

How Preoperative Closed Reduction and Time to Surgery Impact Postoperative Palmar Inclination in Distal Radius Fractures
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
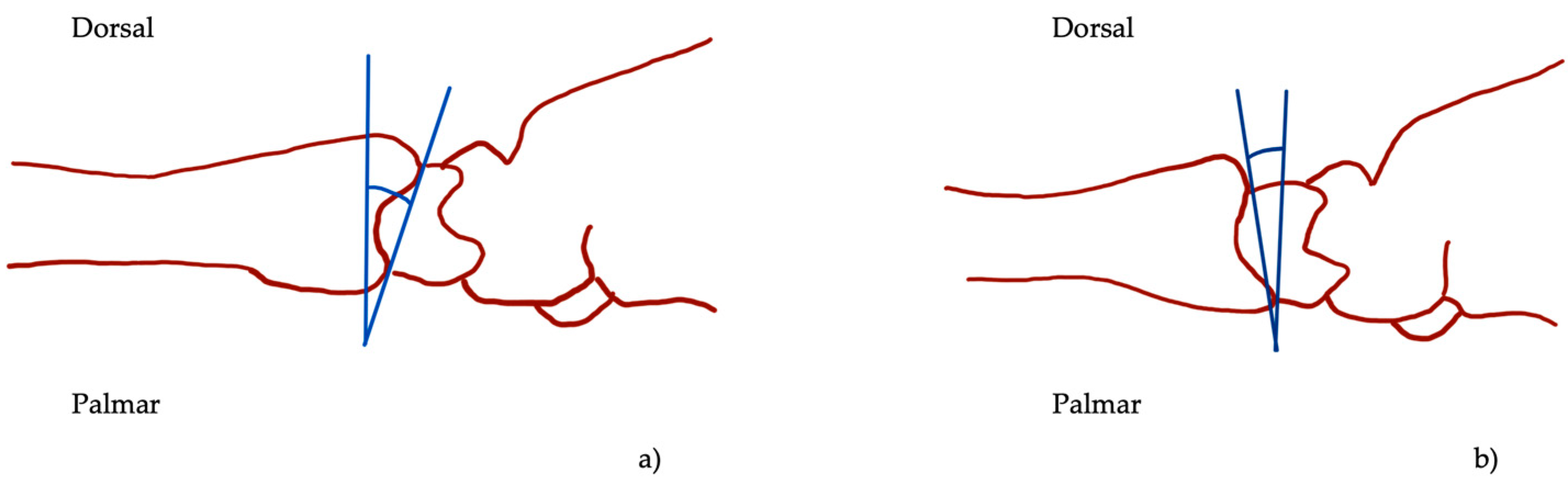
2.1. Experimental Setup
2.2. Patient Characteristics
2.3. Data Analysis
2.4. Statistical Methods
3. Results
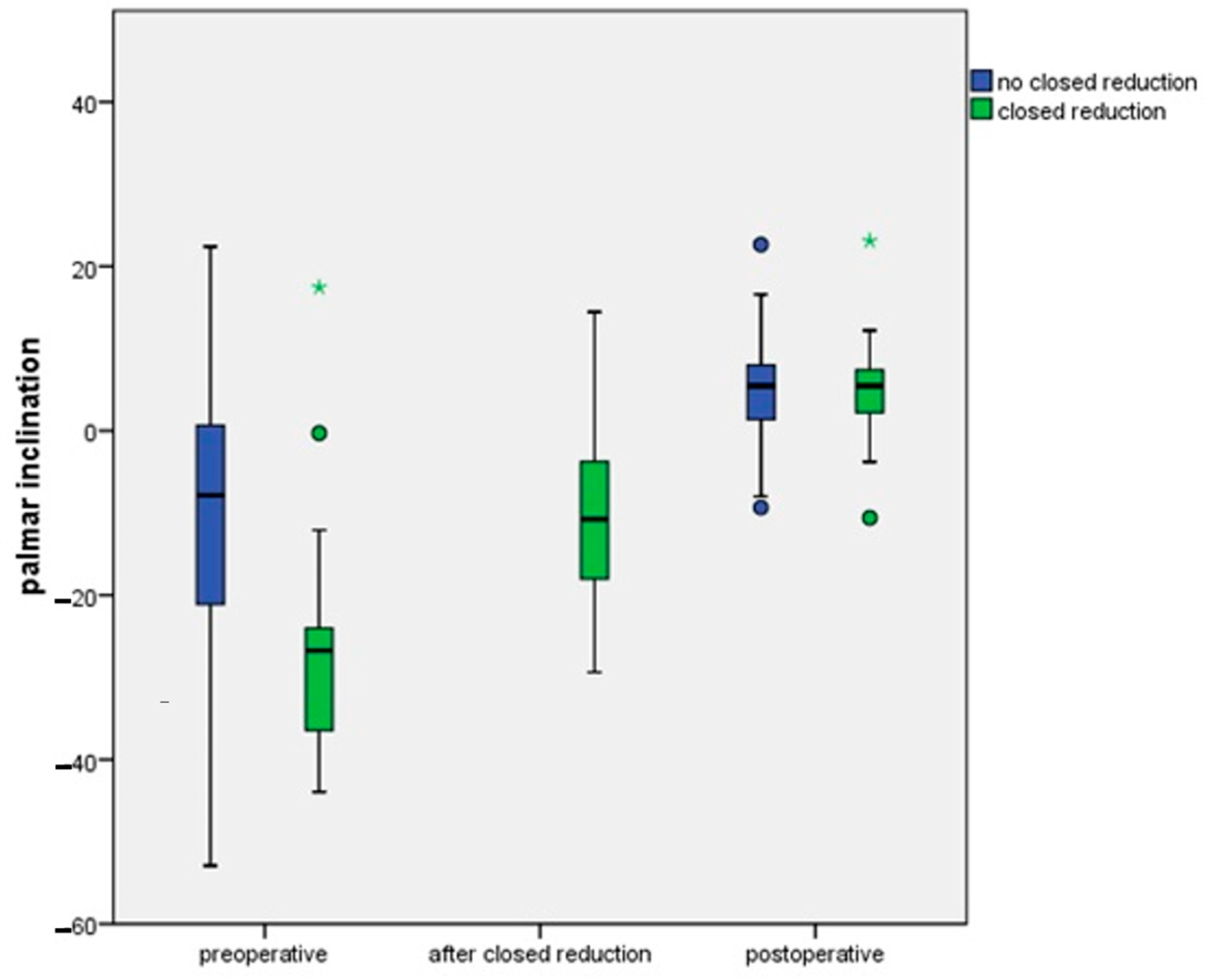
3.1. Radiological Measurements
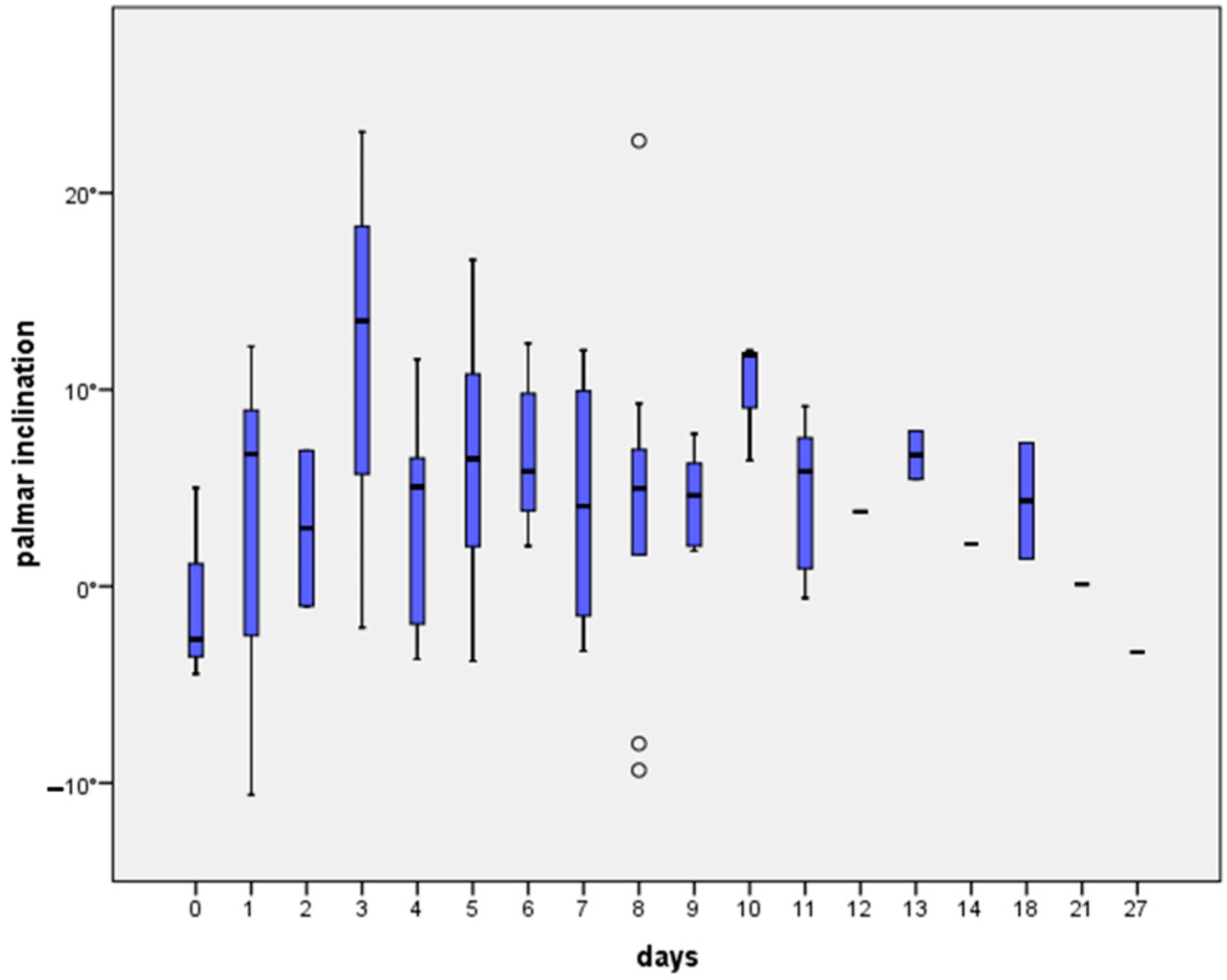
3.2. Time and Palmar Inclination
3.3. Interobserver Reliability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karl, J.W.; Olson, P.R.; Rosenwasser, M.P. The Epidemiology of Upper Extremity Fractures in the United States, 2009. J. Orthop. Trauma 2015, 29, e242–e244. [Google Scholar] [CrossRef] [PubMed]
- Dewan, N.; MacDermid, J.C.; Grewal, R.; Beattie, K. Risk factors predicting subsequent falls and osteoporotic fractures at 4 years after distal radius fracture-a prospective cohort study. Arch. Osteoporos. 2018, 13, 32. [Google Scholar] [CrossRef] [PubMed]
- Handoll, H.H.; Madhok, R. Surgical interventions for treating distal radial fractures in adults. Cochrane Database Syst. Rev. 2001, CD003209. [Google Scholar] [CrossRef]
- Autor, F.; Dresing, K.; Bonnaire, F.; Yves, D.P.-D.D.D.; Basel, P.A.S.; Locarno, M.A.S.; Wien, P.; Hamburg, K.-H.F.; Braunschweig, T.G.; Hamburg, L.G. Leitlinie Distale Radiusfraktur des Erwachsenen; DGU Leitlinien Kommission: Berlin, Germany, 2021. [Google Scholar]
- Singer, B.R.; McLauchlan, G.J.; Robinson, C.M.; Christie, J. Epidemiology of fractures in 15,000 adults: The influence of age and gender. J. Bone Jt. Surg. Br. 1998, 80, 243–248. [Google Scholar] [CrossRef]
- Lindau, T.R.; Aspenberg, P.; Arner, M.; Redlundh-Johnell, I.; Hagberg, L. Fractures of the distal forearm in young adults. An epidemiologic description of 341 patients. Acta Orthop. Scand. 1999, 70, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Barton, J.R. Views and Treatment of an Important Injury of the Wrist. Med. Exam (Phila) 1838, 1, 365–368. [Google Scholar] [CrossRef] [PubMed]
- Buxton, S.J. Colles and Carr: Some history of the wrist fracture. Ann. R. Coll. Surg. Engl. 1966, 38, 253–257. [Google Scholar] [PubMed]
