
Optimizing Care Delivery in Patients with Chronic Kidney Disease in the United States: Proceedings of a Multidisciplinary Roundtable Discussion and Literature Review
 ,
, 
Abstract
:1. Introduction
1.1. Epidemiology of CKD
1.2. Risk Factors for CKD
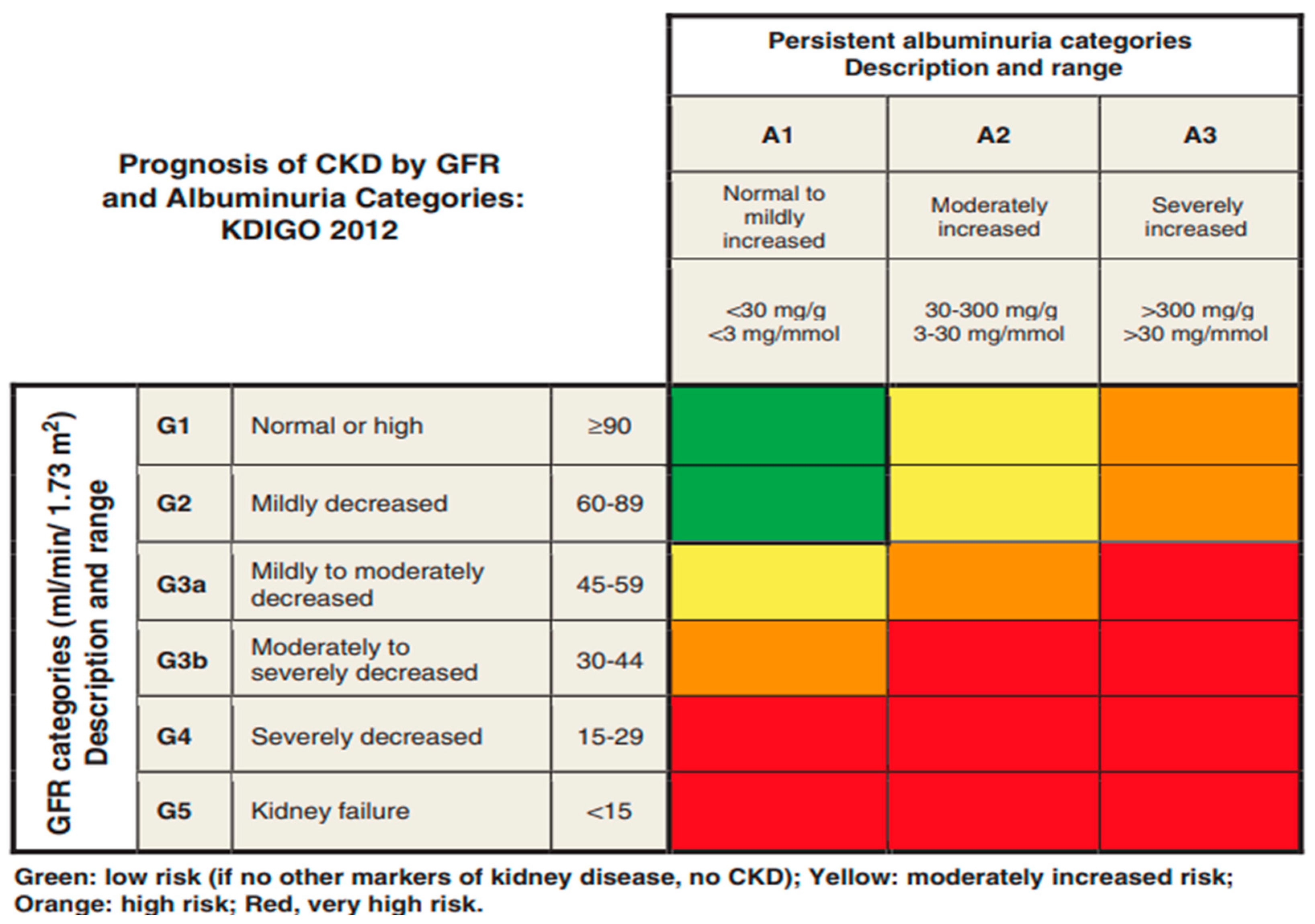
1.3. Staging of CKD
1.4. Economic Implications
1.5. Clinical Guidelines and Societal Work
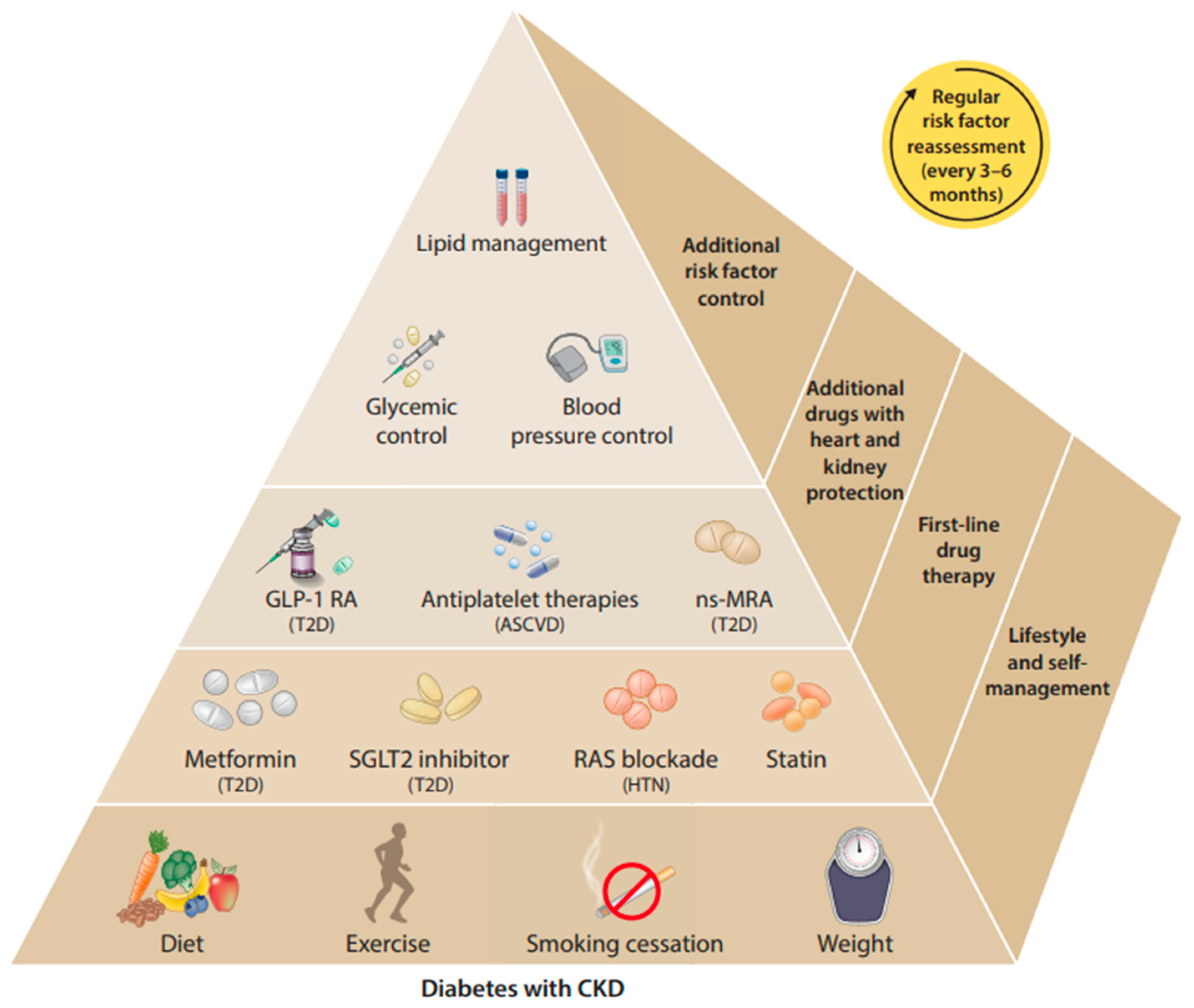
1.6. Treatment Recommendations
1.7. Limitations of Guidelines
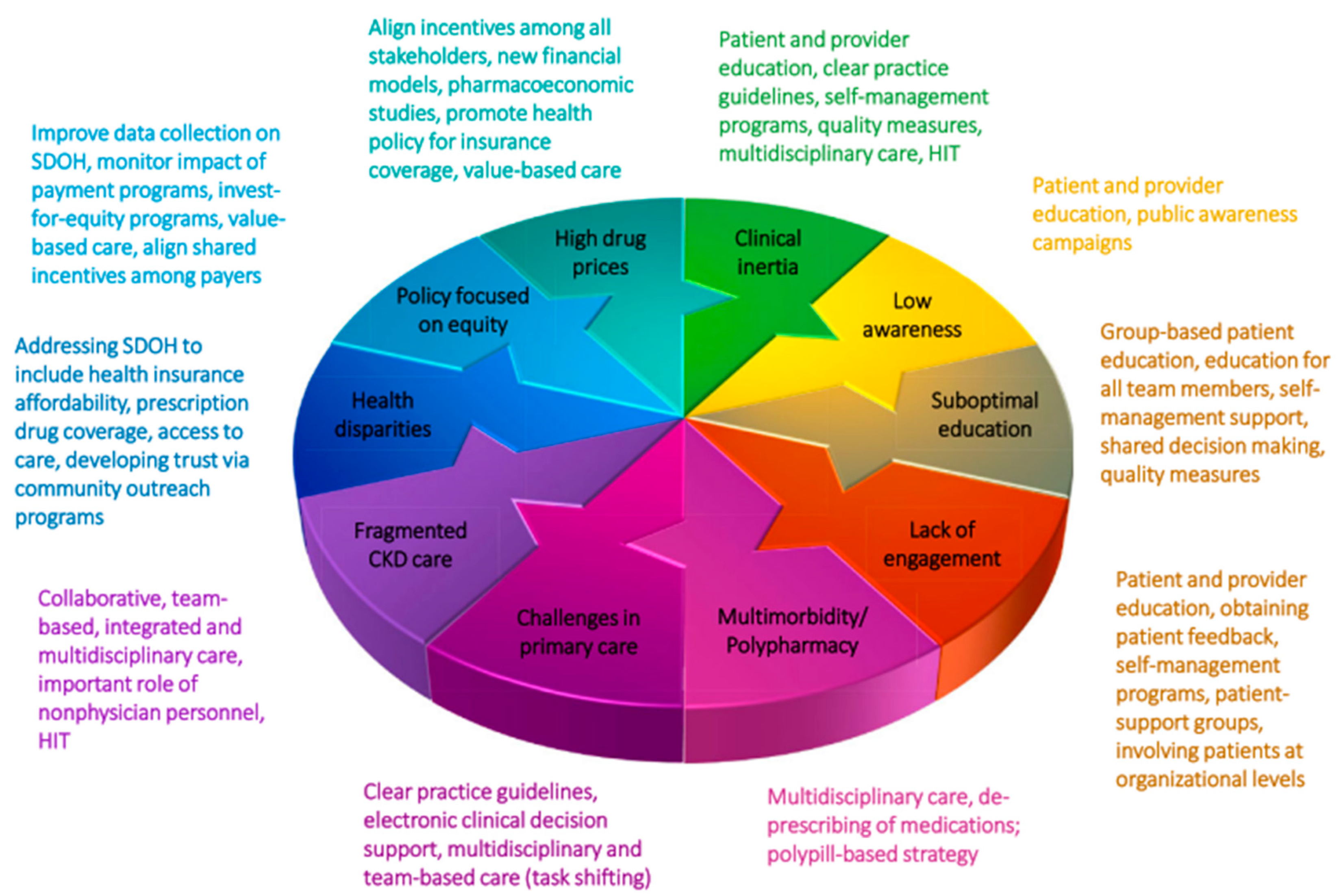
2. Overcoming Barriers to CKD Care Delivery
2.1. Methodology
2.2. CKD Education Unmet Needs
2.2.1. Patient and Provider CKD Education Gaps
2.2.2. Resource and Education Reimbursement Challenges
2.2.3. Stakeholder Opportunities
2.3. Challenges to CKD Care Delivery
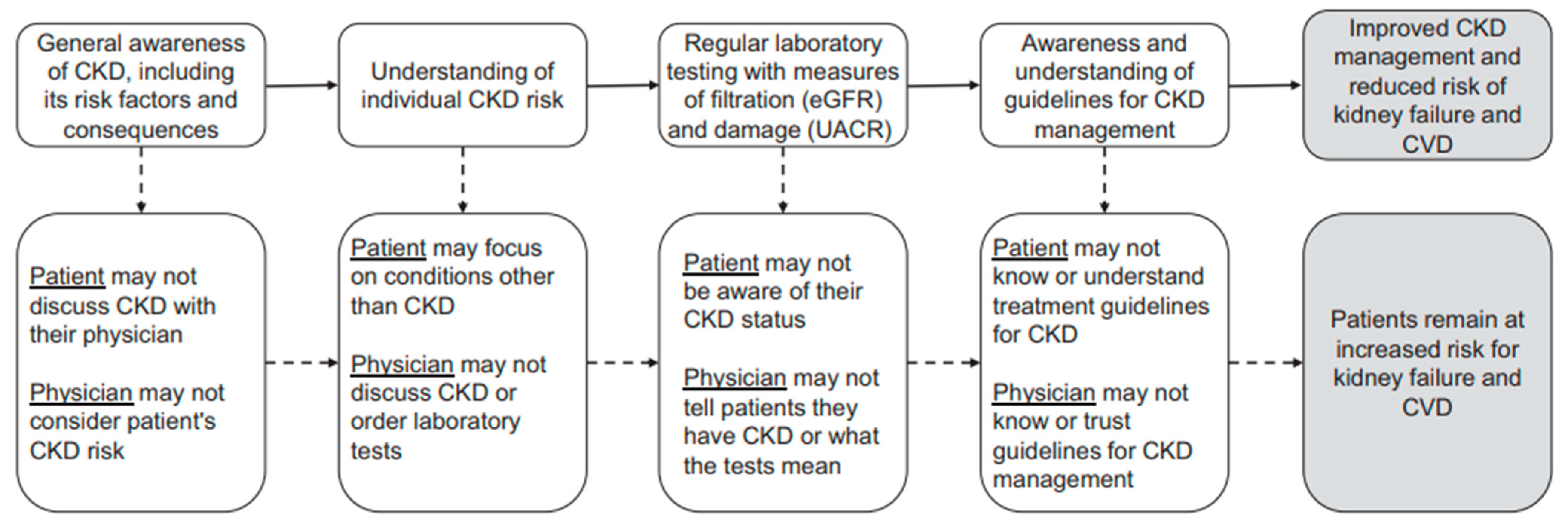
2.3.1. Barriers to Identification and Diagnosis of Patients with CKD
2.3.2. Lack of Bandwidth and Support for Providers
2.3.3. Financial Challenges
2.3.4. Stakeholder Opportunities
2.4. Existing Care Pathways
2.4.1. Clinical Biomarkers and Risk Prediction Equations
2.4.2. Screening and Early Identification of Patients
2.4.3. Workflows and Referral Pathways
2.4.4. Stakeholder Opportunities
2.5. Optimal CKD Care Delivery
2.5.1. Characteristics of an Optimal Care Pathway
2.5.2. Potential Barriers and Limitations
2.5.3. Reimagining CKD Management
2.5.4. Stakeholder Opportunities
3. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Society of Nephrology. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2013, 3, 1–163. [Google Scholar]
- McGill, J.B.; Haller, H.; Roy-Chaudhury, P.; Cherrington, A.; Wada, T.; Wanner, C.; Ji, L.; Rossing, P. Making an impact on kidney disease in people with type 2 diabetes: The importance of screening for albuminuria. BMJ Open Diabetes Res. Care 2022, 10, e002806. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. United States Renal Data System: 2022 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2022. [Google Scholar]
- Centers for Disease Control and Prevention. Chronic Kidney Disease in the United States. 2023. Available online: https://www.cdc.gov/kidneydisease/publications-resources/CKD-national-facts.html (accessed on 24 January 2024).
