
Creatinine-Based Definition of Kidney Disease in the Charlson Comorbidity Index May Underestimate Prognosis in Males Compared to an Estimated Glomerular Filtration Rate Definition

Abstract
:1. Introduction
2. Methods
2.1. Study Design and Patient Selection
2.2. Chronic Kidney Disease
2.3. Charlson Comorbidity Index and Other Definitions
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
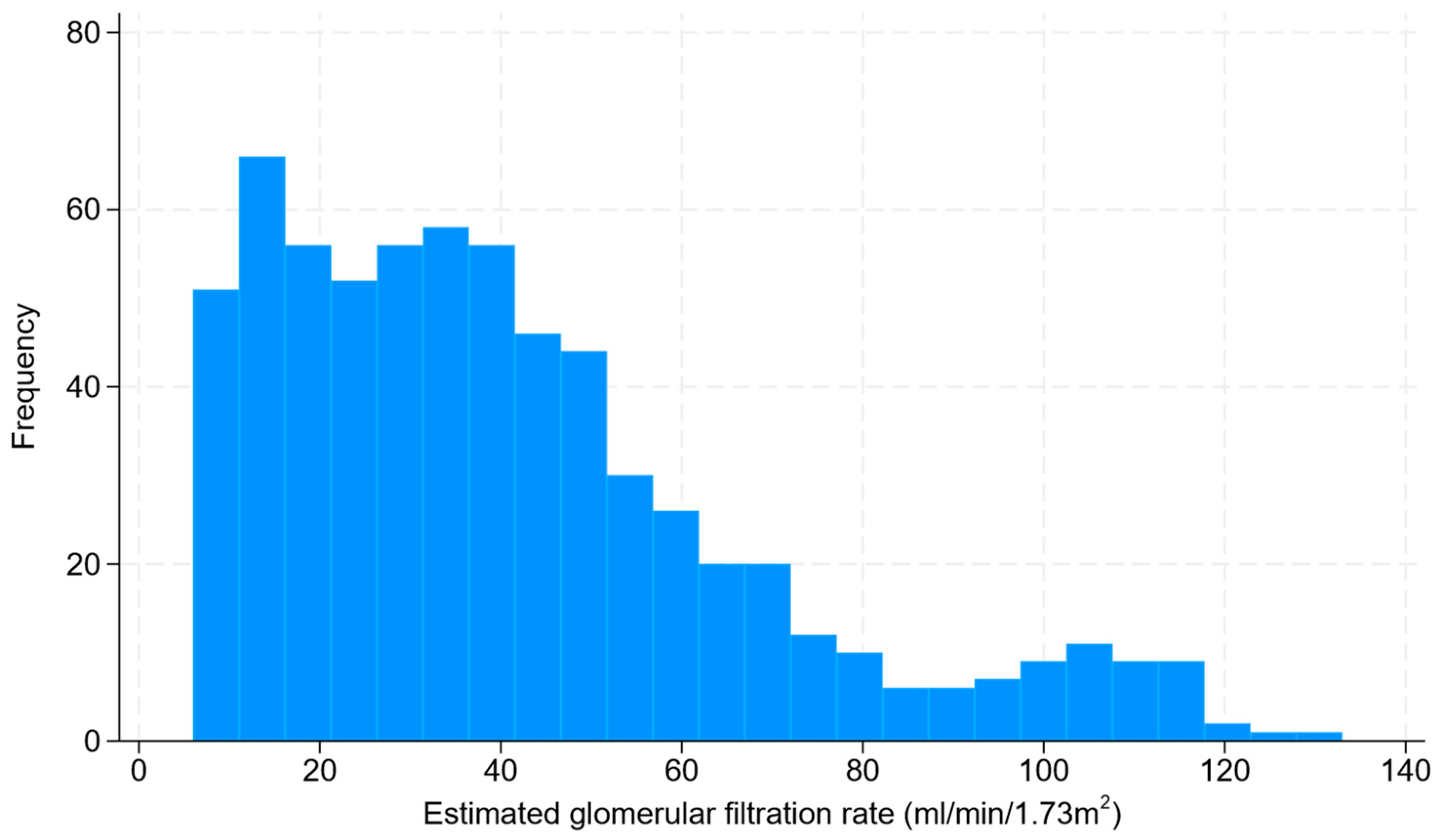
3.2. Chronic Kidney Disease
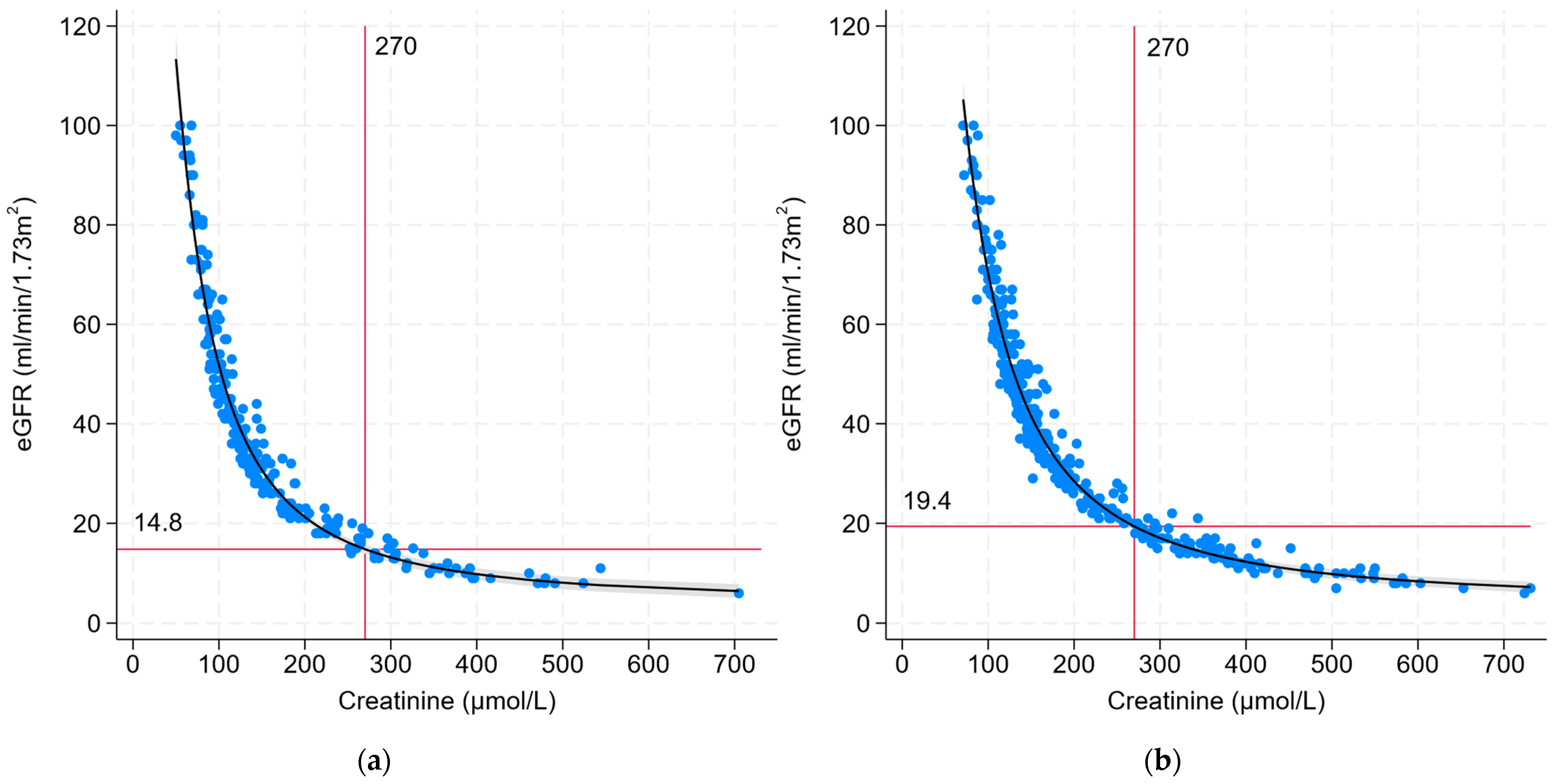
3.3. Correlation between eGFR and Creatinine
3.4. Charlson Index and Survival Estimates by CKD Definition
4. Discussion
4.1. Strengths and Limitations
4.2. Implications for Clinical Practice
4.3. Research Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Comorbidity | Points |
|---|---|
| Age: 50–59 years | +1 |
| Age: 60–69 years | +2 |
| Age: 70–79 years | +3 |
| Age: ≥80 years | +4 |
| Prior myocardial infarction | +1 |
| Congestive heart failure | +1 |
| Peripheral vascular disease | +1 |
| Stroke or transient ischemic attack | +1 |
| Dementia | +1 |
| Chronic pulmonary disease | +1 |
| Connective tissue disease | +1 |
| Peptic ulcer disease | +1 |
| Liver disease: Mild | +1 |
| Liver disease: Moderate–severe | +3 |
| Diabetes: uncomplicated | +1 |
| Diabetes: End-organ damage | +2 |
| Hemiplegia or paraplegia | +2 |
| Chronic kidney disease | +2 |
| Solid tumor: Localized | +2 |
| Solid tumor: Metastatic | +6 |
| Leukemia | +2 |
| Lymphoma | +2 |
| AIDS | +6 |
References
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Charlson, M.E.; Carrozzino, D.; Guidi, J.; Patierno, C. Charlson Comorbidity Index: A Critical Review of Clinimetric Properties. Psychother. Psychosom. 2022, 91, 8–35. [Google Scholar] [CrossRef]
- Jiang, L.; Chou, A.C.C.; Nadkarni, N.; Ng, C.E.Q.; Chong, Y.S.; Howe, T.S.; Koh, J.S.B. Charlson Comorbidity Index Predicts 5-Year Survivorship of Surgically Treated Hip Fracture Patients. Geriatr. Orthop. Surg. Rehabil. 2018, 9, 2151459318806442. [Google Scholar] [CrossRef] [PubMed]
