
Augmented Reality-Assisted Transcanal Endoscopic Ear Surgery for Middle Ear Cholesteatoma
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
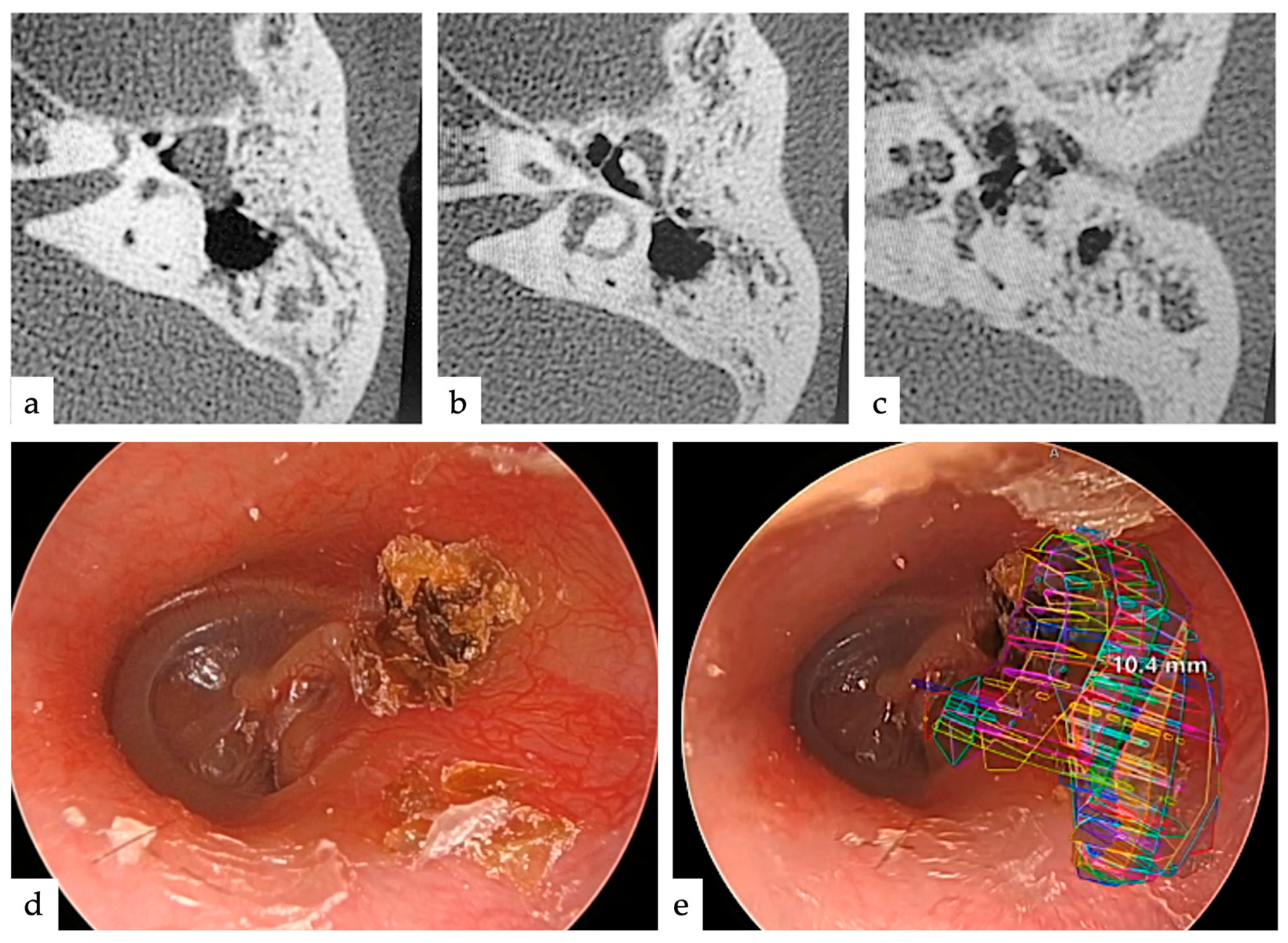
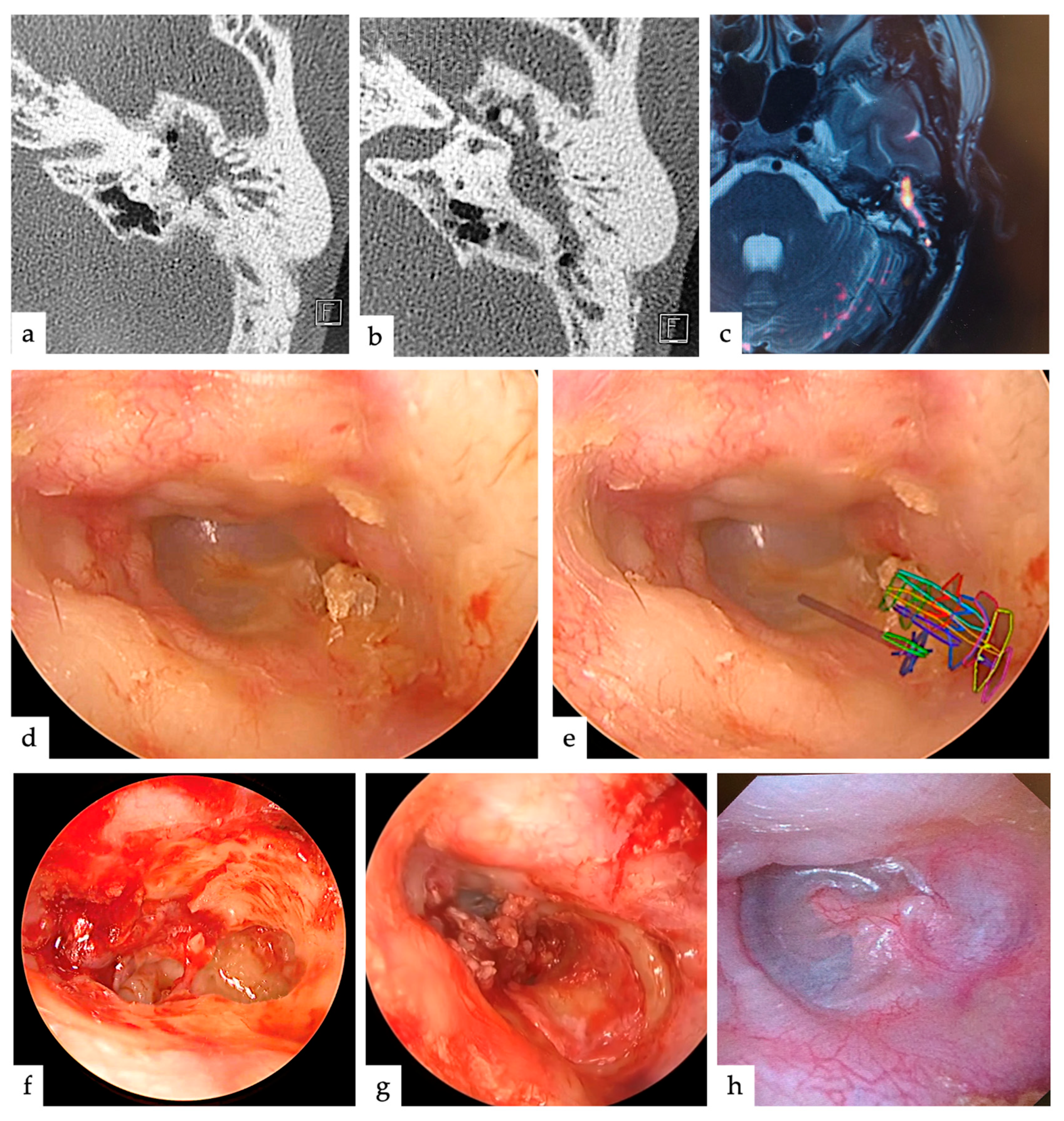
2.1. Cases and Treatment Strategies
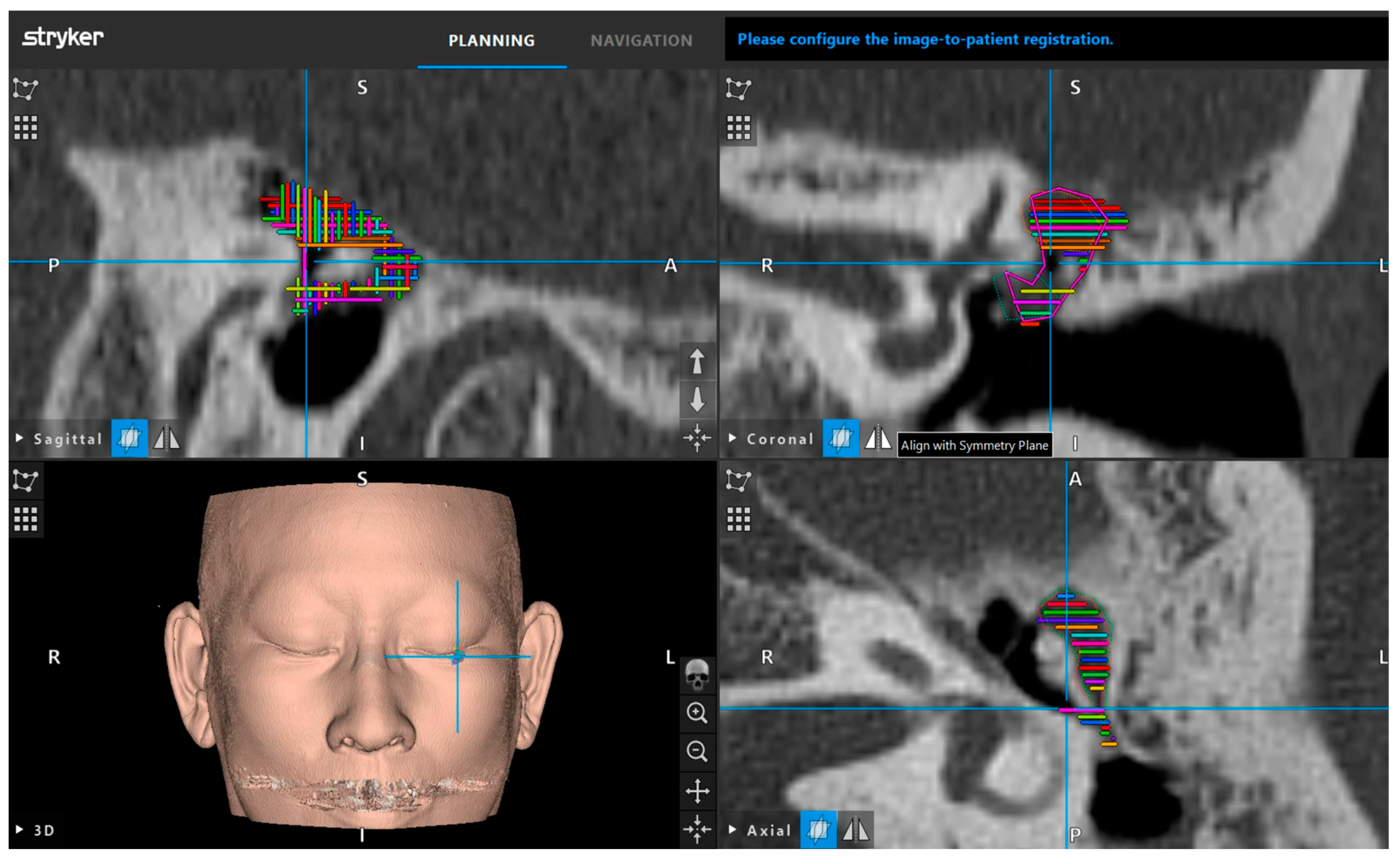
2.2. Navigation Systems
2.3. Setup
2.4. Registration
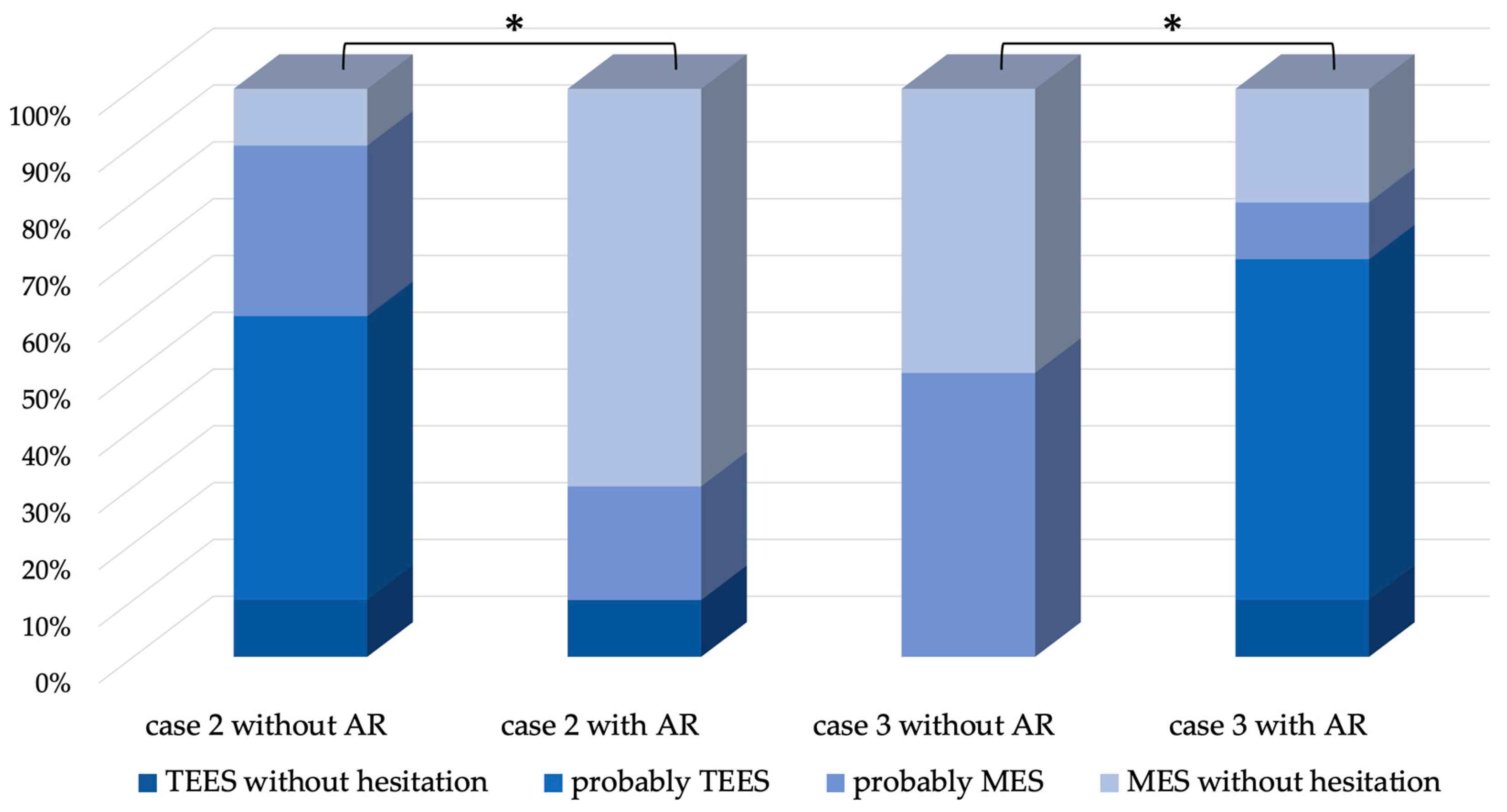
2.5. Questionnaires
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hashimoto-Ikehara, M.; Mishiro, Y.; Kitahara, T.; Sakagami, M. The 10-year disease-free rate of attic cholesteatoma based on a new staging system. J. Int. Adv. Otol. 2011, 7, 289–292. [Google Scholar]
- Nakazawa, T.; Yamamoto, Y.; Kanno, K.; Kurihara, S.; Takahashi, M.; Morino, T.; Motegi, M.; Yamamoto, K.; Sakurai, Y.; Kojima, H. Time analysis of recidivism in acquired cholesteatoma using the Kaplan-Meier method. Otol. Neurotol. 2023, 44, e393–e397. [Google Scholar] [CrossRef] [PubMed]
- Stangerup, S.E.; Drozdziewicz, D.; Tos, M.; Hougaard-Jensen, A. Recurrence of attic cholesteatoma: Different methods of estimating recurrence rates. Otolaryngol. Head Neck Surg. 2000, 123, 283–287. [Google Scholar]
- Mishiro, Y.; Sakagami, M.; Kitahara, T.; Kondoh, K.; Okumura, S. The investigation of the recurrence rate of cholesteatoma using Kaplan-Meier survival analysis. Otol. Neurotol. 2008, 29, 803–806. [Google Scholar] [CrossRef]
- Møller, P.R.; Pedersen, C.N.; Grosfjeld, L.R.; Faber, C.E.; Djurhuus, B.D. Recurrence of cholesteatoma—A retrospective study including 1,006 patients for more than 33 years. Int. Arch. Otorhinolaryngol. 2020, 24, e18–e23. [Google Scholar] [CrossRef] [PubMed]
