
Adverse Events and Clinical Correlates in Asian Patients with Atrial Fibrillation and Diabetes Mellitus: A Report from Asia Pacific Heart Rhythm Society Atrial Fibrillation Registry
 , , ,
, , ,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Scores
2.2. Rhythm Control Definitions
2.3. Study Outcomes
2.4. Statistical Analyses
3. Results
3.1. Clinical Characteristics
3.2. Antithrombotic Management
3.3. Rhythm Control
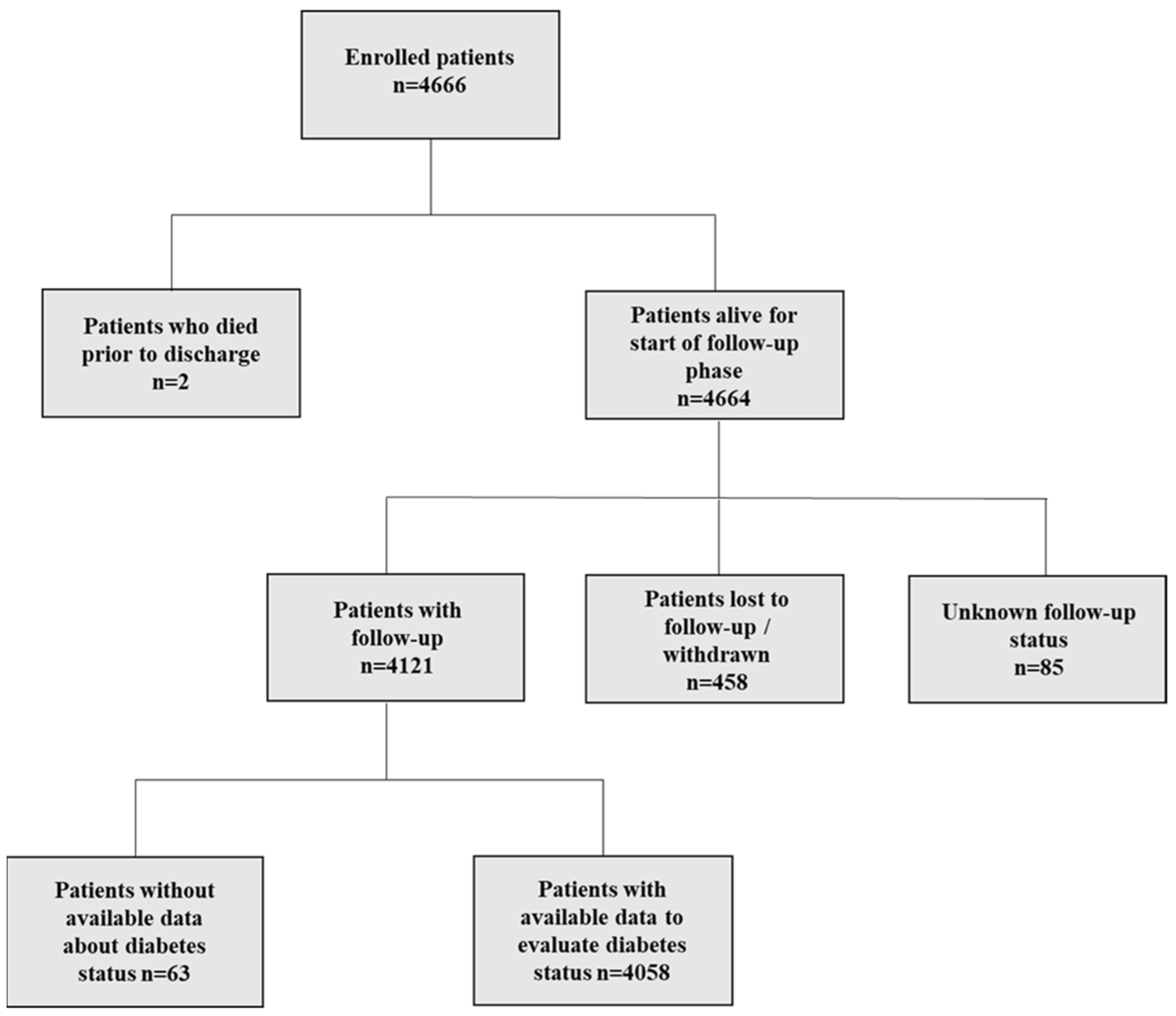
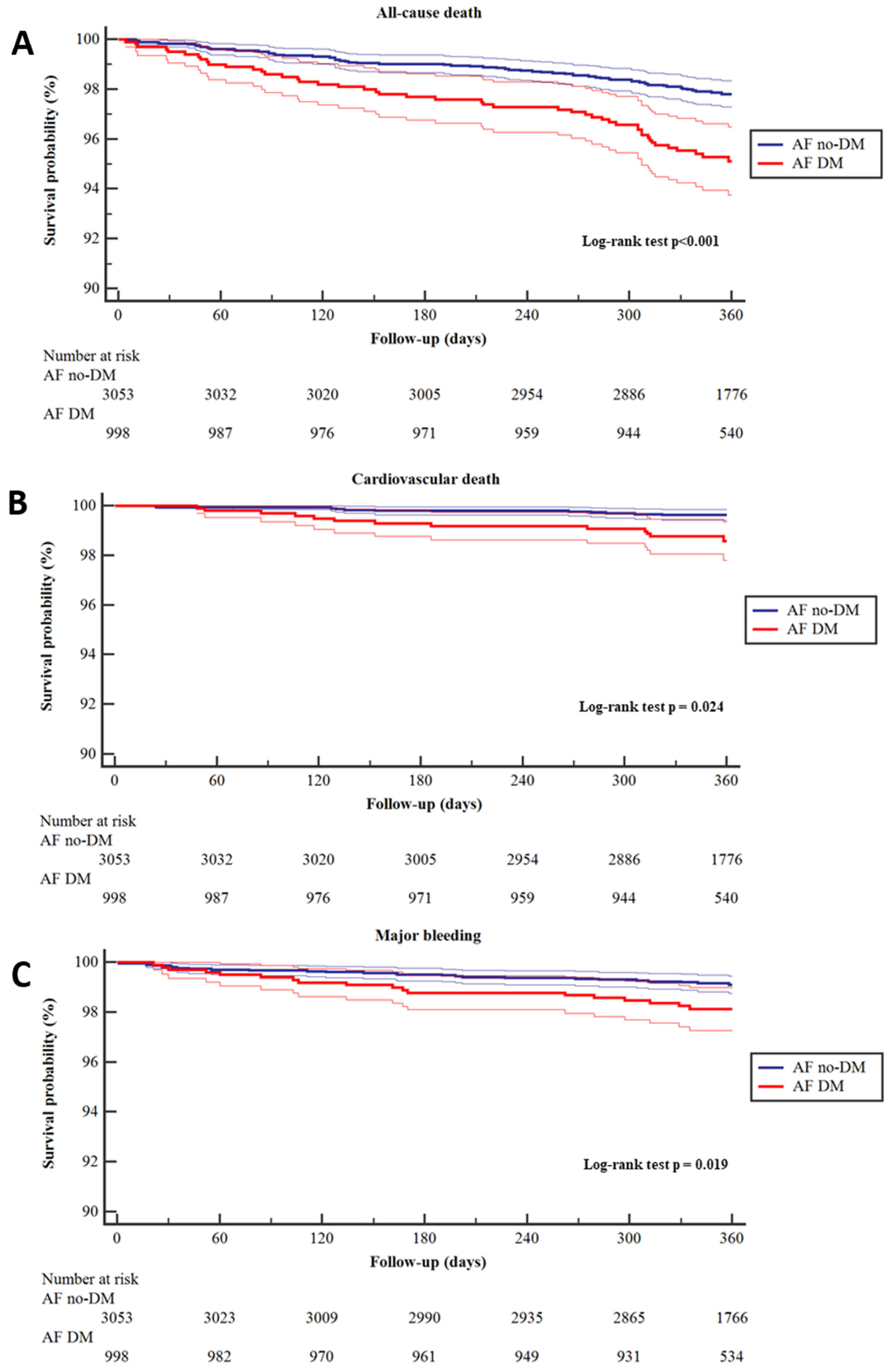
3.4. Follow-Up
3.5. Sensitivity Analysis
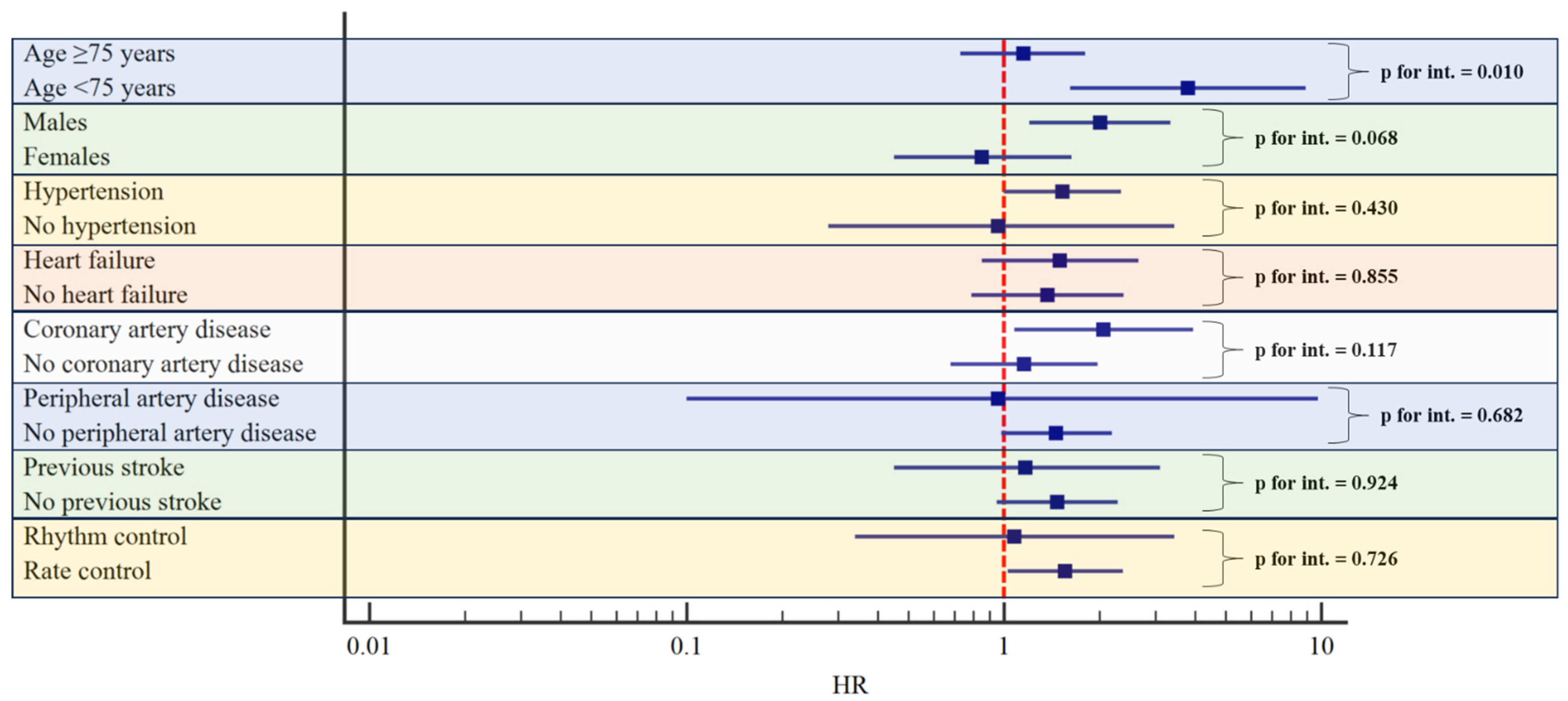
3.6. Subgroup Analyses
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lippi, G.; Sanchis-Gomar, F.; Cervellin, G. Global epidemiology of atrial fibrillation: An increasing epidemic and public health challenge. Int. J. Stroke 2021, 16, 217–221. [Google Scholar] [CrossRef]
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Al Kaabi, J. Epidemiology of Type 2 Diabetes—Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2020, 10, 107–111. [Google Scholar] [CrossRef]
- Movahed, M.R.; Hashemzadeh, M.; Jamal, M.M. Diabetes mellitus is a strong, independent risk for atrial fibrillation and flutter in addition to other cardiovascular disease. Int. J. Cardiol. 2005, 105, 315–318. [Google Scholar] [CrossRef]
- Chao, T.F.; Liu, C.J.; Tuan, T.C.; Chen, T.J.; Hsieh, M.H.; Lip, G.Y.; Chen, S.A. Lifetime Risks, Projected Numbers, and Adverse Outcomes in Asian Patients With Atrial Fibrillation: A Report From the Taiwan Nationwide AF Cohort Study. Chest 2018, 153, 453–466. [Google Scholar] [CrossRef]
- Kim, D.; Yang, P.-S.; Jang, E.; Yu, H.T.; Kim, T.-H.; Uhm, J.-S.; Kim, J.-Y.; Pak, H.-N.; Lee, M.-H.; Joung, B.; et al. 10-year nationwide trends of the incidence, prevalence, and adverse outcomes of non-valvular atrial fibrillation nationwide health insurance data covering the entire Korean population. Am. Heart J. 2018, 202, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, A.; Ma, R.C.; Snehalatha, C. Diabetes in Asia. Lancet 2010, 375, 408–418. [Google Scholar] [CrossRef]
- Tuomi, T.; Santoro, N.; Caprio, S.; Cai, M.; Weng, J.; Groop, L. The many faces of diabetes: A disease with increasing heterogeneity. Lancet 2014, 383, 1084–1094. [Google Scholar] [CrossRef]
- Ma, R.C.; Chan, J.C. Type 2 diabetes in East Asians: Similarities and differences with populations in Europe and the United States. Ann. N. Y. Acad. Sci. 2013, 1281, 64–91. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.; Laroche, C.; Ioachim, P.M.; Rasmussen, L.H.; Vitali-Serdoz, L.; Petrescu, L.; Darabantiu, D.; Crijns, H.J.; Kirchhof, P.; Vardas, P.; et al. Prognosis and treatment of atrial fibrillation patients by European cardiologists: One year follow-up of the EURObservational Research Programme-Atrial Fibrillation General Registry Pilot Phase (EORP-AF Pilot registry). Eur. Heart J. 2014, 35, 3365–3376. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; de Vos, C.B.; Crijns, H.J.; Lip, G.Y. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: The Euro Heart Survey. Chest 2010, 138, 1093–1100. [Google Scholar] [CrossRef]
