

Is Active Synovitis of Metacarpophalangeal Joints a Neuropathic Condition in Rheumatoid Arthritis Patients? Results from an Ultrasound Study of Palmar Digital Nerves
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinical, Laboratory, and Radiographic Assessments
2.3. US Assessment
2.3.1. Acquisition of Articular Images
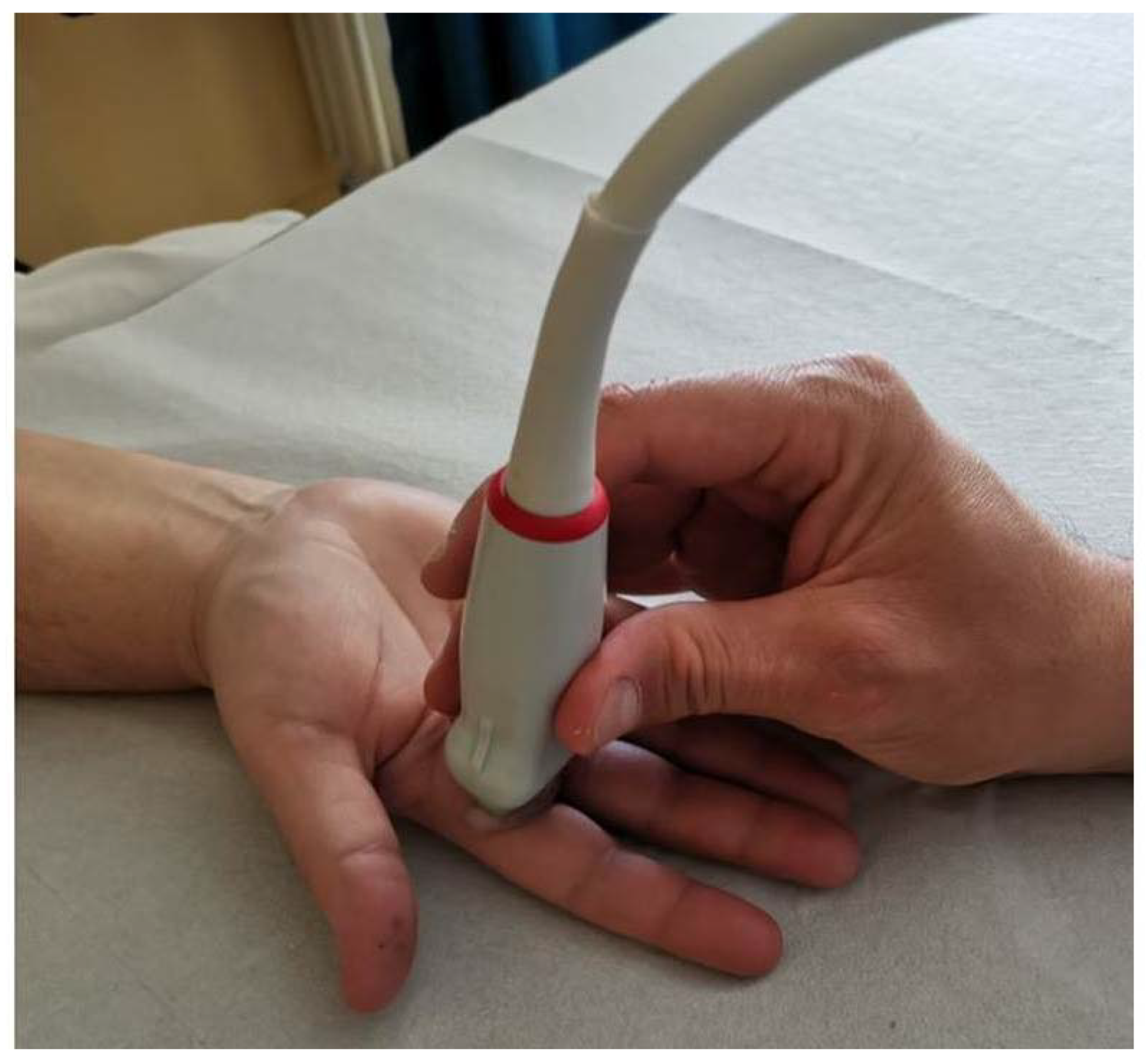
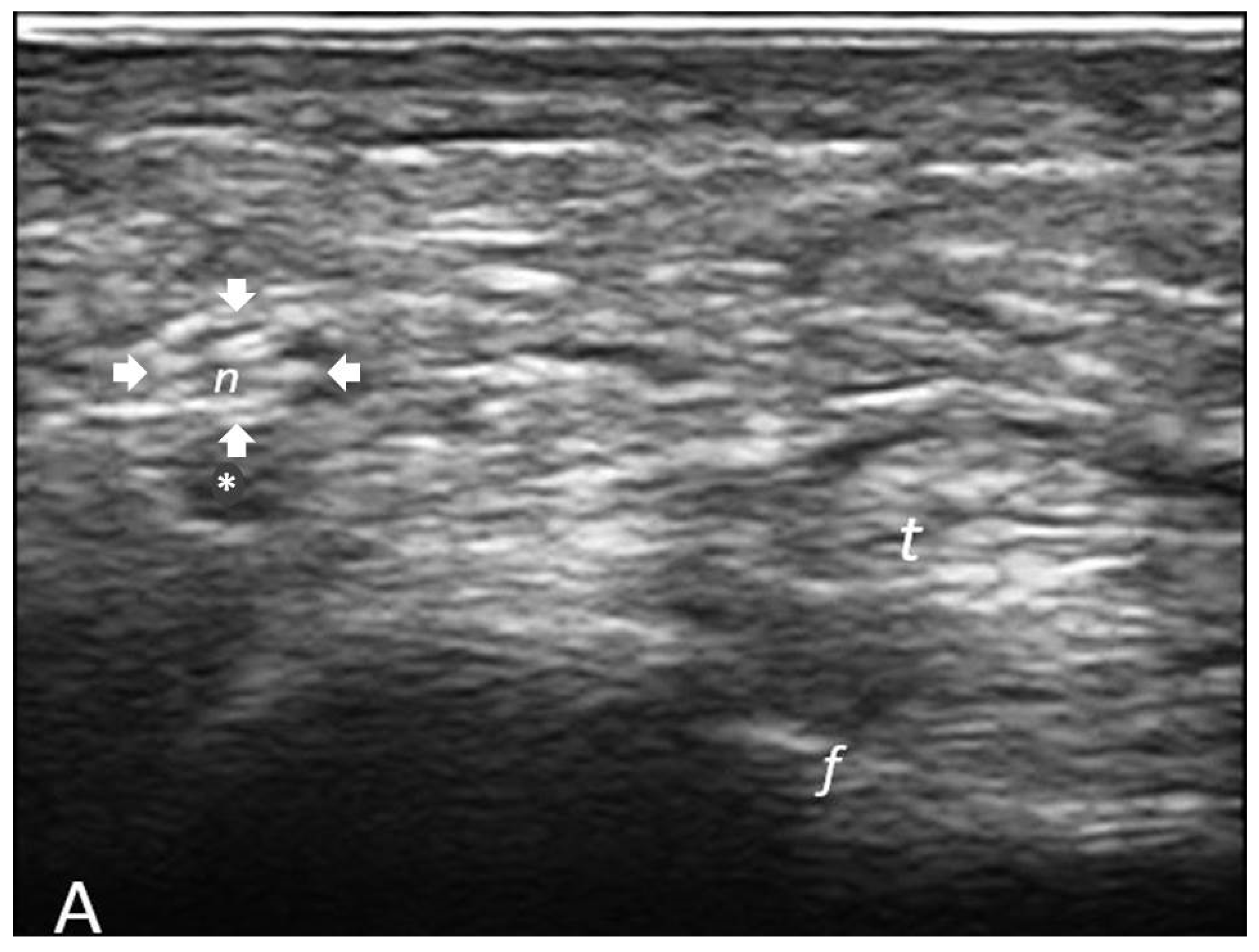
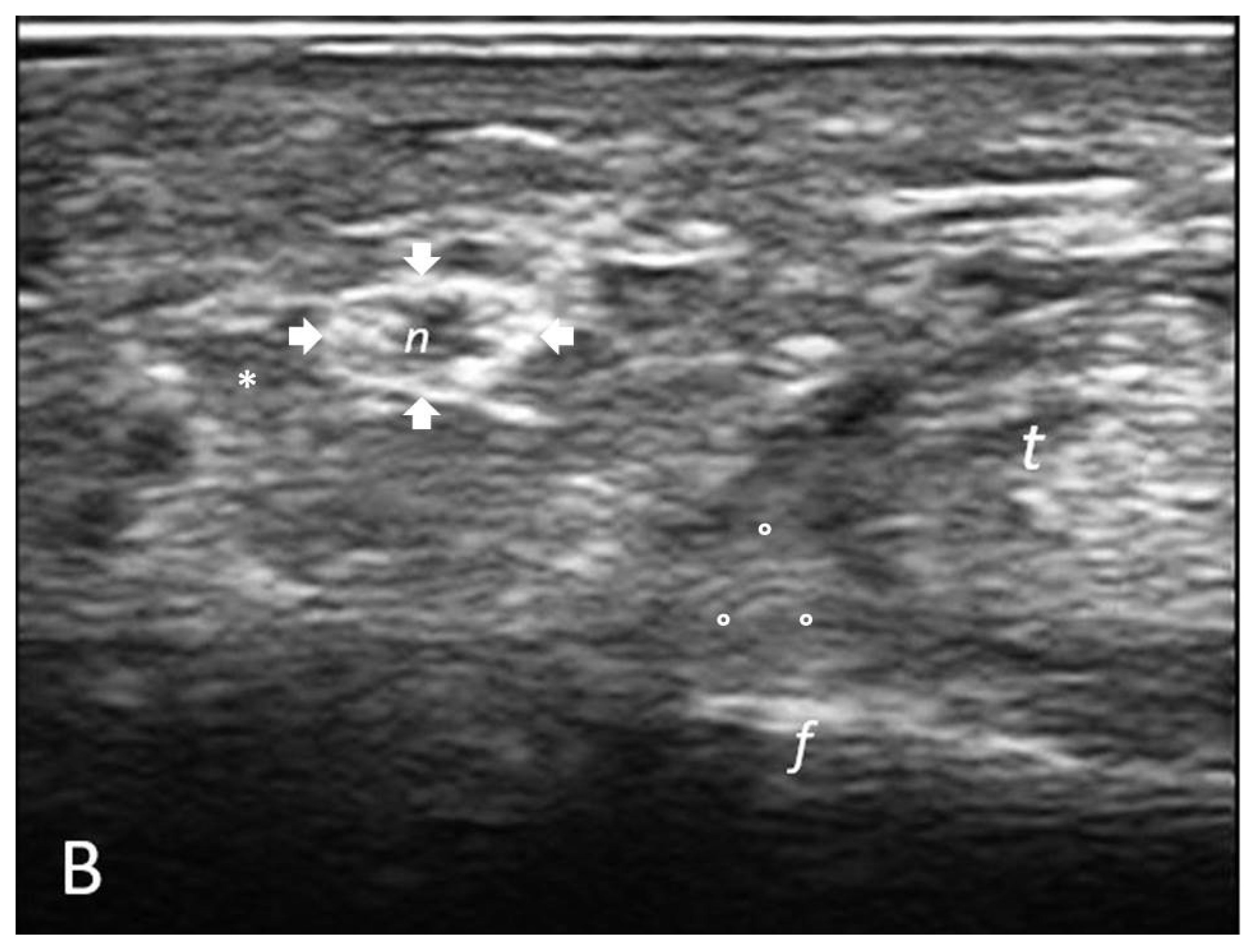
2.3.2. Determination of Cross-Sectional Area (CSA) of Palmar Digital Nerves
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Correlation Analyses
3.3. Multivariate Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smolen, J.S.; Aletaha, D.; McInnes, I.B. Rheumatoid arthritis. Lancet 2016, 388, 2023–2038. [Google Scholar] [CrossRef]
- Koop, S.M.; ten Klooster, P.M.; Vonkeman, H.E.; Steunebrink, L.M.; van de Laar, M.A. Neuropathic-like pain features and cross-sectional associations in rheumatoid arthritis. Arthritis Res. Ther. 2015, 17, 237. [Google Scholar] [CrossRef] [PubMed]
- Rifbjerg-Madsen, S.; Christensen, A.W.; Christensen, R.; Hetland, M.L.; Bliddal, H.; Kristensen, L.E.; Danneskiold-Samsøe, B.; Amris, K. Pain and pain mechanisms in patients with inflammatory arthritis: A Danish nationwide cross-sectional DANBIO registry survey. PLoS ONE 2017, 12, e0180014. [Google Scholar] [CrossRef] [PubMed]
- Salaffi, F.; Di Carlo, M.; Carotti, M.; Sarzi-Puttini, P. The Effect of Neuropathic Pain Symptoms on Remission in Patients with Early Rheumatoid Arthritis. Curr. Rheumatol. Rev. 2019, 15, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Pinho-Ribeiro, F.A.; Verri, W.A., Jr.; Chiu, I.M. Nociceptor Sensory Neuron-Immune Interactions in Pain and Inflammation. Trends Immunol. 2017, 38, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Sarzi-Puttini, P.; Zen, M.; Arru, F.; Giorgi, V.; Choy, E.A. Residual pain in rheumatoid arthritis: Is it a real problem? Autoimmun. Rev. 2023, 22, 103423. [Google Scholar] [CrossRef] [PubMed]
