
Changes of Sublingual Microcirculation during the Treatment of Severe Diabetic Ketoacidosis


1
Department of Pediatrics, Masaryk Hospital, Krajska Zdravotni, 40113 Usti nad Labem, Czech Republic
2
Faculty of Medicine in Hradec Kralove, Charles University, 50003 Hradec Kralove, Czech Republic
3
Department of Pediatrics, Trutnov Regional Hospital, 54101 Trutnov, Czech Republic
4
Department of Pediatrics, Faculty of Medicine in Hradec Kralove, Charles University, 50003 Hradec Kralove, Czech Republic
5
Department of Pediatrics, University Hospital Hradec Kralove, 50005 Hradec Kralove, Czech Republic
6
Department of Anaesthesiology and Intensive Care Medicine, Faculty of Medicine in Hradec Kralove, Charles University, 50003 Hradec Kralove, Czech Republic
7
Department of Anaesthesiology and Intensive Care Medicine, University Hospital Hradec Kralove, 50005 Hradec Kralove, Czech Republic
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2024, 13(6), 1655; https://doi.org/10.3390/jcm13061655
Submission received: 19 February 2024
/
Revised: 4 March 2024
/
Accepted: 12 March 2024
/
Published: 14 March 2024
(This article belongs to the Special Issue New Insights into Type 1 Diabetes)
Abstract
:Introduction: Diabetic ketoacidosis (DKA) is associated with volume depletion and hemodynamic alterations. Changes in systemic microcirculation during DKA have not been described so far. Methods: In this case report, we describe the evolution of sublingual microcirculatory changes, monitored using sidestream dark field (SDF) imaging during the treatment of severe diabetic ketoacidosis in a 13-year-old girl. The patient presented a pH of 6.84, a glycemia level of 27.2 mmol/L, a ketonemia level of 5.6 mmol/L, a base excess of −29.4 mmol/L, hypernatremia, hyperosmolality due to acute gastritis, and a malfunction of the glucose sensor. Sublingual microcirculation measurements using an SDF probe were initiated 60 min after the initiation of treatment, which was then repeated 2, 3, 4, 6, 12, and 24 h after treatment initiation, as well as on the day of discharge. Results: Substantial alterations of microvascular perfusion parameters, both total and small vessel densities, perfused vessel densities, and the DeBacker score, were observed during the first 6 to 12 h of treatment. The degree of microcirculatory alteration was strongly negatively correlated with calculated osmolality, sodium levels, ketone and lactate levels, and blood pressure values. Conclusions: DKA is, in its complexity, associated with a serious microcirculatory alteration. SDF imaging provides insight into the severity of the patient’s microcirculatory alteration and its evolution during treatment.
1. Introduction
Diabetic ketoacidosis (DKA) is a grievous acute complication of type 1 diabetes mellitus (T1D) that occurs when there is a lack of insulin in the body [1,2]. DKA is associated with volume depletion as a result of osmotic diuresis, vomiting, and hyperventilation [2], although its gradation does not correlate well with other patients’ clinical characteristics or laboratory findings [3]. In clinical studies, the mean dehydration was 5.2% and 5.7% of the bodyweight, respectively [4,5]. More severe dehydration was associated with a new onset of diabetes, higher blood urea nitrogen, lower pH, higher anion gap, and diastolic hypertension [5]. Clinical assessment was shown to be a poor predictor of the severity of dehydration and overestimated the dehydration in 67% of patients; therefore, it is recommended to assume moderate dehydration and to make adjustments in fluid therapy according to the clinical response [6].
During DKA, systemic hypotension due to volume depletion and vasodilation associated with ketoacidosis should theoretically occur [7]. On the contrary, some patients present hypertension [3]. Unfortunately, a loss of coherence between macrohemadynamic parameters and microcirculation may occur in hemodynamically unstable patients [8], and several mechanisms leading to impaired microcirculation due to a neurohumoral response to hyperosmolarity [9] could also be involved during DKA.
Microcirculation abnormalities have been known to correlate with organ dysfunction and mortality in various pathological situations, both in adults and in children, such as in sepsis and other hemodynamically compromised patients [8,10,11,12,13,14,15]. Changes in the microcirculation can be detected in the initial stages of the disease, and can persist even after normalization of macrohemodynamic parameters [10,16,17,18]. Thus, microcirculation monitoring is advised in patients diagnosed with circulatory shock [16,18].
