

Whole-Body Cryostimulation in Multiple Sclerosis: A Scoping Review
 ,
,  , , , ,
, , , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Search Processing
2.3. Inclusion and Exclusion Criteria
2.4. Selection of Sources of Evidence
2.5. Data Extraction
2.6. Synthesis of Results
3. Results
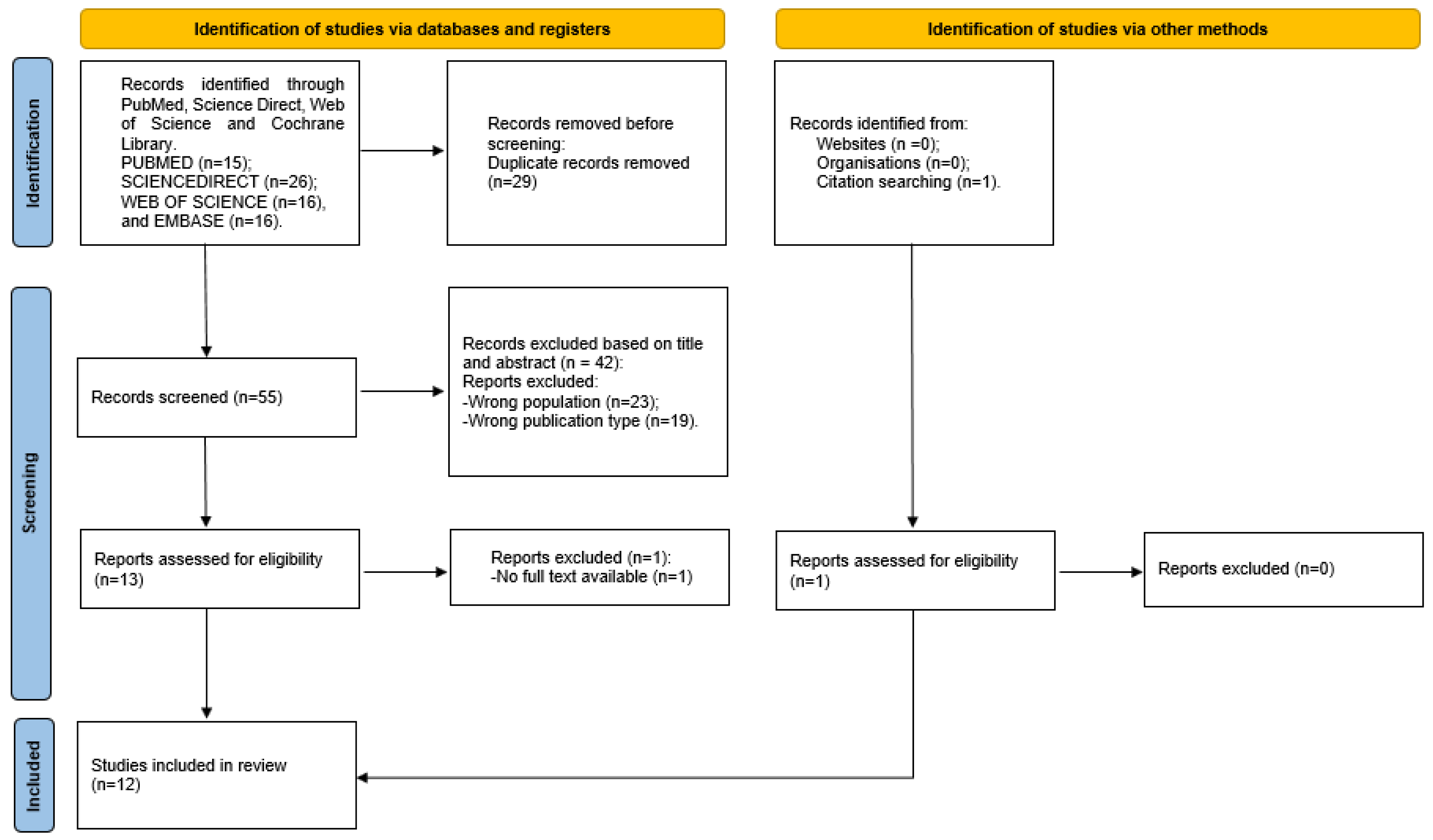
3.1. Study Selection
3.2. Study Features
3.3. WBC Application Modality
3.4. Outcome Measures
3.4.1. Blood Values
3.4.2. Functional Evaluation
3.4.3. Psychological Effects
3.5. Adverse Effects
4. Discussion
4.1. Physiological Parameters
4.1.1. Antioxidative Capacity and Antioxidant Enzymes
- -
- WBC can increase the TAS and could play an important role in the activation process of antioxidative properties in MS patients, suggesting the positive antioxidant effects of WBC as a short-term adjuvant treatment for MS.
- -
- No significant changes in antioxidant enzymes (CAT, GPx, and R-GSSG) were detected, except for SOD when the WBC sessions increased to 30, suggesting that different cooling interventions could affect changes in the antioxidant capacity.
4.1.2. Nitric Oxide
- -
- No significant impact of WBC on NO concentration was reported.
4.1.3. Uric Acid Plasma Concentration
- -
- WBC can increase the plasma UA levels in SPMS patients not only immediately, but also one and three months later.
4.1.4. Metalloproteinases’ Serum Levels
- -
- WBC seems to have no effect on the level of MMP-9 in females with MS.
4.1.5. Haematological Parameters and Inflammatory Markers
- -
- A cycle of 20 WBCs did not influence changes in the blood counts, rheology, and biochemistry in women with MS.
- -
- The use of WBC had a positive effect on the rheological properties of blood, increasing the deformability of erythrocytes and decreasing the Hct values (within the physiological norms) of healthy women.
- -
- WBC does not adversely affect RBC deformability and aggregation, making it safe for MS patients.
4.2. Physical, Functional, and Psychological Parameters
- -
- WBC can lead to a reduction in fatigue and an improvement in functional status, potentially improving the overall well-being and quality of life of people with MS.
- -
- Cryostimulation has a significant effect on both mental and physical well-being, with a particular focus on improving the symptoms of mood, anxiety, and depression.
- -
- The effects of WBC on improvements in functional status observed in people with MS may be due to adaptive changes in bioelectrical muscle activity.