- Wynn, G.J.; Todd, D.M.; Webber, M.; Bonnett, L.; McShane, J.; Kirchhof, P.; Gupta, D. The European Heart Rhythm Association symptom classification for atrial fibrillation: Validation and improvement through a simple modification. Europace 2014, 16, 965–972. [Google Scholar] [CrossRef]
- Bucci, T.; Shantsila, A.; Romiti, G.F.; Teo, W.-S.; Park, H.-W.; Shimizu, W.; Mei, D.A.; Tse, H.-F.; Proietti, M.; Chao, T.-F.; et al. Sex-related differences in presentation, treatment, and outcomes of Asian patients with atrial fibrillation: A report from the prospective APHRS-AF Registry. Sci. Rep. 2023, 13, 18375. [Google Scholar] [CrossRef]
- Schulman, S.; Kearon, C. Subcommittee on Control of Anticoagulation of the S, Standardization Committee of the International Society on T, Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Ding, W.Y.; Kotalczyk, A.; Boriani, G.; Marin, F.; Blomström-Lundqvist, C.; Potpara, T.S.; Fauchier, L.; Lip, G.; Tavazzi, L.; Maggioni, A.; et al. Impact of diabetes on the management and outcomes in atrial fibrillation: An analysis from the ESC-EHRA EORP-AF Long-Term General Registry. Eur. J. Intern. Med. 2022, 103, 41–49. [Google Scholar] [CrossRef]
- Xu, J.; Sun, Y.; Gong, D.; Fan, Y. Impact of preexisting diabetes mellitus on cardiovascular and all-cause mortality in patients with atrial fibrillation: A meta-analysis. Front. Endocrinol. 2022, 13, 921159. [Google Scholar] [CrossRef] [PubMed]
- Fumagalli, S.; A Said, S.; Laroche, C.; Gabbai, D.; Boni, S.; Marchionni, N.; Boriani, G.; Maggioni, A.P.; Musialik-Lydka, A.; Sokal, A.; et al. Management and prognosis of atrial fibrillation in diabetic patients: An EORP-AF General Pilot Registry report. Eur. Heart J. Cardiovasc. Pharmacother. 2018, 4, 172–179. [Google Scholar] [CrossRef]
- Seyed Ahmadi, S.; Svensson, A.M.; Pivodic, A.; Rosengren, A.; Lind, M. Risk of atrial fibrillation in persons with type 2 diabetes and the excess risk in relation to glycaemic control and renal function: A Swedish cohort study. Cardiovasc. Diabetol. 2020, 19, 9. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.; John Mitchell, A.R.; Ashmore, L.; Holland, C. Quality of life among people with atrial fibrillation with and without diabetes: A comparison study. Br. J. Cardiol. 2021, 28, 42. [Google Scholar]