- Eggink, M.C.; de Wolf, M.J.F.; Ebbens, F.A.; Dikkers, F.G.; van Spronsen, E. Assessing the prognostic value of the ChOLE classification in predicting the severity of acquired cholesteatoma. Otol. Neurotol. 2022, 43, 472–480. [Google Scholar] [CrossRef]
- Presutti, L.; Anschuetz, L.; Rubini, A.; Ruberto, M.; Alicandri-Ciufelli, M.; Dematte, M.; Caversaccio, M.; Marchioni, D. The impact of the transcanal endoscopic approach and mastoid preservation on recurrence of primary acquired attic cholesteatoma. Otol. Neurotol. 2018, 39, 445–450. [Google Scholar] [CrossRef]
- Kakehata, S.; Watanabe, T.; Ito, T.; Kubota, T.; Furukawa, T. Extension of indications for transcanal endoscopic ear surgery using an ultrasonic bone curette for cholesteatomas. Otol. Neurotol. 2014, 35, 101–107. [Google Scholar] [CrossRef]
- Kakehata, S.; Furukawa, T.; Ito, T.; Kubota, T.; Futai, K.; Watanabe, T. Comparison of postoperative pain in patients following transcanal endoscopic versus microscopic ear surgery. Otol. Neurotol. 2018, 39, 847–853. [Google Scholar] [CrossRef]
- Takahashi, M.; Motegi, M.; Yamamoto, K.; Yamamoto, Y.; Kojima, H. Quantitative study of bone removal region in transcanal endoscopic approach to the attic and antrum using a 70° endoscope. J. Int. Adv. Otol. 2022, 18, 232–235. [Google Scholar] [CrossRef]
- Takahashi, M.; Yamamoto, Y.; Kojima, H. Transcanal endoscopic approach for pars flaccida cholesteatoma using a 70-degree angled endoscope. Eur. Arch. Otorhinolaryngol. 2021, 278, 1283–1288. [Google Scholar] [CrossRef] [PubMed]
