
Detection of Alpha-1 Antitrypsin Levels in Chronic Obstructive Pulmonary Disease in Respiratory Clinics in Spain: Results of the EPOCONSUL 2021 Audit
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Characteristics of the Participating Hospitals and Resources of the Respiratory Units and Their Association with AAT Testing
3.2. Clinical Characteristics of the Audited Cases and Their Association with AAT Testing
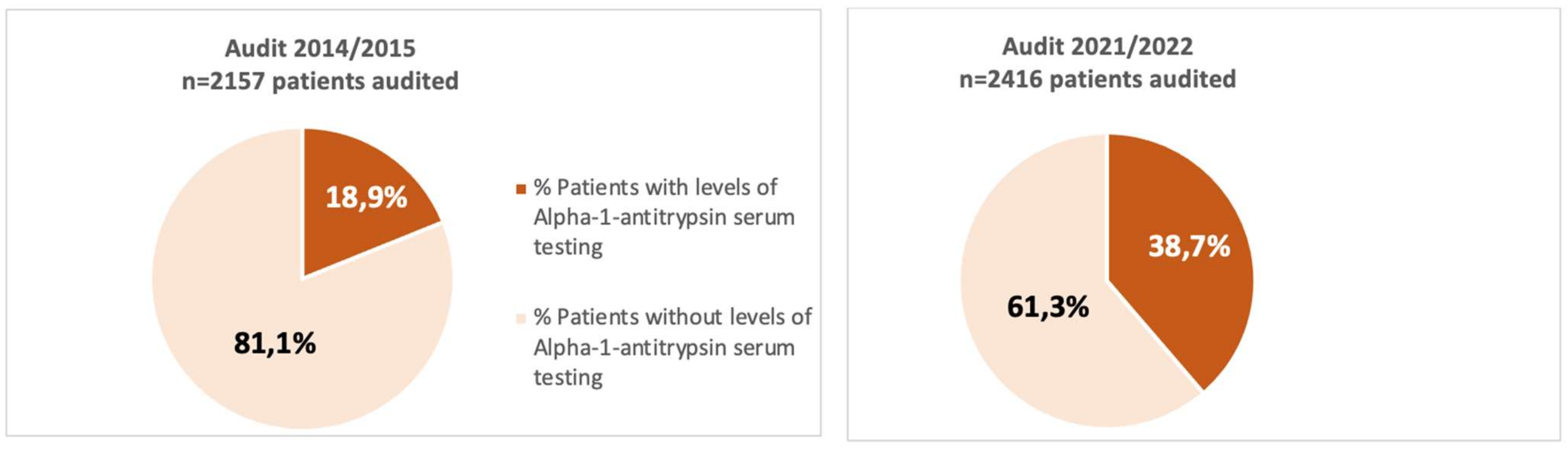
3.3. Variations in Testing AAT between the 2 Audits
3.4. Clinical Characteristics of Patients According to AAT Levels and Procedures Conducted for COPD Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stoller, J.K.; Aboussouan, L.S. Alpha1-antitrypsin deficiency. Lancet 2005, 365, 2225–2236. [Google Scholar] [CrossRef] [PubMed]
- Stoller, J.K.; Aboussouan, L.S. A review of α1-antitrypsin deficiency. Am. J. Respir. Crit. Care Med. 2012, 185, 246–259. [Google Scholar] [CrossRef] [PubMed]
- Silverman, E.K.; Sandhaus, R.A. Clinical practice. Alpha1-antitrypsin deficiency. N. Engl. J. Med. 2009, 360, 2749–2757. [Google Scholar] [CrossRef] [PubMed]
- Blanco, I.; Diego, I.; Castañón, C.; Bueno, P.; Miravitlles, M. Estimated Worldwide Prevalence of the PI*ZZ Alpha-1 Antitrypsin Genotype in Subjects with Chronic Obstructive Pulmonary Disease. Arch. Bronconeumol. 2023, 59, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Stoller, J.K. Detecting Alpha-1 Antitrypsin Deficiency. Ann. Am. Thorac. Soc. 2016, 13 (Suppl. S4), S317–S325. [Google Scholar] [CrossRef]
- Stoller, J.K.; Strange, C.; Schwarz, L.; Kallstrom, T.J.; Chatburn, R.L. Detection of alpha-1 antitrypsin deficiency by respiratory therapists: Experience with an educational program. Respir. Care 2014, 59, 667–672. [Google Scholar] [CrossRef]
- De Serres, F.J.; Blanco, I. Prevalence of α1-antitrypsin deficiency alleles PI*S and PI*Z worldwide and effective screening for each of the five phenotypic classes PI*MS, PI*MZ, PI*SS, PI*SZ, and PI*ZZ: A comprehensive review. Ther. Adv. Respir. Dis. 2012, 6, 277–295. [Google Scholar] [CrossRef]
- Tsechkovski, M.; Boulyjenkov, V.; Heuck, C. Alpha1-antitrypsin deficiency: Memorandum from a WHO meeting. Bull. World Health Organ. 1997, 75, 397–415. [Google Scholar]