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.W.; et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: Reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [PubMed]
- Pugh, D.; Gallacher, P.J.; Dhaun, N. Management of Hypertension in Chronic Kidney Disease. Drugs 2019, 79, 365–379. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.E.; Mouton, A.J.; da Silva, A.A.; Omoto, A.C.M.; Wang, Z.; Li, X.; do Carmo, J.M. Obesity, kidney dysfunction, and inflammation: Interactions in hypertension. Cardiovasc. Res. 2021, 117, 1859–1876. [Google Scholar] [CrossRef] [PubMed]
- Lakkis, J.I.; Weir, M.R. Obesity and Kidney Disease. Prog. Cardiovasc. Dis. 2018, 61, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; de Jong, P.E.; Coresh, J.; El Nahas, M.; Astor, B.C.; Matsushita, K.; Gansevoort, R.T.; Kasiske, B.L.; Eckardt, K.U. The definition, classification, and prognosis of chronic kidney disease: A KDIGO Controversies Conference report. Kidney Int. 2011, 80, 17–28. [Google Scholar] [CrossRef]
- Stengel, B.; Muenz, D.; Tu, C.; Speyer, E.; Alencar de Pinho, N.; Combe, C.; Yamagata, K.; Reichel, H.; Fliser, D.; Massy, Z.A.; et al. Adherence to the Kidney Disease: Improving Global Outcomes CKD Guideline in Nephrology Practice across Countries. Kidney Int. Rep. 2021, 6, 437–448. [Google Scholar] [CrossRef]
- Bramlage, P.; Lanzinger, S.; Tittel, S.R.; Hess, E.; Fahrner, S.; Heyer, C.H.J.; Friebe, M.; Buschmann, I.; Danne, T.; Seufert, J.; et al. Guidelines adherence in the prevention and management of chronic kidney disease in patients with diabetes mellitus on the background of recent European recommendations—A registry-based analysis. BMC Nephrol. 2021, 22, 184. [Google Scholar] [CrossRef]
- Shin, J.I.; Chang, A.R.; Grams, M.E.; Coresh, J.; Ballew, S.H.; Surapaneni, A.; Matsushita, K.; Bilo, H.J.G.; Carrero, J.J.; Chodick, G.; et al. Albuminuria Testing in Hypertension and Diabetes: An Individual-Participant Data Meta-Analysis in a Global Consortium. Hypertension 2021, 78, 1042–1052. [Google Scholar] [CrossRef]
- Chu, C.D.; Powe, N.R.; Shlipak, M.G.; Scherzer, R.; Tummalapalli, S.L.; Estrella, M.M.; Tuot, D.S. Albuminuria testing and nephrology care among insured US adults with chronic kidney disease: A missed opportunity. BMC Prim. Care 2022, 23, 299. [Google Scholar] [CrossRef]
- Murton, M.; Goff-Leggett, D.; Bobrowska, A.; Garcia Sanchez, J.J.; James, G.; Wittbrodt, E.; Nolan, S.; Sorstadius, E.; Pecoits-Filho, R.; Tuttle, K. Burden of Chronic Kidney Disease by KDIGO Categories of Glomerular Filtration Rate and Albuminuria: A Systematic Review. Adv. Ther. 2021, 38, 180–200. [Google Scholar] [CrossRef] [PubMed]
- Flammia, R.S.; Tufano, A.; Proietti, F.; Gerolimetto, C.; De Nunzio, C.; Franco, G.; Leonardo, C. Renal surgery for kidney cancer: Is preoperative proteinuria a predictor of functional and survival outcomes after surgery? A systematic review of the literature. Minerva Urol. Nephrol. 2022, 74, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes Blood Pressure Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney Int. 2021, 99, S1–S87. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes Diabetes Work G: KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int. 2022, 102, S1–S127. [CrossRef] [PubMed]
- Sundstrom, J.; Bodegard, J.; Bollmann, A.; Vervloet, M.G.; Mark, P.B.; Karasik, A.; Taveira-Gomes, T.; Botana, M.; Birkeland, K.I.; Thuresson, M.; et al. Prevalence, outcomes, and cost of chronic kidney disease in a contemporary population of 2.4 million patients from 11 countries: The CaReMe CKD study. Lancet Reg. Health Eur. 2022, 20, 100438. [Google Scholar] [CrossRef] [PubMed]
- Pollock, C.; James, G.; Garcia Sanchez, J.J.; Carrero, J.J.; Arnold, M.; Lam, C.S.P.; Chen, H.T.; Nolan, S.; Pecoits-Filho, R.; Wheeler, D.C. Healthcare resource utilisation and related costs of patients with CKD from the UK: A report from the DISCOVER CKD retrospective cohort. Clin. Kidney J. 2022, 15, 2124–2134. [Google Scholar] [CrossRef]
- Garcia Sanchez, J.J.; James, G.; Carrero, J.J.; Arnold, M.; Lam, C.S.P.; Pollock, C.; Chen, H.T.; Nolan, S.; Wheeler, D.C.; Pecoits-Filho, R. Health Care Resource Utilization and Related Costs of Patients with CKD from the United States: A Report from the DISCOVER CKD Retrospective Cohort. Kidney Int. Rep. 2023, 8, 785–795. [Google Scholar] [CrossRef]
- National Kidney Foundation. KDOQI Clinical Practice Guideline for Diabetes and CKD: 2012 Update. Am. J. Kidney Dis. 2012, 60, 850–886. [Google Scholar] [CrossRef]
- Inker, L.A.; Astor, B.C.; Fox, C.H.; Isakova, T.; Lash, J.P.; Peralta, C.A.; Kurella Tamura, M.; Feldman, H.I. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am. J. Kidney Dis. 2014, 63, 713–735. [Google Scholar] [CrossRef] [PubMed]
- Department of Veterans Affairs, United States Department of Defense. VA/DoD Clinical Practice Guidelines for the Management of Chronic Kidney Disease; Version 4.0.; Department of Veterans Affairs: Washington, DC, USA, 2019. [Google Scholar]
- de Boer, I.H.; Khunti, K.; Sadusky, T.; Tuttle, K.R.; Neumiller, J.J.; Rhee, C.M.; Rosas, S.E.; Rossing, P.; Bakris, G. Diabetes Management in Chronic Kidney Disease: A Consensus Report by the American Diabetes Association (ADA) and Kidney Disease: Improving Global Outcomes (KDIGO). Diabetes Care 2022, 45, 3075–3090. [Google Scholar] [CrossRef] [PubMed]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef] [PubMed]
- Gaitonde, D.Y.; Cook, D.L.; Rivera, I.M. Chronic Kidney Disease: Detection and Evaluation. Am. Fam. Physician 2017, 96, 776–783. [Google Scholar] [PubMed]
