
The Efficacy of Elonide Nasal Corticosteroids in Managing Allergic Rhinitis: A Randomized, Double-Blinded Trial
 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
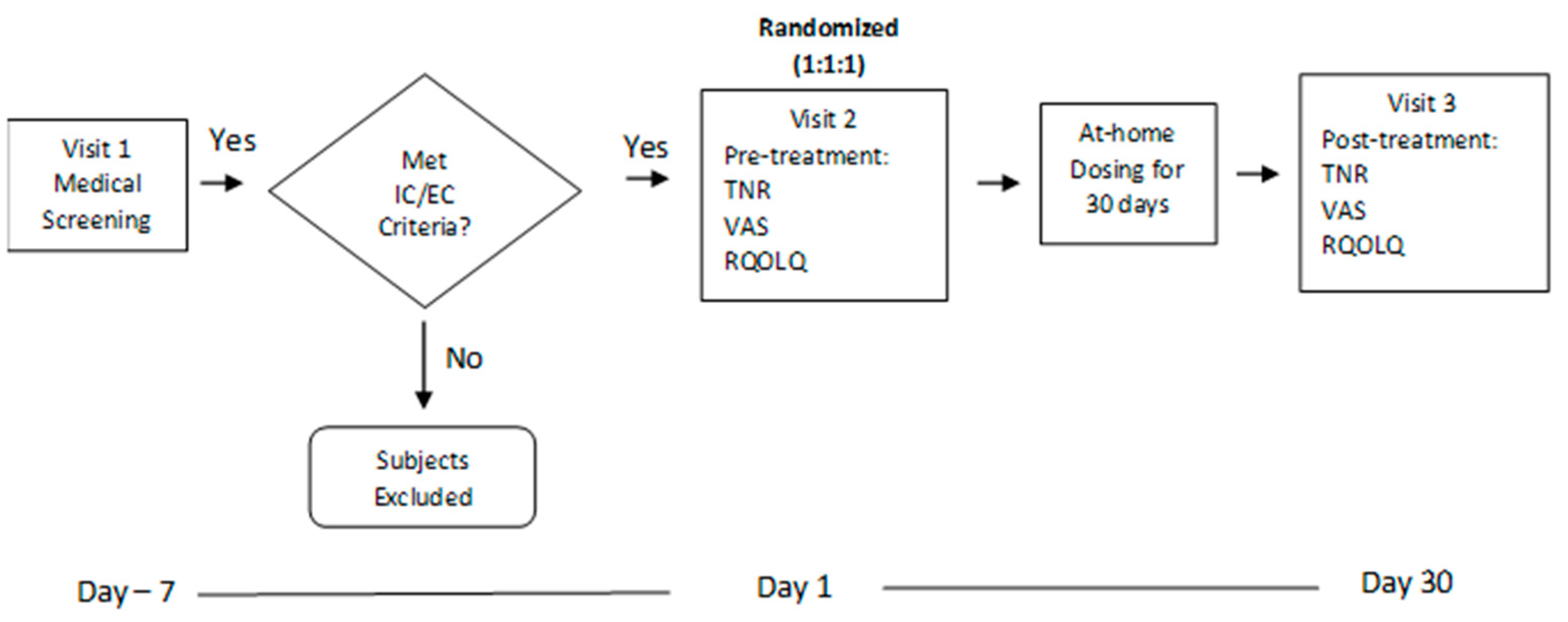
2.1. Study Design
2.2. Participants
2.3. Intervention
2.4. Outcome Measures
2.5. Sample Size
2.6. Statistical Analysis
3. Results
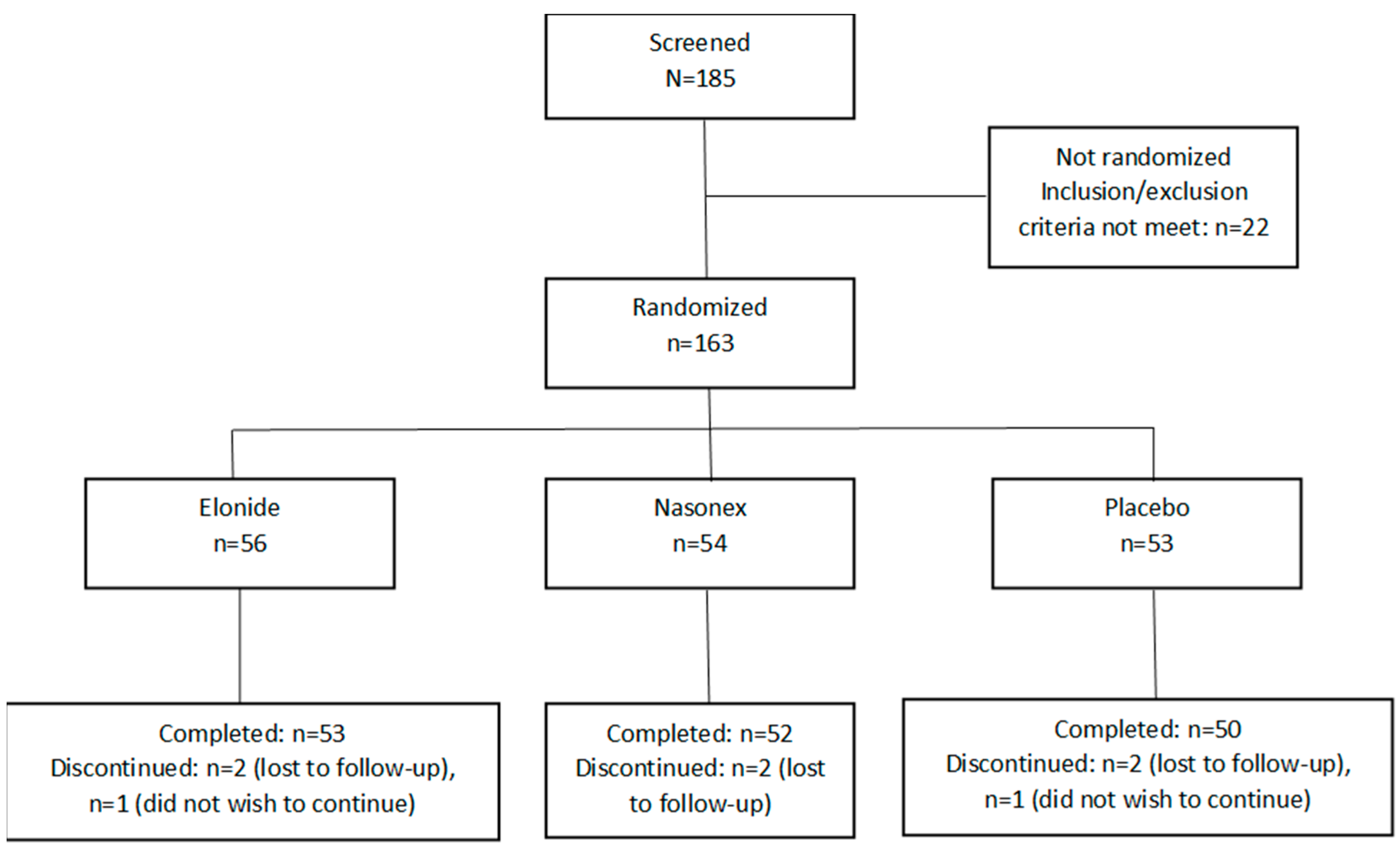
3.1. Participants
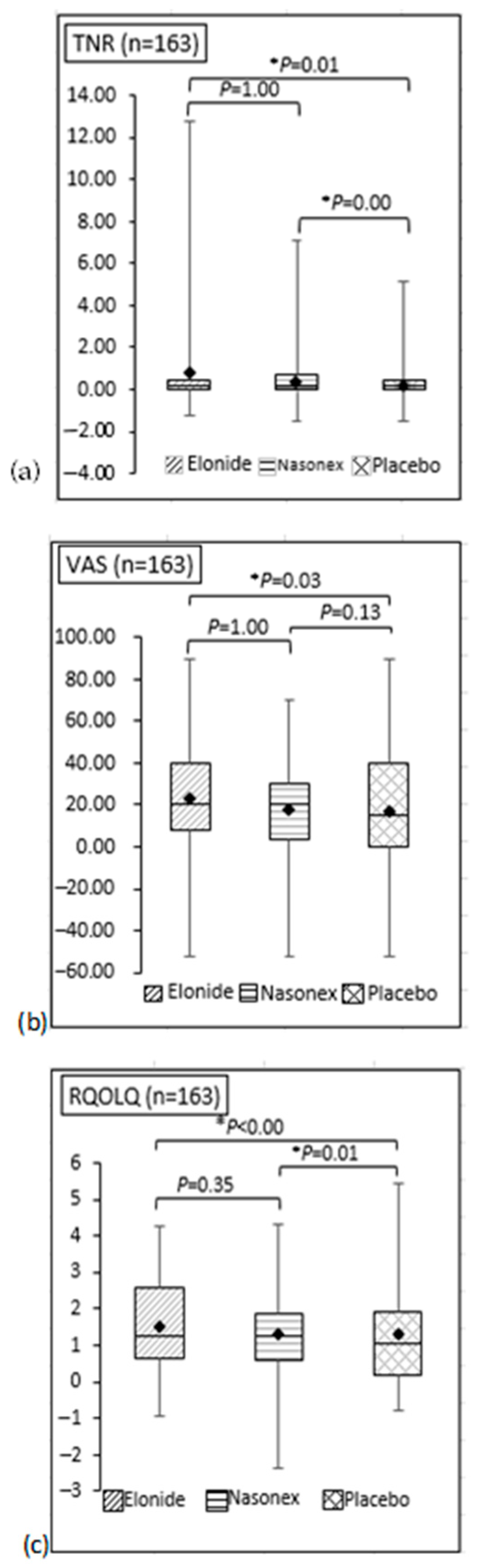
3.2. Efficacy Outcomes
3.3. Safety Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bousquet, J.; Van Cauwenberge, P.; Khaltaev, N.; Aria Workshop Group; World Health Organization. Allergic rhinitis and its impact on asthma. J. Allergy Clin. Immunol. 2001, 108, 147–334. [Google Scholar] [CrossRef]
- Bauchau, V.; Durham, S.R. Prevalence and rate of diagnosis of allergic rhinitis in Europe. Eur. Respir. J. 2004, 24, 758–764. [Google Scholar] [CrossRef]
- Wise, S.K.; Lin, S.Y.; Toskala, E.; Orlandi, R.R.; Akdis, C.A.; Alt, J.A.; Azar, A.; Baroody, F.M.; Bachert, C.; Canonica, G.W.; et al. International Consensus Statement on Allergy and Rhinology: Allergic Rhinitis. Int. Forum Allergy Rhinol. 2018, 8, 108–352. [Google Scholar] [CrossRef]
- Gendeh, B.S.; Murad, S.; Razi, A.M.; Abdullah, N.; Mohamed, A.S.; Kadir, K.A. Skin prick test reactivity to foods in adult Malaysians with rhinitis. Otolaryngol. Head Neck Surg. 2000, 122, 758–762. [Google Scholar] [CrossRef]
- Aneeza, W.H.; Husain, S.; Rahman, R.A.; Van Dort, D.; Abdullah, A.; Gendeh, B.S. Efficacy of Mometasone Furoate and Fluticasone Furoate on Persistent Allergic Rhinoconjunctivitis. Allergy Rhinol. 2013, 4, e120–e126. [Google Scholar] [CrossRef]
- Corren, J. Intranasal corticosteroids for allergic rhinitis: How do different agents compare? J. Allergy Clin. Immunol. 1999, 104, 144–149. [Google Scholar] [CrossRef]
- Gotoh, M.; Sugita, K.; Saito, A.; Honda, T.; Hoashi, K.; Miyazaki, T. A Study of the Therapeutic Equivalence of Generic vs. Mometasone Nasal Spray in Patients with Seasonal Allergic Rhinitis. Nihon Bika Gakkai Kaishi (Jpn. J. Rhinol.) 2018, 57, 7–16. [Google Scholar] [CrossRef]