- Carbone, F.; Bonaventura, A.; Liberale, L.; Paolino, S.; Torre, F.; Dallegri, F.; Montecucco, F.; Cutolo, M. Atherosclerosis in Rheumatoid Arthritis: Promoters and Opponents. Clin. Rev. Allergy Immunol. 2020, 58, 1–14. [Google Scholar] [CrossRef]
- Zaottini, F.; Picasso, R.; Pistoia, F.; Sanguinetti, S.; Pansecchi, M.; Tovt, L.; Viglino, U.; Cabona, C.; Garnero, M.; Benedetti, L.; et al. High-resolution ultrasound of peripheral neuropathies in rheumatological patients: An overview of clinical applications and imaging findings. Front. Med. 2022, 9, 984379. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2010, 69, 1580–1588. [Google Scholar] [CrossRef]
- van der Heijde, D.; van der Helm-van Mil, A.H.; Aletaha, D.; Bingham, C.O.; Burmester, G.R.; Dougados, M.; Emery, P.; Felson, D.; Knevel, R.; Kvien, T.K.; et al. EULAR definition of erosive disease in light of the 2010 ACR/EULAR rheumatoid arthritis classification criteria. Ann. Rheum. Dis. 2013, 72, 479–481. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Smolen, J.S. The Simplified Disease Activity Index (SDAI) and Clinical Disease Activity Index (CDAI) to monitor patients in standard clinical care. Best Pract. Res. Clin. Rheumatol. 2007, 21, 663–675. [Google Scholar] [CrossRef]
- Franchignoni, F.; Ferriero, G.; Giordano, A.; Sartorio, F.; Vercelli, S.; Brigatti, E. Psychometric properties of QuickDASH—A classical test theory and Rasch analysis study. Man. Ther. 2011, 16, 177–182. [Google Scholar] [CrossRef]