4.3. Limitations
5. Conclusions
6. Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ghasemi, N.; Razavi, S.; Nikzad, E. Multiple Sclerosis: Pathogenesis, Symptoms, Diagnoses and Cell-Based Therapy. Cell J. 2017, 19, 1–10. [Google Scholar] [CrossRef]
- Ramagopalan, S.V.; Sadovnick, A.D. Epidemiology of multiple sclerosis. Neurol. Clin. 2011, 29, 207–217. [Google Scholar] [CrossRef]
- Dimitrov, L.G.; Turner, B. What’s new in multiple sclerosis? Br. J. Gen. Pract. 2014, 64, 612–613. [Google Scholar] [CrossRef]
- Barkhane, Z.; Elmadi, J.; Satish Kumar, L.; Pugalenthi, L.S.; Ahmad, M.; Reddy, S. Multiple Sclerosis and Autoimmunity: A Veiled Relationship. Cureus 2022, 14, e24294. [Google Scholar] [CrossRef]
- Landry, R.L.; Embers, M.E. The Probable Infectious Origin of Multiple Sclerosis. NeuroSci 2023, 4, 211–234. [Google Scholar] [CrossRef]
- Briones-Buixassa, L.; Milà, R.; Aragonès, J.M.; Bufill, E.; Olaya, B.; Arrufat, F.X. Stress and multiple sclerosis: A systematic review considering potential moderating and mediating factors and methods of assessing stress. Health Psychol. Open 2015, 2, 2055102915612271. [Google Scholar] [CrossRef]
- Kamel, F.O. Factors Involved in Relapse of Multiple Sclerosis. J. Microsc. Ultrastruct. 2019, 7, 103–108. [Google Scholar] [CrossRef]
- Kuhlmann, T.; Moccia, M.; Coetzee, T.; Cohen, J.A.; Correale, J.; Graves, J.; Marrie, R.A.; Montalban, X.; Yong, V.W.; Thompson, A.J.; et al. Multiple sclerosis progression: Time for a new mechanism-driven framework. Lancet Neurol. 2023, 22, 78–88. [Google Scholar] [CrossRef]
- Dimitriou, N.G.; Meuth, S.G.; Martinez-Lapiscina, E.H.; Albrecht, P.; Menge, T. Treatment of Patients with Multiple Sclerosis Transitioning Between Relapsing and Progressive Disease. CNS Drugs 2023, 37, 69–92. [Google Scholar] [CrossRef] [PubMed]
- Klineova, S.; Lublin, F.D. Clinical Course of Multiple Sclerosis. Cold Spring Harb. Perspect. Med. 2018, 8, a028928. [Google Scholar] [CrossRef] [PubMed]
- Silveira, C.; Guedes, R.; Maia, D.; Curral, R.; Coelho, R. Neuropsychiatric Symptoms of Multiple Sclerosis: State of the Art. Psychiatry Investig. 2019, 16, 877–888. [Google Scholar] [CrossRef]
- Lassmann, H. Pathogenic Mechanisms Associated With Different Clinical Courses of Multiple Sclerosis. Front. Immunol. 2018, 9, 3116. [Google Scholar] [CrossRef]
- Ohl, K.; Tenbrock, K.; Kipp, M. Oxidative stress in multiple sclerosis: Central and peripheral mode of action. Exp. Neurol. 2016, 277, 58–67. [Google Scholar] [CrossRef]
- Sudol-Szopinska, I.; Pracon, G. Diagnostic imaging of psoriatic arthritis. Part II: Magnetic resonance imaging and ultrasonography. J. Ultrason. 2016, 16, 163–174. [Google Scholar] [CrossRef]
- Besler, H.T.; Çomoğlu, S. Lipoprotein Oxidation, Plasma Total Antioxidant Capacity and Homocysteine Level in Patients with Multiple Sclerosis. Nutr. Neurosci. 2003, 6, 189–196. [Google Scholar] [CrossRef]
- Glabinski, A.; Tawsek, N.S.; Bartosz, G. Increased generation of superoxide radicals in the blood of MS patients. Acta Neurol. Scand. 1993, 88, 174–177. [Google Scholar] [CrossRef]
- Lu, F.; Selak, M.; O’Connor, J.; Croul, S.; Lorenzana, C.; Butunoi, C.; Kalman, B. Oxidative damage to mitochondrial DNA and activity of mitochondrial enzymes in chronic active lesions of multiple sclerosis. J. Neurol. Sci. 2000, 177, 95–103. [Google Scholar] [CrossRef]
- Vladimirova, O.; Lu, F.M.; Shawver, L.; Kalman, B. The activation of protein kinase C induces higher production of reactive oxygen species by mononuclear cells in patients with multiple sclerosis than in controls. Inflamm. Res. 1999, 48, 412–416. [Google Scholar] [CrossRef]
- Hoftberger, R.; Lassmann, H. Inflammatory demyelinating diseases of the central nervous system. Handb. Clin. Neurol. 2017, 145, 263–283. [Google Scholar] [CrossRef] [PubMed]
- Popescu, B.F.; Pirko, I.; Lucchinetti, C.F. Pathology of multiple sclerosis: Where do we stand? Contin. Lifelong Learn. Neurol. 2013, 19, 901–921. [Google Scholar] [CrossRef] [PubMed]
- Cree, B.A.C.; Arnold, D.L.; Chataway, J.; Chitnis, T.; Fox, R.J.; Pozo Ramajo, A.; Murphy, N.; Lassmann, H. Secondary Progressive Multiple Sclerosis: New Insights. Neurology 2021, 97, 378–388. [Google Scholar] [CrossRef] [PubMed]
- Faraclas, E. Interventions to Improve Quality of Life in Multiple Sclerosis: New Opportunities and Key Talking Points. Degener. Neurol. Neuromuscul. Dis. 2023, 13, 55–68. [Google Scholar] [CrossRef]
- Ayache, S.S.; Serratrice, N.; Abi Lahoud, G.N.; Chalah, M.A. Fatigue in Multiple Sclerosis: A Review of the Exploratory and Therapeutic Potential of Non-Invasive Brain Stimulation. Front. Neurol. 2022, 13, 813965. [Google Scholar] [CrossRef]
- Miller, E. Multiple sclerosis. Adv. Exp. Med. Biol. 2012, 724, 222–238. [Google Scholar] [CrossRef]
- Christogianni, A.; O’Garro, J.; Bibb, R.; Filtness, A.; Filingeri, D. Heat and cold sensitivity in multiple sclerosis: A patient-centred perspective on triggers, symptoms, and thermal resilience practices. Mult. Scler. Relat. Disord. 2022, 67, 104075. [Google Scholar] [CrossRef]