- Vaidyanathan, S.; Barnes, M.; Lipworth, B.J. Comparative safety and efficacy of 2 formulations of fluticasone aqueous nasal spray in persistent allergic rhinitis. Ann. Allergy Asthma Immunol. 2009, 102, 76–83. [Google Scholar] [CrossRef]
- Kuribayashi, R.; Kasuga, M.; Kuwana, K.; Yamaguchi, T. First Approval of Generic Mometasone Furoate Nasal Suspension Spray in Japan: Similarities and Differences Between Japan and the USA. Ther. Innov. Regul. Sci. 2022, 57, 173–177. [Google Scholar] [CrossRef]
- Klimek, L.; Bachert, C.; Pfaar, O.; Becker, S.; Bieber, T.; Brehler, R.; Buhl, R.; Casper, I.; Chaker, A.; Czech, W.; et al. ARIA guideline 2019: Treatment of allergic rhinitis in the German health system. Allergologie 2019, 3, 22–50. [Google Scholar] [CrossRef]
- Heyworth-Smith, D.; Campbell, P. Laboratory Diagnosis of Allergy; QML Pathology Newsletter: Brisbane, Australia, 2017. [Google Scholar]
- Gupta, S.K. Intention-to-treat concept: A review. Perspect. Clin. Res. 2011, 2, 109–112. [Google Scholar] [CrossRef]
- Buhl, R.; Tanase, A.-M.; Hosoe, M.; Cao, W.; Demin, I.; Bartels, C.; Jauernig, J.; Ziegler, D.; Patalano, F.; Hederer, B.; et al. A randomized, double-blind study to compare the efficacy and safety of two doses of mometasone furoate delivered via Breezhaler® or Twisthaler® in patients with asthma. Pulm. Pharmacol. Ther. 2020, 62, 101919. [Google Scholar] [CrossRef]
- Small, C.B.; Hernandez, J.; Reyes, A.; Schenkel, E.; Damiano, A.; Stryszak, P.; Staudinger, H.; Danzig, M. Efficacy and safety of mometasone furoate nasal spray in nasal polyposis. J. Allergy Clin. Immunol. 2005, 116, 1275–1281. [Google Scholar] [CrossRef]
- Lange, B.; Lukat, K.-F.; Rettig, K.; Holtappels, G.; Bachert, C. Efficacy, cost-effectiveness, and tolerability of mometasone furoate, levocabastine, and disodium cromoglycate nasal sprays in the treatment of seasonal allergic rhinitis. Ann. Allergy Asthma Immunol. 2005, 95, 272–282. [Google Scholar] [CrossRef]
- Mak, K.-K.; Ku, M.-S.; Lu, K.-H.; Sun, H.-L.; Lue, K.-H. Comparison of Mometasone Furoate Monohydrate (Nasonex) and Fluticasone Propionate (Flixonase) Nasal Sprays in the Treatment of Dust Mite-sensitive Children with Perennial Allergic Rhinitis. Pediatr. Neonatol. 2013, 54, 239–245. [Google Scholar] [CrossRef]