- Peltier, L.F. Fractures of the distal end of the radius. An historical account. Clin. Orthop. Relat. Res. 1984, 187, 18–22. [Google Scholar] [CrossRef]
- Pulos, N.; Shin, A.Y. Strategies for Specific Reduction in High-Energy Distal Radius Fractures. Hand Clin. 2021, 37, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Mackenney, P.J.; McQueen, M.M.; Elton, R. Prediction of instability in distal radial fractures. J. Bone Jt. Surg. Am. 2006, 88, 1944–1951. [Google Scholar] [CrossRef]
- Dumont, C. Fractures, dislocations and subluxations of the upper extremity: Wrist. In Dresing K, Trafton PGStuttgart; Georg. Thieme Verlag/AO Foundation: New York, NY, USA, 2014; pp. 120–134. [Google Scholar]
- Leone, J.; Bhandari, M.; Adili, A.; McKenzie, S.; Moro, J.K.; Dunlop, R.B. Predictors of early and late instability following conservative treatment of extra-articular distal radius fractures. Arch. Orthop. Trauma Surg. 2004, 124, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Abramo, A.; Kopylov, P.; Tagil, M. Evaluation of a treatment protocol in distal radius fractures: A prospective study in 581 patients using DASH as outcome. Acta Orthop. 2008, 79, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.B. Distal radius fracture: Diagnosis, treatment, and controversies. Clin. Plast. Surg. 2014, 41, 481–499. [Google Scholar] [CrossRef] [PubMed]
- Rozental, T.D.; Blazar, P.E.; Franko, O.I.; Chacko, A.T.; Earp, B.E.; Day, C.S. Functional outcomes for unstable distal radial fractures treated with open reduction and internal fixation or closed reduction and percutaneous fixation. A prospective randomized trial. J. Bone Jt. Surg. Am. 2009, 91, 1837–1846. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.S.; Chun, K.J.; Kim, J.Y.; Lee, J.S. Necessity of acceptable radiologic alignment by preoperative closed reduction for unstable distal radius fractures treated with volar locking plates. Eur. J. Trauma Emerg. Surg. 2021, 47, 1881–1887. [Google Scholar] [CrossRef] [PubMed]
- Conry, K.T.; Weinberg, D.S.; Wilber, J.H.; Liu, R.W. Assessment of Splinting Quality: A Prospective Study Comparing Different Practitioners. Iowa Orthop. J. 2021, 41, 155. [Google Scholar] [PubMed]
