

Adjuvant Chemotherapy in Patients with Locally Advanced Upper Tract Urothelial Carcinoma with or without Kidney Transplantation

Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemotherapy Regimen and Schedule
2.2. Outcome Measures
2.3. Statistical Analysis
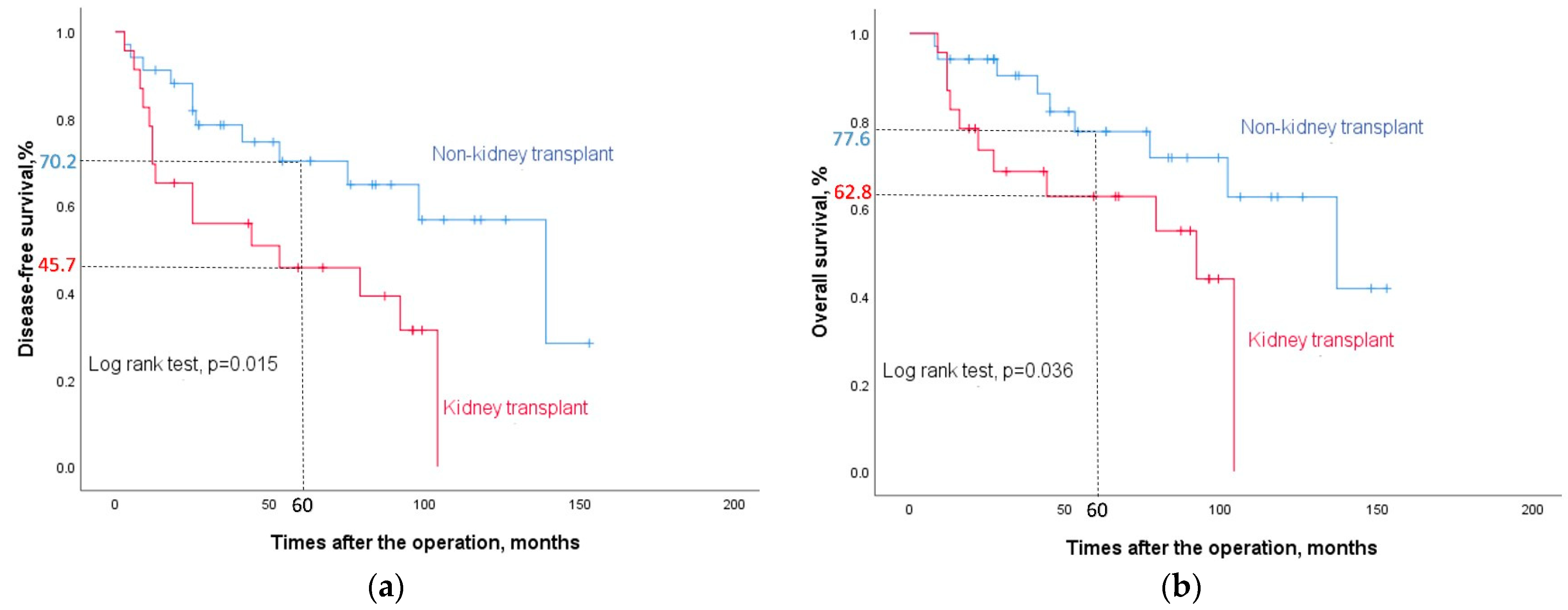
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Health Promotion Administration, Ministry of Health and Welfare, Taiwan. Cancer Registry Annual Report, 2021, Taiwan. Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=269&pid=17639 (accessed on 1 October 2023).