- Freynhagen, R.; Tölle, T.R.; Gockel, U.; Baron, R. The painDETECT project—Far more than a screening tool on neuropathic pain. Curr. Med. Res. Opin. 2016, 32, 1033–1057. [Google Scholar] [CrossRef]
- Möller, I.; Janta, I.; Backhaus, M.; Ohrndorf, S.; Bong, D.A.; Martinoli, C.; Filippucci, E.; Sconfienza, L.M.; Terslev, L.; Damjanov, N.; et al. The 2017 EULAR standardised procedures for ultrasound imaging in rheumatology. Ann. Rheum. Dis. 2017, 76, 1974–1979. [Google Scholar] [CrossRef]
- Terslev, L.; Naredo, E.; Aegerter, P.; Wakefield, R.J.; Backhaus, M.; Balint, P.; Bruyn, G.A.W.; Iagnocco, A.; Jousse-Joulin, S.; Schmidt, W.A.; et al. Scoring ultrasound synovitis in rheumatoid arthritis: A EULAR-OMERACT ultrasound taskforce—Part 2: Reliability and application to multiple joints of a standardised consensus-based scoring system. RMD Open 2017, 3, e000427. [Google Scholar] [CrossRef] [PubMed]
- Dede, B.T.; Oğuz, M.; Bulut, B.; Bağcıer, F.; Aytekin, E. Carpal tunnel syndrome evaluation with ultrasound in rheumatoid arthritis patients. ARP Rheumatol. 2023, 2, 330–337. [Google Scholar] [PubMed]
- Filippucci, E.; Cipolletta, E.; Mashadi Mirza, R.; Carotti, M.; Giovagnoni, A.; Salaffi, F.; Tardella, M.; Di Matteo, A.; Di Carlo, M. Ultrasound imaging in rheumatoid arthritis. Radiol. Med. 2019, 124, 1087–1100. [Google Scholar] [CrossRef]
- Coraci, D.; Loreti, C.; Fusco, A.; Giovannini, S.; Padua, L. Peripheral Neuropathies Seen by Ultrasound: A Literature Analysis through Lexical Evaluation, Geographical Assessment and Graph Theory. Brain Sci. 2021, 11, 113. [Google Scholar] [CrossRef] [PubMed]