- Wyse, D.G.; Waldo, A.L.; DiMarco, J.P.; Domanski, M.J.; Rosenberg, Y.; Schron, E.B.; Kellen, J.C.; Greene, H.L.; Mickel, M.C.; E Dalquist, J.; et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. N. Engl. J. Med. 2002, 347, 1825–1833. [Google Scholar]
- Van Gelder, I.C.; Hagens, V.E.; Bosker, H.A.; Kingma, J.H.; Kamp, O.; Kingma, T.; Said, S.A.; Darmanata, J.I.; Timmermans, A.J.; Tijssen, J.G.; et al. A comparison of rate control and rhythm control in patients with recurrent persistent atrial fibrillation. N. Engl. J. Med. 2002, 347, 1834–1840. [Google Scholar] [CrossRef]
- Opolski, G.; Torbicki, A.; Kosior, D.A.; Szulc, M.; Wozakowska-Kapłon, B.; Kołodziej, P.; Achremczyk, P. Rate control vs rhythm control in patients with nonvalvular persistent atrial fibrillation: The results of the Polish How to Treat Chronic Atrial Fibrillation (HOT CAFE) Study. Chest 2004, 126, 476–486. [Google Scholar] [CrossRef]
- Roy, D.; Talajic, M.; Nattel, S.; Wyse, D.G.; Dorian, P.; Lee, K.L.; Bourassa, M.G.; Arnold, J.M.O.; Buxton, A.E.; Camm, A.J.; et al. Rhythm control versus rate control for atrial fibrillation and heart failure. N. Engl. J. Med. 2008, 358, 2667–2677. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, J.Ö.; Miketic, S.; Windeler, J.Ü.; Cuneo, A.; Haun, S.; Micus, S.; Walter, S.; Tebbe, U.; STAF investigators. Randomized trial of rate-control versus rhythm-control in persistent atrial fibrillation: The Strategies of Treatment of Atrial Fibrillation (STAF) study. J. Am. Coll. Cardiol. 2003, 41, 1690–1696. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Camm, A.J.; Goette, A.; Brandes, A.; Eckardt, L.; Elvan, A.; Fetsch, T.; van Gelder, I.C.; Haase, D.; Haegeli, L.M.; et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation. N. Engl. J. Med. 2020, 383, 1305–1316. [Google Scholar] [CrossRef]
- Chirinos, J.A.; Sardana, M.; Ansari, B.; Satija, V.; Kuriakose, D.; Edelstein, I.; Oldland, G.; Miller, R.; Gaddam, S.; Lee, J.; et al. Left Atrial Phasic Function by Cardiac Magnetic Resonance Feature Tracking Is a Strong Predictor of Incident Cardiovascular Events. Circ. Cardiovasc. Imaging 2018, 11, e007512. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESCGuidelines for the diagnosis management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the, E.S.C. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [PubMed]
- Chao, T.-F.; Joung, B.; Takahashi, Y.; Lim, T.W.; Choi, E.-K.; Chan, Y.-H.; Guo, Y.; Sriratanasathavorn, C.; Oh, S.; Okumura, K.; et al. 2021 Focused Update Consensus Guidelines of the Asia Pacific Heart Rhythm Society on Stroke Prevention in Atrial Fibrillation: Executive Summary. Thromb. Haemost. 2022, 122, 20–47. [Google Scholar] [CrossRef] [PubMed]