- Caudell, T.; Mizell, D. Augmented reality: An application of heads-up display technology to manual manufacturing processes. In Proceedings of the Twenty-Fifth Hawaii International Conference on System Sciences, Kauai, HI, USA, 7–10 January 1992. [Google Scholar] [CrossRef]
- Howard, G. A new collimating-telescope gunsight for large and small ordnance. Sci. Trans. R. Dublin Soc. 1901, 7, 321–330. [Google Scholar]
- Citardi, M.J.; Batra, P.S. Intraoperative surgical navigation for endoscopic sinus surgery: Rationale and indications. Curr. Opin. Otolaryngol. Head Neck Surg. 2007, 15, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Besharati Tabrizi, L.; Mahvash, M. Augmented reality-guided neurosurgery: Accuracy and intraoperative application of an image projection technique. J. Neurosurg. 2015, 123, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, N.; Hattori, A.; Iimura, J.; Otori, N.; Onda, S.; Okamoto, T.; Yanaga, K. Development of AR surgical navigation systems for multiple surgical regions. Stud. Health Technol. Inform. 2014, 196, 404–408. [Google Scholar] [PubMed]
- Winne, C.; Khan, M.; Stopp, F.; Jank, E.; Keeve, E. Overlay visualization in endoscopic ENT surgery. Int. J. Comput. Assist. Radiol. Surg. 2011, 6, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Ghaednia, H.; Fourman, M.S.; Lans, A.; Detels, K.; Dijkstra, H.; Lloyd, S.; Sweeney, A.; Oosterhoff, J.H.F.; Schwab, J.H. Augmented and virtual reality in spine surgery, current applications and future potentials. Spine J. 2021, 21, 1617–1625. [Google Scholar] [CrossRef]
- Sun, P.; Zhao, Y.; Men, J.; Ma, Z.-R.; Jiang, H.-Z.; Liu, C.-Y.; Feng, W. Application of virtual and augmented reality technology in hip surgery: Systematic review. J. Med. Internet Res. 2023, 25, e37599. [Google Scholar] [CrossRef]