- Miravitlles, M.; Calle, M.; Molina, J.; Almagro, P.; Gómez, J.T.; Trigueros, J.A.; Cosío, B.G.; Casanova, C.; López-Camposb, J.L.; Riescob, J.A.; et al. Spanish COPD Guidelines (GesEPOC) 2021: Up-dated Pharmacological treatment of stable COPD. Arch. Bronconeumol. 2022, 58, 69–81. [Google Scholar] [CrossRef]
- Stoller, J.K.; Snider, G.L.; Brantly, M.L.; Fallat, R.J.; Stockley, R.A.; Turino, G.M.; Konietzko, N.; Dirksen, A.; Eden, E.; Luisetti, M.; et al. American Thoracic Society/European Respiratory Society Statement: Standards for the diagnosis and management of in-di-viduals with alpha1-antitrypsin deficiency. Am. J. Respir. Crit. Care Med. 2003, 168, 818–900. [Google Scholar]
- Miravitlles, M.; Dirksen, A.; Ferrarotti, I.; Koblizek, V.; Lange, P.; Mahadeva, R.; McElvaney, N.G.; Parr, D.; Piitulainen, E.; Roche, N.; et al. European Respiratory Society statement: Di-agnosis and treatment of pulmonary disease in α1-antitrypsin deficiency. Eur. Respir. J. 2017, 50, 1700610. [Google Scholar] [CrossRef] [PubMed]
- Stoller, J.K.; Brantly, M. The challenge of detecting alpha-1 antitrypsindeficiency. J. Chronic Obstr. Pulm. Dis 2013, 10 (Suppl. S1), 26–34. [Google Scholar] [CrossRef] [PubMed]
- Halpin, D.M.G. Clinical Management of COPD in the Real World: Can Studies Reveal Errors in Management and Pathways to Improve Patient Care? Pragmat. Obs. Res. 2023, 14, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.; Roberts, M. National cohort data from Sweden to the National COPD audit in England and Wales: Grand designs for quality improvement. Prim. Care Respir. J. 2014, 23, 7–8. [Google Scholar] [CrossRef] [PubMed]
- Calle Rubio, M.; López-Campos, J.L.; Miravitlles, M.; Soler Cataluña, J.J.; Alcázar Navarrete, B.; Fuentes Ferrer, M.E.; Hermosa, J.L.R. Variations in Chronic Obstructive Pulmonary Disease Outpatient Care in Respiratory Clinics: Results from the 2021 EPOCONSUL Audit. Arch. Bronconeumol. 2023, 59, 295–304. [Google Scholar] [CrossRef]
- Calle Rubio, M.; Soriano, J.B.; López-Campos, J.L.; Soler-Cataluña, J.J.; Alcázar Navarrete, B.; Rodríguez González-Moro, J.M.; Miravitlles, M.; Barrecheguren, M.; Fuentes Ferrer, M.E.; Rodriguez Hermosa, J.L.; et al. Testing for alpha-1 antitrypsin in COPD in outpatient respiratory clinics in Spain: A multilevel, cross-sectional analysis of the EPOCONSUL study. PLoS ONE 2018, 13, e0198777. [Google Scholar] [CrossRef]
- Miravitlles, M.; Herr, C.; Ferrarotti, I.; Jardi, R.; Rodriguez-Frias, F.; Luisetti, M.; Bals, R. Laboratory testing of individuals with severe alpha1-antitrypsin deficiency in three European centres. Eur. Respir. J. 2010, 35, 960–968. [Google Scholar] [CrossRef]