Microcirculatory changes can be observed via direct visualization of the sublingual microcirculation by handheld vital microscopes, such as devices that utilize sidestream dark field imaging (SDF). These devices illuminate the tissue in depth (up to 3 mm, according to the manufacturer) by emitting green light, which is absorbed by the hemoglobin of the red blood cells in the surface vessels. This leads to the visualization of arterioles, capillaries, and venules containing erythrocytes [17,18]. SDF imaging has been used to study changes in microcirculation under various clinical conditions in animal and human studies, and is also a well-validated modality used to observe microcirculation [11,18,19]. This method was also recently tested for the early noninvasive detection of diabetic nephropathy [20].
In this case report, we describe the evolution of microcirculatory changes monitored using sidestream dark field imaging during the treatment of a child subject with severe diabetic ketoacidosis.
2. Case Presentation
A 13-year old girl with severe diabetic ketoacidosis was diagnosed with T1D a year and a half earlier. She was treated with multiple daily doses of subcutaneous insulin. She had unsatisfying home treatment results with HbA1c 63 mmol/mol measured from blood samples taken on admission. The patient presented symptoms of acute gastritis and severe ketoacidosis. She was somnolent and hyperventilating, with a pH of 6.84, glycemia levels of 27.2 mmol/L, ketonemia levels of 5.6 mmol/L, and a base excess of −29.4 mmol/L, corrected sodium levels of 155 mmol/L, and a calculated hyperosmolality of 324 mOsmol/kg. The continuous glucose sensor was malfunctioning. Fluid therapy and therapy with continuous insulin, according to current recommendations [21], were initiated. After an explanation of the procedure and parents’ informed consent, sublingual microcirculation measurements were initiated. The recorded data were not used to adjust the treatment. The continuous intravenous insulin application lasted two days. On the third day, the patient was transferred to a standard ward with adjusted multiple subcutaneous insulin doses, and the patient was discharged on the fourth day.
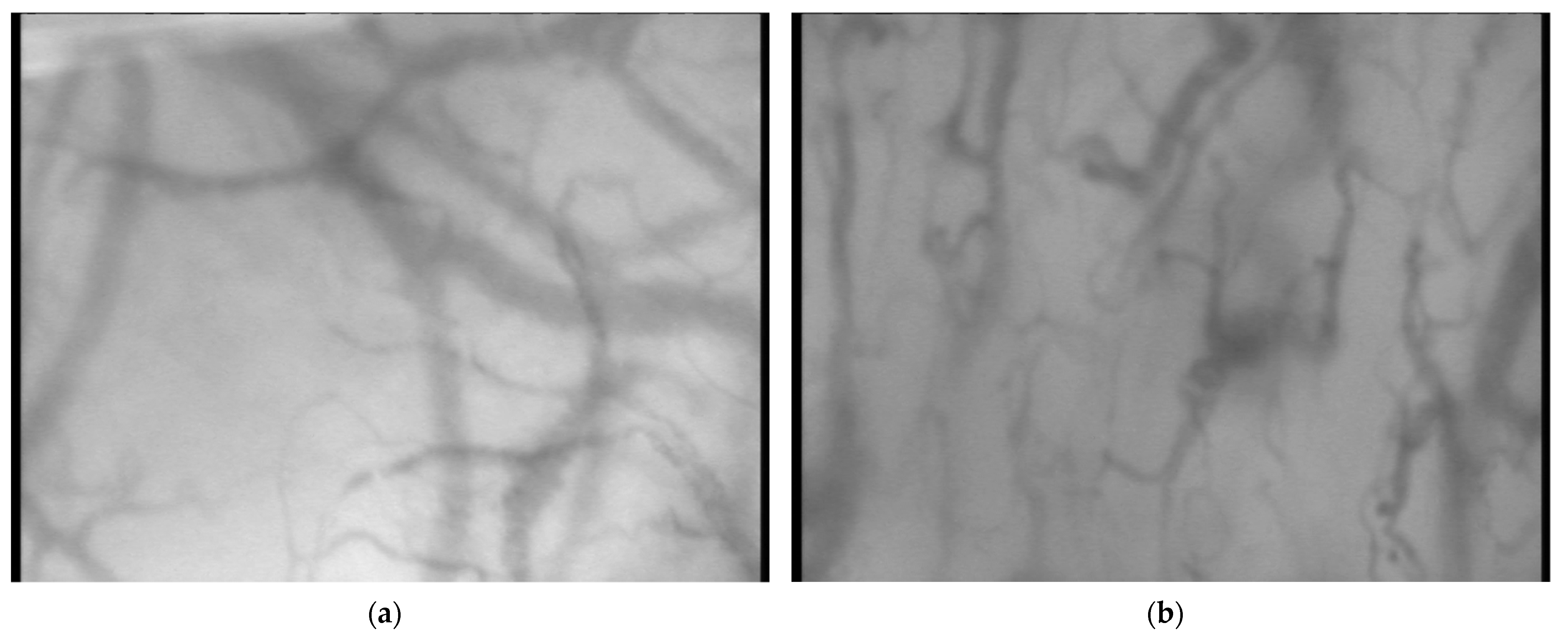
Sublingual microcirculation measurements using an SDF probe (MicroScan; MicroVision Medical, Amsterdam, The Netherlands) were performed in a supine position and initiated 60 min after the initiation of treatment. A total of three video clips of 20 s each from different parts of the sublingual region were recorded immediately after each other. The measurements were repeated 2, 3, 4, 6, 12, and 24 h after the treatment initiation, as well as on the day of discharge from the hospital by a single examiner. At the time of blood sampling, the acid–base balance, glycemia levels, and ketonemia levels from capillary arterialized blood were examined. Sample pictures of sublingual microcirculation from recorded video clips during and after the resolution of DKA are presented in Figure 1.