- Chang, C.W.; Ou, C.H.; Yu, C.C.; Lo, C.W.; Tsai, C.Y.; Cheng, P.Y.; Chen, Y.T.; Huang, H.C.; Wu, C.C.; Li, C.C.; et al. Comparative analysis of patients with upper urinary tract urothelial carcinoma in black-foot disease endemic and non-endemic area. BMC Cancer 2021, 21, 80. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.J.; Huang, Y.H.; Hsieh, T.Y.; Yang, M.H.; Wang, S.C.; Chen, W.J.; Lee, T.H.; Sung, W.W.; Chen, S.L. Native Kidney Hydronephrosis Is Associated with Upper Urinary Tract Urothelial Carcinoma in Post-Kidney Transplantation Patients. J. Clin. Med. 2021, 10, 4474. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.J.; Lian, J.D.; Yang, C.R.; Cheng, C.H.; Chen, C.H.; Lee, W.C.; Shu, K.H.; Tang, M.J. High cumulative incidence of urinary tract transitional cell carcinoma after kidney transplantation in Taiwan. Am. J. Kidney Dis. 2004, 43, 1091–1097. [Google Scholar] [CrossRef]
- Aziz, A.; Dobruch, J.; Hendricksen, K.; Kluth, L.A.; Necchi, A.; Noon, A.; Rink, M.; Roghmann, F.; Seiler, R.; Gontero, P.; et al. Perioperative chemotherapy in upper tract urothelial carcinoma: A comprehensive review. World J. Urol. 2017, 35, 1401–1407. [Google Scholar] [CrossRef] [PubMed]
- Roupret, M.; Babjuk, M.; Comperat, E.; Zigeuner, R.; Sylvester, R.J.; Burger, M.; Cowan, N.C.; Gontero, P.; Van Rhijn, B.W.G.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2017 Update. Eur. Urol. 2018, 73, 111–122. [Google Scholar] [CrossRef]
- Birtle, A.; Johnson, M.; Chester, J.; Jones, R.; Dolling, D.; Bryan, R.T.; Harris, C.; Winterbottom, A.; Blacker, A.; Catto, J.W.F.; et al. Adjuvant chemotherapy in upper tract urothelial carcinoma (the POUT trial): A phase 3, open-label, randomised controlled trial. Lancet 2020, 395, 1268–1277. [Google Scholar] [CrossRef]
- Bajorin, D.F.; Witjes, J.A.; Gschwend, J.E.; Schenker, M.; Valderrama, B.P.; Tomita, Y.; Bamias, A.; Lebret, T.; Shariat, S.F.; Park, S.H.; et al. Adjuvant Nivolumab versus Placebo in Muscle-Invasive Urothelial Carcinoma. N. Engl. J. Med. 2021, 384, 2102–2114. [Google Scholar] [CrossRef]
- Chen, C.H.; Dickman, K.G.; Moriya, M.; Zavadil, J.; Sidorenko, V.S.; Edwards, K.L.; Gnatenko, D.V.; Wu, L.; Turesky, R.J.; Wu, X.R.; et al. Aristolochic acid-associated urothelial cancer in Taiwan. Proc. Natl. Acad. Sci. USA 2012, 109, 8241–8246. [Google Scholar] [CrossRef]
- Seisen, T.; Krasnow, R.E.; Bellmunt, J.; Roupret, M.; Leow, J.J.; Lipsitz, S.R.; Vetterlein, M.W.; Preston, M.A.; Hanna, N.; Kibel, A.S.; et al. Effectiveness of Adjuvant Chemotherapy After Radical Nephroureterectomy for Locally Advanced and/or Positive Regional Lymph Node Upper Tract Urothelial Carcinoma. J. Clin. Oncol. 2017, 35, 852–860. [Google Scholar] [CrossRef]