- Abdul Latiff, A.H.; Husain, S.; Abdullah, B.; Suppiah, P.; Tan, V.; Ing Ping, T.; Woo, K.; Yap, Y.-Y.; Bachert, C.; Schunemann, J.H.; et al. ARIA Care Pathways 2019: Next-Generation Allergic Rhinitis Care and Allergen Immunotherapy in Malaysia. J. Pers. Med. 2023, 13, 835. [Google Scholar] [CrossRef]
- Tarmizi, N.E.; Hamizan, A.W.; Ng, C.S.; Gendeh, H.S.; Guan, L.S.; Zahedi, F.D.; Baki, M.M.; Husain, S. The Nasal Endoscopic Features of Postnasal Drip: A Cross Sectional Study. Int. Arch. Otorhinolaryngol. 2023, 28, e95–e100. [Google Scholar] [CrossRef]
- Hamizan, A.W.; Rimmer, J.; Alvarado, R.; Sewell, W.A.; Tatersall, J.; Barham, H.P.; Kalish, L.; Harvey, R.J. Turbinate-Specific IgE in Normal and Rhinitic Patients. Am. J. Rhinol. Allergy 2019, 33, 178–183. [Google Scholar] [CrossRef]
- Brożek, J.L.; Bousquet, J.; Agache, I.; Agarwal, A.; Bachert, C.; Bosnic-Anticevich, S.; Brignardello-Petersen, R.; Canonica, G.W.; Casale, T.; Chavannes, N.H.; et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines—2016 revision. J. Allergy Clin. Immunol. 2017, 140, 950–958. [Google Scholar] [CrossRef]
- Dykewicz, M.S.; Wallace, D.V.; Baroody, F.; Bernstein, J.; Craig, T.; Finegold, I.; Huang, F.; Larenas-Linnemann, D.; Meltzer, E.; Steven, G.; et al. Treatment of seasonal allergic rhinitis: An evidence-based focused 2017 guideline update. Ann. Allergy Asthma Immunol. 2017, 119, 489–511. [Google Scholar] [CrossRef]
- Krouse, J.H.; Roland, P.S.; Marple, B.F.; Wall, G.M.; Hannley, M.; Golla, S.; Hunsaker, D. Optimal Duration of Allergic Rhinitis Clinical Trials. Otolaryngol. Neck Surg. 2005, 133, 467–487, discussion 488. [Google Scholar] [CrossRef] [PubMed]
- Scadding, G.K.; Durham, S.R.; Mirakian, R.; Jones, N.S.; Leech, S.C.; Farooque, S.; Ryan, D.; Walker, S.M.; Clark, A.T.; Dixon, T.A.; et al. British Society for Allergy and Clinical Immunology. BSACI guidelines for the management of allergic and non-allergic rhinitis. Clin. Exp. Allergy 2008, 38, 19–42. [Google Scholar] [CrossRef]