The recorded videos were processed offline using AVA V3.0 software (AMC, University of Amsterdam, Amsterdam, The Netherlands) by one trained and experienced evaluator. The three best and most stable parts of each video clip were analyzed. A 20 μm cut-off was used to separate small vessels (mostly capillaries) from large vessels (mostly venules). The following microcirculatory parameters were analyzed: The total small-vessel density (SVD) and all-vessel density (TVD) were defined as the total length of the respective vessels inside the image divided by the total area of the image. Small vessels were defined as those with diameters ≤ 20 μm [17,18]. The DeBacker score, given in mm−1, was defined as the number of vessels crossing three arbitrary horizontal and three vertical equidistant lines (drawn on the screen) divided by the total length of the lines [17]. The perfused small vessel density (PSVD) and the perfused vessel density (PVD) were obtained via the multiplication of the SVD and TVD by the respective proportion of perfused vessels [17]. The normal ranges of these parameters in children were recently published [22].
The recorded parameters included gender, age, height, weight, non-invasively measured blood pressure, heart rate, venous blood osmolality, urea, creatinine, C-reactive protein (CRP), acid–base balance, pH, PaO2, PaCO2, base excess, actual bicarbonate, sodium, potassium, chlorides, and lactate. A point-of-care glucometer which allowed for ketonemia measurements was used for sampling. The corrected sodium level was calculated using a calculator available at https://www.mdcalc.com/calc/50/sodium-correction-hyperglycemia, accessed on 12 December 2023, according to Hillier et al. [23].
The anthropometric and baseline laboratory parameters of the patient are summarized in Table 1.
Table 2 summarizes the evolution of selected microcirculatory, macrocirculatory, and laboratory parameters during the treatment. Microcirculatory parameters reached normal values after 6 to 12 h of treatment.
The correlations between clinical and microcirculatory parameters in this individual patient are presented in Table 3 and Table 4. They are listed according to the strength of the association between the parameter and TVD, measured using the Kendall rank correlation coefficient (the statistical software Medcalc 7.6.0/Medcalc, Ostend, Belgium/was used to perform statistical analyses).
3. Discussion
According to our knowledge, this is the first report describing the evolution of microcirculatory alterations in DKA using SDF imaging.
In this patient, severe microcirculatory alteration lasting from 6 to 12 h was associated with mild hypertension and hypernatremia. The pathophysiology of hypertension during DKA has yet to be fully understood. In children, hypertension was present in up to 82% of patients during the first 6 h following admission [24]. In a recently published analysis, higher blood glucose and higher glucose-corrected sodium levels and a low baseline pH, low pCO2, and low Glasgow Coma Scale levels were all identified as risk factors for hypertension during DKA [3]. This patient presented stage one systolic hypertension and diastolic prehypertension [25]. Her blood pressure normalized during therapy, parallel with an improving sublingual microcirculation. Although it was suggested that hypertension might reflect a neurophysiological response to altered brainstem perfusion [26], hypertension could also be a consequence of the increased release of vasopressin, or the over-activity of the renin-angiotensin system often described in patients with DKA [27].
Principally, four types of microcirculatory alterations could be identified: type 1, heterogeneous microcirculatory flow; type 2, reduced capillary density; type 3, microcirculatory flow reduction caused by vasoconstriction or tamponade; and type 4, tissue edema [8]. In this case, reduced capillary density was the leading alteration. Several mechanisms could be involved. The endothelial and smooth muscle cells predominantly regulate the microvascular blood flow via three main mechanisms: myogenic, neurohumoral, and metabolic control. Ketoacidosis could be associated with catecholamine release [28]. The lower partial pressure of CO2 (pCO2), lactate, adenosine, and H+, and the increased partial pressure of oxygen (pO2) are associated with vasoconstriction. Precapillary sphincters also constrict in response to concentrations of potassium, magnesium, osmolarity, and adenosine [29].