- Telleman, J.A.; Herraets, I.J.; Goedee, H.S.; van Asseldonk, J.T.; Visser, L.H. Ultrasound scanning in the diagnosis of peripheral neuropathies. Pract. Neurol. 2021, 21, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Bandinelli, F.; Kaloudi, O.; Candelieri, A.; Conforti, M.L.; Casale, R.; Cammarata, S.; Grassiri, G.; Miniati, I.; Melchiorre, D.; Matucci-Cerinic, M. Early detection of median nerve syndrome at the carpal tunnel with high-resolution 18 MHz ultrasonography in systemic sclerosis patients. Clin. Exp. Rheumatol. 2010, 28 (Suppl. 62), S15–S18. [Google Scholar]
- Wu, W.T.; Chang, K.V.; Hsu, Y.C.; Tsai, Y.Y.; Mezian, K.; Ricci, V.; Özçakar, L. Ultrasound Imaging and Guidance for Distal Peripheral Nerve Pathologies at the Wrist/Hand. Diagnostics 2023, 13, 1928. [Google Scholar] [CrossRef]
- Padua, L.; Cuccagna, C.; Giovannini, S.; Coraci, D.; Pelosi, L.; Loreti, C.; Bernabei, R.; Hobson-Webb, L.D. Carpal tunnel syndrome: Updated evidence and new questions. Lancet Neurol. 2023, 22, 255–267. [Google Scholar] [CrossRef]
- Smerilli, G.; Di Matteo, A.; Cipolletta, E.; Carloni, S.; Incorvaia, A.; Di Carlo, M.; Grassi, W.; Filippucci, E. Ultrasound assessment of carpal tunnel in rheumatoid arthritis and idiopathic carpal tunnel syndrome. Clin. Rheumatol. 2021, 40, 1085–1092. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, V.; Singh, R.; Wiclaf Chauhan, S.; Tahlan, A.; Ahuja, C.K.; Goel, D.; Pal, L. A clinical, electrophysiological, and pathological study of neuropathy in rheumatoid arthritis. Clin. Rheumatol. 2008, 27, 841–844. [Google Scholar] [CrossRef]
- Créange, A.; Barlovatz-Meimon, G.; Gherardi, R.K. Cytokines and peripheral nerve disorders. Eur. Cytokine Netw. 1997, 8, 145–151. [Google Scholar]