- Klimek, L.; Bergmann, K.C.; Biedermann, T.; Bousquet, J.; Hellings, P.; Jung, K.; Merk, H.; Olze, H.; Schlenter, W.; Stock, P.; et al. Visual analogue scales (VAS): Measuring instruments for the documentation of symptoms and therapy monitoring in cases of allergic rhinitis in everyday health care: Position Paper of the German Society of Allergology (AeDA) and the German Society of Allergy and Clinical Immunology (DGAKI), ENT Section, in collaboration with the working group on Clinical Immunology, Allergology and Environmental Medicine of the German Society of Otorhinolaryngology, Head and Neck Surgery (DGHNOKHC). Allergo J. Int. 2017, 26, 16–24. [Google Scholar]
- Larenas-Linnemann, D.; Dinger, H.; Shah-Hosseini, K.; Michels, A.; Mösges, R.; Mexican Study Group on Allergic Rhinitis and SPT Sensitivity. Over Diagnosis of Persistent Allergic Rhinitis in Perennial Allergic Rhinitis Patients: A Nationwide Study in Mexico. Am. J. Rhinol. Allergy 2013, 27, 495–501. [Google Scholar] [CrossRef]
- Demoly, P.; Bousquet, P.J.; Mesbah, K.; Bousquet, J.; Devillier, P. Visual analogue scale in patients treated for allergic rhinitis: An observational prospective study in primary care. Clin. Exp. Allergy 2013, 43, 881–888. [Google Scholar] [CrossRef]
- Bousquet, J.; Bachert, C.; Canonica, G.W.; Mullol, J.; Van Cauwenberge, P.; Jensen, C.B.; Fokkens, W.J.; Ring, J.; Keith, P.; Lorber, R.; et al. Efficacy of desloratadine in intermittent allergic rhinitis: A GA2LEN study. Allergy 2009, 64, 1516–1523. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Bachert, C.; Canonica, G.W.; Mullol, J.; Van Cauwenberge, P.; Jensen, C.B.; Fokkens, W.J.; Ring, J.; Keith, P.; Gopalan, G.; et al. Efficacy of desloratadine in persistent allergic rhinitis—A GA2LEN study. Int. Arch. Allergy Immunol. 2010, 153, 395–402. [Google Scholar] [CrossRef]
- Juniper, E.F.; Guyatt, G.H.; Griffith, L.E.; Ferrie, P.J. Interpretation of rhinoconjunctivitis quality of life questionnaire data. J. Allergy Clin. Immunol. 1996, 98, 843–845. [Google Scholar] [CrossRef]
- Juniper, E.F.; Guyatt, G.H. Development and testing of a new measure of health status for clinical trials in rhinoconjunctivitis. Clin. Exp. Allergy 1991, 21, 77–83. [Google Scholar] [CrossRef]
- Juniper, E.F.; Thompson, A.K.; Ferrie, P.J.; Roberts, J.N. Validation of the standardized version of the Rhinoconjunctivitis Quality of Life Questionnaire. J Allergy Clin Immunol. 1999, 104, 364–369. [Google Scholar] [CrossRef]