- Romiti, G.F.; Pastori, D.; Rivera-Caravaca, J.M.; Ding, W.Y.; Gue, Y.X.; Menichelli, D.; Gumprecht, J.; Kozieł, M.; Yang, P.S.; Guo, Y.; et al. Adherence to the ‘Atrial Fibrillation Better Care’ Pathway in Patients with Atrial Fibrillation: Impact on Clinical Outcomes-A Systematic Review and Meta-Analysis of 285,000 Patients. Thromb. Haemost. 2022, 122, 406–414. [Google Scholar] [CrossRef]
- Guo, Y.; Lane, D.A.; Zhang, H.; Wang, H.; Zhang, W.; Wen, J.; Xing, Y.; Wu, F.; Xia, Y.; Liu, T.; et al. Mobile Health Technology to Improve Care for Patients With Atrial Fibrillation. J. Am. Coll. Cardiol. 2020, 75, 1523–1534. [Google Scholar] [CrossRef]
- Romiti, G.F.; Proietti, M.; Bonini, N.; Ding, W.Y.; Boriani, G.; Huisman, M.V.; Lip, G.Y. Adherence to the Atrial Fibrillation Better Care (ABC) pathway and the risk of major outcomes in patients with atrial fibrillation: A post-hoc analysis from the prospective GLORIA-AF Registry. EClinicalMedicine 2023, 55, 101757. [Google Scholar] [CrossRef]
- Bucci, T.; Proietti, M.; Shantsila, A.; Romiti, G.F.; Teo, W.-S.; Park, H.-W.; Shimizu, W.; Tse, H.-F.; Lip, G.Y.; Chao, T.-F. Integrated Care for Atrial Fibrillation Using the ABC Pathway in the Prospective APHRS-AF Registry. JACC Asia 2023, 3, 580–591. [Google Scholar] [CrossRef]
- Domek, M.; Gumprecht, J.; Li, Y.; Proietti, M.; Rashed, W.; Al Qudaimi, A.; Gumprecht, J.; Zubaid, M.; Lip, G.Y.H. Compliance of atrial fibrillation treatment with the ABC pathway in patients with concomitant diabetes mellitus in the Middle East based on the Gulf SAFE registry. Eur. J. Clin. Investig. 2021, 51, e13385. [Google Scholar] [CrossRef]
- Guo, Y.; Corica, B.; Romiti, G.F.; Proietti, M.; Zhang, H.; Lip, G.Y.H.; mAF-App II Trial Investigators. Mobile health technology integrated care in atrial fibrillation patients with diabetes mellitus in China: A subgroup analysis of the mAFA-II cluster randomized clinical trial. Eur. J. Clin. Investig. 2023, 53, e14031. [Google Scholar] [CrossRef]
- Domek, M.; Li, Y.G.; Gumprecht, J.; Asaad, N.; Rashed, W.; Alsheikh-Ali, A.; Nabrdalik, K.; Gumprecht, J.; Zubaid, M.; Lip, G.Y. One-year all-cause mortality risk among atrial fibrillation patients in Middle East with and without diabetes: The Gulf SAFE registry. Int. J. Cardiol. 2020, 302, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Papazoglou, A.S.; Kartas, A.; Samaras, A.; Vouloagkas, I.; Vrana, E.; Moysidis, D.V.; Akrivos, E.; Kotzampasis, G.; Baroutidou, A.; Papanastasiou, A.; et al. Prognostic significance of diabetes mellitus in patients with atrial fibrillation. Cardiovasc. Diabetol. 2021, 20, 40. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, T.A.; Lasker, S.S. Complications and cardiovascular risk factors in South Asians and Europeans with early-onset type 2 diabetes. QJM 2002, 95, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, A.J.; Laing, S.P.; Dos Santos Silva, I.; Slater, S.D.; Burden, A.C.; Botha, J.L.; Waugh, N.R.; Morris, A.D.; Gatling, W.; Bingley, P.J.; et al. Mortality of South Asian patients with insulin-treated diabetes mellitus in the United Kingdom: A cohort study. Diabet. Med. 2004, 21, 845–851. [Google Scholar] [CrossRef]