- Flensner, G.; Ek, A.C.; Soderhamn, O.; Landtblom, A.M. Sensitivity to heat in MS patients: A factor strongly influencing symptomology--an explorative survey. BMC Neurol. 2011, 11, 27. [Google Scholar] [CrossRef] [PubMed]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Rudick, R.A.; Lee, J.C.; Cutter, G.R.; Miller, D.M.; Bourdette, D.; Weinstock-Guttman, B.; Hyde, R.; Zhang, H.; You, X. Disability progression in a clinical trial of relapsing-remitting multiple sclerosis: Eight-year follow-up. Arch. Neurol. 2010, 67, 1329–1335. [Google Scholar] [CrossRef]
- Hauser, S.L.; Cree, B.A.C. Treatment of Multiple Sclerosis: A Review. Am. J. Med. 2020, 133, 1380–1390.e2. [Google Scholar] [CrossRef]
- Amin, M.; Hersh, C.M. Updates and advances in multiple sclerosis neurotherapeutics. Neurodegener. Dis. Manag. 2023, 13, 47–70. [Google Scholar] [CrossRef]
- Yang, J.H.; Rempe, T.; Whitmire, N.; Dunn-Pirio, A.; Graves, J.S. Therapeutic Advances in Multiple Sclerosis. Front. Neurol. 2022, 13, 824926. [Google Scholar] [CrossRef]
- Duan, H.; Jing, Y.; Li, Y.; Lian, Y.; Li, J.; Li, Z. Rehabilitation treatment of multiple sclerosis. Front. Immunol. 2023, 14, 1168821. [Google Scholar] [CrossRef]
- Dighriri, I.M.; Aldalbahi, A.A.; Albeladi, F.; Tahiri, A.A.; Kinani, E.M.; Almohsen, R.A.; Alamoudi, N.H.; Alanazi, A.A.; Alkhamshi, S.J.; Althomali, N.A.; et al. An Overview of the History, Pathophysiology, and Pharmacological Interventions of Multiple Sclerosis. Cureus 2023, 15, e33242. [Google Scholar] [CrossRef]
- Russo, M.; Maggio, M.G.; Naro, A.; Portaro, S.; Porcari, B.; Balletta, T.; De Luca, R.; Raciti, L.; Calabrò, R.S. Can powered exoskeletons improve gait and balance in multiple sclerosis? A retrospective study. Int. J. Rehabil. Res. 2021, 44, 126–130. [Google Scholar] [CrossRef]
- Halabchi, F.; Alizadeh, Z.; Sahraian, M.A.; Abolhasani, M. Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC Neurol. 2017, 17, 185. [Google Scholar] [CrossRef]
- Heine, M.; van de Port, I.; Rietberg, M.B.; van Wegen, E.E.; Kwakkel, G. Exercise therapy for fatigue in multiple sclerosis. Cochrane Database Syst. Rev. 2015, 2015, CD009956. [Google Scholar] [CrossRef]
- Celesti, A.; Cimino, V.; Naro, A.; Portaro, S.; Fazio, M.; Villari, M.; Calabró, R.S. Recent Considerations on Gaming Console Based Training for Multiple Sclerosis Rehabilitation. Med. Sci. 2022, 10, 13. [Google Scholar] [CrossRef]
- Lombardi, G.; Ziemann, E.; Banfi, G. Whole-Body Cryotherapy in Athletes: From Therapy to Stimulation. An Updated Review of the Literature. Front. Physiol. 2017, 8, 258. [Google Scholar] [CrossRef]
- Fontana, J.M.; Alito, A.; Pitera, P.; Verme, F.; Cattaldo, S.; Cornacchia, M.; Mai, S.; Brunani, A.; Capodaglio, P. Whole-Body Cryostimulation in Post-COVID Rehabilitation for Patients with Obesity: A Multidisciplinary Feasibility Study. Biomedicines 2023, 11, 3092. [Google Scholar] [CrossRef]
- Zakynthinos, G.E.; Stavrou, V.T.; Malli, F.; Papathanasiou, I.V.; Zakynthinos, E.; Gourgoulianis, K.I.; Kalabakas, K.; Karagiannis, D.; Basdekis, G. The Effect of Whole-Body Cryostimulation in Healthy Adults: Whole-Body Cryostimulation According to Gender and Smoking Status. Adv. Exp. Med. Biol. 2021, 1337, 315–321. [Google Scholar] [CrossRef]
- Miller, E.; Kostka, J.; Wlodarczyk, T.; Dugue, B. Whole-body cryostimulation (cryotherapy) provides benefits for fatigue and functional status in multiple sclerosis patients. A case-control study. Acta Neurol. Scand. 2016, 134, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Piterà, P.; Springhetti, I.; Alito, A.; Verme, F.; Fontana, J.M.; Capodaglio, P. Whole-Body Cryostimulation, a Complementary Treatment for Phantom Limb Syndrome: Preliminary Evidence from a Case Study. Medicina 2024, 60, 22. [Google Scholar] [CrossRef] [PubMed]
- Rymaszewska, J.; Lion, K.M.; Pawlik-Sobecka, L.; Pawłowski, T.; Szcześniak, D.; Trypka, E.; Rymaszewska, J.E.; Zabłocka, A.; Stanczykiewicz, B. Efficacy of the Whole-Body Cryotherapy as Add-on Therapy to Pharmacological Treatment of Depression-A Randomized Controlled Trial. Front. Psychiatry 2020, 11, 522. [Google Scholar] [CrossRef] [PubMed]
- Verme, F.; Scarpa, A.; Varallo, G.; Pitera, P.; Capodaglio, P.; Fontana, J.M. Effects of Whole-Body Cryostimulation on Pain Management and Disease Activity in Active Rheumatic Polymyalgia: A Case-Report. Biomedicines 2023, 11, 1594. [Google Scholar] [CrossRef] [PubMed]
- Guillot, X.; Tordi, N.; Mourot, L.; Demougeot, C.; Dugue, B.; Prati, C.; Wendling, D. Cryotherapy in inflammatory rheumatic diseases: A systematic review. Expert Rev. Clin. Immunol. 2014, 10, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Verme, F.; Fontana, J.M.; Pitera, P.; Alito, A.; Saffioti, S.; Baccalaro, G.; Zebellin, G.; Capodaglio, P. Whole-Body Cryostimulation in Functional Neurological Disorders: A Case Report. Healthcare 2023, 12, 71. [Google Scholar] [CrossRef] [PubMed]
- Miller, E. Cryostimulation factor supporting rehabilitation patients with multiple sclerosis and fatigue syndrome. Wiad. Lek. 2010, 63, 41–45. [Google Scholar] [PubMed]