- Yamada, T.; Yamamoto, H.; Kubo, S.; Sakashita, M.; Tokunaga, T.; Susuki, D.; Narita, N.; Ogi, K.; Kanno, M.; Yamashita, S.; et al. Efficacy of mometasone furoate nasal spray for nasal symptoms, quality of life, rhinitis-disturbed sleep, and nasal nitric oxide in patients with perennial allergic rhinitis. Allergy Asthma Proc. 2012, 33, e9–e16. [Google Scholar] [CrossRef]
- Marple, B.F.; Fornadley, J.A.; Patel, A.A.; Fineman, S.M.; Fromer, L.; Krouse, J.H.; Lanier, B.Q.; Penna, P.; American Academy of Otolaryngic Allergy Working Group on Allergic Rhinitis. Keys to successful management of patients with allergic rhinitis: Focus on patient confidence, compliance, and satisfaction. Otolaryngol. Neck Surg. 2007, 136, S107–S124. [Google Scholar] [CrossRef]
- Juliá, J.C.; Burchés, M.E.; Martorell, A. Active anterior rhinomanometry in paediatrics. Normality criteria. Allergol. Et Immunopathol. 2011, 39, 342–346. [Google Scholar] [CrossRef]
- Carney, A.; Bateman, N.; Jones, N. Reliable and reproducible anterior active rhinomanometry for the assessment of unilateral nasal resistance. Clin. Otolaryngol. 2000, 25, 499–503. [Google Scholar] [CrossRef]
- Takeuchi, H.; Jawad, M.; Eccles, R. Changes in unilateral nasal airflow in patients with seasonal allergic rhinitis measured in and out of season. Auris Nasus Larynx 2000, 27, 141–145. [Google Scholar] [CrossRef]
- Kobayashi, R.; Miyazaki, S.; Karaki, M.; Kobayashi, E.; Karaki, R.; Akiyama, K.; Matsubara, A.; Mori, N. Measurement of nasal resistance by rhinomanometry in 892 Japanese elementary school children. Auris Nasus Larynx 2011, 38, 73–76. [Google Scholar] [CrossRef]
- Sharpe, S.A.; Sandweiss, V.; Tuazon, J.; Giordano, M.; Witchey-Lakshmanan, L.; Hart, J.; Sequeira, J. Comparison of the Flow Properties of Aqueous Suspension Corticosteroid Nasal Sprays Under Differing Sampling Conditions. Drug Dev. Ind. Pharm. 2003, 29, 1005–1012. [Google Scholar] [CrossRef]
- Elonide (Mometasone Furoate) Nasal Spray, 50 mcg Full Prescribing Info. Available online: https://www.mims.com/malaysia/drug/info/elonide?type=full (accessed on 3 January 2024).