- Chapman, K.R.; Burdon, J.G.W.; Piitulainen, E.; Sandhaus, R.A.; Seersholm, N.; Stocks, J.M.; Stoel, B.C.; Huang, L.; Yao, Z.; Edelman, J.M.; et al. Intravenous augmentation treatment and lung density in severe α1 antitrypsin deficiency (RAPID): A randomised, double-blind, placebocontrolled trial. Lancet 2015, 386, 360–368. [Google Scholar] [CrossRef]
- Tejwani, V.; Nowacki, A.S.; Fye, E.; Sanders, C.; Stoller, J.K. The Impact of Delayed Diagnosis of Alpha-1 Antitrypsin Deficiency: The Association between Diagnostic Delay and Worsened Clinical Status. Respir. Care 2019, 64, 915–922. [Google Scholar] [CrossRef]
- Campos, M.A.; Wanner, A.; Zhang, G.; Sandhaus, R.A. Trends in the Diagnosis of Symptomatic Patients with alpha1 -Antitrypsin Deficiency Between 1968 and 2003. Chest 2005, 128, 1179–1186. [Google Scholar] [CrossRef]
- Köhnlein, T.; Janciauskiene, S.; Welte, T. Diagnostic delay and clinical modifiers in alpha-1 antitrypsin deficiency. Ther. Adv. Respir. Dis. 2010, 4, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Greulich, T.; Ottaviani, S.; Bals, R.; Lepper, P.M.; Vogelmeier, C.; Luisetti, M.; Ferrarotti, I. Alpha1-antitrypsin deficiency—Diagnostic testing and disease awareness in Germany and Italy. Respir. Med. 2013, 107, 1400–1408. [Google Scholar] [CrossRef]
- Greulich, T.; Vogelmeier, C.F. Alpha-1-antitrypsin deficiency: Increasing awareness and improving diagnosis. Ther. Adv. Respir. Dis. 2015, 10, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Chorostowska-Wynimko, J. Targeted screening programmes in COPD: How to identify individuals with α1-antitrypsin defi-ciency. Eur. Respir. Rev. 2015, 24, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Casas, F.; Blanco, I.; Martínez, M.T.; Bustamante, A.; Miravitlles, M.; Cadenas, S.; Hernández, J.M.; Lázaro, L.; Rodríguez, E.; Rodríguez-Frías, F.; et al. Indications for active case searches and intra-venous alpha-1 antitrypsin treatment for patients with alpha-1 antitrypsin deficiency chronic obstructive pulmonary disease: An update. Arch. Bronconeumol. 2015, 51, 185–192. [Google Scholar] [CrossRef]
- McElvaney, N.G. Diagnosing α1-antitrypsin deficiency: How to improve the current algorithm. Eur. Respir. Rev. 2015, 24, 52–57. [Google Scholar] [CrossRef]