- Miller, E.; Mrowicka, M.; Malinowska, K.; Mrowicki, J.; Saluk-Juszczak, J.; Kedziora, J. Effects of whole-body cryotherapy on a total antioxidative status and activities of antioxidative enzymes in blood of depressive multiple sclerosis patients. World J. Biol. Psychiatry 2011, 12, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Ptaszek, B.; Podsiadlo, S.; Czerwinska-Ledwig, O.; Teleglow, A.; Pilch, W.; Wojcik, A.; Sadowska-Krepa, E. The effect of a series of whole-body cryotherapy treatments on the activity of antioxidant enzymes in healthy women and women with multiple sclerosis. Acta Neurobiol. Exp. 2023, 83, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Ptaszek, B.; Podsiadlo, S.; Adamiak, J.; Marchewka, J.; Tota, L.; Teleglow, A. Effect of Whole-Body Cryotherapy on Oxidant-Antioxidant Imbalance in Women with Multiple Sclerosis. J. Clin. Med. 2023, 12, 5958. [Google Scholar] [CrossRef] [PubMed]
- Ptaszek, B.; Podsiadlo, S.; Czerwinska-Ledwig, O.; Maciejczyk, M.; Teleglow, A. Effect of Whole-Body Cryotherapy on Iron Status and Biomarkers of Neuroplasticity in Multiple Sclerosis Women. Healthcare 2022, 10, 1681. [Google Scholar] [CrossRef] [PubMed]
- Radecka, A.; Knyszynska, A.; Luczak, J.; Lubkowska, A. Adaptive changes in muscle activity after cryotherapy treatment: Potential mechanism for improvement the functional state in patients with multiple sclerosis. NeuroRehabilitation 2021, 48, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Ptaszek, B.; Teleglow, A.; Adamiak, J.; Glodzik, J.; Podsiadlo, S.; Mucha, D.; Marchewka, J.; Halski, T.; Mucha, D. Effect of Whole-Body Cryotherapy on Morphological, Rheological and Biochemical Indices of Blood in People with Multiple Sclerosis. J. Clin. Med. 2021, 10, 2833. [Google Scholar] [CrossRef] [PubMed]
- Lubkowska, A.; Radecka, A.; Knyszyńska, A.; Łuczak, J. Effect of whole-body cryotherapy treatments on the functional state of patients with MS (multiple sclerosis) in a Timed 25-Foot Walk Test and Hand Grip Strength Test. Pomeranian J. Life Sci. 2019, 65, 46–49. [Google Scholar] [CrossRef]
- Pawik, M.; Kowalska, J.; Rymaszewska, J. The effectiveness of whole-body cryotherapy and physical exercises on the psychological well-being of patients with multiple sclerosis: A comparative analysis. Adv. Clin. Exp. Med. 2019, 28, 1477–1483. [Google Scholar] [CrossRef] [PubMed]
- Bryczkowska, I.; Radecka, A.; Knyszyńska, A.; Łuczak, J.; Lubkowska, A. Effect of whole body cryotherapy treatments on antioxidant enzyme activity and biochemical parameters in patients with multiple sclerosis. Fam. Med. Amp Prim. Care Rev. 2018, 20, 214–217. [Google Scholar] [CrossRef]
- Miller, E.; Saluk, J.; Morel, A.; Wachowicz, B. Long-term effects of whole body cryostimulation on uric acid concentration in plasma of secondary progressive multiple sclerosis patients. Scand. J. Clin. Lab. Investig. 2013, 73, 635–640. [Google Scholar] [CrossRef]
- Miller, E.; Mrowicka, M.; Malinowska, K.; Mrowicki, J.; Saluk-Juszczak, J.; Kędziora, J. The effects of whole-body cryotherapy on oxidative stress in multiple sclerosis patients. J. Therm. Biol. 2010, 35, 406–410. [Google Scholar] [CrossRef]
- Miller, E.; Mrowicka, M.; Malinowska, K.; Zolynski, K.; Kedziora, J. Effects of the whole-body cryotherapy on a total antioxidative status and activities of some antioxidative enzymes in blood of patients with multiple sclerosis-preliminary study. J. Med. Investig. 2010, 57, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Ienco, E.C.; LoGerfo, A.; Carlesi, C.; Orsucci, D.; Ricci, G.; Mancuso, M.; Siciliano, G. Oxidative stress treatment for clinical trials in neurodegenerative diseases. J. Alzheimer’s Dis. 2011, 24 (Suppl. S2), 111–126. [Google Scholar] [CrossRef] [PubMed]
- Jena, A.B.; Samal, R.R.; Bhol, N.K.; Duttaroy, A.K. Cellular Red-Ox system in health and disease: The latest update. Biomed. Pharmacother. 2023, 162, 114606. [Google Scholar] [CrossRef] [PubMed]
- Dugue, B.; Smolander, J.; Westerlund, T.; Oksa, J.; Nieminen, R.; Moilanen, E.; Mikkelsson, M. Acute and long-term effects of winter swimming and whole-body cryotherapy on plasma antioxidative capacity in healthy women. Scand. J. Clin. Lab. Investig. 2005, 65, 395–402. [Google Scholar] [CrossRef]
- Tengan, C.H.; Rodrigues, G.S.; Godinho, R.O. Nitric oxide in skeletal muscle: Role on mitochondrial biogenesis and function. Int. J. Mol. Sci. 2012, 13, 17160–17184. [Google Scholar] [CrossRef] [PubMed]
- Tuteja, N.; Chandra, M.; Tuteja, R.; Misra, M.K. Nitric Oxide as a Unique Bioactive Signaling Messenger in Physiology and Pathophysiology. J. Biomed. Biotechnol. 2004, 2004, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.Y.; Hong, F.F.; Yang, S.L. The Roles of Nitric Oxide Synthase/Nitric Oxide Pathway in the Pathology of Vascular Dementia and Related Therapeutic Approaches. Int. J. Mol. Sci. 2021, 22, 4540. [Google Scholar] [CrossRef]
- Mittal, M.; Siddiqui, M.R.; Tran, K.; Reddy, S.P.; Malik, A.B. Reactive oxygen species in inflammation and tissue injury. Antioxid. Redox Signal 2014, 20, 1126–1167. [Google Scholar] [CrossRef]
- Adamczyk, B.; Adamczyk-Sowa, M. New Insights into the Role of Oxidative Stress Mechanisms in the Pathophysiology and Treatment of Multiple Sclerosis. Oxid. Med. Cell Longev. 2016, 2016, 1973834. [Google Scholar] [CrossRef]
- Abdel Naseer, M.; Rabah, A.M.; Rashed, L.A.; Hassan, A.; Fouad, A.M. Glutamate and Nitric Oxide as biomarkers for disease activity in patients with multiple sclerosis. Mult. Scler. Relat. Disord. 2020, 38, 101873. [Google Scholar] [CrossRef] [PubMed]
