
Cortical Thickness Index and Canal Calcar Ratio: A Comparison of Proximal Femoral Fractures and Non-Fractured Femora in Octogenarians to Centenarians
Abstract
:1. Introduction
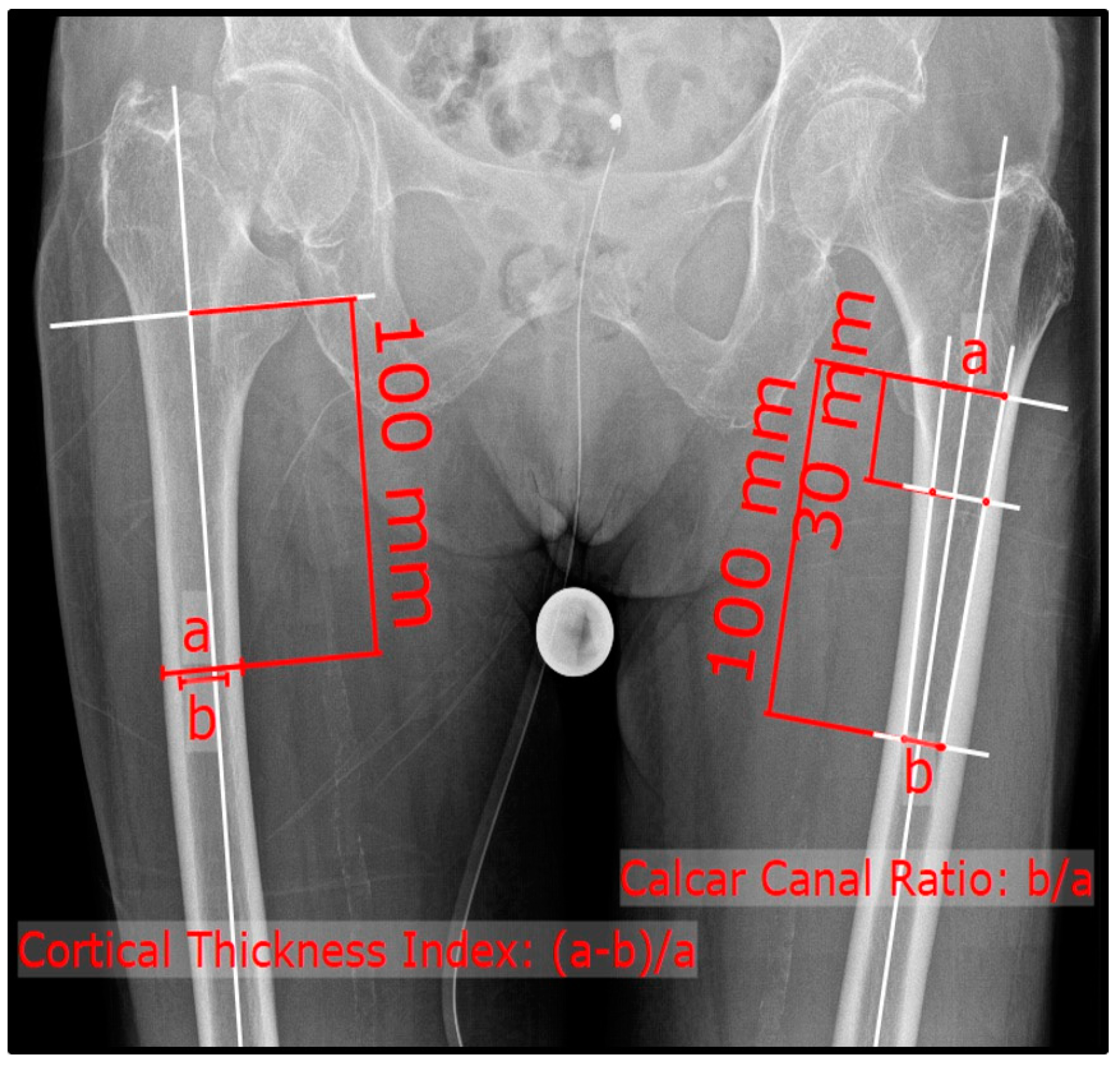
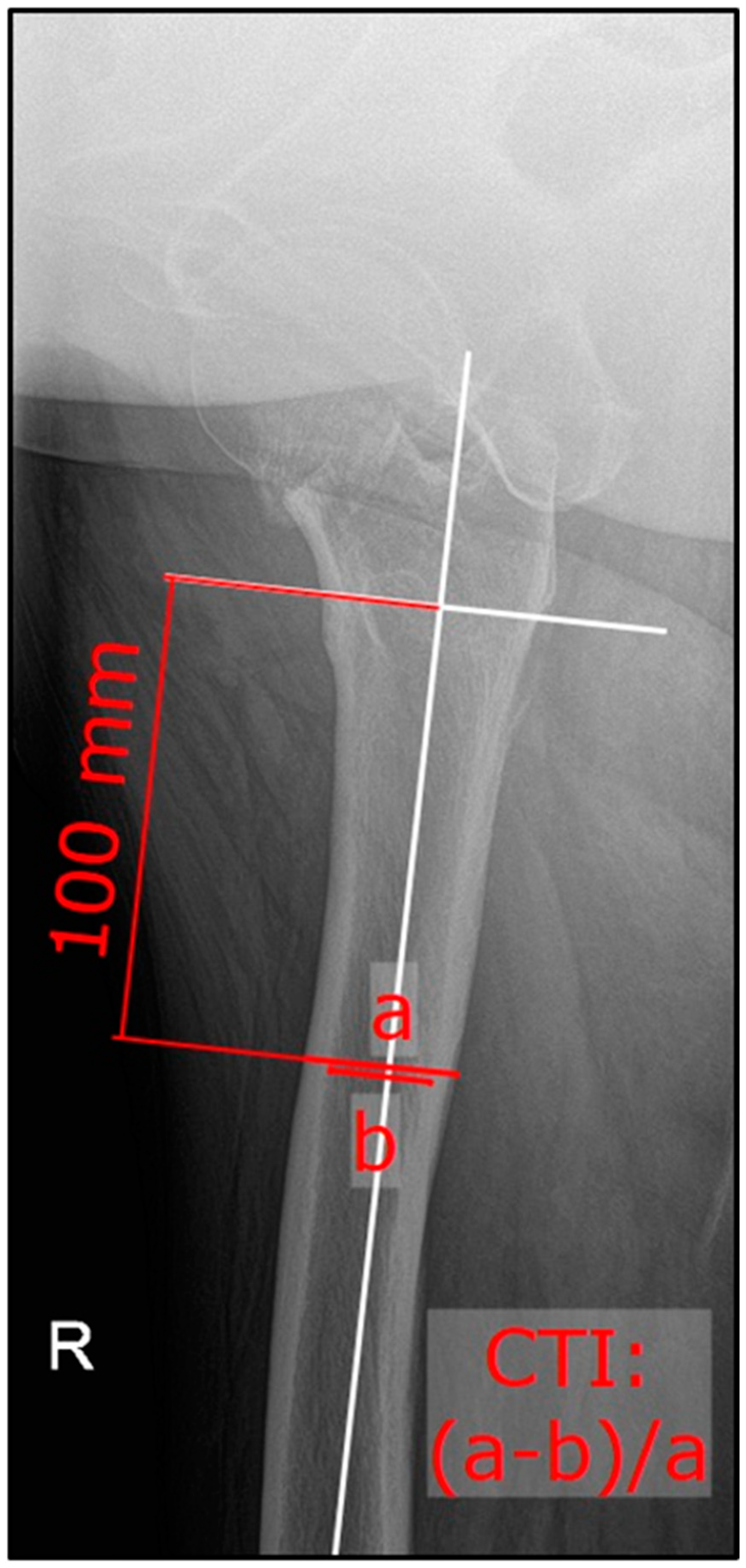
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Patient Demographic Characteristics
3.2. Inter-Rater Reliability
3.3. Comparison of CTI and CCR within the Sub-Groups
3.4. Analysis of Gender-Specific Differences within the Sub-Groups
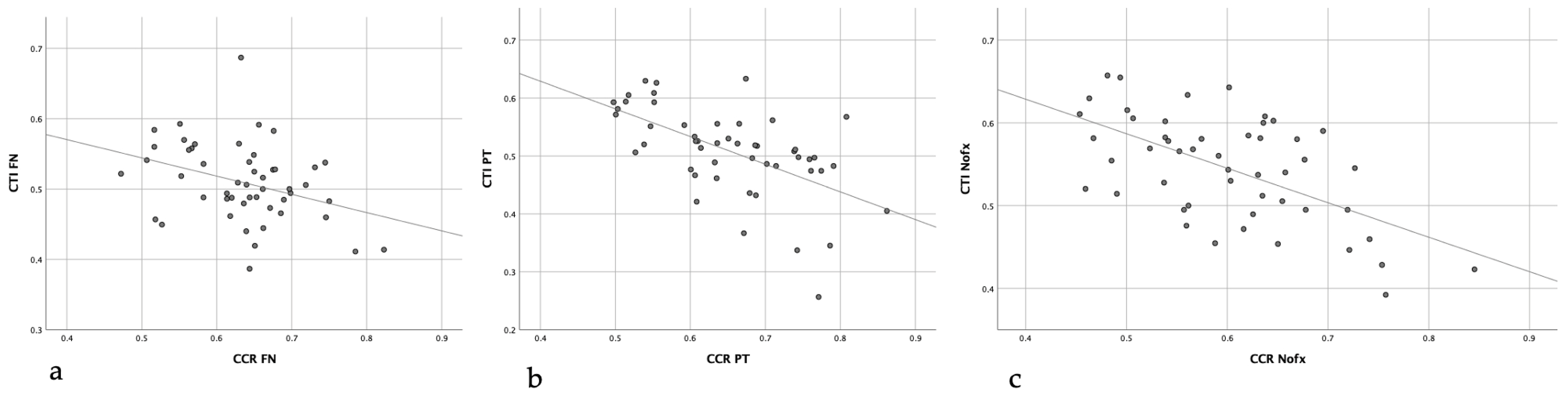
3.5. Correlations between CTI and CCR within the Sub-Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sambrook, P.; Cooper, C. Osteoporosis. Lancet 2006, 367, 2010–2018. [Google Scholar] [CrossRef]
- Cooper, C.; Melton, L.J. Epidemiology of osteoporosis. Trends Endocrinol. Metab. 1992, 3, 224–229. [Google Scholar] [CrossRef]
- Keene, G.S.; Parker, M.J.; Pryor, G.A. Mortality and morbidity after hip fractures. BMJ 1993, 307, 1248–1250. [Google Scholar] [CrossRef] [PubMed]
- Gullberg, B.; Johnell, O.; Kanis, J.A. World-wide Projections for Hip Fracture. Osteoporos. Int. 1997, 7, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Dyer, S.M.; Crotty, M.; Fairhall, N.; Magaziner, J.; Beaupre, L.A.; Cameron, I.D.; Sherrington, C. A critical review of the long-term disability outcomes following hip fracture. BMC Geriatr. 2016, 16, 158. [Google Scholar] [CrossRef] [PubMed]
- Guzon-Illescas, O.; Fernandez, E.P.; Villarias, N.C.; Donate, F.J.Q.; Peña, M.; Alonso-Blas, C.; García-Vadillo, A.; Mazzucchelli, R. Mortality after osteoporotic hip fracture: Incidence, trends, and associated factors. J. Orthop. Surg. Res. 2019, 14, 203. [Google Scholar] [CrossRef] [PubMed]