Hyperglycemia is well known for its lowering effect on serum sodium levels [23]. Although hyponatremia in DKA is, therefore, a more common symptom, hypernatremia can also occur. Its exact etiology is unclear, and several mechanisms related to water deficit from inadequate oral intake and free water loss have been proposed [26]. An excessive intake of carbonated carbohydrate-rich beverages has also worsened hypernatremia [30,31]. In our patient, sodium levels, especially glucose-corrected sodium, were increased, probably due to vomiting, a low oral intake of fluids, and urinary water loss. The degree of hypernatremia was strongly associated with the severity of microcirculatory alteration. Although we cannot generalize the relationships observed in this single case, this observation adds a further mechanistic explanation for the previously described evolution of peripheral gangrene in children with hypernatremic dehydration [32]. High sodium levels were shown to augment vasoconstrictor responses to catecholamines [33]. Hyperosmolarity also increases the release of vasopressin with the potential to alter microcirculation [9]. Hyperosmolarity, both due to high glucose levels and hypernatremia, could also induce vasoconstriction through the Rho/Rho-kinase signaling pathway [34]. The development of hypertension and microcirculatory alteration share several pathophysiological mechanisms, and both could reflect the intensity of the neurohumoral response to water depletion and hyperosmolarity during DKA.
The monitoring of microcirculatory alterations during DKA using SDF imaging is of potential clinical interest. This method of microcirculatory monitoring is noninvasive, repeatable, and validated under several clinical conditions. It may improve our understanding of DKA pathophysiology and our ability to predict the development of DKA complications early on [20]. Identifying microcirculatory alterations and the responses to treatment could enable personalized fluid therapy for groups of patients [35]. In theory, assessing the severity of microcirculatory alteration during DKA could also help distinguish non-genetic influences of the development of long-term complications of diabetes, such as retinopathy, neuropathy, or nephropathy. More studies on patients with both mild and severe forms of DKA, both with/without hypernatremia and hypertension, are needed to improve our understanding of DKA as it pertains to microcirculatory alteration and the clinical utility of SDF imaging.
4. Conclusions
In a child with mild hypertension, DKA with hypernatremia was associated with a serious alteration of sublingual microcirculation. SDF ismaging provided insight into the severity of the patient’s microcirculatory alteration and its evolution during treatment.
Author Contributions
Conceptualization, V.K. and D.N. Data collection, V.K.; Diabetic ketoacidosis treatment, J.S.; SDF measurement, V.K.; offline analysis, V.K.; methodology, V.K., P.D. and D.N.; writing—original draft preparation, V.K.; writing—review and editing, P.D. and D.N.; funding acquisition, P.D. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Charles University Cooperatio Program, research area INCA. The study’s planning and conduction, data interpretation, and the writing of the present manuscript are completely independent of the funder.
Institutional Review Board Statement
The case study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Medical Ethics Committee of the Regional Health a.s., Masaryk Hospital in Ústí nad Labem, o.z., file number 302/1.
Informed Consent Statement
Written informed consent was obtained from the patient to publish this case report and any accompanying images.
Data Availability Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Syed, F.Z. Type 1 Diabetes Mellitus. Ann. Intern. Med. 2022, 175, ITC33–ITC48. [Google Scholar] [CrossRef] [PubMed]