- Giovannoni, G.; Heales, S.J.R.; Land, J.M.; Thompson, E.J. The potential role of nitric oxide in multiple sclerosis. Mult. Scler. J. 1998, 4, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Acar, G.; Idiman, F.; Idiman, E.; Kirkali, G.; Cakmakçi, H.; Ozakbaş, S. Nitric oxide as an activity marker in multiple sclerosis. J. Neurol. 2003, 250, 588–592. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.J.; Lassmann, H. The role of nitric oxide in multiple sclerosis. Lancet Neurol. 2002, 1, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Broholm, H.; Andersen, B.; Wanscher, B.; Frederiksen, J.L.; Rubin, I.; Pakkenberg, B.; Larsson, H.B.; Lauritzen, M. Nitric oxide synthase expression and enzymatic activity in multiple sclerosis. Acta Neurol. Scand. 2004, 109, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Schwid, S.R.; Petrie, M.D.; Murray, R.; Leitch, J.; Bowen, J.; Alquist, A.; Pelligrino, R.; Roberts, A.; Harper-Bennie, J.; Milan, M.D.; et al. A randomized controlled study of the acute and chronic effects of cooling therapy for MS. Neurology 2003, 60, 1955–1960. [Google Scholar] [CrossRef] [PubMed]
- El Ridi, R.; Tallima, H. Physiological functions and pathogenic potential of uric acid: A review. J. Adv. Res. 2017, 8, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Hooper, D.C.; Spitsin, S.; Kean, R.B.; Champion, J.M.; Dickson, G.M.; Chaudhry, I.; Koprowski, H. Uric acid, a natural scavenger of peroxynitrite, in experimental allergic encephalomyelitis and multiple sclerosis. Proc. Natl. Acad. Sci. USA 1998, 95, 675–680. [Google Scholar] [CrossRef]
- Massa, J.; O’Reilly, E.; Munger, K.L.; Delorenze, G.N.; Ascherio, A. Serum uric acid and risk of multiple sclerosis. J. Neurol. 2009, 256, 1643–1648. [Google Scholar] [CrossRef]
- Atya, H.B.; Ali, S.A.; Hegazy, M.I.; El Sharkawi, F.Z. Urinary Urea, Uric Acid and Hippuric Acid as Potential Biomarkers in Multiple Sclerosis Patients. Indian J. Clin. Biochem. 2018, 33, 163–170. [Google Scholar] [CrossRef]
- Latronico, T.; Liuzzi, G. Metalloproteinases and their inhibitors as therapeutic targets for multiple sclerosis: Current evidence and future perspectives. Met. Med. 2017, 4, 1–13. [Google Scholar] [CrossRef]
- Yong, V.W.; Zabad, R.K.; Agrawal, S.; Goncalves Dasilva, A.; Metz, L.M. Elevation of matrix metalloproteinases (MMPs) in multiple sclerosis and impact of immunomodulators. J. Neurol. Sci. 2007, 259, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Sato, W.; Tomita, A.; Ichikawa, D.; Lin, Y.; Kishida, H.; Miyake, S.; Ogawa, M.; Okamoto, T.; Murata, M.; Kuroiwa, Y.; et al. CCR2+CCR5+ T cells produce matrix metalloproteinase-9 and osteopontin in the pathogenesis of multiple sclerosis. J. Immunol. 2012, 189, 5057–5065. [Google Scholar] [CrossRef]
- Fainardi, E.; Castellazzi, M.; Bellini, T.; Manfrinato, M.C.; Baldi, E.; Casetta, I.; Paolino, E.; Granieri, E.; Dallocchio, F. Cerebrospinal fluid and serum levels and intrathecal production of active matrix metalloproteinase-9 (MMP-9) as markers of disease activity in patients with multiple sclerosis. Mult. Scler. 2006, 12, 294–301. [Google Scholar] [CrossRef]
- Liuzzi, G.M.; Trojano, M.; Fanelli, M.; Avolio, C.; Fasano, A.; Livrea, P.; Riccio, P. Intrathecal synthesis of matrix metalloproteinase-9 in patients with multiple sclerosis: Implication for pathogenesis. Mult. Scler. 2002, 8, 222–228. [Google Scholar] [CrossRef]
- Trentini, A.; Castellazzi, M.; Cervellati, C.; Manfrinato, M.C.; Tamborino, C.; Hanau, S.; Volta, C.A.; Baldi, E.; Kostic, V.; Drulovic, J.; et al. Interplay between Matrix Metalloproteinase-9, Matrix Metalloproteinase-2, and Interleukins in Multiple Sclerosis Patients. Dis. Markers 2016, 2016, 3672353. [Google Scholar] [CrossRef]
- Ljubisavljevic, S.; Stojanovic, I.; Basic, J.; Vojinovic, S.; Stojanov, D.; Djordjevic, G.; Pavlovic, D. The Role of Matrix Metalloproteinase 3 and 9 in the Pathogenesis of Acute Neuroinflammation. Implications for Disease Modifying Therapy. J. Mol. Neurosci. 2015, 56, 840–847. [Google Scholar] [CrossRef] [PubMed]
- Bastian, T.W.; Rao, R.; Tran, P.V.; Georgieff, M.K. The Effects of Early-Life Iron Deficiency on Brain Energy Metabolism. Neurosci. Insights 2020, 15, 2633105520935104. [Google Scholar] [CrossRef]
- Zierfuss, B.; Wang, Z.; Jackson, A.N.; Moezzi, D.; Yong, V.W. Iron in multiple sclerosis—Neuropathology, immunology, and real-world considerations. Mult. Scler. Relat. Disord. 2023, 78, 104934. [Google Scholar] [CrossRef]
- Khalil, M.; Riedlbauer, B.; Langkammer, C.; Enzinger, C.; Ropele, S.; Stojakovic, T.; Scharnagl, H.; Culea, V.; Petzold, A.; Teunissen, C.; et al. Cerebrospinal fluid transferrin levels are reduced in patients with early multiple sclerosis. Mult. Scler. J. 2014, 20, 1569–1577. [Google Scholar] [CrossRef]
- Gouel, F.; Rolland, A.-S.; Devedjian, J.-C.; Burnouf, T.; Devos, D. Past and Future of Neurotrophic Growth Factors Therapies in ALS: From Single Neurotrophic Growth Factor to Stem Cells and Human Platelet Lysates. Front. Neurol. 2019, 10, 835. [Google Scholar] [CrossRef]
- Cobianchi, S.; Arbat-Plana, A.; Lopez-Alvarez, V.M.; Navarro, X. Neuroprotective Effects of Exercise Treatments After Injury: The Dual Role of Neurotrophic Factors. Curr. Neuropharmacol. 2017, 15, 495–518. [Google Scholar] [CrossRef]
- Bathina, S.; Das, U.N. Brain-derived neurotrophic factor and its clinical implications. Arch. Med. Sci. 2015, 11, 1164–1178. [Google Scholar] [CrossRef]