- Cree, M.; Soskolne, C.L.; Belseck, E.; Hornig, J.; McElhaney, J.E.; Brant, R.; Suarez-Almazor, M. Mortality and institutionalization following hip fracture. J. Am. Geriatr. Soc. 2000, 48, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Burge, R.; Dawson-Hughes, B.; Solomon, D.H.; Wong, J.B.; King, A.; Tosteson, A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J. Bone Miner. Res. 2007, 22, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Guilley, E.; Herrmann, F.; Rapin, C.-H.; Hoffmeyer, P.; Rizzoli, R.; Chevalley, T. Socioeconomic and living conditions are determinants of hip fracture incidence and age occurrence among community-dwelling elderly. Osteoporos. Int. 2011, 22, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Birge, S.J.; Morrow-Howell, N.; Proctor, E.K. Hip Fracture. Clin. Geriatr. Med. 1994, 10, 589–609. [Google Scholar] [CrossRef]
- Grisso, J.A.; Kelsey, J.L.; Strom, B.L.; O’Brien, L.A.; Maislin, G.; LaPann, K.; Samelson, L.; Hoffman, S. Risk Factors for Hip Fracture in Black Women. N. Engl. J. Med. 1994, 330, 1555–1559. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.; Sambrook, P.; Kelly, P.; Jones, G.; Lord, S.; Freund, J.; Eisman, J. Prediction of osteoporotic fractures by postural instability and bone density. Br. Med. J. 1993, 307, 1111–1115. [Google Scholar] [CrossRef] [PubMed]
- Hui, S.L.; Slemenda, C.W.; Johnston, C.C. Age and bone mass as predictors of fracture in a prospective study. J. Clin. Investig. 1988, 81, 1804–1809. [Google Scholar] [CrossRef]
- Consensus development conference: Diagnosis, prophylaxis, and treatment of osteoporosis. Am. J. Med. 1993, 94, 646–650. [CrossRef] [PubMed]
- Faulkner, K.A.; Chan, B.K.S.; Cauley, J.A.; Marshall, L.M.; Ensrud, K.E.; Stefanick, M.L.; Orwoll, E.S. Histories including number of falls may improve risk prediction for certain non-vertebral fractures in older men. Inj. Prev. 2009, 15, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Nazarian, A.; Muller, J.; Zurakowski, D.; Müller, R.; Snyder, B.D. Densitometric, morphometric and mechanical distributions in the human proximal femur. J. Biomech. 2007, 40, 2573–2579. [Google Scholar] [CrossRef]