- Tabrizi, A.; Mirza Tolouei, F.; Hassani, E.; Taleb, H.; Elmi, A. Hematoma Block Versus General Anesthesia in Distal Radius Fractures in Patients Over 60 Years in Trauma Emergency. Anesth. Pain Med. 2017, 7, e40619. [Google Scholar] [CrossRef] [PubMed]
- Handoll, H.H.; Madhok, R.; Dodds, C. Anaesthesia for treating distal radial fracture in adults. Cochrane Database Syst. Rev. 2002, 2002, CD003320. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Garcia, R.J.; Oda, T.; Shauver, M.J.; Chung, K.C. A systematic review of outcomes and complications of treating unstable distal radius fractures in the elderly. J. Hand Surg. 2011, 36, 824–835. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.; Gross, L. Treatment of distal radius fractures. J. Am. Acad. Orthop. Surg. 2013, 21, 502–505. [Google Scholar] [CrossRef] [PubMed]
- Levin, L.S.; Rozell, J.C.; Pulos, N. Distal Radius Fractures in the Elderly. J. Am. Acad. Orthop. Surg. 2017, 25, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Schermann, H.; Kadar, A.; Dolkart, O.; Atlan, F.; Rosenblatt, Y.; Pritsch, T. Repeated closed reduction attempts of distal radius fractures in the emergency department. Arch. Orthop. Trauma Surg. 2018, 138, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Löw, S.; Papay, M.; Spies, C.K.; Unglaub, F.; Eingartner, C. The Requirement for Closed Reduction of Dorsally Displaced Unstable Distal Radius Fractures Before Operative Treatment. Dtsch. Arztebl. Int. 2020, 117, 783–789. [Google Scholar] [CrossRef]
- Tuohy, C.J.; Weikert, D.R.; Watson, J.T.; Lee, D.H. Hand and body radiation exposure with the use of mini C-arm fluoroscopy. J. Hand Surg. 2011, 36, 632–638. [Google Scholar] [CrossRef]
- Appukuttan, A.; Chukwulobelu, R.; Ragoowansi, R. ‘Hands up technique’: An alternative surgical setup for Brachioplasty. JPRAS Open 2019, 21, 23–27. [Google Scholar] [CrossRef]
- Tsuge, S.; Nakamura, R. Anatomical risk factors for Kienbock’s disease. J. Hand Surg. 1993, 18, 70–75. [Google Scholar] [CrossRef]
- Howard, M.; Curtis, A.; Everett, S.; Harries, L.; Donaldson, O.; Sheridan, B. Does a delay in surgery for distal radial fractures affect patient outcome? J. Hand Surg. Eur. Vol. 2021, 46, 69–74. [Google Scholar] [CrossRef]
- Arora, R.; Lutz, M.; Deml, C.; Krappinger, D.; Haug, L.; Gabl, M. A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and older. J. Bone Jt. Surg. Am. 2011, 93, 2146–2153. [Google Scholar] [CrossRef] [PubMed]