- Mottl, A.K.; Alicic, R.; Argyropoulos, C.; Brosius, F.C.; Mauer, M.; Molitch, M.; Nelson, R.G.; Perreault, L.; Nicholas, S.B. KDOQI US Commentary on the KDIGO 2020 Clinical Practice Guideline for Diabetes Management in CKD. Am. J. Kidney Dis. 2022, 79, 457–479. [Google Scholar] [CrossRef]
- Stempniewicz, N.; Vassalotti, J.A.; Cuddeback, J.K.; Ciemins, E.; Storfer-Isser, A.; Sang, Y.; Matsushita, K.; Ballew, S.H.; Chang, A.R.; Levey, A.S.; et al. Chronic Kidney Disease Testing among Primary Care Patients with Type 2 Diabetes Across 24 U.S. Health Care Organizations. Diabetes Care 2021, 44, 2000–2009. [Google Scholar] [CrossRef] [PubMed]
- Alfego, D.; Ennis, J.; Gillespie, B.; Lewis, M.J.; Montgomery, E.; Ferre, S.; Vassalotti, J.A.; Letovsky, S. Chronic Kidney Disease Testing among At-Risk Adults in the U.S. Remains Low: Real-World Evidence from a National Laboratory Database. Diabetes Care 2021, 44, 2025–2032. [Google Scholar] [CrossRef] [PubMed]
- Delgado, C.; Baweja, M.; Crews, D.C.; Eneanya, N.D.; Gadegbeku, C.A.; Inker, L.A.; Mendu, M.L.; Miller, W.G.; Moxey-Mims, M.M.; Roberts, G.V.; et al. A Unifying Approach for GFR Estimation: Recommendations of the NKF-ASN Task Force on Reassessing the Inclusion of Race in Diagnosing Kidney Disease. J. Am. Soc. Nephrol. 2021, 32, 2994–3015. [Google Scholar] [CrossRef]
- Lees, J.S.; Rutherford, E.; Stevens, K.I.; Chen, D.C.; Scherzer, R.; Estrella, M.M.; Sullivan, M.K.; Ebert, N.; Mark, P.B.; Shlipak, M.G. Assessment of Cystatin C Level for Risk Stratification in Adults with Chronic Kidney Disease. JAMA Netw. Open 2022, 5, e2238300. [Google Scholar] [CrossRef]
- Levey, A.S.; Becker, C.; Inker, L.A. Glomerular filtration rate and albuminuria for detection and staging of acute and chronic kidney disease in adults: A systematic review. JAMA 2015, 313, 837–846. [Google Scholar] [CrossRef]
- Raghavan, D.; Holley, J.L. Conservative Care of the Elderly CKD Patient: A Practical Guide. Adv. Chronic Kidney Dis. 2016, 23, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Flory, J.H.; Guelce, D.; Goytia, C.; Li, J.; Min, J.Y.; Mushlin, A.; Orloff, J.; Mayer, V. Prescriber Uncertainty as Opportunity to Improve Care of Type 2 Diabetes with Chronic Kidney Disease: Mixed Methods Study. J. Gen. Intern. Med. 2023, 38, 1476–1483. [Google Scholar] [CrossRef] [PubMed]
- Weckmann, G.F.C.; Stracke, S.; Haase, A.; Spallek, J.; Ludwig, F.; Angelow, A.; Emmelkamp, J.M.; Mahner, M.; Chenot, J.F. Diagnosis and management of non-dialysis chronic kidney disease in ambulatory care: A systematic review of clinical practice guidelines. BMC Nephrol. 2018, 19, 258. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M.J.; Gil, S.; Hemmelgarn, B.R.; Manns, B.J.; Tonelli, M.; Jun, M.; Donald, M. A scoping review of adult chronic kidney disease clinical pathways for primary care. Nephrol. Dial. Transplant. 2017, 32, 838–846. [Google Scholar] [CrossRef]
- Manns, L.; Scott-Douglas, N.; Tonelli, M.; Weaver, R.; Tam-Tham, H.; Chong, C.; Hemmelgarn, B. A Population-Based Analysis of Quality Indicators in CKD. Clin. J. Am. Soc. Nephrol. 2017, 12, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Bansal, S.; Mader, M.; Pugh, J.A. Screening and Recognition of Chronic Kidney Disease in VA Health Care System Primary Care Clinics. Kidney360 2020, 1, 904–915. [Google Scholar] [CrossRef] [PubMed]
- Skolnik, N.S.; Style, A.J. Importance of Early Screening and Diagnosis of Chronic Kidney Disease in Patients with Type 2 Diabetes. Diabetes Ther. 2021, 12, 1613–1630. [Google Scholar] [CrossRef] [PubMed]
- Folkerts, K.; Petruski-Ivleva, N.; Comerford, E.; Blankenburg, M.; Evers, T.; Gay, A.; Fried, L.; Kovesdy, C.P. Adherence to Chronic Kidney Disease Screening Guidelines among Patients with Type 2 Diabetes in a US Administrative Claims Database. Mayo Clin. Proc. 2021, 96, 975–986. [Google Scholar] [CrossRef]
- Yuen, J.; Harasemiw, O.; Singer, A.; Bello, A.; Ronksley, P.E.; Bohm, C.; Drummond, N.; Tangri, N. Risk of CKD Progression and Quality-of-Care Indicators in the Primary Care Setting. Am. J. Kidney Dis. 2023, 81, 247–249. [Google Scholar] [CrossRef]
- Chu, C.D.; McCulloch, C.E.; Banerjee, T.; Pavkov, M.E.; Burrows, N.R.; Gillespie, B.W.; Saran, R.; Shlipak, M.G.; Powe, N.R.; Tuot, D.S.; et al. CKD Awareness among US Adults by Future Risk of Kidney Failure. Am. J. Kidney Dis. 2020, 76, 174–183. [Google Scholar] [CrossRef]
- Chen, J.; Fowler, K.J.; Grams, M.E. Knowledge Is Power: Patient Education as a Tool for Patient Activation. Am. J. Kidney Dis. 2020, 76, 163–165. [Google Scholar] [CrossRef]
- Quinones, J.; Hammad, Z. Social Determinants of Health and Chronic Kidney Disease. Cureus 2020, 12, e10266. [Google Scholar] [CrossRef]
- Haase, A.; Stracke, S.; Chenot, J.F.; Weckmann, G. Perspective of General Practitioners on Management of Non-dialysis Chronic Kidney Disease—A Qualitative Study. Dtsch. Med. Wochenschr. 2021, 146, e97–e102. [Google Scholar] [PubMed]
- Blakeman, T.; Protheroe, J.; Chew-Graham, C.; Rogers, A.; Kennedy, A. Understanding the management of early-stage chronic kidney disease in primary care: A qualitative study. Br. J. Gen. Pract. 2012, 62, e233–e242. [Google Scholar] [CrossRef] [PubMed]
- Waterman, A.D.; Nair, D.; Purnajo, I.; Cavanaugh, K.L.; Mittman, B.S.; Peipert, J.D. The Knowledge Assessment of Renal Transplantation (KART) 2.0: Development and Validation of CKD and Transplant Knowledge Scales. Clin. J. Am. Soc. Nephrol. 2022, 17, 555–564. [Google Scholar] [CrossRef] [PubMed]
- National Committee for Quality Assurance. Chronic Kidney Disease Disparities: Educational Guide for Primary Care; Centers for Medicare and Medicaid, Office of Minority Health: Baltimore, MD, USA, 2021. Available online: https://www.cms.gov/files/document/chronic-kidney-disease-disparities-educational-guide-primary-care.pdf (accessed on 24 January 2024).