- Pellegrini, A.; Tacci, F.; Leigheb, M.; Costantino, C.; Pedrazzini, A.; Pedrazzi, G.; Vaienti, E.; Ceccarelli, F.; Pogliacomi, F. Injuries of the trochanteric region: Can analysis of radiographic indices help in prediction of recurrent osteoporotic hip fractures? Acta Biomed. 2017, 88, 43–49. [Google Scholar]
- Wang, Z.; Tutaworn, T.; Wishman, M.D.; Levin, J.E.; Hentschel, I.G.; Lane, J.M. Fracture Risk Assessment Tool Scores and Radiographical Bone Measurements in Total Hip Arthroplasty Patients. J. Arthroplasty 2022, 37, 2381–2386. [Google Scholar] [CrossRef]
- Sah, A.P.; Thornhill, T.S.; LeBoff, M.S.; Glowacki, J. Correlation of Plain Radiographic Indices of the Hip with Quantitative Bone Mineral Density. Osteoporos. Int. 2007, 18, 1119–1126. [Google Scholar] [CrossRef]
- Dorr, L.D.; Faugere, M.-C.; Mackel, A.M.; Gruen, T.A.; Bognar, B.; Malluche, H.H. Structural and cellular assessment of bone quality of proximal femur. Bone 1993, 14, 231–242. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Köse, Ö.; Kiliçaslan, Ö.F.; Arik, H.O.; Sarp, Ü.; Toslak, I.E.; Uçar, M.; Başaran, S.; Evlice, A.; Erdem, M.; Demirkıran, M. Prediction of osteoporosis through radiographic assessment of proximal femoral morphology and texture in elderly; is it valid and reliable? Turk. Osteoporoz Derg. 2015, 21, 46–52. [Google Scholar] [CrossRef]
- Faundez, J.; Carmona, M.; Klaber, I.; Zamora, T.; Botello, E.; Schweitzer, D. Radiographic Assessment of Bone Quality Using 4 Radiographic Indexes: Canal Diaphysis Ratio Is Superior. J. Arthroplasty 2024, 39, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Ilyas, G.; Ipci, F.B. Evaluation of the Relationship between Osteoporosis Parameters in Plain Hip Radiography and DXA Results in 156 Patients at a Single Center in Turkey. Diagnostics 2023, 13, 2519. [Google Scholar] [CrossRef] [PubMed]