- Necchi, A.; Lo Vullo, S.; Mariani, L.; Moschini, M.; Hendricksen, K.; Rink, M.; Sosnowski, R.; Dobruch, J.; Raman, J.D.; Wood, C.G.; et al. Adjuvant chemotherapy after radical nephroureterectomy does not improve survival in patients with upper tract urothelial carcinoma: A joint study by the European Association of Urology-Young Academic Urologists and the Upper Tract Urothelial Carcinoma Collaboration. BJU Int. 2018, 121, 252–259. [Google Scholar] [CrossRef]
- Zhang, P.; Zhang, X.D.; Wang, Y.; Wang, W. Feasibility of pre- and postoperative gemcitabine-plus-cisplatin systemic chemotherapy for the treatment of locally advanced urothelial carcinoma in kidney transplant patients. Transplant. Proc. 2013, 45, 3293–3297. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.P.; Wang, W.Y.; Zhu, Y.C.; Xiao, J.; Lin, J.; Guo, Y.W.; Tian, Y. Adjuvant Chemotherapy With Gemcitabine Plus Cisplatin for Kidney Transplant Patients With Locally Advanced Transitional Cell Carcinoma: A Single-center Experience. Transplant. Proc. 2016, 48, 2076–2079. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.L.; Chiang, P.H.; Cheng, Y.T.; Chen, Y.T. Propensity-Matched Survival Analysis of Upper Urinary Tract Urothelial Carcinomas between End-Stage Renal Disease with and without Kidney Transplantation. Biomed. Res. Int. 2019, 2019, 2979142. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.S.; Lu, C.L.; Huang, L.C.; Shen, C.H.; Chen, S.C. Chronic Kidney Disease is Associated With Upper Tract Urothelial Carcinoma: A Nationwide Population-Based Cohort Study in Taiwan. Medicine 2016, 95, e3255. [Google Scholar] [CrossRef]
- Correia, J.; Mendes, G.; Texeira, B.; Madanelo, M.; Fraga, A.; Silva-Ramos, M. Perioperative and oncological outcomes of laparoscopic and open radical nephroureterectomy for locally advanced upper tract urothelial carcinoma: A single-center cohort study. Cent. Eur. J. Urol. 2022, 75, 257–264. [Google Scholar] [CrossRef]
- Charbit, L.; Gendreau, M.C.; Mee, S.; Cukier, J. Tumors of the upper urinary tract: 10 years of experience. J. Urol. 1991, 146, 1243–1246. [Google Scholar] [CrossRef]
- Katayama, S.; Mori, K.; Schuettfort, V.M.; Pradere, B.; Mostafaei, H.; Quhal, F.; Rajwa, P.; Motlagh, R.S.; Laukhtina, E.; Moschini, M.; et al. Accuracy and Clinical Utility of a Tumor Grade- and Stage-based Predictive Model in Localized Upper Tract Urothelial Carcinoma. Eur. Urol. Focus. 2022, 8, 761–768. [Google Scholar] [CrossRef]
- Kwak, C.; Lee, S.E.; Jeong, I.G.; Ku, J.H. Adjuvant systemic chemotherapy in the treatment of patients with invasive transitional cell carcinoma of the upper urinary tract. Urology 2006, 68, 53–57. [Google Scholar] [CrossRef]
- Yu, J.; Lee, C.U.; Kang, M.; Jeon, H.G.; Jeong, B.C.; Seo, S.I.; Jeon, S.S.; Lee, H.M.; Sung, H.H. Incidences and oncological outcomes of urothelial carcinoma in kidney transplant recipients. Cancer Manag. Res. 2019, 11, 157–166. [Google Scholar] [CrossRef]