- National Institute of Diabetes and Digestive and Kidney Diseases. Explaining Your Kidney Test Results: A Tool for Clinical Use; United States Department of Health and Human Services, National Institutes of Health: Bethesda, MD, USA, 2014. Available online: https://www.niddk.nih.gov/health-information/professionals/advanced-search/explain-kidney-test-results (accessed on 24 January 2024).
- Chronic Kidney Disease Network. Integrating Risk-Based Care for Patients with Chronic Kidey Disease in the Community (Learn More): The Kidney Failure Risk Equation; Chronic Disease Innovation Centre: Winnipeg, MB, Canada, 2022; Available online: https://www.kidneyfailurerisk.com/ (accessed on 24 January 2024).
- National Kidney Foundation. eGFR Calculator; National Kidney Foundation: New York, NY, USA, 2021; Available online: https://www.kidney.org/apps/professionals/egfr-calculator (accessed on 24 January 2024).
- National Institute of Diabetes and Digestive and Kidney Diseases. Kidney Disease for Health Professionals; United States Department of Health and Human Services, National Institutes of Health: Bethesda, MD, USA, 2023. Available online: https://www.niddk.nih.gov/health-information/professionals/clinical-tools-patient-management/kidney-disease (accessed on 24 January 2024).
- National Kidney Foundation. Relative Risk, Monitoring and Referral in Patients with Ckd; App Center; NKF: New York, NY, USA, 2024; Available online: https://www.kidney.org/apps/professionals/relative-risk-monitoring-and-referral-patients-ckd (accessed on 24 January 2024).
- National Kidney Foundation. KDOQI App; NKF: New York, NY, USA, 2024; Available online: https://www.kidney.org/apps/professionals/kdoqi-app (accessed on 24 January 2024).
- National Institute of Diabetes and Digestive and Kidney Diseases. United States Renal Data System Website; United States Department of Health and Human Services, National Institutes of Health: Bethesda, MD, USA, 2024. Available online: https://www.niddk.nih.gov/about-niddk/strategic-plans-reports/usrds (accessed on 24 January 2024).
- Centers for Disease Control and Prevention Website. Kidney Disease Surveillance System: Chronic Kidney Disease Risk Calculators; 2024. Available online: https://nccd.cdc.gov/ckd/Calculators.aspx (accessed on 24 January 2024).
- Tuttle, K.R.; Alicic, R.Z.; Short, R.A.; Neumiller, J.J.; Gates, B.J.; Daratha, K.B.; Barbosa-Leiker, C.; McPherson, S.M.; Chaytor, N.S.; Dieter, B.P.; et al. Medication Therapy Management after Hospitalization in CKD: A Randomized Clinical Trial. Clin. J. Am. Soc. Nephrol. 2018, 13, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Saxena, N.; Rizk, D.V. The interdisciplinary team: The whole is larger than the parts. Adv. Chronic. Kidney Dis. 2014, 21, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Hahr, A.I.; Molitch, M.E. Manament of Diabetes Mellitus in Patients with CKD: Core Curriculum 2022. Am. J. Kidney Dis. 2022, 79, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Helou, N.; Talhouedec, D.; Shaha, M.; Zanchi, A. The impact of a multidisciplinary self-care management program on quality of life, self-care, adherence to anti-hypertensive therapy, glycemic control, and renal function in diabetic kedney disease: A Crossover Study Protocol. BMC Nephrol. 2016, 17, 88. [Google Scholar] [CrossRef] [PubMed]
- Bello, A.K.; Johnson, D.W. Educating primary healthcare providers about kidney disease. Nat. Rev. Nephrol. 2022, 18, 133–134. [Google Scholar] [CrossRef]
- Micallef, R.; Kayyali, R.A. Systematic Review of Models Used and Preferences for Continuing Education and Continuing Professional Development of Pharmacists. Pharmacy 2019, 7, 154. [Google Scholar] [CrossRef] [PubMed]
- Lesko, L.J.; Johnson, J.A. Academia at the crossroads: Education and training in pharmacogenomics. Pers. Med. 2012, 9, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Diamantidis, C.J.; Becker, S. Health information technology (IT) to improve the care of patients with chronic kidney disease (CKD). BMC Nephrol. 2014, 15, 7. [Google Scholar] [CrossRef] [PubMed]
- Green, J.A.; Ephraim, P.L.; Hill-Briggs, F.; Browne, T.; Strigo, T.S.; Hauer, C.L.; Yule, C.; Stametz, R.A.; Littlewood, D.; Pendergast, J.F.; et al. Integrated Digital Health System Tools to Support Decision Making and Treatment Preparation in CKD: The PREPARE NOW Study. Kidney Med. 2021, 3, 565–575.e1. [Google Scholar] [CrossRef] [PubMed]
- Sequist, T.D.; Holliday, A.M.; Orav, E.J.; Bates, D.W.; Denker, B.M. Physician and patient tools to improve chronic kidney disease care. Am. J. Manag. Care 2018, 24, e107–e114. [Google Scholar] [PubMed]
- Betts, K.A.; Song, J.; Elliott, J.; Warnock, N.; Farej, R.; Wu, A.; Singh, R. Geographical variation in kidney function testing and associations with health care costs among patients with chronic kidney disease and type 2 diabetes. Am. J. Manag. Care 2022, 28, S112–S119. [Google Scholar] [PubMed]
- Foti, K.; Chang, A.R. CKD Management in Primary Care: Supporting Systems Change. Am. J. Kidney Dis. 2020, 76, 613–615. [Google Scholar] [CrossRef]
- Martinez, Y.V.; Benett, I.; Lewington, A.J.P.; Wierzbicki, A.S.; Guideline, C. Chronic kidney disease: Summary of updated NICE guidance. BMJ 2021, 374, n1992. [Google Scholar] [CrossRef]
- Tangri, N.; Stevens, L.A.; Griffith, J.; Tighiouart, H.; Djurdjev, O.; Naimark, D.; Levin, A.; Levey, A.S. A predictive model for progression of chronic kidney disease to kidney failure. JAMA 2011, 305, 1553–1559. [Google Scholar] [CrossRef]
- Ahmed, S.; Mothi, S.S.; Sequist, T.; Tangri, N.; Khinkar, R.M.; Mendu, M.L. The Kidney Failure Risk Equation Score and CKD Care Delivery Measures: A Cross-sectional Study. Kidney Med. 2022, 4, 100375. [Google Scholar] [CrossRef]
- Sumida, K.; Nadkarni, G.N.; Grams, M.E.; Sang, Y.; Ballew, S.H.; Coresh, J.; Matsushita, K.; Surapaneni, A.; Brunskill, N.; Chadban, S.J.; et al. Conversion of Urine Protein-Creatinine Ratio or Urine Dipstick Protein to Urine Albumin-Creatinine Ratio for Use in Chronic Kidney Disease Screening and Prognosis: An Individual Participant-Based Meta-analysis. Ann. Intern. Med. 2020, 173, 426–435. [Google Scholar] [CrossRef]
- Maciejewski, M. Chronic Kidney Disease Often Undiagnosed in Medicare Beneficiaries; CMS OMH Data Highlight No. 20; CMS Office of Minority Health: Baltimore, MD, USA, 2020. [Google Scholar]
- Renal Physicians Association Position Paper. Guidance on Delivery of Optimal Advanced CKD Care. 2021. Available online: https://cdn.ymaws.com/www.renalmd.org/resource/resmgr/whats_new/guidance_on_delivery_of_opti.pdf (accessed on 14 February 2024).