- Mandl, M.; Nolop, K.; Lutsky, B. Comparison of Once Daily Mometasone Furoate (Nasonex) and Fluticasone Propionate Aqueous Nasal Sprays for the Treatment of Perennial Rhinitis. Ann. Allergy Asthma Immunol. 1997, 79, 370–378. [Google Scholar] [CrossRef]
- Rollema, C.; van Roon, E.N.; van Boven, J.F.M.; Hagedoorn, P.; Klemmeier, T.; Kocks, J.H.; Metting, E.I.; Elberink, H.N.G.O.; Peters, T.T.A.; Giorgi, M.R.M.S.; et al. Pharmacology, particle deposition and drug administration techniques of intranasal corticosteroids for treating allergic rhinitis. Clin. Exp. Allergy 2022, 52, 1247–1263. [Google Scholar] [CrossRef]
- Penagos, M.; Compalati, E.; Tarantini, F.; Baena-Cagnani, C.E.; Passalacqua, G.; Canonica, G.W. Efficacy of mometasone furoate nasal spray in the treatment of allergic rhinitis. Meta-analysis of randomized, double-blind, placebo-controlled, clinical trials. Allergy 2008, 63, 1280–1291. [Google Scholar] [CrossRef]
- Meltzer, E.O.; Bachert, C.; Staudinger, H. Treating acute rhinosinusitis: Comparing efficacy and safety of mometasone furoate nasal spray, amoxicillin, and placebo. J. Allergy Clin. Immunol. 2005, 116, 1289–1295. [Google Scholar] [CrossRef] [PubMed]
- Gawchik, S.; Goldstein, S.; Prenner, B.; John, A. Relief of cough and nasal symptoms associated with allergic rhinitis by mometasone furoate nasal spray. Ann. Allergy Asthma Immunol. 2003, 90, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Berkowitz, R.B.; Bernstein, D.I.; LaForce, C.; Pedinoff, A.J.; Rooklin, A.R.; Damaraju, C.R.; Mesarina-Wicki, B.; Nolop, K.B. Onset of action of mometasone furoate nasal spray (NASONEX) in seasonal allergic rhinitis. Allergy 1999, 54, 64–69. [Google Scholar] [CrossRef]
- Bronsky, E.A.; Aaronson, D.W.; Berkowitz, R.B.; Chervinsky, P.; Graft, D.; Kaiser, H.B.; Moss, B.; Nathan, R.A.; Pearlman, D.S.; Ratner, P.H.; et al. Dose ranging study of mometasone furoate (Nasonex) in seasonal allergic rhinitis. Ann. Allergy Asthma Immunol. 1997, 79, 51–56. [Google Scholar] [CrossRef]
- Carvalho, V.; Olej, B.; de Moraes, J.R.; Boechat, J.L. Mometasone furoate is not superior to saline for chronic rhinitis in the elderly. World Allergy Organ. J. 2019, 12, 100064. [Google Scholar] [CrossRef]