- Begagic, E.; Bečulić, H.; Pugonja, R.; Memić, Z.; Balogun, S.; Džidić-Krivić, A.; Milanović, E.; Salković, N.; Nuhović, A.; Skomorac, R.; et al. Augmented reality integration in skull base neurosurgery: A systematic review. Medicina 2024, 60, 335. [Google Scholar] [CrossRef]
- Liu, W.P.; Azizian, M.; Sorger, J.; Taylor, R.H.; Reilly, B.K.; Cleary, K.; Preciado, D. Cadaveric feasibility study of da Vinci Si–assisted cochlear implant with augmented visual navigation for otologic surgery. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 208–214. [Google Scholar] [CrossRef]
- Schwam, Z.G.; Kaul, V.F.; Bu, D.D.; Iloreta, A.-M.C.; Bederson, J.B.; Perez, E.; Cosetti, M.K.; Wanna, G.B. The utility of augmented reality in lateral skull base surgery: A preliminary report. Am. J. Otolaryngol. 2021, 42, 102942. [Google Scholar] [CrossRef] [PubMed]
- Yung, M.; Tono, T.; Olszewska, E.; Yamamoto, Y.; Sudhoff, H.; Sakagami, M.; Mulder, J.; Kojima, H.; İncesulu, A.; Trabalzini, F.; et al. EAONO/JOS Joint Consensus statements on the definitions, classification and staging of middle ear cholesteatoma. J. Int. Adv. Otol. 2017, 13, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Mochizuki, H.; Watanabe, T.; Kubota, T.; Furukawa, T.; Koike, T.; Kakehata, S. Safety of ultrasonic bone curette in ear surgery by measuring skull bone vibrations. Otol. Neurotol. 2014, 35, e135–e139. [Google Scholar] [CrossRef] [PubMed]
- Batra, P.S.; Kanowitz, S.J.; Citardi, M.J. Clinical utility of intraoperative volume computed tomography scanner for endoscopic sinonasal and skull base procedures. Am. J. Rhinol. 2008, 22, 511–515. [Google Scholar] [CrossRef] [PubMed]