- Schmolders, J.; Friedrich, M.J.; Michel, R.; Strauss, A.C.; Wimmer, M.D.; Randau, T.M.; Pennekamp, P.H.; Wirtz, D.C.; Gravius, S. Validation of the Charlson comorbidity index in patients undergoing revision total hip arthroplasty. Int. Orthop. 2015, 39, 1771–1777. [Google Scholar] [CrossRef]
- St-Louis, E.; Iqbal, S.; Feldman, L.S.; Sudarshan, M.; Deckelbaum, D.L.; Razek, T.S.; Khwaja, K.M. Using the age-adjusted Charlson comorbidity index to predict outcomes in emergency general surgery. J. Trauma Acute Care Surg. 2015, 78, 318–323. [Google Scholar] [CrossRef]
- Di Iorio, B.; Cillo, N.; Cirillo, M.; De Santo, N.G. Charlson Comorbidity Index is a predictor of outcomes in incident hemodialysis patients and correlates with phase angle and hospitalization. Int. J. Artif. Organs 2004, 27, 330–336. [Google Scholar] [CrossRef]
- Wu, P.-H.; Lin, Y.-T.; Lee, T.-C.; Lin, M.-Y.; Kuo, M.-C.; Chiu, Y.-W.; Hwang, S.-J.; Chen, H.-C. Predicting mortality of incident dialysis patients in Taiwan—A longitudinal population-based study. PLoS ONE 2013, 8, e61930. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.; Bernardini, J.; Piraino, B. Charlson comorbidity index as a predictor of outcomes in incident peritoneal dialysis patients. Am. J. Kidney Dis. 2001, 37, 337–342. [Google Scholar] [CrossRef]
- Lin, Y.; Yang, C.; Chu, H.; Wu, J.; Lin, K.; Shi, Y.; Wang, H.; Kong, G.; Zhang, L.; China Kidney Disease Network Working Group. Association between the Charlson Comorbidity Index and the risk of 30-day unplanned readmission in patients receiving maintenance dialysis. BMC Nephrol. 2019, 20, 363. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Becker, C.; Inker, L.A. Glomerular filtration rate and albuminuria for detection and staging of acute and chronic kidney disease in adults: A systematic review. JAMA 2015, 313, 837–846. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Inter. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Inker, L.A.; Eneanya, N.D.; Coresh, J.; Tighiouart, H.; Wang, D.; Sang, Y.; Crews, D.C.; Doria, A.; Estrella, M.M.; Froissart, M.; et al. New Creatinine- and Cystatin C-Based Equations to Estimate GFR without Race. N. Engl. J. Med. 2021, 385, 1737–1749. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 5–14. [Google Scholar] [CrossRef]
- Kidney Health Australia. eGFR Calculator; Kidney Health Australia: Melbourne, Australia, 2020; Available online: https://kidney.org.au/health-professionals/egfr-calculator (accessed on 10 November 2023).
- MDCalc. Charlson Comorbidity Index (CCI). Available online: https://www.mdcalc.com/calc/3917/charlson-comorbidity-index-cci (accessed on 10 November 2023).
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Volk, M.L.; Hernandez, J.C.; Lok, A.S.; Marrero, J.A. Modified Charlson comorbidity index for predicting survival after liver transplantation. Liver Transpl. 2007, 13, 1515–1520. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.; Kim, M.H.; Kim, H.J.; Park, J.Y.; Ryu, D.R.; Lee, H.; Lee, J.P.; Lim, C.S.; Kim, K.H.; Oh, K.H.; et al. Development and Validation of the Modified Charlson Comorbidity Index in Incident Peritoneal Dialysis Patients: A National Population-Based Approach. Perit. Dial. Int. 2017, 37, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Koseki, Y.; Hikage, M.; Fujiya, K.; Kamiya, S.; Tanizawa, Y.; Bando, E.; Terashima, M. Utility of a modified age-adjusted Charlson Comorbidity Index in predicting cause-specific survival among patients with gastric cancer. Eur. J. Surg. Oncol. 2021, 47, 2010–2015. [Google Scholar] [CrossRef]
- Kirwan, C.J.; Philips, B.J.; Macphee, I.A. Estimated glomerular filtration rate correlates poorly with four-hour creatinine clearance in critically ill patients with acute kidney injury. Crit. Care Res. Pract. 2013, 2013, 406075. [Google Scholar] [CrossRef] [PubMed]