- Elendu, C.; David, J.A.M.; Udoyen, A.-O.M.; Egbunu, E.O.M.; Ogbuiyi-Chima, I.C.M.; Unakalamba, L.O.M.; Temitope, A.I.M.; Ibhiedu, J.O.M.; Ibhiedu, A.O.M.; Nwosu, P.U.M.; et al. Comprehensive review of diabetic ketoacidosis: An update. Ann. Med. Surg. 2023, 85, 2802–2807. [Google Scholar] [CrossRef] [PubMed]
- DePiero, A.; Kuppermann, N.; Brown, K.M.; Schunk, J.E.; McManemy, J.K.; Rewers, A.; Stoner, M.J.; Tzimenatos, L.; Garro, A.; Myers, S.R.; et al. Hypertension during Diabetic Ketoacidosis in Children. J. Pediatr. 2020, 223, 156–163.e5. [Google Scholar] [CrossRef] [PubMed]
- Trainor, J.L.; Glaser, N.S.; Tzimenatos, L.; Stoner, M.J.; Brown, K.M.; McManemy, J.K.; Schunk, J.E.; Quayle, K.S.; Nigrovic, L.E.; Rewers, A.; et al. Clinical and Laboratory Predictors of Dehydration Severity in Children with Diabetic Ketoacidosis. Ann. Emerg. Med. 2023, 82, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Ugale, J.; Mata, A.; Meert, K.L.; Sarnaik, A.P. Measured degree of dehydration in children and adolescents with type 1 diabetic ketoacidosis. Pediatr. Crit. Care Med. 2012, 13, e103–e107. [Google Scholar] [CrossRef]
- Fagan, M.J.; Avner, J.; Khine, H. Initial Fluid Resuscitation for Patients with Diabetic Ketoacidosis: How Dry Are They? Clin. Pediatr. 2008, 47, 851–855. [Google Scholar] [CrossRef]
- Singh, D.; Cantu, M.; Marx, M.H.M.; Akingbola, O. Diabetic Ketoacidosis and Fluid Refractory Hypotension. Clin. Pediatr. 2015, 55, 182–184. [Google Scholar] [CrossRef]
- Ince, C. Hemodynamic coherence and the rationale for monitoring the microcirculation. Crit. Care 2015, 19 (Suppl. S3), S8. [Google Scholar] [CrossRef]
- Charlton, J.A.; Thompson, C.J.; Baylis, P.H. Possible mechanisms responsible for the rise in plasma vasopressin associated with diabetic ketoacidosis in the rat. J. Endocrinol. 1988, 116, 343–348. [Google Scholar] [CrossRef]
- Salgado, D.R.; Favory, R.; De Backer, D. Microcirculatory assessment in daily clinical practice—Not yet ready but not too far! Einstein 2010, 8, 107–116. [Google Scholar] [CrossRef]
- De Backer, D.; Creteur, J.; Preiser, J.-C.; Dubois, M.-J.; Vincent, J.-L. Microvascular Blood Flow Is Altered in Patients with Sepsis. Am. J. Respir. Crit. Care Med. 2002, 166, 98–104. [Google Scholar] [CrossRef]
- Erdem, Ö.; Ince, C.; Tibboel, D.; Kuiper, J.W. Assessing the Microcirculation with Handheld Vital Microscopy in Critically Ill Neonates and Children: Evolution of the Technique and Its Potential for Critical Care. Front. Pediatr. 2019, 7, 273. [Google Scholar] [CrossRef] [PubMed]
- González, R.; Urbano, J.; Solana, M.J.; Hervías, M.; Pita, A.; Pérez, R.; Álvarez, R.; Teigell, E.; Gil-Jaurena, J.-M.; Zamorano, J.; et al. Microcirculatory Differences in Children with Congenital Heart Disease According to Cyanosis and Age. Front. Pediatr. 2019, 7, 264. [Google Scholar] [CrossRef] [PubMed]
- Wright, I.M.R.; Latter, J.L.; Dyson, R.M.; Levi, C.R.; Clifton, V.L. Videomicroscopy as a tool for investigation of the microcirculation in the newborn. Physiol. Rep. 2016, 4, e12941. [Google Scholar] [CrossRef] [PubMed]
- Nussbaum, C.; Heringa, A.C.F.; Mormanova, Z.; Puchwein-Schwepcke, A.F.; Pozza, S.B.-D.; Genzel-Boroviczény, O. Early Microvascular Changes with Loss of the Glycocalyx in Children with Type 1 Diabetes. J. Pediatr. 2014, 164, 584–589.e1. [Google Scholar] [CrossRef] [PubMed]
- Dilken, O.; Ergin, B.; Ince, C. Assessment of sublingual microcirculation in critically ill patients: Consensus and debate. Ann. Transl. Med. 2020, 8, 793. [Google Scholar] [CrossRef] [PubMed]
- De Backer, D.; Hollenberg, S.; Boerma, C.; Goedhart, P.; Büchele, G.; Ospina-Tascon, G.; Dobbe, I.; Ince, C. How to evaluate the microcirculation: Report of a round table conference. Crit. Care 2007, 11, R101. [Google Scholar] [CrossRef]
- Ince, C.; Boerma, E.C.; Cecconi, M.; De Backer, D.; Shapiro, N.I.; Duranteau, J.; Pinsky, M.R.; Artigas, A.; Teboul, J.-L.; Reiss, I.K.M.; et al. Second consensus on the assessment of sublingual microcirculation in critically ill patients: Results from a task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2018, 44, 281–299. [Google Scholar] [CrossRef]