- Bathala, L.; Kumar, P.; Kumar, K.; Visser, L.H. Ultrasonographic cross-sectional area normal values of the ulnar nerve along its course in the arm with electrophysiological correlations in 100 Asian subjects. Muscle Nerve 2013, 47, 673–676. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, P.C.; Chang, K.H.; Wu, Y.R.; Ro, L.S.; Chu, C.C.; Lyu, R.K.; Liao, M.F.; Kuo, H.C. Cross-Sectional Area Reference Values for Sonography of Peripheral Nerves in Taiwanese Adults. Front. Neurol. 2021, 12, 722403. [Google Scholar] [CrossRef]
- McWilliams, D.F.; Walsh, D.A. Pain mechanisms in rheumatoid arthritis. Clin. Exp. Rheumatol. 2017, 35 (Suppl. 107), 94–101. [Google Scholar] [PubMed]
- Di Carlo, M.; Ventura, C.; Cesaroni, P.; Carotti, M.; Giovagnoni, A.; Salaffi, F. Sural Nerve Size in Fibromyalgia Syndrome: Study on Variables Associated with Cross-Sectional Area. Front. Med. 2020, 7, 360. [Google Scholar] [CrossRef]
- Di Carlo, M.; Bianchi, B.; Cipolletta, E.; Farah, S.; Filippucci, E.; Salaffi, F. Imaging of the peripheral nervous system in nociplastic pain: An ultrasound study in patients with fibromyalgia. J. Neuroimaging 2023, 33, 558–565. [Google Scholar] [CrossRef]
- Chang, K.V.; Mezian, K.; Naňka, O.; Wu, W.T.; Lou, Y.M.; Wang, J.C.; Martinoli, C.; Özçakar, L. Ultrasound Imaging for the Cutaneous Nerves of the Extremities and Relevant Entrapment Syndromes: From Anatomy to Clinical Implications. J. Clin. Med. 2018, 7, 457. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Synovitis Grade | Features |
|---|---|
| 0 | Normal joint: absence of synovial hypertrophy regardless of the presence of effusion, absence of power Doppler signal |
| 1 | Mild synovitis: synovial hypertrophy without protrusion from the line connecting the upper bony margins of the metacarpal head and the proximal phalanx, on power Doppler examination up to three individual spots or one confluent spot and two individual spots or two confluent spots |