- Madison, S.; Brown, E.A.; Franklin, R.; A Wickersham, E.; McCarthy, L.H. Clinical Question: Nasal saline or intranasal corticosteroids to treat allergic rhinitis in children. J. Okla State Med. Assoc. 2016, 109, 152–153. [Google Scholar]
- Wang, Y.; Jin, L.; Liu, S.-X.; Fan, K.; Qin, M.-L.; Yu, S.-Q. Role of nasal saline irrigation in the treatment of allergic rhinitis in children and adults: A systematic analysis. Allergol. et Immunopathol. 2020, 48, 360–367. [Google Scholar] [CrossRef]
- Head, K.; Snidvongs, K.; Glew, S.; Scadding, G.; Schilder, A.G.; Philpott, C.; Hopkins, C. Saline irrigation for allergic rhinitis. Cochrane Database Syst. Rev. 2018, 6, CD012597. [Google Scholar] [CrossRef]
- Zhu, X. Comparison of Four Methods for Handing Missing Data in Longitudinal Data Analysis through a Simulation Study. Open J. Stat. 2014, 1, 933–944. [Google Scholar] [CrossRef]
- Rezvan, P.H.; Lee, K.J.; A Simpson, J. The rise of multiple imputation: A review of the reporting and implementation of the method in medical research. BMC Med. Res. Methodol. 2015, 15, 30. [Google Scholar] [CrossRef]
- Austin, P.C.; White, I.R.; Lee, D.S.; van Buuren, S. Missing Data in Clinical Research: A Tutorial on Multiple Imputation. Can. J. Cardiol. 2020, 37, 1322–1331. [Google Scholar] [CrossRef] [PubMed]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2010, 30, 377–399. [Google Scholar] [CrossRef] [PubMed]
- Di Leo, G.; Sardanelli, F. Statistical significance: P value, 0.05 threshold, and applications to radiomics—Reasons for a conservative approach. Eur. Radiol. Exp. 2020, 4, 18. [Google Scholar] [CrossRef] [PubMed]
- Guideline on The Choice of the Non-Inferiority Margin. Committee for Medicinal Products for Human Use. European Medicines Agency. 2005. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-choice-non-inferiority-margin_en.pdf (accessed on 3 January 2024).
- Ministry of Health Malaysia. Malaysia National Health Accounts. Health Expenditure Report 1997–2019. 2021. Available online: https://www.moh.gov.my/moh/resources/Penerbitan/Penerbitan%20Utama/MNHA/MNHA_Health_Expenditure_Report_1997-2019_02092021.pdf (accessed on 3 January 2024).