- Lopez-Campos, J.L.; Casas-Maldonado, F.; Torres-Duran, M.; Medina-Gonzálvez, A.; Rodriguez-Fidalgo, M.L.; Carrascosa, I.; Calle, M.; Osaba, L.; Rapun, N.; Drobnic, E.; et al. Results of a Diagnostic Procedure Based on Multiplex Technology on Dried Blood Spots and Buccal Swabs for Subjects with Sus-pected Alpha1 Antitrypsin Deficiency. Arch. Bronconeumol. 2021, 57, 42–50. [Google Scholar] [CrossRef]
- O’brien, M.E.; Pennycooke, K.; Carroll, T.P.; Shum, J.; Fee, L.T.; O’Connor, C.; Logan, P.M.; Reeves, E.P.; McElvaney, N.G. The Impact of Smoke Exposure on the Clinical Phenotype of Alpha-1 Antitrypsin Deficiency in Ireland: Exploiting a National Registry to Understand a Rare Disease. J. Chronic Obstr. Pulm. Dis. 2015, 12, 2–9. [Google Scholar] [CrossRef]
- Parr, D.G.; Guest, P.G.; Reynolds, J.H.; Dowson, L.J.; Stockley, R.A. Prevalence and Impact of Bronchiectasis in alpha1-Antitrypsin Deficiency. Am. J. Respir. Crit. Care Med. 2007, 176, 1215–1221. [Google Scholar] [CrossRef]
- Ward, H.; Turner, A.M.; Stockley, R.A. Spirometric and gas transfer discordance in alpha-1 antitrypsin deficiency; patient charac-teristics and progression. Chest 2014, 145, 1316–1324. [Google Scholar] [CrossRef]
- Campos, M.A.; Alazemi, S.; Zhang, G.; Salathe, M.; Wanner, A.; Sandhaus, R.A.; Baier, H. Clinical characteristics of subjects with symptoms of alpha1-antitrypsin deficiency older than 60 years. Chest 2009, 135, 600–608. [Google Scholar] [CrossRef]
- Blanco, I.; Bueno, P.; Diego, I.; Pérez-Holanda, S.; Casas-Maldonado, F.; Esquinas, C.; Miravitlles, M. Alpha-1 antitrypsin Pi*Z gene frequency and Pi*ZZ genotype numbers worldwide: An update. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Brantly, M.; Campos, M.; Davis, A.M.; D’armiento, J.; Goodman, K.; Hanna, K.; O’day, M.; Queenan, J.; Sandhaus, R.; Stoller, J.; et al. Detection of alpha-1 antitrypsin deficiency: The past, present and future. Orphanet J. Rare Dis. 2020, 15, 96. [Google Scholar] [CrossRef] [PubMed]
- Da Costa, C.H.; Noronha Filho, A.J.; Marques, E.S.R.M.F.; da Cruz, T.F.; de Oliveira Monteiro, V.; Pio, M.; Rufino, R.L. Alpha 1-antitrypsin deficiency in patients with chronic obstructive pulmonary disease patients: Is systematic screening necessary? BMC Res. Notes 2019, 12, 10. [Google Scholar] [CrossRef]