| 2 | Moderate synovitis: synovial hypertrophy extending beyond the line but with a concave or flat superior surface, power Doppler greater than Grade 1 but with signal involving less than 50% of the region with synovial hypertrophy |
| 3 | Severe synovitis: marked synovial hypertrophy extending above the joint line and with a convex upper margin, power Doppler signal involving more than 50% of the region with synovial hypertrophy |
| Variables | Results |
|---|---|
| Age, years, mean (SD) | 64.1 (12.0) |
| Sex, female, n (%) | 47 (74.6) |
| Body mass index (kg/m2), mean (SD) | 24.6 (4.5) |
| Coexisting osteoarthritis, n (%) | 17 (27.0) |
| Coexisting fibromyalgia, n (%) | 7 (11.1) |
| Disease duration, years, median (IQR) | 8.0 (6.0–16.0) |
| RF presence, n (%) | 48 (76.2) |
| ACPA presence, n (%) | 49 (77.8) |
| Erosive disease, n (%) | 38 (60.3) |
| CDAI, median (IQR) | 9.0 (4.0–18.0) |
| Sum of CSAs, mm2, median (IQR) | 17 (13–19) |
| Number of patients with at least one joint with ultrasound score > 0, n (%) | 29 (46.0) |
| Number of patients with at least one tendon with ultrasound score > 0, n (%) | 5 (7.9) |
| PDQ, median (IQR) | 14.0 (9.0–20.0) |
| QuickDASH, median (IQR) | 47.7 (34.1–65.9) |
| Steroid use, n (%) | 24 (38.1) |
| - Low dose, n (%) | 18 (28.6) |
| - High dose, n (%) | 6 (9.5) |
| cDMARDs use, n (%) | 43 (68.3) |
| - Leflunomide, n (%) | 1 (1.6) |
| - Methotrexate, n (%) | 34 (54.0) |
| - Hydroxychloroquine, n (%) | 14 (22.2) |
| bDMARDs use, n (%) | 43 (68.3) |
| - anti-tumor necrosis factor alpha, n (%) | 20 (31.7) |
| - anti-interleukin 6, n (%) | 7 (11.1) |
| - anti-CD20, n (%) | 7 (11.1) |
| - anti-CTLA4, n (%) | 14 (22.2) |
| Area of Digital Nerves (Sum of CSAs) | CDAI | PDQ | |
|---|---|---|---|