- Dixon, B.J.; Daly, M.J.; Chan, H.; Vescan, A.; Witterick, I.J.; Irish, J.C. Augmented real-time navigation with critical structure proximity alerts for endoscopic skull base surgery. Laryngoscope 2014, 124, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Jackman, A.H.; Palmer, J.N.; Chiu, A.G.; Kennedy, D.W. Use of intraoperative CT scanning in endoscopic sinus surgery: A preliminary report. Am. J. Rhinol. 2008, 22, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Leong, J.L.; Batra, P.S. Citardi MJ. CT-MRT image fusion for the management of skull base lesions. Otolaryngol. Head Neck Surg. 2006, 134, 868–876. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Yang, J.; Chu, Y.; Wu, W.; Xue, J.; Liang, P.; Chen, L. A novel augmented reality navigation system for endoscopic sinus and skull base surgery: A feasibility study. PLoS ONE 2016, 11, e0146996. [Google Scholar] [CrossRef]
- Maximilian, L. Augmented Reality-Enhanced Navigation in Endoscopic Sinus Surgery: A Prospective, Randomized, Controlled Clinical Trial. Laryngoscope Investig. Otol. 2020, 5, 621–629. [Google Scholar]
- Guigou, C.; Hussain, R.; Lalande, A.; Bozorg Grayeli, A. Augmented reality based transmodiolar cochlear implantation. Otol. Neurotol. 2022, 43, 190–198. [Google Scholar] [CrossRef]
- Miller, R.S.; Hashisaki, G.T.; Kesser, B.W. Image-guided localization of the internal auditory canal via the middle cranial fossa approach. Otolaryngol. Head Neck Surg. 2006, 134, 778–782. [Google Scholar] [CrossRef]
- Metzger, M.C.; Rafii, A.; Holhweg-Majert, B.; Pham, A.M.; Strong, B. Comparison of 4 registration strategies for computer-aided maxillofacial surgery. Otolaryngol. Head Neck Surg. 2007, 137, 93–99. [Google Scholar] [CrossRef]
