 to −3.0 | <0.001 |
| 65–74 years | −5.2 | −6.2 to −5.0 | <0.001 |
| ≥75 years | −6.0 | −6.6 to −5.4 | <0.001 |
| Male | −4.9 | −5.2 to −4.5 | <0.001 |
| Female | −5.8 | −6.4 to −5.4 | <0.001 |
| Total population | −5.1 | −5.6 to −4.7 | <0.001 |
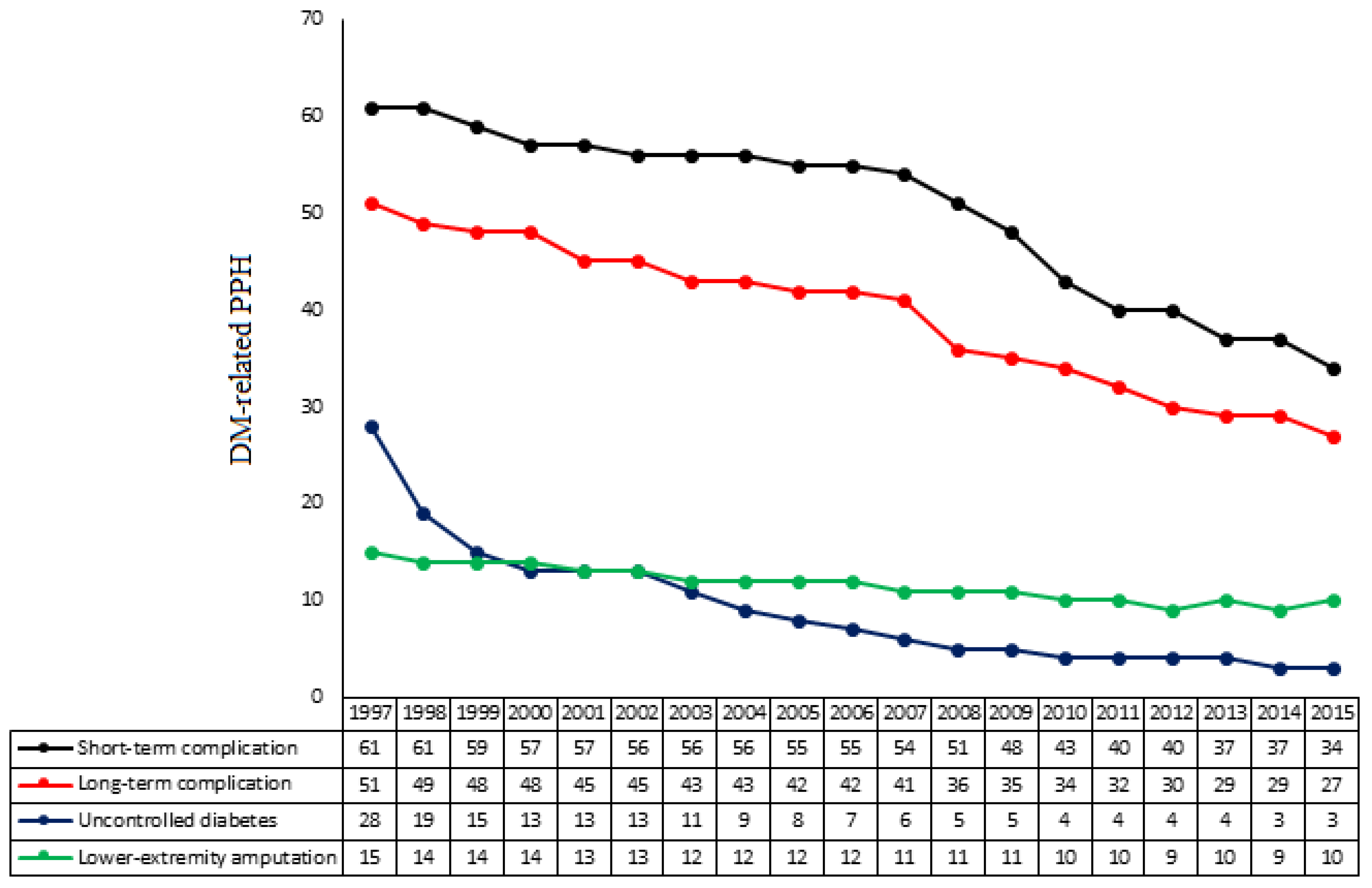
| Short-term complications | |||
| 18–44 years | −1.9 | −2.9 to −1.1 | <0.01 |
| 45–64 years | −3.7 | −4.2 to −3.1 | <0.001 |
| 65–74 years | −5.7 | −6.3 to −5.3 | <0.001 |
| ≥75 years | −6.0 | −6.5 to −5.5 | <0.001 |
| Male | −5.5 | −5.8 to −5.1 | <0.001 |
| Female | −5.1 | −5.7 to −4.5 | <0.001 |
| Total population | −5.4 | −6.1 to −4.9 | <0.001 |
| Long-term complication | |||
| 18–44 years | −1.9 | −2.8 to −1.3 | <0.01 |
| 45–64 years | −2.6 | −3.7 to −2.1 | <0.001 |
| 65–74 years | −3.9 | −4.6 to −3.0 | <0.001 |
| ≥75 years | −4.2 | −4.9 to −3.4 | <0.001 |
| Male | −4.0 | −4.5 to −3.5 | <0.001 |
| Female | −4.8 | −5.4 to −4.1 | <0.001 |
| Total population | −4.6 | −5.1 to −3.9 | <0.001 |
| Uncontrolled diabetes | |||
| 18–44 years | −2.4 | −3.2 to −1.9 | <0.001 |
| 45–64 years | −3.8 | −4.8 to −3.1 | <0.001 |
| 65–74 years | −5.1 | −6.0 to −4.4 | <0.001 |
| ≥75 years | −6.4 | −7.9 to −5.2 | <0.001 |
| Male | −6.1 | −6.9 to −5.3 | <0.001 |
| Female | −7.2 | −8.5 to −6.2 | <0.001 |
| Total population | −5.6 | -6.7 to −4.7 | <0.001 |
| Lower-extremity amputations | |||
| 18–44 years | −0.2 | −0.4 to −0.1 | 0.111 |
| 45–64 years | −0.3 | −0.5 to −0.1 | 0.104 |
| 65–74 years | −1.6 | −2.7 to −1.2 | <0.01 |