- Bragadottir, G.; Redfors, B.; Ricksten, S.E. Assessing glomerular filtration rate (GFR) in critically ill patients with acute kidney injury—True GFR versus urinary creatinine clearance and estimating equations. Crit. Care 2013, 17, R108. [Google Scholar] [CrossRef]
- Rothberg, A.E.; McEwen, L.N.; Herman, W.H. Severe obesity and the impact of medical weight loss on estimated glomerular filtration rate. PLoS ONE 2020, 15, e0228984. [Google Scholar] [CrossRef]
- Lemoine, S.; Guebre-Egziabher, F.; Sens, F.; Nguyen-Tu, M.S.; Juillard, L.; Dubourg, L.; Hadj-Aissa, A. Accuracy of GFR estimation in obese patients. Clin. J. Am. Soc. Nephrol. 2014, 9, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, K.; Mahmoodi, B.K.; Woodward, M.; Emberson, J.R.; Jafar, T.H.; Jee, S.H.; Polkinghorne, K.R.; Shankar, A.; Smith, D.H.; Tonelli, M.; et al. Chronic Kidney Disease Prognosis Consortium. Comparison of risk prediction using the CKD-EPI equation and the MDRD study equation for estimated glomerular filtration rate. JAMA 2012, 307, 1941–1951. [Google Scholar] [CrossRef] [PubMed]


| Characteristics and Comorbidities | Total (N = 664) | Male (n = 386) | Female (n = 278) |
|---|---|---|---|
| Age in years, median (IQR) | 68 (54–76) | 69 (55–76) | 65 (52–77) |
| Obesity, n (%) [1] | 242 (42.1) | 136 (39.9) | 106 (45.3) |
| Diabetes mellitus, n (%) | 320 (48.1) | 193 (50.0) | 127 (45.7) |
| Ischemic heart disease, n (%) [2] | 158 (23.8) | 119 (30.8) | 39 (14.0) |
| Heart failure, n (%) | 117 (17.6) | 73 (18.9) | 44 (15.8) |
| Chronic lung disease, n (%) | 67 (10.1) | 43 (11.1) | 24 (8.6) |
| Chronic liver disease, n (%) | 28 (4.2) | 14 (3.6) | 14 (5.0) |
| Stroke or transient ischemic attack, n (%) | 64 (9.6) | 42 (10.9) | 22 (7.9) |
| Peripheral vascular disease, n (%) [2] | 48 (7.2) | 41 (10.6) | 7 (2.5) |
| Dementia, n (%) | 13 (2.0) | 8 (2.1) | 5 (1.8) |
| Connective tissue disease, n (%) | 36 (5.4) | 19 (4.9) | 17 (6.1) |