- Mather, H.M.; Chaturvedi, N.; Fuller, J.H. Mortality and morbidity from diabetes in South Asians and Europeans: 11-year follow-up of the Southall Diabetes Survey, London, UK. Diabet. Med. 1998, 15, 53–59. [Google Scholar] [CrossRef]
- Peacock, W.F.; Tamayo, S.; Sicignano, N.; Hopf, K.P.; Yuan, Z.; Patel, M. Comparison of the Incidence of Major Bleeding with Rivaroxaban Use among Nonvalvular Atrial Fibrillation Patients with Versus Without Diabetes Mellitus. Am. J. Cardiol. 2017, 119, 753–759. [Google Scholar] [CrossRef]
- Karayiannides, S.; Lundman, P.; Friberg, L.; Norhammar, A. High overall cardiovascular risk and mortality in patients with atrial fibrillation and diabetes: A nationwide report. Diabetes Vasc. Dis. Res. 2018, 15, 31–38. [Google Scholar] [CrossRef]
- Kosciuszek, N.D.; Kalta, D.; Singh, M.; Savinova, O.V. Vitamin K antagonists and cardiovascular calcification: A systematic review and meta-analysis. Front. Cardiovasc. Med. 2022, 9, 938567. [Google Scholar] [CrossRef]
- Bucci, T.; Shantsila, A.; Romiti, G.F.; Teo, W.-S.; Chao, T.-F.; Shimizu, W.; Boriani, G.; Tse, H.-F.; Krittayaphong, R.; Lip, G.Y. External Validation of COOL-AF Scores in the Asian Pacific Heart Rhythm Society Atrial Fibrillation Registry. JACC Asia 2024, 4, 59–69. [Google Scholar] [CrossRef]
- Simoni, A.H.; Bucci, T.; Romiti, G.F.; Frydenlund, J.; Johnsen, S.P.; Abdul-Rahim, A.H.; Lip, G.Y.H. Social determinants of health and clinical outcomes among patients with atrial fibrillation. Evidence from a global federated health research network. QJM 2023, hcad275. [Google Scholar] [CrossRef]
- van Niel, J.; Geelhoed-Duijvestijn, P.; Numans, M.E.; Kharagjitsing, A.V.; Vos, R.C. Type 2 diabetes in South Asians compared to Europeans: Higher risk and earlier development of major cardiovascular events irrespective of the presence and degree of retinopathy. Results from The HinDu The Hague Diabetes Study. Endocrinol. Diabetes Metab. 2021, 4, e00242. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.J.; Aroda, V.R.; Collins, B.S.; Gabbay, R.A.; Green, J.; Maruthur, N.M.; Rosas, S.E.; Del Prato, S.; Mathieu, C.; Mingrone, G.; et al. Management of Hyperglycemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2022, 45, 2753–2786. [Google Scholar] [CrossRef] [PubMed]