- Sorroche, P.B.; Acquier, M.F.; Jove, O.L.; Giugno, E.; Pace, S.; Livellara, B.; Legal, S.; Oyhamburu, J.; Saez, M.S. Alpha-1 Antitrypsin Deficiency in COPD Patients: A Cross-Sectional Study. Arch. Bronconeumol. 2015, 51, 539–543. [Google Scholar] [CrossRef]
- Tejwani, V.; Stoller, J.K. The spectrum of clinical sequelae associated with alpha-1 antitrypsin deficiency. Ther. Adv. Chronic Dis. 2021, 12, 2040622321995691. [Google Scholar] [CrossRef]
- Fregonese, L.; Stolk, J. Hereditary alpha-1-antitrypsin deficiency and its clinical consequences. Orphanet J. Rare Dis. 2008, 3, 16. [Google Scholar] [CrossRef]
- Bradi, A.C.; Audisho, N.; Casey, D.K.; Chapman, K.R. Alpha-1 Antitrypsin Deficiency in Canada: Regional Disparities in Diagnosis and Management. COPD J. Chronic Obstr. Pulm. Dis. 2015, 12 (Suppl. S1), 15–21. [Google Scholar] [CrossRef] [PubMed]
- Annunziata, A.; Ferrarotti, I.; Coppola, A.; Lanza, M.; Imitazione, P.; Spinelli, S.; Di Micco, P.; Fiorentino, G. Alpha-1 Antitrypsin Screening in a Selected Cohort of Patients Affected by Chronic Pulmonary Diseases in Naples, Italy. J. Clin. Med. 2021, 10, 1546. [Google Scholar] [CrossRef]
- Greulich, T.; Nell, C.; Herr, C.; Vogelmeier, C.; Kotke, V.; Wiedmann, S.; Wencker, M.; Bals, R.; Koczulla, A.R. Results from a large targeted screening program for alpha-1-antitrypsin deficiency: 2003–2015. Orphanet J. Rare Dis. 2016, 11, 71. [Google Scholar] [CrossRef]
- Horváth, I.; Canotilho, M.; Chlumský, J.; Chorostowska-Wynimko, J.; Corda, L.; Derom, E.; Ficker, J.H.; Kneussl, M.; Miravitlles, M.; Sucena, M.; et al. Diagnosis and management of α1-antitrypsin deficiency in Europe: An expert survey. ERJ Open Res. 2019, 5, 00171–02018. [Google Scholar] [CrossRef] [PubMed]
- Ingebrigtsen, T.S.; Marott, J.L.; Rode, L.; Vestbo, J.; Lange, P.; Nordestgaard, B.G. Fibrinogen and α1-antitrypsin in COPD exacerbations. Thorax 2015, 70, 1014–1021. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
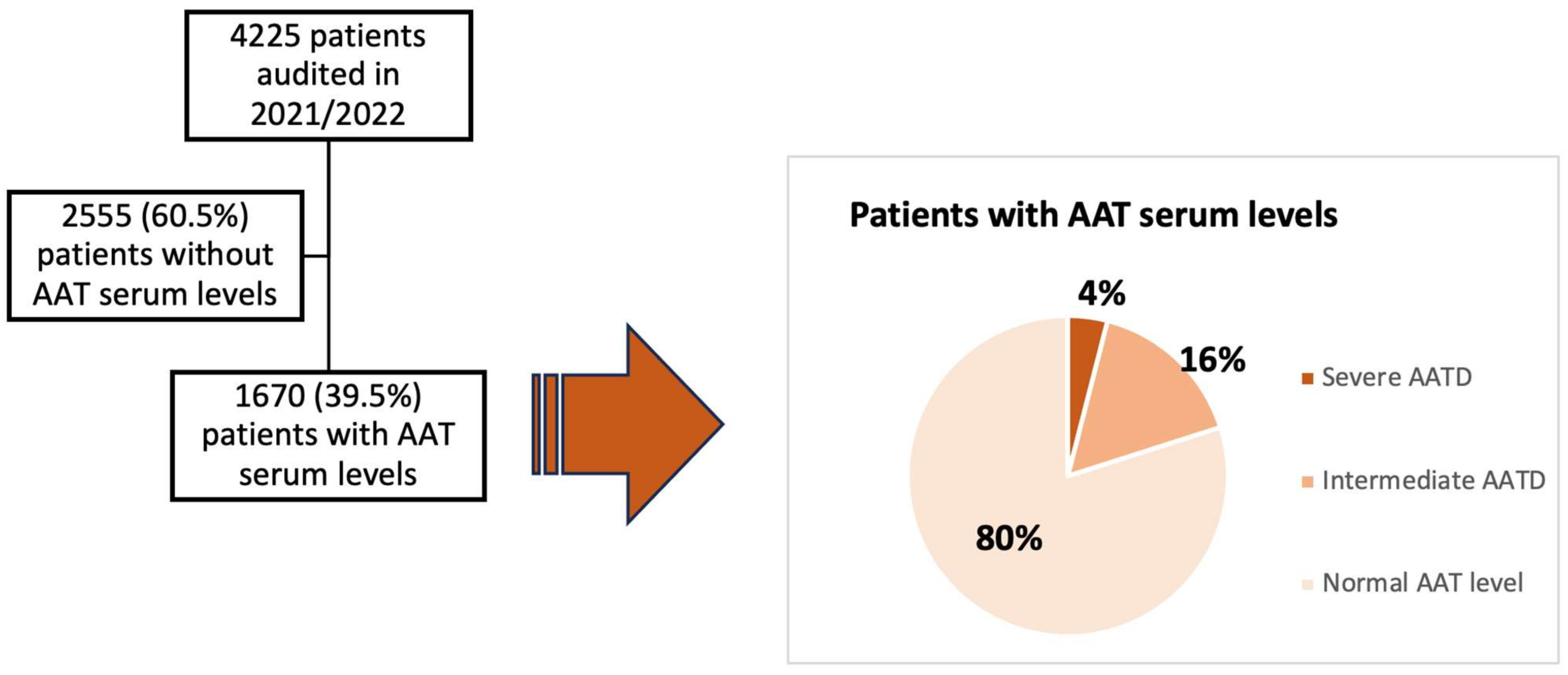
| All Patients (n = 4.225) | AAT Levels Test n = 1670 (39.5%) | AAT Levels Not Tested n = 2555 (60.5%) | OR (95%CI) | p | |
|---|---|---|---|---|---|
| Hospital complexity level, n (%) | |||||
| Level II (reference) | 1 | ||||
| Level III | 3271 (77.4) | 1255 (75.1) | 2016 (78.9) | 0.80 (0.43–1.49) | 0.499 |
| University hospital, n (%) | |||||
| No (reference) | 1 | ||||
| Yes | 3593 (85) | 1412 (84.6) | 2181 (85.4) | 0.93 (0.47–1.84) | 0.853 |
| Minutes at outpatient respiratory visit available, n (%) | |||||