- Bäcker, H.C.; Wu, C.H.; Maniglio, M.; Wittekindt, S.; Hardt, S.; Perka, C. Epidemiology of proximal femoral fractures. J. Clin. Orthop. Trauma 2021, 12, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Baumgärtner, R.; Heeren, N.; Quast, D.; Babst, R.; Brunner, A. Is the cortical thickness index a valid parameter to assess bone mineral density in geriatric patients with hip fractures? Arch. Orthop. Trauma Surg. 2015, 135, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Nash, W.; Harris, A. The Dorr type and cortical thickness index of the proximal femur for predicting peri-operative complications during hemiarthroplasty. J. Orthop. Surg. 2014, 22, 92–95. [Google Scholar] [CrossRef]
- Avulapati, S.K.; Boddu, S.; Bajjuri, A.; Konka, S.K.C.; Koneru, S. Cortical thickness index (CTI): Can it influence type of hip fracture in proximal femur? Int. J. Orthop. Sci. 2020, 6, 1114–1118. [Google Scholar] [CrossRef]
- Pothong, W.; Adulkasem, N. Comparative evaluation of radiographic morphologic parameters for predicting subsequent contralateral fragility hip fracture. Int. Orthop. 2023, 47, 1837–1843. [Google Scholar] [CrossRef]
- Kanis, J.A.; Johnell, O.; Oden, A.; Johansson, H.; McCloskey, E. FRAXTM and the assessment of fracture probability in men and women from the UK. Osteoporos. Int. 2008, 19, 385–397. [Google Scholar] [CrossRef]
- Nguyen, B.N.; Hoshino, H.; Togawa, D.; Matsuyama, Y. Cortical thickness index of the proximal femur: A radiographic parameter for preliminary assessment of bone mineral density and osteoporosis status in the age 50 years and over population. CiOS Clin. Orthop. Surg. 2018, 10, 149–156. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Femoral Neck Fracture | Trochanteric Fracture | Non-Fracture |
|---|---|---|---|
| Number of Patients | 50 | 50 | 50 |
| Gender, n (%) | |||
| female | 36 (72) | 42 (84) | 31 (62) |
| male | 14 (28) | 8 (16) | 19 (38) |
| Age | 92.4 ± 2.4 | 91.7 ± 3.8 | 87.7 ± 4.7 |
| Affected side, n (%) | |||
| left | 19 (38) | 19 (38) | 24 (48) |
| right | 31 (62) | 31 (62) | 26 (52) |
| Fractured/Measured | Non-Fractured | p-Value | |
|---|---|---|---|
| ap CTI * | |||
| FNFx | 0.434 ± 0.08 | 0.509 ± 0.06 | <0.001 |