- Azzopardi, R.; Nicholls, S.J.; Nerlekar, N.; Scherer, D.J.; Chandramouli, C.; Lam, C.S.; Muthalaly, R.; Tan, S.; Wong, C.X.; Chew, D.P.; et al. Asia-Pacific Investigators and Asian Enrollment in Cardiometabolic Trials. JACC Asia 2023, 3, 724–735. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No Diabetes (n = 3059) | Diabetes (n = 999) | p-Value | |
|---|---|---|---|
| Age (years), mean ± SD | 67.6 ± 12.1 | 71.4 ± 10.6 | <0.001 |
| Women, n (%) | 1031 (33.7) | 364 (36.4) | 0.114 |
| Medical examination, mean ± SD | |||
| Heart rate (bpm) | 76.3 ± 16.3 | 77.5 ± 16.3 | 0.057 |
| Systolic blood pressure (mmHg) | 127.8 ± 18.4 | 132.6 ± 18.7 | <0.001 |
| Dyastolic blood pressure (mmHg) | 74.7 ± 12.3 | 73.6 ± 12.5 | 0.010 |
| BMI (kg/m2) | 24.6 ± 4.04 | 26.2 ± 4.5 | <0.001 |
| Comorbidities, n (%) | |||
| Hypertension | 1684 (55.4) | 795 (79.9) | <0.001 |
| Dyslipidaemia | 985 (32.5) | 560 (56.7) | <0.001 |
| Heart Failure | 593 (19.6) | 255 (26.0) | <0.001 |
| Coronary artery disease | 499 (16.6) | 282 (28.8) | <0.001 |
| Ischaemic stroke/transient ischemic attack | 285 (9.4) | 106 (10.7) | 0.223 |
| Haemorrhagic stroke | 44 (1.4) | 26 (2.6) | 0.014 |
| Haemorrhagic event | 213 (7.0) | 92 (9.3) | 0.019 |
| Chronic Kidney disease | 173 (5.7) | 135 (13.5) | <0.001 |
| Chronic obstructive pulmonary disease | 84 (2.8) | 28 (2.8) | 0.924 |
| Sleep apnoea | 94 (3.1) | 36 (3.6) | 0.408 |
| Peripheral artery disease | 31 (1.0) | 21 (2.1) | 0.008 |
| Cancer | 66 (2.2) | 29 (2.9) | 0.176 |
| Liver disease | 113 (3.7) | 70 (7.0) | <0.001 |
| Dementia | 40 (1.3) | 32 (3.2) | <0.001 |
| Current smoking | 245 (8.0) | 106 (10.6) | 0.011 |
| Medications, n (%) | |||
| ACE inhibitor | 348 (11.4) | 188 (18.9) | <0.001 |
| Aldosterone blocker | 192 (6.3) | 73 (7.3) | 0.507 |
| ARB | 727 (23.9) | 337 (33.8) | <0.001 |
| Beta-blocker | 1482 (48.7) | 565 (56.8) | <0.001 |
| CCB | 699 (22.9) | 245 (24.6) | 0.281 |
| CCB-non DHP | 413 (13.5) | 146 (14.6) | 0.658 |
| Digoxin | 333 (10.9) | 121 (12.1) | 0.284 |
| Diuretic | 675 (22.1) | 219 (22.0) | 0.936 |
| Statin | 983 (32.3) | 550 (55.4) | <0.001 |
| AF classification, n (%) | |||
| First detected | 208 (6.8) | 84 (8.4) | |
| Paroxysmal | 1333 (43.7) | 371 (37.2) | |
| Persistent | 745 (24.4) | 229 (23.0) | <0.001 |
| Long-standing persistent | 279 (9.1) | 103 (10.3) | |
| Permanent | 485 (15.9) | 209 (21.0) | |
| EHRA classification, n (%) | |||
| EHRA I (no symptoms) | 1885 (61.6) | 712 (71.3) | |
| EHRA II (mild symptoms) | 962 (31.4) | 239 (23.9) | |
| EHRA III (severe symptoms) | 186 (6.1) | 45 (4.5) | <0.001 |
| EHRA IV (disabling symptoms) | 26 (0.8) | 3 (0.3) | |
| Symptoms, n (%) | |||
| Palpitations | 765 (25.0) | 159 (15.9) | <0.001 |
| Dyspnoea | 343 (11.2) | 92 (9.2) | 0.076 |
| Fatigue | 119 (3.9) | 42 (4.2) | 0.659 |
| Non-wellbeing | 58 (1.9) | 14 (1.4) | 0.304 |