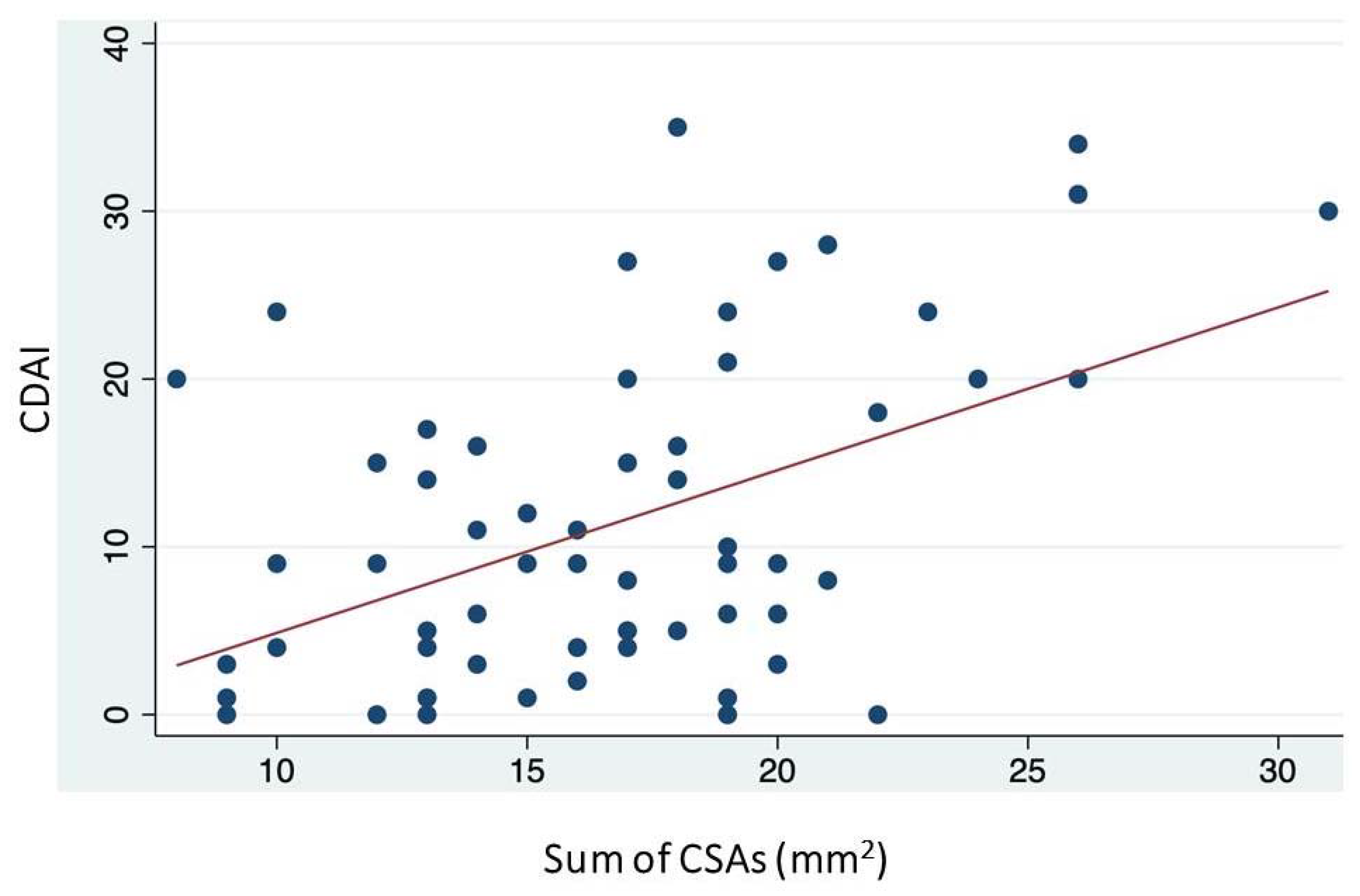
| CDAI | r = 0.387 p = 0.001 | ||
| PDQ | r = −0.049 p = 0.702 | r = 0.312 p = 0.012 | |
| QuickDASH | r = 0.128 p = 0.316 | r = 0.585 p < 0.001 | r = 0.560 p < 0.001 |
| Area of Digital Nerves (Sum of CSAs) | CDAI | Ultrasound Grades 1–3 | Ultrasound Grades 2–3 | |
|---|---|---|---|---|
| CDAI | r = 0.387 p = 0.001 | |||
| Ultrasound Grades 1–3 | r = 0.381 p = 0.002 | r = 0.596 p < 0.001 | ||
| Ultrasound Grades 2–3 | r = 0.290 p = 0.021 | r = 0.308 p = 0.014 | r = 0.596 p < 0.001 | |
| Ultrasound Grade 3 | r = 0.205 p = 0.106 | r = 0.263 p = 0.037 | r = 0.419 p < 0.001 | r = 0.638 p < 0.001 |
| Area of Digital Nerves (Sum of CSAs) | Coefficient | Standard Error | t | p | 95% CI |
|---|---|---|---|---|---|
| CDAI | 0.258 | 0.060 | 4.25 | <0.001 | 0.136–0.381 |
| Disease duration (years) | −0.070 | 0.071 | −0.98 | 0.333 | −0.214–0.074 |
| Age | 0.037 | 0.045 | 0.81 | 0.422 | −0.054–0.128 |
| Sex (male) | 2.892 | 1.266 | 2.28 | 0.026 | 0.351–5.433 |
| BMI | 0.127 | 0.119 | 1.06 | 0.294 | −0.113–0.367 |
| ACPA presence | 0.040 | 1.672 | 0.02 | 0.981 | −3.315–3.395 |
| RF presence | 0.631 | 1.707 | 0.37 | 0.713 | −2.793–4.056 |
| Erosive disease presence | −0.350 | 1.381 | −0.25 | 0.801 | −3.121–2.421 |
| Coexisting fibromyalgia | 1.674 | 1.840 | 0.91 | 0.367 | −2.017–5.367 |
| Coexisting osteoarthritis | 0.020 | 1.260 | 0.02 | 0.987 | −2.510–2.550 |
| constant | 7.913 | 4.401 | 1.80 | 0.078 | −0.917–16.745 |
| Area of Digital Nerves (Sum of CSAs) | Coefficient | Standard Error | t | p | 95% CI |
|---|---|---|---|---|---|
| Ultrasound Grades 1–3 | 1.706 | 0.443 | 3.85 | <0.001 | 0.817–2.596 |
| Disease duration (years) | −0.107 | 0.075 | −1.43 | 0.159 | −0.259–0.043 |
| Age | 0.020 | 0.046 | 0.43 | 0.665 | −0.073–0.114 |