| Solid tumors, n (%) [2] | 40 (6.0) | 33 (8.6) | 7 (2.5) |
| Charlson chronic kidney disease, n (%) [2] | 141 (21.2) | 105 (27.2) | 36 (13.0) |
| Charlson index score, mean (SD) [2] | 4.3 (2.6) | 4.7 (2.7) | 3.7 (2.4) |
| Chronic Kidney Disease Stage | Total (N = 664) | Male (n = 386) | Female (n = 278) |
|---|---|---|---|
| 1. eGFR ≥ 90, n (%) | 55 (8.3) | 21 (5.4) | 34 (12.2) |
| 2. eGFR 60–89, n (%) | 79 (11.9) | 49 (12.7) | 30 (10.8) |
| 3. eGFR 30–59, n (%) | 273 (41.1) | 163 (42.1) | 110 (39.6) |
| 4. eGFR 15–29, n (%) | 171 (25.8) | 99 (25.7) | 72 (25.9) |
| 5. eGFR < 15, n (%) | 86 (13.0) | 54 (14.0) | 32 (11.5) |
| Serum creatinine, median (IQR) [1] | 149 (112–236) | 161 (125–280) | 128 (92–190) |
| eGFR, median (IQR) | 36 (21–54) | 36 (20–52) | 36 (22–57) |
| Albuminuria | |||
| Normal (<3.4 mg/mmol), n (%) | 188 (28.4) | 86 (22.4) | 102 (36.7) |
| Mild/moderate (3.4–34 mg/mmol), n (%) | 204 (30.8) | 121 (31.5) | 83 (29.9) |
| Heavy/severe (>34 mg/mmol), n (%) | 270 (40.8) | 177 (46.1) | 93 (33.5) |
| Etiology | |||
| Diabetes mellitus, n (%) | 244 (36.8) | 154 (39.9) | 90 (32.4) |
| Hypertensive nephrosclerosis, n (%) | 119 (17.9) | 52 (13.5) | 67 (24.1) |
| Glomerulonephritis or glomerulopathy, n (%) | 80 (12.1) | 49 (12.7) | 31 (11.2) |
| Renovascular disease, n (%) | 69 (10.4) | 43 (11.1) | 26 (9.4) |
| Obstructive uropathy, n (%) | 36 (5.4) | 26 (6.7) | 10 (3.6) |
| Polycystic kidney disease, n (%) | 23 (3.5) | 13 (3.4) | 10 (3.6) |
| Interstitial nephritis/nephrotoxins, n (%) | 14 (2.1) | 8 (2.1) | 6 (2.2) |
| Severe/recurrent acute kidney injury, n (%) | 12 (1.8) | 10 (2.6) | 2 (0.7) |
| Nephrectomy/single kidney, n (%) | 12 (1.8) | 6 (1.6) | 6 (2.2) |
| Congenital/reflux nephropathy, n (%) | 11 (1.7) | 6 (1.6) | 5 (1.8) |
| Nephrocalcinosis, n (%) | 9 (1.4) | 1 (0.3) | 8 (2.9) |
| Unclear or others, n (%) | 35 (5.3) | 18 (4.7) | 17 (6.1) |
| Model | Coefficients (95% CI) | Powers [1] | R2 |
|---|---|---|---|