- Lughezzani, G.; Sun, M.; Perrotte, P.; Shariat, S.F.; Jeldres, C.; Budaus, L.; Latour, M.; Widmer, H.; Duclos, A.; Benard, F.; et al. Gender-related differences in patients with stage I to III upper tract urothelial carcinoma: Results from the Surveillance, Epidemiology, and End Results database. Urology 2010, 75, 321–327. [Google Scholar] [CrossRef]
- Yang, M.H.; Chen, K.K.; Yen, C.C.; Wang, W.S.; Chang, Y.H.; Huang, W.J.; Fan, F.S.; Chiou, T.J.; Liu, J.H.; Chen, P.M. Unusually high incidence of upper urinary tract urothelial carcinoma in Taiwan. Urology 2002, 59, 681–687. [Google Scholar] [CrossRef]
- Wu, Y.T.; Luo, H.L.; Wang, H.J.; Chen, Y.T.; Cheng, Y.T.; Chiang, P.H. Gender effect on the oncologic outcomes of upper urinary tract urothelial carcinoma in Taiwan. Int. Urol. Nephrol. 2020, 52, 1043–1048. [Google Scholar] [CrossRef]
- Lin, M.Y.; Niu, S.W.; Li, W.M.; Lee, H.L.; Chen, L.T.; Wu, W.J.; Hwang, S.J. Incidence and survival variations of upper tract urothelial cancer in Taiwan (2001–2010). Int. J. Urol. 2022, 29, 121–127. [Google Scholar] [CrossRef]
- Kao, Y.L.; Ou, Y.C.; Yang, C.R.; Ho, H.C.; Su, C.K.; Shu, K.H. Transitional cell carcinoma in renal transplant recipients. World J. Surg. 2003, 27, 912–916. [Google Scholar] [CrossRef]
- Tan, L.B.; Chen, K.T.; Guo, H.R. Clinical and epidemiological features of patients with genitourinary tract tumour in a blackfoot disease endemic area of Taiwan. BJU Int. 2008, 102, 48–54. [Google Scholar] [CrossRef]
- Kaczmarek, K.; Leminski, A.; Golab, A.; Slojewski, M. Survival differences of patients with ureteral versus pelvicalyceal tumours: A systematic review and meta-analysis. Arch. Med. Sci. 2021, 17, 603–612. [Google Scholar] [CrossRef]
- Li, W.H.; Chen, Y.J.; Tseng, W.C.; Lin, M.W.; Chen, T.J.; Chu, S.Y.; Hwang, C.Y.; Chen, C.C.; Lee, D.D.; Chang, Y.T.; et al. Malignancies after renal transplantation in Taiwan: A nationwide population-based study. Nephrol. Dial. Transplant. 2012, 27, 833–839. [Google Scholar] [CrossRef]
- Yin, W.Y.; Lee, M.C.; Lai, N.S.; Lu, M.C. BK virus as a potential oncovirus for bladder cancer in a renal transplant patient. J. Formos. Med. Assoc. 2015, 114, 373–374. [Google Scholar] [CrossRef]
- Hellemans, R.; Pengel, L.H.M.; Choquet, S.; Maggiore, U.; ESOT Workstream 3 of the TLJ. Managing immunosuppressive therapy in potentially cured post-kidney transplant cancer (excluding non-melanoma skin cancer): An overview of the available evidence and guidance for shared decision-making. Transpl. Int. 2021, 34, 1789–1800. [Google Scholar] [CrossRef]
- Powles, T.; Bellmunt, J.; Comperat, E.; De Santis, M.; Huddart, R.; Loriot, Y.; Necchi, A.; Valderrama, B.P.; Ravaud, A.; Shariat, S.F.; et al. Bladder cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2022, 33, 244–258. [Google Scholar] [CrossRef]