| <15 min (reference) | 1 | ||||
| ≥15 min | 2258 (53.4) | 979 (58.6) | 1279 (50.1) | 1.41 (0.85–2.32) | 0.173 |
| Genotyping of AATD availability, n (%) | |||||
| Not available (reference) | 1 | ||||
| Yes | 3750 (88.8) | 1426 (85.4) | 2324 (91) | 0.58 80.35–0.94) | 0.030 |
| Specialized COPD outpatient clinic available, n (%) | |||||
| Not available (reference) | 1 | ||||
| Yes | 2729 (64.6) | 1076 (64.4) | 1653 (64.7) | 0.98 (0.58–1.66) | 0.965 |
| Outpatient respiratory nursing clinic availability, n (%) | |||||
| Not (reference) | 1 | ||||
| Yes | 2373 (56.2) | 969 (58) | 1404 (55) | 1.13 (0.67–1.88) | 0.632 |
| Written COPD protocol available, n (%) | |||||
| Not available (reference) | 1 | ||||
| Yes | 1747 (41.3) | 761 (45.6) | 986 (38.6) | 1.33 (0.78–2.25) | 0.286 |
| Attended in specialized COPD outpatient clinic, n (%) | |||||
| Not available (reference) | 1 | ||||
| Yes | 1620 (38.5) | 757 (45.5) | 863 (33.9) | 1.63 (1.04–2.55) | 0.032 |
| All Patients (n = 4.225) | Patients with Levels of AAT n = 1670 (39.5%) | Patients without Levels of AAT n = 2555 (60.5%) | OR (95%CI) | p | |
|---|---|---|---|---|---|
| Sex, n (%) | |||||
| Male (reference) | 1 | ||||
| Female | 1152 (27.2) | 498 (29.8) | 654 (25.5) | 1.23 (1.04–1.47) | 0.016 |
| Age (years), m (SD) | 70.0 (9.3) | 67.9 (8.9) | 71.3 (9.2) | 0.96 (0.94–0.97) | <0.001 |
| >55, (n, %) (reference) | 1 | ||||
| ≤55, (n, %) | 268 (6.3) | 150 (9) | 118 (4.6) | 2.03 (1.36–3.04) | 0.001 |
| IPA (×10 Pack-years), m (SD) | 49.6 (24.0) | 48.9 (23.1) | 50.1 (24.6) | 0.99 (0.99–1.00) | 0.368 |
| Active smokers, n (%) | |||||
| No (reference) | 1 | ||||
| Yes | 1053 (24.9) | 439 (26.3) | 614 (24) | 1.12 (0.91–1.38) | 0.225 |
| BMI kg/m2, m (SD) | 27.8 (5.6) | 27.1 (5.6) | 28.3 (5.6) | 0.96 (0.95–0.97) | 0.001 |
| >21 (n, %) (reference) | 1 | ||||
| ≤21 (n, %) | 364 (9.1) | 172 (10.6) | 192 (8.1) | 1.33 (1.02–1.74) | 0.031 |
| Charlson index, n (%) | |||||
| <3 (reference) | 1 | ||||
| ≥3 | 1185 (28.1) | 388 (23.3) | 797 (31.2) | 0.66 (0.54–0.81) | <0.001 |
| Dyspnea (MRC-m), n (%) | |||||
| <2 (reference) | 1 | ||||
| ≥2 | 1787 (56) | 746 (54.8) | 1041 (56.9) | 0.91 (0.70–1.189 | 0.512 |
| Chronic bronchitis criteria, n (%) | |||||
| Not (reference) | 1 | ||||
| Yes | 1298 (30.7) | 552 (33.1) | 746 (29.2) | 1.19 (0.89–1.599 | 0.217 |
| History of asthma, n (%) | |||||