- Azzopardi, T.; Ehrendorfer, S.; Coulton, T.; Abela, M. Unstable extra-articular fractures of the distal radius: A prospective, randomised study of immobilisation in a cast versus supplementary percutaneous pinning. J. Bone Jt. Surg. Br. 2005, 87, 837–840. [Google Scholar] [CrossRef]
- Egol, K.A.; Walsh, M.; Romo-Cardoso, S.; Dorsky, S.; Paksima, N. Distal radial fractures in the elderly: Operative compared with nonoperative treatment. J. Bone Jt. Surg. Am. 2010, 92, 1851–1857. [Google Scholar] [CrossRef] [PubMed]
- Kreder, H.J.; Hanel, D.P.; McKee, M.; Jupiter, J.; McGillivary, G.; Swiontkowski, M.F. X-ray film measurements for healed distal radius fractures. J. Hand Surg. 1996, 21, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Gliatis, J.D.; Plessas, S.J.; Davis, T.R. Outcome of distal radial fractures in young adults. J. Hand Surg. 2000, 25, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Hammert, W.C.; Kramer, R.C.; Graham, B.; Keith, M.W. AAOS appropriate use criteria: Treatment of distal radius fractures. J. Am. Acad. Orthop. Surg. 2013, 21, 506–509. [Google Scholar] [CrossRef] [PubMed]
- Minnema, A.J.; Mehta, A.; Boling, W.W.; Schwab, J.; Simard, J.M.; Farhadi, H.F. SCING-Spinal Cord Injury Neuroprotection with Glyburide: A pilot, open-label, multicentre, prospective evaluation of oral glyburide in patients with acute traumatic spinal cord injury in the USA. BMJ Open 2019, 9, e031329. [Google Scholar] [CrossRef] [PubMed]
- Brogren, E.; Hofer, M.; Petranek, M.; Dahlin, L.B.; Atroshi, I. Fractures of the distal radius in women aged 50 to 75 years: Natural course of patient-reported outcome, wrist motion and grip strength between 1 year and 2-4 years after fracture. J. Hand Surg. Eur. Vol. 2011, 36, 568–576. [Google Scholar] [CrossRef] [PubMed]
- Anzarut, A.; Johnson, J.A.; Rowe, B.H.; Lambert, R.G.; Blitz, S.; Majumdar, S.R. Radiologic and patient-reported functional outcomes in an elderly cohort with conservatively treated distal radius fractures. J. Hand Surg. 2004, 29, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Fujii, K.; Henmi, T.; Kanematsu, Y.; Mishiro, T.; Sakai, T.; Terai, T. Fractures