- Aloe, L.; Rocco, M.L.; Balzamino, B.O.; Micera, A. Nerve Growth Factor: A Focus on Neuroscience and Therapy. Curr. Neuropharmacol. 2015, 13, 294–303. [Google Scholar] [CrossRef]
- Ksiazek-Winiarek, D.J.; Szpakowski, P.; Glabinski, A. Neural Plasticity in Multiple Sclerosis: The Functional and Molecular Background. Neural Plast. 2015, 2015, 307175. [Google Scholar] [CrossRef]
- Janowska, J.; Gargas, J.; Ziemka-Nalecz, M.; Zalewska, T.; Sypecka, J. Oligodendrocyte Response to Pathophysiological Conditions Triggered by Episode of Perinatal Hypoxia-Ischemia: Role of IGF-1 Secretion by Glial Cells. Mol. Neurobiol. 2020, 57, 4250–4268. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.M.; Beales, J.T.; Montierth, M.D.; Briggs, F.B.; Frodsham, S.F.; Davis, M.F. The Impact of Multiple Sclerosis Disease Status and Subtype on Hematological Profile. Int. J. Environ. Res. Public. Health 2021, 18, 3318. [Google Scholar] [CrossRef]
- Alito, A.; Quartarone, A.; Leonardi, G.; Tisano, A.; Bruschetta, A.; Cucinotta, F.; Milardi, D.; Portaro, S. Brown adipose tissue human biomarkers: Which one fits best? A narrative review. Medicine 2022, 101, e32181. [Google Scholar] [CrossRef] [PubMed]
- Wyrostek, J.; Piotrowska, A.; Czerwińska-Ledwig, O.; Zuziak, R.; Szyguła, Z.; Cisoń, T.; Żychowska, M.; Pilch, W. Complex effects of whole body cryostimulation on hematological markers in patients with obesity. PLoS ONE 2021, 16, e0249812. [Google Scholar] [CrossRef]
- Youngchan, K.; Kyoohyun, K.; YongKeun, P. Measurement Techniques for Red Blood Cell Deformability: Recent Advances. In Blood Cell; Terry, E.M., Ed.; IntechOpen: Rijeka, Croatia, 2012; Chapter 10. [Google Scholar]
- Miranda Acuña, J.; Hidalgo de la Cruz, M.; Ros, A.L.; Tapia, S.P.; Martínez Ginés, M.L.; de Andrés Frutos, C.D. Elevated plasma fibrinogen levels in multiple sclerosis patients during relapse. Mult. Scler. Relat. Disord. 2017, 18, 157–160. [Google Scholar] [CrossRef]
- Langer, H.F.; Choi, E.Y.; Zhou, H.; Schleicher, R.; Chung, K.J.; Tang, Z.; Göbel, K.; Bdeir, K.; Chatzigeorgiou, A.; Wong, C.; et al. Platelets contribute to the pathogenesis of experimental autoimmune encephalomyelitis. Circ. Res. 2012, 110, 1202–1210. [Google Scholar] [CrossRef] [PubMed]
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and Treatment of Multiple Sclerosis: A Review. JAMA 2021, 325, 765–779. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, Z.; Homayuni, A.; Etemadifar, M. Barriers to quality of life in patients with multiple sclerosis: A qualitative study. BMC Neurol. 2022, 22, 174. [Google Scholar] [CrossRef] [PubMed]
- Chacko, G.; Patel, S.; Galor, A.; Kumar, N. Heat Exposure and Multiple Sclerosis-A Regional and Temporal Analysis. Int. J. Environ. Res. Public. Health 2021, 18, 5962. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.L.; Wilson, T.E.; White, A.T.; Frohman, E.M. Thermoregulation in multiple sclerosis. J. Appl. Physiol. 2010, 109, 1531–1537. [Google Scholar] [CrossRef] [PubMed]
- Bilgin, A.; Kesik, G.; Ozdemir, L. The Effects of Cooling Therapies on Fatigue, Physical Activity, and Quality of Life in Multiple Sclerosis: A Meta-Analysis. Rehabil. Nurs. 2022, 47, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, L.F.; Short, C.A.; Westwood, D.A.; Cheung, S.S. Head pre-cooling improves symptoms of heat-sensitive multiple sclerosis patients. Can. J. Neurol. Sci. 2011, 38, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Stevens, C.J.; Singh, G.; Peterson, B.; Vargas, N.T.; Périard, J.D. The effect of cooling garments to improve physical function in people with multiple sclerosis: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2023, 78, 104912. [Google Scholar] [CrossRef] [PubMed]
- Rymaszewska, J.; Ramsey, D.; Chładzińska-Kiejna, S. Whole-body cryotherapy as adjunct treatment of depressive and anxiety disorders. Arch. Immunol. Ther. Exp. 2008, 56, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Garcia, C.; Karri, J.; Zacharias, N.A.; Abd-Elsayed, A. Use of Cryotherapy for Managing Chronic Pain: An Evidence-Based Narrative. Pain Ther. 2021, 10, 81–100. [Google Scholar] [CrossRef]


{kind=link}
| Criteria | Application |
|---|---|
| Population | Patients with MS |
| Intervention | WBC |
| Comparisons | Comparing before and post intervention |
| Outcomes | Technique-related improvements |
| Study design | Clinical trial, prospective trial, observational study |
| Database | Query Terms |
|---|---|
| PubMed | (“whole-body cryostimulation” OR “whole-body cryotherapy”) AND multiple sclerosis |
| ScienceDirect | (“whole-body cryostimulation” OR “whole-body cryotherapy”) AND “multiple sclerosis” |
| Web of Science | ((ALL = (“whole-body cryostimulation”)) OR ALL = (“whole-body cryotherapy”)) AND ALL = (“multiple sclerosis”) |
| Embase | (“multiple sclerosis”/exp OR “multiple sclerosis” OR “ms”) AND (“whole body cryotherapy”/exp OR “whole body cryotherapy” OR “whole body cryostimulation”/exp OR “whole body cryostimulation”) |
| Author, Year | Study Design | Patients’ Features | WBC Application Modality | Outcome Measures | Results | Adverse Effects |
|---|---|---|---|---|---|---|