- Kohan, D.; Jethanamest, D. Imageguided surgical naevigation in otology. Laryngoscope 2012, 122, 2291–2299. [Google Scholar] [CrossRef]
- Baba, A.; Kurihara, S.; Ogihara, A.; Matsushima, S.; Yamauchi, H.; Ikeda, K.; Kurokawa, R.; Ota, Y.; Takahashi, M.; Sakurai, Y.; et al. Preoperative predictive criteria for mastoid extension in pars flaccida cholesteatoma in assessments using temporal bone high-resolution computed tomography. Auris Nasus Larynx 2021, 48, 609–614. [Google Scholar] [CrossRef]
- Baba, A.; Kurokawa, R.; Kurokawa, M.; Ota, Y.; Matsushima, S.; Fukuda, T.; Yamauchi, H.; Kano, R.; Shoji, T.; Kurihara, S.; et al. Preoperative prediction for mastoid extension of middle ear cholesteatoma using temporal subtraction serial HRCT studies. Eur. Radiol. 2022, 32, 3631–3638. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Noda, K.; Yoshida, K.; Tsuchida, K.; Yui, R.; Nakazawa, T.; Kurihara, S.; Baba, A.; Motegi, M.; Yamamoto, K.; et al. Preoperative prediction by artificial intelligence for mastoid extension in pars flaccida cholesteatoma using temporal bone high-resolution computed tomography: A retrospective study. PLoS ONE 2022, 17, e0273915. [Google Scholar] [CrossRef] [PubMed]
- Baba, A.; Kurihara, S.; Fukuda, T.; Yamauchi, H.; Matsushima, S.; Ikeda, K.; Kurokawa, R.; Ota, Y.; Takahashi, M.; Sakurai, Y.; et al. Non-echoplanar diffusion weighed imaging and T1-weighted imaging for cholesteatoma mastoid extension. Auris Nasus Larynx 2021, 48, 846–851. [Google Scholar] [CrossRef] [PubMed]
- Migirov, L.; Wolf, M.; Greenberg, G.; Eyal, A. Non-EPI DW MRI in planning the surgical approach to primary and recurrent cholesteatoma. Otol. Neurotol. 2014, 35, 121–125. [Google Scholar] [CrossRef]