- Value-Based Frameworks Can Help Transform Kidney Care Delivery. Available online: https://www.ajmc.com/view/value-based-frameworks-can-help-transform-kidney-care-delivery (accessed on 24 January 2024).
- Chong, C.; Smekal, M.; Hemmelgarn, B.; Elliott, M.; Allu, S.; Wick, J.; McBrien, K.; Jackson, W.; Bello, A.; Jindal, K.; et al. Use of Google Analytics to Explore Dissemination Activities for an Online CKD Clinical Pathway: A Retrospective Study. Can. J. Kidney Health Dis. 2022, 9, 20543581221097456. [Google Scholar] [CrossRef]
- Donald, M.; Smekal, M.D.; Elliott, M.J.; McBrien, K.; Weaver, R.G.; Manns, B.J.; Tonelli, M.; Bello, A.; Straus, S.E.; Scott-Douglas, N.; et al. Online clinical pathway for chronic kidney disease management in primary care: A retrospective cohort study. BMC Nephrol. 2021, 22, 332. [Google Scholar] [CrossRef]
- Zhang, Y.; Padman, R.; Wasserman, L. On Learning and Visualizing Practice-based Clinical Pathways for Chronic Kidney Disease. AMIA Annu. Symp. Proc. 2014, 2014, 1980–1989. [Google Scholar] [PubMed]
- Zhang, Y.; Padman, R. An Interactive Platform to Visualize Data-Driven Clinical Pathways for the Management of Multiple Chronic Conditions. Stud. Health Technol. Inform. 2017, 245, 672–676. [Google Scholar] [PubMed]
- Centers for Medicare and Medicaid Services. HHS to Transform Care Delivery for Patients with Chronic Kidney Disease; Centers for Medicare and Medicaid Services: Baltimore, MD, USA, 2019. [Google Scholar]
- Tsang, J.Y.; Blakeman, T.; Hegarty, J.; Humphreys, J.; Harvey, G. Understanding the implementation of interventions to improve the management of chronic kidney disease in primary care: A rapid realist review. Implement. Sci. 2016, 11, 47. [Google Scholar] [CrossRef] [PubMed]
- Cockcroft, D.W.; Gault, M.H. Prediction of creatinine clearance from serum creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N. Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.J.; Munoz, A.; Schneider, M.F.; Mak, R.H.; Kaskel, F.; Warady, B.A.; Furth, S.L. New equations to estimate GFR in children with CKD. J. Am. Soc. Nephrol. 2009, 20, 629–637. [Google Scholar] [CrossRef]
- Inker, L.A.; Eneanya, N.D.; Coresh, J.; Tighiouart, H.; Wang, D.; Sang, Y.; Crews, D.C.; Doria, A.; Estrella, M.M.; Froissart, M.; et al. New Creatinine- and Cystatin C-Based Equations to Estimate GFR without Race. N. Engl. J. Med. 2021, 385, 1737–1749. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Diabetes of Digestive and Kidney Diseases. CKD Biomarkers Consortium. Available online: https://repository.niddk.nih.gov/studies/ckd-biocon/ (accessed on 24 January 2024).
- Bang, H.; Vupputuri, S.; Shoham, D.A.; Klemmer, P.J.; Falk, R.J.; Mazumdar, M.; Gipson, D.; Colindres, R.E.; Kshirsagar, A.V. SCreening for Occult REnal Disease (SCORED): A simple prediction model for chronic kidney disease. Arch. Intern. Med. 2007, 167, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.; Ning, H.; Bansal, N.; Cohen, J.; Srivastava, A.; Dobre, M.; Michos, E.D.; Rahman, M.; Townsend, R.; Seliger, S.; et al. Ten-Year Risk-Prediction Equations for Incident Heart Failure Hospitalizations in Chronic Kidney Disease: Findings from the Chronic Renal Insufficiency Cohort Study and the Multi-Ethnic Study of Atherosclerosis. J. Card. Fail. 2022, 28, 540–550. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Peter, S.S.; Chu, C.D.; Tuot, D.S.; Chen, J.H. Analysis of Specialty Nephrology Care among Patients with Chronic Kidney Disease and High Risk of Disease Progression. JAMA Netw. Open 2022, 5, e2225797. [Google Scholar] [CrossRef] [PubMed]
- Oliva-Damaso, N.; Delanaye, P.; Oliva-Damaso, E.; Payan, J.; Glassock, R.J. Risk-based versus GFR threshold criteria for nephrology referral in chronic kidney disease. Clin. Kidney J. 2022, 15, 1996–2005. [Google Scholar] [CrossRef] [PubMed]
- International Society of Nephrology. Early Diagnosis of Chronic Kidney Disease; A Discussion Paper for Building Resilience and Sustainability of Healthcare Systems; International Society of Nephrology: St. Josse Ten Noode, Belgium, 2021. [Google Scholar]
- Curtis, S.; Komenda, P. Screening for chronic kidney disease: Moving toward more sustainable health care. Curr. Opin. Nephrol. Hypertens. 2020, 29, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Llewellyn, S. Screening for chronic kidney disease in a hypertensive primary care cohort. J. Am. Assoc. Nurse Pract. 2020, 33, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Burgos-Calderon, R.; Depine, S.A.; Aroca-Martinez, G. Population Kidney Health. A New Paradigm for Chronic Kidney Disease Management. Int. J. Environ. Res. Public Health 2021, 18, 6786. [Google Scholar] [CrossRef]
- Hao, S.; Fu, T.; Wu, Q.; Jin, B.; Zhu, C.; Hu, Z.; Guo, Y.; Zhang, Y.; Yu, Y.; Fouts, T.; et al. Estimating One-Year Risk of Incident Chronic Kidney Disease: Retrospective Development and Validation Study Using Electronic Medical Record Data from the State of Maine. JMIR Med. Inform. 2017, 5, e21. [Google Scholar] [CrossRef]
- Mendu, M.L.; Ahmed, S.; Maron, J.K.; Rao, S.K.; Chaguturu, S.K.; May, M.F.; Mutter, W.P.; Burdge, K.A.; Steele, D.J.R.; Mount, D.B.; et al. Development of an electronic health record-based chronic kidney disease registry to promote population health management. BMC Nephrol. 2019, 20, 72. [Google Scholar] [CrossRef]
- Lim, D.; Randall, S.; Robinson, S.; Thomas, E.; Williamson, J.; Chakera, A.; Napier, K.; Schwan, C.; Manuel, J.; Betts, K.; et al. Unlocking Potential within Health Systems Using Privacy-Preserving Record Linkage: Exploring Chronic Kidney Disease Outcomes through Linked Data Modelling. Appl. Clin. Inform. 2022, 13, 901–909. [Google Scholar] [CrossRef]
- Norris, K.C.; Duru, O.K.; Alicic, R.Z.; Daratha, K.B.; Nicholas, S.B.; McPherson, S.M.; Bell, D.S.; Shen, J.I.; Jones, C.R.; Moin, T.; et al. Rationale and design of a multicenter Chronic Kidney Disease (CKD) and at-risk for CKD electronic health records-based registry: CURE-CKD. BMC Nephrol. 2019, 20, 416. [Google Scholar] [CrossRef] [PubMed]