| TFx | 0.451 ± 0.09 | 0.508 ± 0.08 | <0.001 |
| NFx | 0.545 ± 0.06 | 0.548 ± 0.07 | 0.527 |
| lateral CTI * | |||
| FNFx | 0.417 ± 0.07 | ||
| TFx | 0.416 ± 0.06 | ||
| NFx | 0.458 ± 0.08 | ||
| CCR * | |||
| FNFx | 0.735 ± 0.11 | 0.636 ± 0.08 | <0.001 |
| TFx | 0.770 ± 0.17 | 0.653 ± 0.09 | <0.001 |
| NFx | 0.6 ± 0.09 | 0.592 ± 0.1 | 0.291 |
| Female | Male | p-Value | |
|---|---|---|---|
| ap CTI * | |||
| FNFx | |||
| fractured | 0.422 ± 0.08 | 0.463 ± 0.1 | 0.128 |
| non-fractured | 0.503 ± 0.05 | 0.525 ± 0.07 | 0.199 |
| TFx | |||
| fractured | 0.453 ± 0.08 | 0.439 ± 0.09 | 0.290 |
| NFx | |||
| measured | 0.53 ± 0.07 | 0.57 ± 0.05 | 0.031 |
| contralateral | 0.53 ± 0.07 | 0.57 ± 0.05 | 0.030 |
| lateral CTI * | |||
| FNFx | 0.401 ± 0.06 | 0.457 ± 0.08 | 0.022 |
| TFx | 0.404 ± 0.06 | 0.451 ± 0.06 | 0.603 |
| NFx | 0.437 ± 0.08 | 0.491 ± 0.08 | 0.021 |
| CCR * | |||
| FNFx | 0.741 ± 0.1 | 0.721 ± 0.1 | 0.554 |
| TFx | 0.656 ± 0.9 | 0.638 ± 0.1 | 0.653 |
| NFx | 0.622 ± 0.1 | 0.565 ± 0.7 | 0.029 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guyan, F.; Gianduzzo, E.; Waltenspül, M.; Dietrich, M.; Kabelitz, M. Cortical Thickness Index and Canal Calcar Ratio: A Comparison of Proximal Femoral Fractures and Non-Fractured Femora in Octogenarians to Centenarians. J. Clin. Med. 2024, 13, 981. https://doi.org/10.3390/jcm13040981
Guyan F, Gianduzzo E, Waltenspül M, Dietrich M, Kabelitz M. Cortical Thickness Index and Canal Calcar Ratio: A Comparison of Proximal Femoral Fractures and Non-Fractured Femora in Octogenarians to Centenarians. Journal of Clinical Medicine. 2024; 13(4):981. https://doi.org/10.3390/jcm13040981
Chicago/Turabian StyleGuyan, Flurina, Estelle Gianduzzo, Manuel Waltenspül, Michael Dietrich, and Method Kabelitz. 2024. "Cortical Thickness Index and Canal Calcar Ratio: A Comparison of Proximal Femoral Fractures and Non-Fractured Femora in Octogenarians to Centenarians" Journal of Clinical Medicine 13, no. 4: 981. https://doi.org/10.3390/jcm13040981