- Boerma, E.C.; Mathura, K.R.; Van Der Voort, P.H.; Spronk, P.E.; Ince, C. Quantifying bedside-derived imaging of microcirculatory abnormalities in septic patients: A prospective validation study. Crit. Care 2005, 9, R601–R606. [Google Scholar] [CrossRef]
- Li, Q.; Liu, X.; Jia, M.; Sun, F.; Li, Y.; Zhang, H.; Liu, X.; He, H.; Zhao, Z.; Yan, Z.; et al. Assessment of sublingual microcirculation for the screening of diabetic nephropathy. Diabetol. Metab. Syndr. 2022, 14, 90. [Google Scholar] [CrossRef]
- Glaser, N.; Fritsch, M.; Priyambada, L.; Rewers, A.; Cherubini, V.; Estrada, S.; Wolfsdorf, J.I.; Codner, E. ISPAD Clinical Practice Consensus Guidelines 2022: Diabetic ketoacidosis and hyperglycemic hyperosmolar state. Pediatr. Diabetes 2022, 23, 835–856. [Google Scholar] [CrossRef] [PubMed]
- Krausova, V.; Neumann, D.; Kraus, J.; Dostalova, V.; Dostal, P. Sublingual microcirculation in healthy pediatric population using the sidestream dark-field imaging method. Clin. Hemorheol. Microcirc. 2023, 85, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Hillier, T.A.; Abbott, R.D.; Barrett, E.J. Hyponatremia: Evaluating the correction factor for hyperglycemia. Am. J. Med. 1999, 106, 399–403. [Google Scholar] [CrossRef]
- Deeter, K.H.; Roberts, J.S.; Bradford, H.; Richards, T.; Shaw, D.; Marro, K.; Chiu, H.; Pihoker, C.; Lynn, A.; Vavilala, M.S. Hypertension despite dehydration during severe pediatric diabetic ketoacidosis. Pediatr. Diabetes 2011, 12, 295–301. [Google Scholar] [CrossRef] [PubMed]
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 2004, 114 (Suppl. S2), 555–576. [Google Scholar] [CrossRef]
- Ibarra, G.; Majmundar, M.M.; Pacheco, E.; Zala, H.; Chaudhari, S. Hypernatremia in Diabetic Ketoacidosis: Rare Presentation and a Cautionary Tale. Cureus 2020, 12, e11841. [Google Scholar] [CrossRef] [PubMed]
- Durr, J.A.; Hoffman, W.H.; Hensen, J.; Sklar, A.H.; el Gammal, T.; Steinhart, C.M. Osmoregulation of vasopressin in diabetic ketoacidosis. Am. J. Physiol. Metab. 1990, 259, E723–E728. [Google Scholar] [CrossRef]
- Gandhi, M.J.; Suvarna, T.T. Cardiovascular complications in diabetic ketoacidosis. Int. J. Diab. Dev. Ctries. 1995, 15, 132–133. [Google Scholar]
- Hendricks, N. The microcirculation. S. Afr. J. Anaesth. Analg. 2020, 26 (Suppl. S3), S62–S65. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, D.H.; Jun, Y.H.; Lee, J.E. A rare diabetes ketoacidosis in combined severe hypernatremic hyperosmolarity in a new-onset Asian adolescent with type I diabetes. BMJ Case Rep. 2014, 2014, bcr2014208016. [Google Scholar] [CrossRef]
- McDonnell, C.M.; Pedreira, C.C.; Vadamalayan, B.; Cameron, F.J.; Werther, G.A. Diabetic ketoacidosis, hyperosmolarity and hypernatremia: Are high-carbohydrate drinks worsening initial presentation? Pediatr. Diabetes 2005, 6, 90–94. [Google Scholar] [CrossRef]
- Amitai, I.; Goder, K.; Husseini, N.; Rousso, M. Hypernatremic dehydration complicated by peripheral gangrene in infancy. Isr. J. Med. Sci. 1983, 19, 538–540. [Google Scholar]
- Heistad, D.D.; Abboud, F.M.; Ballard, D.R. Relationship between plasma sodium concentration and vascular reactivity in man. J. Clin. Investig. 1971, 50, 2022–2032. [Google Scholar] [CrossRef] [PubMed]
- Ün, I.; Kurt, A.H.; Büyükafşar, K. Hyperosmolar glucose induces vasoconstriction through Rho/Rho-kinase pathway in the rat aorta. Fundam. Clin. Pharmacol. 2011, 27, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Dai, C.; Zhu, Y.; Han, T.; Zhou, J.; Zhao, L.; Wang, X.; Liu, H.; Qu, J.; Li, W. The effectiveness and feasibility of fluid resuscitation directed by microcirculation monitoring in patients with septic shock: A randomized controlled trial. Ann. Palliat. Med. 2021, 10, 9069–9077. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Sample pictures taken from recorded videoclips during DKA (a) and after DKA resolution (b).
Figure 1.
Sample pictures taken from recorded videoclips during DKA (a) and after DKA resolution (b).


{kind=link}
Table 1.