- Mendu, M.L.; Waikar, S.S.; Rao, S.K. Kidney Disease Population Health Management in the Era of Accountable Care: A Conceptual Framework for Optimizing Care Across the CKD Spectrum. Am. J. Kidney Dis. 2017, 70, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Vassalotti, J.A.; Boucree, S.C. Integrating CKD Into US Primary Care: Bridging the Knowledge and Implementation Gaps. Kidney Int. Rep. 2022, 7, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Nee, R.; Yuan, C.M.; Narva, A.S.; Yan, G.; Norris, K.C. Overcoming barriers to implementing new guideline-directed therapies for chronic kidney disease. Nephrol. Dial. Transplant. 2023, 38, 532–541. [Google Scholar] [CrossRef]
- Shah, A.P.; Mehrotra, R. Searching for new care models for chronic kidney disease. Kidney Int. 2012, 82, 621–623. [Google Scholar] [CrossRef]
- Centers for Medicare and Medicaid Services. Kidney Care Choices (KCC) Model; Centers for Medicare and Medicaid Services: Baltimore, MD, USA. Available online: https://innovation.cms.gov/innovation-models/kidney-care-choices-kcc-model (accessed on 24 January 2024).
- Centers for Medicare and Medicaid Services. CMS Announces Transformative New Model of Care for Medicare Beneficiaries with Chronic Kidney Disease; Centers for Medicare and Medicaid Services: Baltimore, MD, USA, 2020. [Google Scholar]
- Yuan, Q.; Zhang, H.; Deng, T.; Tang, S.; Yuan, X.; Tang, W.; Xie, Y.; Ge, H.; Wang, X.; Zhou, Q.; et al. Role of Artificial Intelligence in Kidney Disease. Int. J. Med. Sci. 2020, 17, 970–984. [Google Scholar] [CrossRef] [PubMed]
- Rashidi, P.; Bihorac, A. Artificial intelligence approaches to improve kidney care. Nat. Rev. Nephrol. 2020, 16, 71–72. [Google Scholar] [CrossRef]
- Nadkarni, G.; HIT Consultant. Can Artificial Intelligence Solve the Chronic Kidney Disease Epidemic? 2019. Available online: https://hitconsultant.net/2019/06/25/ai-chronic-kidney-disease-epidemic/ (accessed on 24 January 2024).
- Ananda Padmanabhan, A.; Balczewski, E.A.; Singh, K. Artificial Intelligence Systems in CKD: Where Do We Stand and What Will the Future Bring? Adv. Chronic Kidney Dis. 2022, 29, 461–464. [Google Scholar] [CrossRef]
- Mosa, A.I.; Watts, D.; Tangri, N. Impacting Management of Chronic Kidney Disease through Primary Care Practice Audits: A Quality Improvement Study. Can. J. Kidney Health Dis. 2022, 9, 20543581221144840. [Google Scholar] [CrossRef]
- Frensius Medical Care. 5 Ways Artificial Intelligence (AI) Is Impacting Kidney Disease. Available online: https://fmcna.com/insights/articles/5-ways-artificial-intelligence-ai-impacting-kidney-disease/ (accessed on 24 January 2024).
- Rashed-Al-Mahfuz, M.; Haque, A.; Azad, A.; Alyami, S.A.; Quinn, J.M.W.; Moni, M.A. Clinically Applicable Machine Learning Approaches to Identify Attributes of Chronic Kidney Disease (CKD) for Use in Low-Cost Diagnostic Screening. IEEE J. Transl. Eng. Health Med. 2021, 9, 4900511. [Google Scholar] [CrossRef]
- Krishnamurthy, S.; Ks, K.; Dovgan, E.; Lustrek, M.; Gradisek Piletic, B.; Srinivasan, K.; Li, Y.J.; Gradisek, A.; Syed-Abdul, S. Machine Learning Prediction Models for Chronic Kidney Disease Using National Health Insurance Claim Data in Taiwan. Healthcare 2021, 9, 546. [Google Scholar] [CrossRef] [PubMed]
- Kanda, E.; Epureanu, B.I.; Adachi, T.; Kashihara, N. Machine-learning-based Web system for the prediction of chronic kidney disease progression and mortality. PLoS Digit. Health 2023, 2, e0000188. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Huth, C.; Covic, M.; Troll, M.; Adam, J.; Zukunft, S.; Prehn, C.; Wang, L.; Nano, J.; Scheerer, M.F.; et al. Machine Learning Approaches Reveal Metabolic Signatures of Incident Chronic Kidney Disease in Individuals with Prediabetes and Type 2 Diabetes. Diabetes 2020, 69, 2756–2765. [Google Scholar] [CrossRef] [PubMed]
- Tangri, N.; Ferguson, T.W. Artificial Intelligence in the Identification, Management, and Follow-Up of CKD. Kidney360 2022, 3, 554–556. [Google Scholar] [CrossRef] [PubMed]
- Urbanski, M.A.; Wilk, A.S.; Escoffery, C.; Patzer, R.E. Dissemination and Implementation Science: A Primer and Applications in Nephrology. Kidney360 2022, 3, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Jhamb, M.; Weltman, M.R.; Yabes, J.G.; Kamat, S.; Devaraj, S.M.; Fischer, G.S.; Rollman, B.L.; Nolin, T.D.; Abdel-Kader, K. Electronic health record based population health management to optimize care in CKD: Design of the Kidney Coordinated Health Management Partnership (K-CHAMP) trial. Contemp. Clin. Trials 2023, 131, 107269. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Resource | User(s) | Description | Reference |
|---|---|---|---|
| KART 2.0 | Primary care | Validated tool to assess patients’ knowledge of CKD and kidney transplantation | Waterman, A.D.; Nair, D.; Purnajo, I.; Cavanaugh, K.L.; Mittman, B.S.; Peipert, J.D. The Knowledge Assessment of Renal Transplantation (KART) 2.0: Development and validation of CKD and transplant knowledge scales. Clin. J. Am. Soc. Nephrol. 2022, 17, 555–564. [48] |
| Chronic Kidney Disease Disparities: Educational Guide for Primary Care (CMS) | Primary care | Educational guide
| https://www.cms.gov/files/document/chronic-kidney-disease-disparities-educational-guide-primary-care.pdf. (accessed on 24 January 2024) [49] |
| Explaining Your Kidney Test Results: A Tool for Clinical Use (NIDDK, NIH) | CKD care teams and patients | Online and printable tool for clinical use to explain kidney test results in a digestible and understandable way to patients | https://www.niddk.nih.gov/health-information/professionals/advanced-search/explain-kidney-test-results. (accessed on 24 January 2024) [50] |
| The Kidney Failure Risk Equation Calculator (CKD Network) | CKD care teams and patients | Validated online tool that uses 4- and 8-variable equations to accurately predict the 2- and 5-year probability of treated kidney failure (dialysis or transplantation) for a potential patient with stage 3 to 5 CKD | https://kidneyfailurerisk.com. (accessed on 24 January 2024) [51] |
| eGFR Calculator (NKF) | CKD care teams | App for estimating kidney function that has five sperate eGFR calculators:
| https://www.kidney.org/apps/professionals/egfr-calculator (accessed on 24 January 2024) [52] |
| Kidney Disease for Health Professionals (NIDDK) | CKD care teams | Online resource for information about
| https://www.niddk.nih.gov/health-information/professionals/clinical-tools-patient-management/kidney-disease (accessed on 24 January 2024) [53] |
| Relative Risk, Monitoring and Referral in Patients with CKD (NKF) | CKD care teams |
| https://www.kidney.org/apps/professionals/relative-risk-monitoring-and-referral-patients-ckd (accessed on 24 January 2024) [54] |
| KDOQI App (NKF) | CKD care teams | App that can be used to access guidelines and commentaries | https://www.kidney.org/apps/professionals/kdoqi-app (accessed on 24 January 2024) [55] |
| United States Renal Data System (NIDDK) | Medical researchers and CKD care teams | Online, national data system that collects, analyzes, and distributes information about CKD and ESRD in the United States | https://www.niddk.nih.gov/about-niddk/strategic-plans-reports/usrds (accessed on 24 January 2024) [56] |
| Chronic Kidney Disease Risk Calculators (CDC) | Medical researchers and CKD care teams | Online risk calculators for
| https://nccd.cdc.gov/ckd/Calculators.aspx (accessed on 24 January 2024) [57] |
| Medication Therapy Management | CKD care teams |
| https://doi.org/10.2215/CJN.06790617 (accessed on 24 January 2024) [58] https://doi.org/10.1053/j.ackd.2014.02.011 (accessed on 24 January 2024) [59] https://doi.org/10.1053/j.ajkd.2021.05.023 (accessed on 24 January 2024) [60] https://doi.org/10.1186/s12882-016-0279-6 (accessed on 24 January 2024) [61] |
| Category | Example | Implementation into Routine Care |
|---|---|---|
| Multidisciplinary collaboration | ||
| “At Ochsner, primary care groups meet for weekly care huddles, sharing clinical information regularly to exchange ways to best care for their patients.” | Conduct regularly scheduled multidisciplinary meetings | |
| “University of Pittsburgh Medical Center [UPMC] has raised the priority of CKD within the leadership of the health system by undergoing a partnership to improve CKD care from a population health perspective. The approach has included a large, multidisciplinary care team to manage patients, including nephrologists, pharmacists, PCPs, educators, social workers, dieticians, etc.” | Ensure all stakeholders are included in CKD population health management | |
| “There are numerous health systems within major cities; therefore, it is not uncommon for patients to see multiple doctors within multiple health systems. This often leads to important patient information not being shared across systems, and as a result, gaps in care.” | Develop a method/database to ensure sharing of clinical information, including EHR interoperability, with easy access for all providers in the health system | |
| Diagnosis and Management of CKD | ||
| “The nephrologists at Yale don’t have the bandwidth to see patients that have an eGFR of <80; typically, the referral to the nephrologist doesn’t happen until a patient is on or nearing dialysis.” | Education of primary care providers for appropriate CKD management strategies | |
| “By intervening in the early stages of CKD, we can reduce the number of patients who go on dialysis—this would be a major cost-saving opportunity.” | Earlier identification of CKD and initiation of appropriate therapeutic strategies to slow or prevent progression of CKD | |
| “Our health system currently estimates a patient’s GFR; however, there is an opportunity to better integrate it into population health efforts to support downstream interventions.” “UPMC has also implemented the Tangri KFRE to create a risk profile. And, once they’ve identified the highest-risk patients, they automatically enroll them into the program, where the PCPs get an e-consult, and the patient receives all the ancillary services.” | Develop institutional algorithm for CKD identification and risk assessment to trigger appropriate consultations | |
| “At Geisinger, there is a referral alert in place to refer a patient to a nephrologist when they are diagnosed with stage 4 CKD, but the alert is not put in at earlier stages of CKD. The alert was put in place to triage later-stage CKD, as the nephrologist does not have the ability to see all patients with CKD in the health system.” | Set up automatic alerts for referrals at clinical threshold, but also educate primary care provider for CKD management strategies | |
| Other | ||
| “UPMC has built out a CKD registry in Epic, which currently contains approximately 80,000 patients across CKD stages 3, 4, and 5.” | Develop institution registry and create awareness so that patients can be appropriately managed | |
| “Dialysis patients have now become eligible for Medicare Advantage plans.” | Ensure enrollment into Medicare Advantage for eligible patients | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hirsch, J.S.; Danna, S.C.; Desai, N.; Gluckman, T.J.; Jhamb, M.; Newlin, K.; Pellechio, B.; Elbedewe, A.; Norfolk, E. Optimizing Care Delivery in Patients with Chronic Kidney Disease in the United States: Proceedings of a Multidisciplinary Roundtable Discussion and Literature Review. J. Clin. Med. 2024, 13, 1206. https://doi.org/10.3390/jcm13051206
Hirsch JS, Danna SC, Desai N, Gluckman TJ, Jhamb M, Newlin K, Pellechio B, Elbedewe A, Norfolk E. Optimizing Care Delivery in Patients with Chronic Kidney Disease in the United States: Proceedings of a Multidisciplinary Roundtable Discussion and Literature Review. Journal of Clinical Medicine. 2024; 13(5):1206. https://doi.org/10.3390/jcm13051206
Chicago/Turabian StyleHirsch, Jamie S., Samuel Colby Danna, Nihar Desai, Ty J. Gluckman, Manisha Jhamb, Kim Newlin, Bob Pellechio, Ahlam Elbedewe, and Evan Norfolk. 2024. "Optimizing Care Delivery in Patients with Chronic Kidney Disease in the United States: Proceedings of a Multidisciplinary Roundtable Discussion and Literature Review" Journal of Clinical Medicine 13, no. 5: 1206. https://doi.org/10.3390/jcm13051206