- Tufano, A.; Perdona, S.; Viscuso, P.; Frisenda, M.; Canale, V.; Rossi, A.; Del Prete, P.; Passaro, F.; Calarco, A. The Impact of Ethnicity and Age on Distribution of Metastases in Patients with Upper Tract Urothelial Carcinoma: Analysis of SEER Data. Biomedicines 2023, 11, 1943. [Google Scholar] [CrossRef] [PubMed]
- Tully, K.H.; Krimphove Md, M.J.; Huynh, M.J.; Marchese, M.; Kibel, A.S.; Noldus, J.; Kluth, L.A.; McGregor, B.; Chang, S.L.; Trinh, Q.D.; et al. Differences in survival and impact of adjuvant chemotherapy in patients with variant histology of tumors of the renal pelvis. World J. Urol. 2020, 38, 2227–2236. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| KT (n = 23) | Non-KT (n = 34) | p Value | |
|---|---|---|---|
| Mean age (years) | 59.39 ± 9.14 | 61.38 ± 10.23 | 0.455 |
| Gender (M/F) | 5/18 | 18/16 | 0.018 |
| pT stage | 0.159 | ||
| pT2 | 6 | 4 | |
| pT3 | 16 | 30 | |
| pT4 | 1 | 0 | |
| N stage | 0.08 | ||
| N0 | 21 | 34 | |
| N1 | 0 | 0 | |
| N2 | 2 | 0 | |
| Tumor size (cm) | 2.85 ± 2.78 | 4.93 ± 3.78 | 0.028 |
| Margin positive/negative | 4/19 | 4/30 | 0.549 |
| Multifocality | 17 | 14 | 0.015 |
| History of contralateral UTUC (%) | 11 (47.8) | 1 (2.9) | <0.001 |
| Previous | 1 (4.3) | 0 (0) | 0.220 |
| Concurrent | 10 (43.5) | 1 (2.9) | <0.001 |
| Recurrent | 2 (8.7) | 0 (0) | 0.08 |
| History of bladder UC (%) | 14 (60.9) | 15(44.1) | 0.215 |
| Previous | 5 (21.7) | 2 (5.9) | 0.074 |
| Concurrent | 8 (34.8) | 5 (14.7) | 0.076 |
| Recurrent | 10 (43.5) | 12 (35.3) | 0.533 |
| High grade | 22 | 32 | 0.799 |
| CIS | 10 | 6 | 0.033 |
| LVI | 10 | 12 | 0.533 |
| Follow-up (months) | 52.35 ± 34.56 | 64.71 ± 42.29 | 0.250 |
| No. operative method (%) Laparoscopic Open | 7 16 | 21 13 | 0.02 |
| No. tumor location (%) Renal pelvis Ureter Synchronous renal pelvis + ureter | 2 5 16 | 15 8 11 | 0.007 |
| Chemotherapy cycle 1–2 3–6 ≥7 unknown | 6 16 0 1 | 5 26 2 1 | 0.306 |
| Adjuvant chemotherapy regimen G + C G + Carbo G MVAC unknown | 13 10 0 0 0 | 18 11 2 2 1 | 0.366 |
| Mean eGFR mL/min | 65.1 ± 26.64 | 57.92 ± 23.26 | 0.285 |
| No. eGFR ≥ 60 mL/min (%) No. eGFR < 60 mL/min (%) | 12 (52.2) 11 (47.8) | 20 (58.8) 14 (41.2) | 0.620 |
| Disease-Free Survival | Overall Survival | |||||||
|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | |||||
| OR (95% CI) | p Value | OR (95% CI) | p Value | OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Kidney transplant | 2.545 (1.159–5.590) | 0.02 | 1.445 (0.575–3.629) | 0.433 | 2.626 (1.031–6.687) | 0.043 | 1.170 (0.400–3.422) | 0.774 |
| Age: <60 vs. ≥60 | 0.976 (0.445–2.142) | 0.952 | 0.592 (0.233–1.506) | 0.271 | ||||
| Gender M vs. F | 1.392 (0.639–3.031) | 0.405 | 0.882 (0.350–2.221) | 0.790 | ||||
| pT stage: ≥pT3 vs. pT2 | 0.720 (0.270–1.916) | 0.510 | 1.156 (0.335–3.990) | 0.891 | ||||