Anthropometric and baseline laboratory parameters.
| Parameter | Value |
|---|---|
| Age | 13 |
| Height (cm) | 153 |
| Weight (kg) | 45.5 |
| Heart rate (/min) | 130 |
| SAP (mmHg) | 128 |
| DAP (mmHg) | 77 |
| MAP (mmHg) | 94 |
| SpO2 (%) | 100 |
| pH | 6.841 |
| pCO2 (kPa) | 3.23 |
| pO2 (kPa) | 15 |
| HCO3− (mmol/L) | 5.8 |
| Base excess (mmol/L) | −29.7 |
| Glucose (mmol/L) | 27.15 |
| Ketones (mmol/L) | 5.6 |
| HbA1c (mmol/moL) | 63 |
| CRP (mg/L) | <1 |
| Calculated Osmolality (mOsmol/kg) | 324 |
| Urea (mmol/L) | 4.6 |
| Creatinine (mmol/L) | 108 |
| Sodium (mmol/L) | 146 |
| Chlorides (mmol/L) | 113 |
| Potassium (mmol/L) | 4.3 |
| Lactate (mmol/L) | 4.1 |
SAP, Systolic arterial pressure; DAP, Diastolic arterial pressure; MAP, Mean arterial pressure; SpO2, O2 saturation of hemoglobin; HbA1c, glycated hemoglobin; CRP, C-reactive protein.
Table 2.
Evolution of selected microcirculatory and laboratory parameters.
| Parameter | Time (h) | |||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 6 | 12 | 24 | 51 | |
| TVD (mm/mm2) | 6.11 | 7.04 | 9.58 | 8.92 | 10.87 | 10.12 | 11.11 | 10.30 |
| SVD (mm/mm2) | 1.37 | 2.88 | 5.11 | 5.23 | 8.35 | 8.64 | 8.50 | 7.82 |
| PVD (mm/mm2) | 5.97 | 6.80 | 9.53 | 8.79 | 10.58 | 10.06 | 11.09 | 10.18 |
| PSVD (mm/mm2) | 1.32 | 2.73 | 5.06 | 5.23 | 8.06 | 8.59 | 8.47 | 7.68 |
| DeBS (1/mm) | 4.04 | 4.70 | 6.13 | 5.81 | 6.37 | 6.38 | 6.99 | 6.29 |
| SAP (mmHg) | 128 | 127 | 124 | 118 | 114 | 117 | 116 | 108 |
| DAP (mmHg) | 77 | 71 | 60 | 65 | 58 | 56 | 64 | 64 |
| MAP (mmHg) | 94 | 90 | 81 | 83 | 77 | 76 | 81 | 79 |
| pH | 6.84 | 7.04 | 7.09 | 7.16 | 7.19 | 7.28 | 7.31 | 7.47 |
| pO2 (kPa) | 15.0 | 15.1 | 15.2 | 15.2 | 12.9 | 7.7 | 9.2 | 9.0 |
| Glucose (mmol/L) | 27.15 | 14.9 | 13.8 | 12.4 | 13.5 | 14 | 15.2 | 10.8 |
| Ketones (mmol/L) | 5.6 | 4.5 | 4.4 | 3.9 | 2.6 | 2.3 | 2.6 | 0 |
| GCNa (mmol/L) | 155 | 149 | 150 | 146 | 145 | 147 | 144 | 144 |
| Lactate (mmol/L) | 4.1 | 1.3 | 1.3 | 1.0 | 0.8 | 0.9 | 0.7 | 2.2 |
| Calculated Osmolality (mOsm/kg) | 324 | 310 | 310 | 303 | 302 | 304 | 299 | 303 |
TVD, total vessel density; SVD, small vessel density; PVD, perfused vessel density; PSVD, perfused small vessel density; DeBS, DeBacker’s score; SAP, systolic arterial pressure; DAP, diastolic arterial pressure; MAP, mean arterial pressure; pO2, parcial O2 pressure; GCNa, glycemia corrected sodium.
Table 3.
Relationship between laboratory and microcirculatory parameters.