| Not (reference) | |||||
| Yes | 411 (9.7) | 211 (12.6) | 200 (7.8) | 1.70 (1.11–2.60) | 0.014 |
| FEV1 (%predicted post-BD), m (SD) ≥ 80, | 53.1 (18.5) | 50.7 (18.1) | 54.7 (18.6) | 0.98 (0.98–0.99). | <0.001 |
| n (%) (reference) | 346 (8.2) | 96 (5.8) | 250 (9.8) | 1 | |
| 50–79%, n (%) | 1952 (46.3) | 727 (43.6) | 1225 (48) | 1.54 (1.13–2.10) | 0.006 |
| <50%, n (%) | 1992 (45.5) | 846 (50.7) | 1076 (42.2) | 2.04 (1.48–2.82) | <0.001 |
| GesEPOC Phenotype, n (%) | |||||
| Non-exacerbator (reference) | 1226 (46.2) | 515 (43.3) | 711 (48.5) | 1 | |
| Exacerbator with chronic bronchitis | 446 (16.8) | 190 (16) | 256 (17.5) | 1.02 (0.71−1.8) | 0.893 |
| Exacerbator with emphysema | 570 (21.5) | 279 (23.4) | 291 (19.8) | 1.32 (0.94−1.8) | 0.101 |
| Asthma-COPD | 414 (15.6) | 206 (17.3) | 208 (14.2) | 1.36 (0.93−1.9) | 0.103 |
| Number of hospital admissions in the last year, n (%) | |||||
| <1 (reference) | 1 | ||||
| ≥1 | 692 (16.4) | 316 (18.9) | 376 (14.7) | 1.35 (1.03−1.76) | 0.025 |
| Chronic colonization, n (%) | |||||
| Not (reference) | 1 | ||||
| Yes | 494 (11.7) | 227 (13.6) | 267 (10.5) | 1.34 (0.83−2.17) | 0.219 |
| Triple therapy, n (%) | |||||
| Not (reference) | 1 | ||||
| Yes | 2034 (50.3) | 870 (54.3) | 1164 (47.7) | 1.30 (1.07−1.58) | 0.007 |
| Long-term oxygen therapy, n (%) | |||||
| Not (reference) | 1 | ||||
| Yes | 1059 (25.1) | 408 (24.4) | 651 (25.5) | 0.94 (0.76−1.16) | 0.601 |
| Home ventilation, n (%) | |||||
| Not (reference) | 1 | ||||
| Yes | 362 (8.6) | 125 (7.5) | 237 (9.3) | 0.79 (0.56−1.11) | 0.180 |
| Respiratory care follow-up (years), (median, IQR) | 5.8 (3.6−9.0) | 5.6 (3.5−8.8) | 6 (3.7−9.2) | 0.98 (0.95−1.00) | 0.185 |
| Variable | OR (95%CI) | p |
|---|---|---|
| Genotyping of AATD availability | ||
| Not (reference) | 1 | |
| Yes | 0.42 (0.26−0.68) | 0.001 |
| Attended in specialized COPD outpatient clinic | ||
| Not (reference) | 1 | |
| Yes | 1.88 (1.19−2.99) | 0.007 |
| %FEV1 postBD | ||
| ≥80% (reference) | 1 | |
| 50−79% | 1.50 (1.08−2.08) | 0.013 |
| <50% | 1.86 (1.36−2.55) | <0.001 |
| BMI kg/m2 | ||
| >21 (reference) | 1 | |
| ≤21 | 1.18 (0.91−1.53) | 0.193 |
| Age (years) | ||
| >55 (reference) | 1 | |
| ≤55 | 1.84 (1.18−2.85) | 0.007 |
| Gender | ||
| Male (reference) | 1 | |
| Female | 1.16 (0.97−1.40) | 0.101 |
| Number of hospital admissions in the last year | ||
| <1 (reference) | 1 | |