| Dizziness | 225 (7.4) | 66 (6.6) | 0.426 |
| Syncope | 55 (1.8) | 7 (0.7) | 0.014 |
| Chest pain | 180 (5.9) | 62 (6.2) | 0.709 |
| Fear/anxiety | 60 (2.0) | 9 (0.9) | 0.024 |
| EuroQoL, mean ± SD | |||
| Mobility | 1.30 ± 0.67 | 1.45 ± 0.84 | <0.001 |
| Self-care | 1.14 ± 0.52 | 1.24 ± 0.72 | <0.001 |
| Usual Activities | 1.24 ± 0.61 | 1.33 ± 0.80 | <0.002 |
| Pain/Discomfort | 1.41 ± 0.67 | 1.44 ± 0.68 | 0.319 |
| Anxiety/Depression | 1.38 ± 0.68 | 1.32 ± 0.61 | 0.018 |
| Thrombotic and hemorrhagic risk | |||
| CHA2DS2-VASc, mean ± SD | 2.3 ± 1.6 | 4 ± 1.5 | <0.001 |
| CHA2DS2-VASc ≥ 2, n (%) | 2000 (65.4) | 968 (96.9) | <0.001 |
| HAS-BLED, mean ± SD | 1.3 ± 1.0 | 1.7 ± 1.1 | <0.001 |
| HAS-BLED ≥ 3, n (%) | 353 (11.5) | 206 (20.6) | <0.001 |
| Antithrombotic treatment, n (%) | |||
| Any antiplatelet | 427 (14.0) | 185 (18.5) | <0.001 |
| Any anticoagulant | 2494 (81.5) | 855 (85.5) | 0.003 |
| Any anticoagulant–any antiplatelet | 157 (5.1) | 97 (9.7) | <0.001 |
| Vitamin K antagonist | 578 (23.2) | 241 (28.2) | 0.003 |
| NOACs | 1916 (76.8) | 614 (71.8) | |
| Apixaban | 558 (18.2) | 197 (19.7) | 0.297 |
| Dabigatran | 354 (11.4) | 132 (13.2) | 0.166 |
| Edoxaban | 326 (10.7) | 69 (6.9) | 0.001 |
| Rivaroxaban | 678 (22.2) | 216 (21.6) | 0.719 |
| Reasons for not using any OAC | |||
| No indication (low risk), n (%) | 276 (48.8) | 40 (27.8) | <0.001 |
| Unwilling to take any OAC, n (%) | 82 (14.5) | 32 (22.2) | 0.025 |
| Prior bleeding, n (%) | 20 (3.5) | 11 (7.6) | 0.032 |
| OAC not considered adequate by physician despite stroke risk, n (%) | 5 (0.9) | 5 (3.5) | 0.190 |
| Recent/planned surgery/intervention, n (%) | 19 (3.4) | 9 (6.3) | 0.112 |
| Active peptic ulcer, n (%) | 4 (0.7) | 1 (0.7) | 0.986 |
| Anemia, n (%) | 22 (3.9) | 14 (9.7) | 0.004 |
| Thrombocytopenia, n (%) | 4 (0.7) | 0 (0.0) | 0.311 |
| Renal dysfunction, n (%) | 12 (2.1) | 13 (9.0) | <0.001 |
| Liver disease, n (%) | 2 (0.4) | 1 (0.7) | 0.574 |
| Malignancy, n (%) | 8 (1.4) | 2 (1.4) | 0.980 |
| Alcohol or drug abuse or psychosocial issues, n (%) | 2 (0.4) | 0 (0.0) | 0.475 |
| Frequent falls, n (%) | 6 (1.1) | 5 (3.5) | 0.037 |
| Dementia, n (%) | 2 (0.4) | 0 (0.0) | 0.475 |
| Recent hemorrhagic stroke, n (%) | 1 (0.2) | 3 (2.1) | 0.006 |
| Intolerance/allergy, n (%) | 3 (0.5) | 0 (0.0) | 0.381 |
| Other, n (%) | 63 (11.2) | 16 (11.1) | 0.989 |
| Rhythm control strategies | |||
| Antiarrhythmics, n (%) | 701 (23.1) | 215 (21.6) | 0.319 |
| Amiodarone, n (%) | 238 (7.8) | 79 (7.9) | 0.904 |
| Dronedarone, n (%) | 71 (2.3) | 29 (2.9) | 0.304 |
| Flecainide, n (%) | 146 (4.8) | 33 (3.3) | 0.049 |
| Propafenone, n (%) | 215 (7.0) | 72 (7.2) | 0.854 |
| Sotalol, n (%) | 56 (1.8) | 15 (1.5) | 0.489 |
| Disopyramide, n (%) | 4 (0.1) | 2 (0.2) | 0.124 |