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | Elonide | Nasonex | Placebo | p Value |
|---|---|---|---|---|---|
| Subjects randomized to treatment, No. (%) | 163 (100) | 56 (34) | 54 (33) | 53 (33) | - |
| Age, mean (SD), (y) | 31.23 (8.29) | 32.16 (8.61) | 31.57 (8.41) | 29.91 (7.78) | 0.25 |
| Gender, No. (%) | |||||
| Male | 51 (31.29) | 19 (33.93) | 16 (29.63) | 16 (30.19) | 0.87 |
| Female | 112 (68.71) | 37 (66.07) | 38 (70.37) | 37 (69.81) | |
| Intent to treat (ITT) | 163 | 56 | 54 | 53 | - |
| Subjects completed treatment | 155 | 53 | 52 | 50 | - |
| Subjects discontinued treatment, No. (%) | 8 (4.9) | 3 (1.84) | 2 (1.23) | 3 (1.84) | - |
| Reason for discontinuation: | |||||
| Lost to follow-up | 6 | 2 | 2 | 2 | - |
| Did not wish to continue | 2 | 1 | 0 | 1 | - |
| Medication(s): | |||||
| Nasal spray only, No. (%) | 157 (96.32) | 55 (33.74) | 54 (33.13) | 48 (29.45) | - |
| Nasal spray + antihistamine, No. (%) | 6 (3.68) | 1 (0.61) | 0 (0) | 5 (3.07) | - |
| VAS (mm), mean (SD) ᵃ | 56.32 (19.74) | 57.09 (17.14) | 54.61 (20.71) | 57.25 (21.38) | 0.71 |
| RQOLQ, mean (SD) ᵃ | 2.98 (1.30) | 2.87 (1.17) | 2.91 (1.38) | 3.15 (1.36) | 0.49 |
| TNR (Pa/cm3/s), mean (SD) ᵃ | 1.12 (1.62) | 1.37 (2.55) | 1.17 (1.48) | 0.81 (0.83) | 0.26 |
| Treatment Group | Outcome Measures | Pretreatment | Post-Treatment | p Value |
|---|---|---|---|---|
| Elonide | TNR (Pa/cm3/s) | 1.37 (2.55) | 0.56 (0.35) | <0.01 |
| VAS (mm) | 57.09 (17.14) | 33.90 (17.80) | <0.01 | |
| RQOLQ | 2.87 (1.17) | 1.39 (0.95) | <0.01 | |
| Nasonex® | TNR (Pa/cm3/s) | 1.17 (1.48) | 0.77 (0.60) | <0.01 |
| VAS (mm) | 54.61 (20.71) | 37.04 (21.73) | <0.01 | |
| RQOLQ | 2.91 (1.38) | 1.59 (1.22) | <0.01 | |
| Placebo | TNR (Pa/cm3/s) | 0.81 (0.83) | 0.64 (0.40) | <0.01 |
| VAS (mm) | 57.25 (21.38) | 40.51 (21.48) | <0.01 | |
| RQOLQ | 3.15 (1.36) | 1.88 (1.39) | <0.01 |
| Treatment Group | ||||
|---|---|---|---|---|
| Side Effects | Elonide (n = 56) | Nasonex® (n = 54) | Placebo (n = 53) | Total |
| Headaches | 2 (4%) | 4 (7%) | 3 (6%) | 9 (17%) |
| Sore throat | 2 (4%) | 4 (7%) | 3 (6%) | 9 (17%) |
| Cough | 1 (2%) | 2 (4%) | 1 (2%) | 4 (8%) |
| Nasal dryness | 1 (2%) | 1 (2%) | 0 (0%) | 2 (4%) |
| Nasal irritation | 0 (0%) | 1 (2%) | 1 (2%) | 2 (4%) |
| Epistaxis | 0 (0%) | 1 (2%) | 0 (0%) | 1 (2%) |
| Imbalance | 0 (0%) | 1 (2%) | 0 (0%) | 1 (2%) |
| Total | 6 (12%) | 14 (26%) | 8 (16%) | 28 (54%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gendeh, H.S.; Hamizan, A.W.; Husain, S.; Nawi, A.M.; Zahedi, F.D.; Megat Ismail, N.F.; M. Farit, N.A. The Efficacy of Elonide Nasal Corticosteroids in Managing Allergic Rhinitis: A Randomized, Double-Blinded Trial. J. Clin. Med. 2024, 13, 1883. https://doi.org/10.3390/jcm13071883
Gendeh HS, Hamizan AW, Husain S, Nawi AM, Zahedi FD, Megat Ismail NF, M. Farit NA. The Efficacy of Elonide Nasal Corticosteroids in Managing Allergic Rhinitis: A Randomized, Double-Blinded Trial. Journal of Clinical Medicine. 2024; 13(7):1883. https://doi.org/10.3390/jcm13071883
Chicago/Turabian StyleGendeh, Hardip S., Aneeza W. Hamizan, Salina Husain, Azmawati M. Nawi, Farah D. Zahedi, Nur Fadhilah Megat Ismail, and N. Ammal M. Farit. 2024. "The Efficacy of Elonide Nasal Corticosteroids in Managing Allergic Rhinitis: A Randomized, Double-Blinded Trial" Journal of Clinical Medicine 13, no. 7: 1883. https://doi.org/10.3390/jcm13071883