| TVD (mm/mm2) | SVD (mm/mm2) | PVD (mm/mm2) | PSVD (mm/mm2) | DeBS (1/mm) | |
|---|---|---|---|---|---|
| Calcutated osmolality (mOsm/kg) | −0.71 p = 0.009 | −0.57 p = 0.035 | −0.71 p = 0.009 | −0.57 p = 0.035 | −0.57 p = 0.035 |
| GCNa (mmol/L) | −0.69 | −0.55 | −0.69 | −0.55 | −0.55 |
| p = 0.012 | p = 0.044 | p = 0.012 | p = 0.044 | p = 0.044 | |
| Sodium (mmol/L) | −0.67 | −0.67 | −0.67 | −0.67 | −0.67 |
| p = 0.015 | p = 0.015 | p = 0.015 | p = 0.015 | p = 0.015 | |
| Ketones (mmol/L) | −0.62 | −0.76 | −0.62 | −0.76 | −0.62 |
| p = 0.023 | p = 0.006 | p = 0.023 | p = 0.006 | p = 0.023 | |
| Lactate (mmol/L) | −0.62 | −0.62 | −0.62 | −0.62 | −0.62 |
| p = 0.023 | p = 0.023 | p = 0.023 | p = 0.023 | p = 0.023 | |
| pO2 (kPa) | −0.26 | −0.47 | −0.26 | −0.47 | −0.40 |
| p = 0.314 | p = 0.078 | p = 0.314 | p = 0.078 | p = 0.131 | |
| Glucose (mmol/L) | −0.21 | −0.21 | −0.21 | −0.21 | −0.07 |
| p = 0.387 | p = 0.387 | p = 0.387 | p = 0.387 | p = 0.711 | |
| Chlorides (mmol/L) | 0.00 | 0.14 | 0.00 | 0.14 | 0.00 |
| p = 0.846 | p = 0.846 | p = 0.846 | p = 0.846 | p = 0.846 | |
| Glucose dose (mg/kg/min) | 0.16 | 0.24 | 0.16 | 0.24 | 0.16 |
| p = 0.675 | p = 0.485 | p = 0.675 | p = 0.485 | p = 0.675 | |
| pCO2 (kPa) | 0.33 | 0.20 | 0.33 | 0.20 | 0.33 |
| p = 0.452 | p = 0.707 | p = 0.452 | p = 0.707 | p = 0.452 | |
| HCO3− (mmol/L) | 0.60 | 0.47 | 0.60 | 0.47 | 0.60 |
| p = 0.133 | p = 0.260 | p = 0.133 | p = 0.260 | p = 0.133 | |
| BE (mmol/L) | 0.60 | 0.47 | 0.60 | 0.47 | 0.60 |
| p = 0.133 | p = 0.260 | p = 0.133 | p = 0.260 | p = 0.133 | |
| pH | 0.71 | 0.71 | 0.71 | 0.71 | 0.71 |
| p = 0.217 | p = 0.197 | p = 0.205 | p = 0.195 | p = 0.225 |
Results are presented as a value of the Kendall’s Tau and its p-value. TVD, total vessel density; SVD, small vessel density; PVD, perfused vessel density; PSVD, perfused small vessel density; DeBS, DeBacker’s score; pCO2, partial CO2 pressure; pO2, partial O2 pressure; HR, heart rate; BE, base excess; GCNa, glycemia corrected sodium.
Table 4.
Relationship between the macrocirculatory and microcirculatory parameters.
| TVD (mm/mm2) | SVD (mm/mm2) | PVD (mm/mm2) | PSVD (mm/mm2) | DeBS (1/mm) | |
|---|---|---|---|---|---|
| SAP (mmHg) | −0.71 | −0.57 | −0.71 | −0.57 | −0.57 |
| p = 0.009 | p = 0.035 | p = 0.009 | p = 0.035 | p = 0.035 | |
| MAP (mmHg) | −0.62 | −0.76 | −0.62 | −0.76 | −0.76 |
| p = 0.023 | p = 0.006 | p = 0.023 | p = 0.006 | p = 0.006 | |
| DAP (mmHg) | −0.55 | −0.69 | −0.55 | −0.69 | −0.69 |
| p = 0.044 | p = 0.012 | p = 0.044 | p = 0.012 | p = 0.012 | |
| HR (/min) | −0.55 | −0.40 | −0.55 | −0.40 | −0.55 |
| p = 0.044 | p = 0.131 | p = 0.044 | p = 0.131 | p = 0.044 |
Results are presented as a value of the Kendall’s Tau and its p-value. TVD, total vessel density; SVD, small vessel density; PVD, perfused vessel density; PSVD, perfused small vessel density; DeBS, DeBacker’s score; SAP, systolic arterial pressure; DAP, diastolic arterial pressure; MAP, mean arterial pressure.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Krausova, V.; Neumann, D.; Skvor, J.; Dostal, P. Changes of Sublingual Microcirculation during the Treatment of Severe Diabetic Ketoacidosis. J. Clin. Med. 2024, 13, 1655. https://doi.org/10.3390/jcm13061655
AMA Style
Krausova V, Neumann D, Skvor J, Dostal P. Changes of Sublingual Microcirculation during the Treatment of Severe Diabetic Ketoacidosis. Journal of Clinical Medicine. 2024; 13(6):1655. https://doi.org/10.3390/jcm13061655
Chicago/Turabian StyleKrausova, Vlasta, David Neumann, Jaroslav Skvor, and Pavel Dostal. 2024. "Changes of Sublingual Microcirculation during the Treatment of Severe Diabetic Ketoacidosis" Journal of Clinical Medicine 13, no. 6: 1655. https://doi.org/10.3390/jcm13061655
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.