- Noschang Lopes da Silva, M.; Selaimen da Costa, S.; André Selaimen, F.; da Costa Huve, F.; Lang Silva, A.; Dias Toshiaki Koga, F.; Martins-Costa, L.L.; Bernard Rosa Nery, M.; Zanardini, M.; Sperling, N. Residual cholesteatoma after endoscopic-assisted canal wall-up tympanomastoidectomy: A randomized controlled trial. Otol. Neurotol. 2022, 43, 803–807. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age | Sex | Type | Range | TEES/MES |
|---|---|---|---|---|---|
| 1 | 44 | Male | pars flaccida | AM | TEES |
| 2 | 51 | Female | pars flaccida | TAM | MES |
| 3 | 41 | Male | pars flaccida | AM | TEES |
| 4 | 5 | Female | congenital | TAM | TEES |
| 5 | 41 | Male | pars flaccida | AM | TEES |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsuchida, K.; Takahashi, M.; Nakazawa, T.; Kurihara, S.; Yamamoto, K.; Yamamoto, Y.; Kojima, H. Augmented Reality-Assisted Transcanal Endoscopic Ear Surgery for Middle Ear Cholesteatoma. J. Clin. Med. 2024, 13, 1780. https://doi.org/10.3390/jcm13061780
Tsuchida K, Takahashi M, Nakazawa T, Kurihara S, Yamamoto K, Yamamoto Y, Kojima H. Augmented Reality-Assisted Transcanal Endoscopic Ear Surgery for Middle Ear Cholesteatoma. Journal of Clinical Medicine. 2024; 13(6):1780. https://doi.org/10.3390/jcm13061780
Chicago/Turabian StyleTsuchida, Keisuke, Masahiro Takahashi, Takara Nakazawa, Sho Kurihara, Kazuhisa Yamamoto, Yutaka Yamamoto, and Hiromi Kojima. 2024. "Augmented Reality-Assisted Transcanal Endoscopic Ear Surgery for Middle Ear Cholesteatoma" Journal of Clinical Medicine 13, no. 6: 1780. https://doi.org/10.3390/jcm13061780