| ≥75 years | −2.0 | −4.0 to −2.1 | <0.001 |
| Male | −1.5 | −2.9 to −1.2 | <0.01 |
| Female | −3.0 | −4.0 to −2.4 | <0.001 |
| Total population | −1.9 | −3.0 to −1.3 | <0.01 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Huelgas, R.; Lara-Rojas, C.M.; López-Carmona, M.D.; Jansen-Chaparro, S.; Barba, R.; Zapatero, A.; Guijarro-Merino, R.; Tinahones, F.J.; Pérez-Belmonte, L.M.; Bernal-López, M.R. Trends in Diabetes-Related Potentially Preventable Hospitalizations in Adult Population in Spain, 1997–2015: A Nation-Wide Population-Based Study. J. Clin. Med. 2019, 8, 492. https://doi.org/10.3390/jcm8040492
Gómez-Huelgas R, Lara-Rojas CM, López-Carmona MD, Jansen-Chaparro S, Barba R, Zapatero A, Guijarro-Merino R, Tinahones FJ, Pérez-Belmonte LM, Bernal-López MR. Trends in Diabetes-Related Potentially Preventable Hospitalizations in Adult Population in Spain, 1997–2015: A Nation-Wide Population-Based Study. Journal of Clinical Medicine. 2019; 8(4):492. https://doi.org/10.3390/jcm8040492
Chicago/Turabian StyleGómez-Huelgas, Ricardo, Carmen M. Lara-Rojas, María D. López-Carmona, Sergio Jansen-Chaparro, Raquel Barba, Antonio Zapatero, Ricardo Guijarro-Merino, Francisco J. Tinahones, Luis M. Pérez-Belmonte, and M. Rosa. Bernal-López. 2019. "Trends in Diabetes-Related Potentially Preventable Hospitalizations in Adult Population in Spain, 1997–2015: A Nation-Wide Population-Based Study" Journal of Clinical Medicine 8, no. 4: 492. https://doi.org/10.3390/jcm8040492