of the distal end of radius in elderly patients: A comparative study of anatomical and functional results. J. Orthop. Surg. 2002, 10, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Kelly, A.J.; Warwick, D.; Crichlow, T.P.; Bannister, G.C. Is manipulation of moderately displaced Colles’ fracture worthwhile? A prospective randomized trial. Injury 1997, 28, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Aro, H.T.; Koivunen, T. Minor axial shortening of the radius affects outcome of Colles’ fracture treatment. J. Hand Surg. 1991, 16, 392–398. [Google Scholar] [CrossRef]
- Kodama, N.; Takemura, Y.; Ueba, H.; Imai, S.; Matsusue, Y. Acceptable parameters for alignment of distal radius fracture with conservative treatment in elderly patients. J. Orthop. Sci. 2014, 19, 292–297. [Google Scholar] [CrossRef] [PubMed]
- McQueen, M.; Caspers, J. Colles fracture: Does the anatomical result affect the final function? J. Bone Jt. Surg. Br. 1988, 70, 649–651. [Google Scholar] [CrossRef] [PubMed]
- Orbay, J.L.; Fernandez, D.L. Volar fixation for dorsally displaced fractures of the distal radius: A preliminary report. J. Hand Surg. 2002, 27, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Orbay, J.L.; Fernandez, D.L. Volar fixed-angle plate fixation for unstable distal radius fractures in the elderly patient. J. Hand Surg. 2004, 29, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Prommersberger, K.J.; Van Schoonhoven, J.; Lanz, U.B. Outcome after corrective osteotomy for malunited fractures of the distal end of the radius. J. Hand Surg. 2002, 27, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Ochen, Y.; Peek, J.; van der Velde, D.; Beeres, F.J.P.; van Heijl, M.; Groenwold, R.H.H.; Houwert, R.M.; Heng, M. Operative vs Nonoperative Treatment of Distal Radius Fractures in Adults: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e203497. [Google Scholar] [CrossRef] [PubMed]