| All patients, including sex variable | Creatinine_1 = 59.0 (57.5–60.5) | −2 | 0.94 |
| Creatinine_2 = 45.4 (42.4–48.4) | −2 | ||
| Male sex = 10.9 (10.0–11.8) | |||
| Female only | Creatinine_1 = 47.5 (45.5–49.5) | −2 | 0.96 |
| Creatinine_2 = 29.2 (25.6–32.7) | −2 | ||
| Male only | Creatinine_1 = 65.9 (64.3–67.5) | −2 | 0.96 |
| Creatinine_2 = 43.9 (38.4–49.3) | −2 |
| Male (n = 374) | Female (n = 254) | |
|---|---|---|
| Mean % (95% CI) | Mean % (95% CI) | |
| 10-year survival (creatinine-based) | 37.7 (33.7, 41.7) | 48.2 (43.6, 52.9) |
| 10-year survival (eGFR-based) | 41.4 (37.4, 45.4) | 48.6 (43.9, 53.2) |
| Difference in 10-year survival | 3.7 (2.5, 4.9) p < 0.001 | 0.3 (0.1, 0.8) p = 0.13 |
| Male (n = 51) | Female (n = 6) | |
|---|---|---|
| Mean % (95% CI) | Mean % (95% CI) | |
| 10-year survival (creatinine-based) | 20.0 (11.3, 28.6) | 63.7 (20.0, 100) |
| 10-year survival (eGFR-based) | 47.1 (36.8, 57.3) | 78.4 (37.2, 100) |
| Difference in 10-year survival | 27.1 (21.1, 33.0) p < 0.001 | 14.8 (−6.7, 36.3) p = 0.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, A.K.H.; Kerr, P.G. Creatinine-Based Definition of Kidney Disease in the Charlson Comorbidity Index May Underestimate Prognosis in Males Compared to an Estimated Glomerular Filtration Rate Definition. J. Clin. Med. 2024, 13, 1007. https://doi.org/10.3390/jcm13041007
Lim AKH, Kerr PG. Creatinine-Based Definition of Kidney Disease in the Charlson Comorbidity Index May Underestimate Prognosis in Males Compared to an Estimated Glomerular Filtration Rate Definition. Journal of Clinical Medicine. 2024; 13(4):1007. https://doi.org/10.3390/jcm13041007
Chicago/Turabian StyleLim, Andy K. H., and Peter G. Kerr. 2024. "Creatinine-Based Definition of Kidney Disease in the Charlson Comorbidity Index May Underestimate Prognosis in Males Compared to an Estimated Glomerular Filtration Rate Definition" Journal of Clinical Medicine 13, no. 4: 1007. https://doi.org/10.3390/jcm13041007