| Quinidine, n (%) | 1 (0.0) | 0 (0.0) | 0.567 |
| Interventional procedures, n (%) | 673 (22.0) | 187 (18.7) | 0.028 |
| Electrical cardioversion, n (%) | 135 (4.4) | 41 (4.1) | 0.677 |
| Pharmacological cardioversion, n (%) | 157 (5.1) | 57 (5.7) | 0.481 |
| Catheter ablation, n (%) | 477 (15.6) | 122 (12.2) | 0.009 |
| No Diabetes (n = 3059) Number of Events (Incidence/100 Persons/Year) | Diabetes (n = 999) Number of Events (Incidence/100 Persons/Year) | p-Value | Univariable Analysis HR (95% CI) | Multivariable Analysis * HR (95% CI) | Sensitivity Analysis Multivariable Model 1 HR (95% CI) | Sensitivity Analysis Multivariable Model 2 HR (95% CI) | |
|---|---|---|---|---|---|---|---|
| All–cause death | 69 (2.3) | 49 (5.0) | <0.001 | 2.02 (1.53–3.18) | 1.48 (1.00–2.19) | 1.33 (0.88–2.00) | 1.40 (0.87–2.26) |
| CV death | 13 (0.4) | 13 (1.3) | 0.023 | 3.10 (1.44–6.69) | 2.33 (1.01–5.40) | 2.38 (1.02–5.52) | 2.61 (1.05–6.51) |
| ACS/PCI | 29 (1.0) | 12 (1.2) | 0.465 | 1.31 (0.67–2.56) | 0.95 (0.47–1.92) | 0.99 (0.48–2.01) | 0.73 (0.30–1.77) |
| Thromboembolic event | 19 (0.6) | 8 (0.8) | 0.521 | 1.39 (0.61–3.19) | 1.42 (0.60–3.37) | 1.43 (0.59–3.44) | 1.36 (0.50–3.73) |
| New or worsening HF | 68 (2.3) | 28 (2.9) | 0.275 | 1.28 (0.83–1.99) | 0.87 (0.53–1.41) | 0.87 (0.53–1.41) | 0.82 (0.47–1.42) |
| Major bleeding | 28 (1.0) | 18 (1.9) | 0.019 | 1.99 (1.10–3.60) | 1.91 (1.01–3.60) | 1.90 (1.01–3.58) | 2.08 (1.09–3.99) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bucci, T.; Nabrdalik, K.; Shantsila, A.; Romiti, G.F.; Teo, W.-S.; Park, H.-W.; Shimizu, W.; Tse, H.-F.; Proietti, M.; Chao, T.-F.; et al. Adverse Events and Clinical Correlates in Asian Patients with Atrial Fibrillation and Diabetes Mellitus: A Report from Asia Pacific Heart Rhythm Society Atrial Fibrillation Registry. J. Clin. Med. 2024, 13, 1274. https://doi.org/10.3390/jcm13051274
Bucci T, Nabrdalik K, Shantsila A, Romiti GF, Teo W-S, Park H-W, Shimizu W, Tse H-F, Proietti M, Chao T-F, et al. Adverse Events and Clinical Correlates in Asian Patients with Atrial Fibrillation and Diabetes Mellitus: A Report from Asia Pacific Heart Rhythm Society Atrial Fibrillation Registry. Journal of Clinical Medicine. 2024; 13(5):1274. https://doi.org/10.3390/jcm13051274
Chicago/Turabian StyleBucci, Tommaso, Katarzyna Nabrdalik, Alena Shantsila, Giulio Francesco Romiti, Wee-Siong Teo, Hyung-Wook Park, Wataru Shimizu, Hung-Fat Tse, Marco Proietti, Tze-Fan Chao, and et al. 2024. "Adverse Events and Clinical Correlates in Asian Patients with Atrial Fibrillation and Diabetes Mellitus: A Report from Asia Pacific Heart Rhythm Society Atrial Fibrillation Registry" Journal of Clinical Medicine 13, no. 5: 1274. https://doi.org/10.3390/jcm13051274