| Sex (male) | 2.733 | 1.294 | 2.11 | 0.040 | 0.135–5.332 |
| BMI | 0.134 | 0.122 | 1.09 | 0.280 | −0.112–0.380 |
| ACPA presence | −2.633 | 1.779 | −1.48 | 0.145 | −6.203–0.936 |
| RF presence | 2.447 | 1.769 | 1.38 | 0.172 | −1.101–5.997 |
| Erosive disease presence | 1.178 | 1.337 | 0.88 | 0.383 | −1.506–3.862 |
| Coexisting fibromyalgia | 2.458 | 1.872 | 1.31 | 0.195 | −1.299–6.216 |
| Coexisting osteoarthritis | −0.541 | 1.289 | −0.42 | 0.676 | −3.128–2.045 |
| constant | 10.328 | 4.461 | 2.32 | 0.025 | 1.376–19.281 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Carlo, M.; Di Battista, J.; Cipolletta, E.; Okano, T.; Chiorrini, R.; Smerilli, G.; Bandinelli, F.; Filippucci, E.; Salaffi, F. Is Active Synovitis of Metacarpophalangeal Joints a Neuropathic Condition in Rheumatoid Arthritis Patients? Results from an Ultrasound Study of Palmar Digital Nerves. J. Clin. Med. 2024, 13, 1599. https://doi.org/10.3390/jcm13061599
Di Carlo M, Di Battista J, Cipolletta E, Okano T, Chiorrini R, Smerilli G, Bandinelli F, Filippucci E, Salaffi F. Is Active Synovitis of Metacarpophalangeal Joints a Neuropathic Condition in Rheumatoid Arthritis Patients? Results from an Ultrasound Study of Palmar Digital Nerves. Journal of Clinical Medicine. 2024; 13(6):1599. https://doi.org/10.3390/jcm13061599
Chicago/Turabian StyleDi Carlo, Marco, Jacopo Di Battista, Edoardo Cipolletta, Tadashi Okano, Riccardo Chiorrini, Gianluca Smerilli, Francesca Bandinelli, Emilio Filippucci, and Fausto Salaffi. 2024. "Is Active Synovitis of Metacarpophalangeal Joints a Neuropathic Condition in Rheumatoid Arthritis Patients? Results from an Ultrasound Study of Palmar Digital Nerves" Journal of Clinical Medicine 13, no. 6: 1599. https://doi.org/10.3390/jcm13061599