- Katt, B.; Seigerman, D.; Lutsky, K.; Beredjiklian, P. Distal Radius Malunion. J. Hand Surg. 2020, 45, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Grewal, R.; MacDermid, J.C. The risk of adverse outcomes in extra-articular distal radius fractures is increased with malalignment in patients of all ages but mitigated in older patients. J. Hand Surg. 2007, 32, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Synn, A.J.; Makhni, E.C.; Makhni, M.C.; Rozental, T.D.; Day, C.S. Distal radius fractures in older patients: Is anatomic reduction necessary? Clin. Orthop. Relat. Res. 2009, 467, 1612–1620. [Google Scholar] [CrossRef] [PubMed]
- Jaremko, J.L.; Lambert, R.G.; Rowe, B.H.; Johnson, J.A.; Majumdar, S.R. Do radiographic indices of distal radius fracture reduction predict outcomes in older adults receiving conservative treatment? Clin. Radiol. 2007, 62, 65–72. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Pre-op | Reduction (n) | Post-op | Pre-Reduction (n) | Post-Reduction | Difference Pre–Post Surgery | Difference from Ideal | |
|---|---|---|---|---|---|---|---|
| A2 (n = 6) | −35.0 ± 8.4 | −12.5 ± 8.6 (3) | 3.3 ± 2.2 | 23.7 ± 12.4 (3) | 19.0 ± 9.0 (3) | 38.3 ± 7.1 | 6.7 ± 2.2 |
| A3 (n = 11) | −17.9 ± 4.2 | −7.8 ± 1.8 (5) | 7.1 ± 2.3 | 17.2 ± 5.0 (5) | 16.6 ± 5.2 (5) | 25.0 ± 4.2 | 2.9 ± 2.3 |
| C1 (n = 3) | 2.6 ± 6.4 | --- (1) | 14.1 ± 4.4 | --- (1) | --- (1) | 11.5 ± 2.0 | 4.1 ± 4.4 |
| C2 (n = 13) | −7.0 ± 4.1 | −2.0 ± 8.4 (3) | 6.3 ± 1.7 | 7.9 ± 5.7 (3) | 8.6 ± 5.5 (3) | 13.3 ± 3.2 | 3.6 ± 1.7 |
| C3 (n = 47) | −15.0 ± 2.8 | −14.9 ± 2.4 (9) | 3.6 ± 0.8 | 18.4 ± 4.2 (9) | 16.0 ± 2.6 (9) | 18.6 ± 2.6 | 6.3 ± 0.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beyer, F.; Oppermann, J.; Prasse, T.; Müller, L.P.; Eysel, P.; Bredow, J. How Preoperative Closed Reduction and Time to Surgery Impact Postoperative Palmar Inclination in Distal Radius Fractures. J. Clin. Med. 2024, 13, 2316. https://doi.org/10.3390/jcm13082316
Beyer F, Oppermann J, Prasse T, Müller LP, Eysel P, Bredow J. How Preoperative Closed Reduction and Time to Surgery Impact Postoperative Palmar Inclination in Distal Radius Fractures. Journal of Clinical Medicine. 2024; 13(8):2316. https://doi.org/10.3390/jcm13082316
Chicago/Turabian StyleBeyer, Frank, Johannes Oppermann, Tobias Prasse, Lars Peter Müller, Peer Eysel, and Jan Bredow. 2024. "How Preoperative Closed Reduction and Time to Surgery Impact Postoperative Palmar Inclination in Distal Radius Fractures" Journal of Clinical Medicine 13, no. 8: 2316. https://doi.org/10.3390/jcm13082316