| N stage N2 vs. N0 | 2.378 (0.556–10.169) | 0.243 | 1.097 (0.144–8.340) | 0.929 | ||||
| Tumor size: ≥4 vs. <4 cm | 1.100 (0.513–2.358) | 0.807 | 0.773 (0.314–1.906) | 0.576 | ||||
| Surgical margin: Positive vs. Negative | 2.639 (1.092–6.378) | 0.031 | 2.069 (0.815–5.250) | 0.126 | 3.258 (1.233–8.605) | 0.017 | 2.159 (0.765–6.092) | 0.146 |
| Multifocality | 1.714 (0.768–3.827) | 0.188 | 2.569 (0.926–7.129) | 0.070 | ||||
| Contralateral UTUC | 1.693 (0.732–3.918) | 0.219 | 1.728 (0.649–4.600) | 0.273 | ||||
| Bladder UC | 1.320 (0.604–2.885) | 0.486 | 0.970 (0.401–2.346) | 0.946 | ||||
| Tumor grade: High vs. Low | 0.534 (0.123–2.305) | 0.400 | 0.524 (0.120–2.293) | 0.391 | ||||
| CIS | 0.811 (0.348–1.892) | 0.628 | 0.777 (0.294–2.057) | 0.612 | ||||
| LVI | 1.546 (0.716–3.340) | 0.268 | 1.783 (0.734–4.332) | 0.202 | ||||
| Operative method: Open vs. Laparoscopy | 5.057 (1.908–13.407) | 0.001 | 3.783 (1.294–11.062) | 0.015 | 4.044 (1.347–12.141) | 0.013 | 3.466 (0.947–12.684) | 0.060 |
| Location | 0.124 | 0.604 | 0.056 | 0.136 | ||||
| Renal pelvis vs. Ureter | 0.281 (0.083–0.951) | 0.041 | 0.540 (0.148–1.973) | 0.351 | 0.071 (0.008–0.615) | 0.016 | 0.100 (0.010–0.962) | 0.046 |
| Renal pelvis + ureter vs. Ureter | 0.681 (0.284–1.633) | 0.389 | 0.702 (0.264–1.867) | 0.478 | 0.648 (0.240–1.752) | 0.393 | 0.710 (0.233–2.163) | 0.546 |
| eGFR < 60 mL/min/1.73 m2 | 0.967 (0.443–2.110) | 0.934 | 0.950 (0.382–2.365) | 0.912 | ||||
| CTCAE | Kidney Transplant | Non-Kidney Transplant | p Value | |
|---|---|---|---|---|
| Neutropenia | 0 1–2 3–4 | 3 4 16 | 1 16 16 | 0.036 |
| Anemia | 0 1–2 3–4 | 0 12 11 | 5 23 5 | 0.01 |
| Thrombocytopenia | 0 1–2 3–4 | 3 10 10 | 10 18 5 | 0.047 |
| Nausea/Vomiting | 0 1–2 3 | 17 5 1 | 24 8 1 | 0.949 |
| Nephrotoxicity | 0 1–2 3–4 | 14 6 3 | 25 6 2 | 0.457 |
| Hepatotoxicity | 0 1–2 3–4 | 17 5 1 | 24 9 0 | 0.449 |
| Skin rash | 0 1–2 | 21 2 | 29 4 | 0.683 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, N.-W.; Huang, Y.-H.; Sung, W.-W.; Chen, S.-L. Adjuvant Chemotherapy in Patients with Locally Advanced Upper Tract Urothelial Carcinoma with or without Kidney Transplantation. J. Clin. Med. 2024, 13, 1831. https://doi.org/10.3390/jcm13071831
Chang N-W, Huang Y-H, Sung W-W, Chen S-L. Adjuvant Chemotherapy in Patients with Locally Advanced Upper Tract Urothelial Carcinoma with or without Kidney Transplantation. Journal of Clinical Medicine. 2024; 13(7):1831. https://doi.org/10.3390/jcm13071831
Chicago/Turabian StyleChang, Nai-Wen, Yu-Hui Huang, Wen-Wei Sung, and Sung-Lang Chen. 2024. "Adjuvant Chemotherapy in Patients with Locally Advanced Upper Tract Urothelial Carcinoma with or without Kidney Transplantation" Journal of Clinical Medicine 13, no. 7: 1831. https://doi.org/10.3390/jcm13071831