| Ptaszek et al., 2023 (a) [52] | Prospective controlled trial EG: MS vs. CG: healthy subjects | 30 (EG: 15 vs. CG: 15) Age: EG: 41.53 vs. CG: 38,47 Sex: EG: 15F vs. CG: 15F EG: EDSS: 3.03 | Wroclaw-type liquid nitrogen-cooled cryochamber, 20 daily WBC sessions 5/week (3 min, at −120 °C) After each treatment, there was a 15 min warm-up on a cycle ergometer. | CAT, GPx, and SOD. Before the start of treatment (T0) and the end of the series (T1). | No changes in the examined parameters (CAT, GPx, and SOD) in the MS or control groups. | Not reported |
| Ptaszek et al., 2023 (b) [53] | Prospective controlled trial EG: WBC—MS vs. CG1: No WBC—MS vs. CG2: Healthy—WBC | 50 F (EG: 15 vs. CG1: 20 vs. CG2: 15) Age: EG: 41.53 vs. CG1: 40.45 vs. CG2: 38.47 EDSS: EG:3.03 vs. CG1:3.08 | Wroclaw-type liquid nitrogen-cooled cryochamber, 20 daily WBC sessions 5/week (3 min, at −120 °C) After each treatment, there was a 15 min warm-up on a cycle ergometer. | TAS/TAC, TOS/TOC, NO, UA, and MMP-9. Before the start of treatment (T0) and at the end of the series (T1). There was a one-time (at baseline) examination of women without WBC intervention. | An insignificant increase in total antioxidant capacity and an insignificant decrease in total oxidative status/total oxidative capacity were observed in the EG. In women with MS, there was no significant effect of cryotherapy on changes in the oxidant/antioxidant imbalance or the concentrations of NO or MMP9. | Not reported |
| Ptaszek et al., 2022 [54] | Prospective study (MS vs. HC) | 30 MS: 15 vs. HC: 15 Age: MS: 41.53 vs. HC: 38.47 Sex: MS: 15 vs. HC: 15 EDDS: 3.03 | Liquid nitrogen-cooled cryochamber, 20 daily WBC sessions 5/week (first treatment, 1.5 min; second treatment, 2 min; and 3–20 treatments, 3 min) at −120 °C. After each treatment, there was a 15 min warm-up on a cycle ergometer. | Iron, transferrin, ferritin serum concentrations, IgG, IgA, IgM, CRP, BDNF, NGF, PDGF, VEGF, and IGF-1. Blood samples were collected before the start of the WBC procedures and after a series of 20 WBC sessions. | A statistically significant decrease in transferrin levels was observed in MS patients (within normal limits—this change could be related to the exercises patients did after WBC or to inflammation). When the other indicators were analysed, favourable directions and trends of changes were observed. However, the changes were not statistically significant. | Not reported |
| Radecka et al., 2021 [55] | RCT single-blind (EG: WBC vs. CG: no WBC) | 114 (EG: 60 vs. CG: 54) Sex: EG: 44 F vs. CG: 39 F Age: EG: 44.95 vs. CG: 45.09 EDSS: EG: 1.76 vs. CG: 1.79 | 20 daily WBC sessions 5/week (2–3 min, at −110 °C). There was a 15 min group kinesiotherapy session after each treatment. | FSS, T25-FW, HGS, and sEMG of the ECR and FCR muscles of the wrist, for the dominant hand. Before the start of treatment (T0), between the second and fourth day, and at the end of the series (T1). | In EG, there was an increase in ECR and a decrease in FCR amplitude, with significant differences in resting sEMG signals between ECR and FC, an increase in HGS, gait improvement, and a decrease in fatigue. No significant changes were observed in CG. | Not reported |
| Ptaszek et al., 2021 [56] | Prospective controlled trial 3 arms EG: WBC—MS CG1: NO WBC—MS CG2: Healthy—WBC | 50 F (EG: 15 vs. CG1: 20 vs. CG2: 15) Age: EG: 41.53 vs. CG1: 40.45 vs. CG2: 38.47 EDSS: EG:3.03 vs. CG1:3.08 | Wroclaw-type liquid nitrogen-cooled cryochamber, 20 daily WBC sessions 5/week (first treatment, 1.5 min; second treatment, 2 min; and 3–20 treatments, 3 min) at −120 °C. After each treatment, there was a 15 min warm-up on a cycle ergometer. | White blood cells, RBC, Hb, HCT, PLT, MCH, MCV, MCHC, RBC, Elongation and Aggregation Indexes, protein serum level, and fibrinogen concentration. Before the start of treatment (T0) and at the end of the series (T1). | There was no significant effect on changes in blood counts, rheology, and biochemistry. WBC significantly increased the deformation capacity of erythrocytes and reduced the hematocrit value (within physiological norms) of healthy women, which had a positive effect on the rheological properties of blood. | Not reported |
| Lubkowska et al., 2020 [57] | Clinical trial WBC—MS | 25 WBC—MS Age: 44.58 Sex: 19 F EDDS: ≤6 | 20 daily WBC sessions 5/week (2–3 min, at −110 °C). After each treatment, there was a 30 min session of individual physical rehabilitation. | HGT, T25-FW, and TS. Before the start of treatment (T0) and at the end of the series (T1). | A marginal but statistically significant increase in thumb strength was observed in the right hand. Other changes in HGT, TS, and T25-FW were not statistically significant. | Not reported |
| Pawik et al., 2019 [58] | Clinical trial WBC + GYM vs. WBC vs. GYM | 60 (WBC + GYM: 20 vs. WBC: 20 vs. GYM: 20) Sex: WBC + GYM: 17 F, 3 M vs. WBC: 11 F, 8 M vs. GYM: 15 F, 5 M Age: WBC + GYM: 48.8 vs. WBC: 45.8 vs. GYM: 53.3 EDDS: WBC + GYM: 2.4 vs. WBC: 2.3 vs. GYM: 2.35 | 10 daily WBC sessions, 5/week (at −110°/−160 °C). | PGWBI, HADS, and RMI. Assessments were made before treatment, 14 days after the start of treatment, and 2 days after the end of the last session. | A statistically significant difference in PGWBI was found in the GYM and WBC + GYM groups. A statistically significant reduction in the severity of anxiety symptoms (HADS-A) was seen in the WBC + GYM group. A significant reduction in depressive symptoms (HADS-D) was seen in the WBC + GYM and WBC groups. A statistically significant improvement in functional status (RMI) was seen in the WBC group. | Not reported |
| Bryczkowska et al., 2018 [59] | Observational study | 30 F Age 45.6 EDDS: >6 | Wroclaw-type liquid nitrogen exchanger cryochamber, 30 daily WBC sessions (3 min, at −130 °C). There was a 30 min group kinesiotherapy session after each treatment. | SOD, CAT, GPx, R-GSSG, GST, total protein, albumin, glucose, and uric acid levels; and Tch, HDL, LDL, and TAG concentrations. | No significant changes in total protein, albumin, uric acid, glucose concentrations, total cholesterol, HDL and LDL cholesterol levels, and triacylglycerol concentrations were observed, and a significant increase in SOD1 activity was associated with a trend towards increased GST activity. | Not reported |
| Miller et al., 2016 [41] | Case-control study 2 groups LF (FSS 38–42) vs. HF (FSS 48–52) | 48 (LF: 24 vs. HF: 24) Sex: (LF: 14 F vs. HF: 14 F) Age LF: 55.6 vs. HF: 55.7 EDDS LF: 5.2 vs. HF: 5.1 | KR2005N-type liquid nitrogen-cooled cryochamber, 10 daily WBC sessions, 5/week, (2–3 min, at −110°–−160 °C). | RMA (RMA 1 gross function, RMA 2 leg and trunk, RMA 3 arm), MSIS-29 (MSIS-29 PHYS, MSIS-29-PSYCH), and EDSS. Before the start of treatment (T0) and at the end of the series (T1). | In both groups, there was a significant improvement in functional status and fatigue, with the changes observed in HF patients being significantly greater, especially in the MSIS-29-PHYS, MSIS-29-PSYCH, RMA1, and RMA3. WBC appears to be effective in improving functional status and fatigue in people with MS, especially in those who are most fatigued. | Not reported |
| Miller et al., 2013 [60] | Clinical trial EG: SPMS vs. CG: healthy | 44 (EG: 22 vs. CG: 22) Sex: EG: 12 F vs. CG: 12 F Age: EG: 48.6 vs. CG: 45.8 EG: EDSS: 4.5 | Liquid nitrogen-cooled cryochamber, 10 daily WBC sessions, 5/week, (3 min, at −130 °C). | UA plasma concentration, EDSS. Four-stage examination: before the WBC (0), directly after 10 days of WBCT (I), and 1 month (II) and 3 months (III) after completion of the series. | WBC increased plasma UA levels in SPMS patients not only immediately, but also one and three months later. In addition, WBC induced positive changes in the EDSS scale both immediately and after 1 and 3 months. | Not reported |
| Miller et al., 2011 [48] | Clinical trial MS-D WBC vs. MS non depression WBC | 22 (15 F) Age: 42.2 (MS-D: 12 vs. MS—non-D: 10) EDSS: 4.5 | 10 daily WBC sessions in a liquid nitrogen-cooled cryochamber, from Monday to Friday (2–3 min at −110°/−160 °C). | TAS, SOD, and CAT. 1h before the start of treatment (T0) and 1h after the end (T1). | WBC increased the level of TAS in depressive MS patients more than in non-depressive MS patients. WBC treatment resulted in a significant increase in plasma TAS levels but had no effect on the activities of SOD and CAT. | Not reported |
| Miller et al., 2010 (b) [61] | Clinical trial MS—WBC vs. HC | 32 MS—WBC: 16 vs. HC: 16 Age: MS—WBC: 43.2 Sex: MS—WBC: 11F MS—WBC: EDSS: 4.5 | MS—WBC: 3 cycles of 10 daily WBC sessions in a liquid nitrogen-cooled cryochamber, from Monday to Friday (2–3 min at −110°/−160 °C). HC: 1 cycle of 10 daily WBC sessions in a liquid nitrogen-cooled cryochamber, from Monday to Friday (2–3 min at −110°/−160 °C). | TAS, SOD, and CAT. MS-WBC: patients were examined at two stages at the beginning of the third cycle of WBC treatment. HC: patients were examined at two stages at the beginning of the end of WBC treatment. | WBC increased TAS but had no effect on the activity of antioxidant enzymes: SOD and CAT. | Not reported |
| Miller et al., 2010 (a) [62] | Clinical trial MS—WBC vs. MS—no WBC vs. HC | 52 MS—WBC: 16 vs. MS—no WBC: 16 vs. HC: 20 Age: not specified Sex: not specified EDDS: not specified | 10 daily WBC sessions in a liquid nitrogen-cooled cryochamber, from Monday to Friday (2–3 min at −110°/−160 °C). | TAS, SOD, and CAT. 1h before the start of treatment (T0) and 1h after the end (T1) MS patients were assessed at the beginning and end of treatment. HC had one examination. | The level of TAS in MS patients was significantly reduced compared to HC. A significant increase in TAS was observed in the WBC group compared to the CG. | Not reported |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alito, A.; Fontana, J.M.; Franzini Tibaldeo, E.; Verme, F.; Piterà, P.; Miller, E.; Cremascoli, R.; Brioschi, A.; Capodaglio, P. Whole-Body Cryostimulation in Multiple Sclerosis: A Scoping Review. J. Clin. Med. 2024, 13, 2003. https://doi.org/10.3390/jcm13072003
Alito A, Fontana JM, Franzini Tibaldeo E, Verme F, Piterà P, Miller E, Cremascoli R, Brioschi A, Capodaglio P. Whole-Body Cryostimulation in Multiple Sclerosis: A Scoping Review. Journal of Clinical Medicine. 2024; 13(7):2003. https://doi.org/10.3390/jcm13072003
Chicago/Turabian StyleAlito, Angelo, Jacopo Maria Fontana, Eleonora Franzini Tibaldeo, Federica Verme, Paolo Piterà, Elzbieta Miller, Riccardo Cremascoli, Andrea Brioschi, and Paolo Capodaglio. 2024. "Whole-Body Cryostimulation in Multiple Sclerosis: A Scoping Review" Journal of Clinical Medicine 13, no. 7: 2003. https://doi.org/10.3390/jcm13072003