| ≥1 | 1.25 (0.96−1.64) | 0.093 |
| Charlson index | ||
| <3 (reference) | 1 | |
| ≥3 | 0.63 (0.52−0.76) | <0.001 |
| History of asthma | ||
| Not (reference) | 1 | |
| Yes | 1.53 (0.96−1.43) | 0.069 |
| Number of Participating Hospitals | Total Number of Patients Assessed in the Two Audits | % Patients with Levels of Alpha-1 Antitrypsin Serum Testing in Audit 2015 | % Patients with Levels of Alpha-1 Antitrypsin Serum Testing in Audit 2021 | OR (95 % CI) | p | Adjusted OR * (95 % CI) | p |
|---|---|---|---|---|---|---|---|
| 25 | 4573 | 408 (18.9) | 934 (38.7) | 2.70 (1.70−4.28) | <0.001 | 2.81 (1.63−4.84) | <0.001 |
Center and patient characteristics in the 2015 and 2021 audits of variables of interest for AAT testing in COPD | |||||||
| In Audit 2015 (n = 2157) | In Audit 2021 (n = 2416) | p | |||||
| Genotyping of AATD availability, n (%) | 1566 (72.6) | 2406 (99.6) | <0.001 | ||||
| Number of attendees in specialized COPD outpatient clinic, n (%) | 765 (35.5) | 1300 (53.9) | <0.001 | ||||
| %FEV1 postBD < 50%, n (%) | 658 (44.6) | 1196 (49.6) | 0.011 | ||||
| BMI (kg/m2) ≤ 21, n (%) | 156 (7.3) | 229 (10) | 0.001 | ||||
| Age (years) ≤ 55, n (%) | 184 (8.5) | 138 (5.7) | <0.001 | ||||
| Female, n (%) | 318 (14.7) | 685 (28.4) | <0.001 | ||||
| Number of hospital admissions in the last year ≥ 1, n (%) | 538 (24.9) | 380 (15.7) | <0.001 | ||||
| Charlson index ≥ 3, n (%) | 920 (42.7) | 666 (27.6) | <0.001 | ||||
| Have history or symptoms of asthma, n (%) | 540 (25) | 237 (9.8) | <0.001 | ||||
| Chronic bronchitis criteria, n (%) | 843 (39.1) | 661 (27.4) | <0.001 | ||||
| Home ventilation, n (%) | 177 (8.2) | 224 (9.3) | 0.111 | ||||
| Characteristics of the Patient Tested for AAT n = 1651 | Patients with AAT Level < 60 mg/dL n = 66 (4%) | Patients with AAT Level ≥ 60 and <116 mg/dL n = 265 (16%) | Patients with AAT Level ≥ 116 mg/dL n = 1320 (80%) | OR (95%CI) AAT Level ≥ 60 and <116 mg/dL vs. ≥116 mg/dL (Reference) | p | OR (95%CI) AAT Level < 60 mg/dL vs. ≥116 mg/dL (Reference) | p |
|---|---|---|---|---|---|---|---|
| AAT plasma level (mg/dL), m(SD) | 19.3 (14.6) | 98.9 (14.2) | 160.9 (58.0) | ||||
| Clinical characteristics | |||||||
| Age (years), m (SD) | 0.98 (0.96−0.99) | 0.99 (0.92−1.06) | 0.836 | ||||
| >55, (n, %) (reference) | 67.6 (11.4) | 66.7 (8.5) | 68.1 (8.8) | 1 | 0.015 | 1 | |
| ≤55, (n, %) | 12 (18.2) | 23 (8.7) | 114 (8.6) | 1.00 (0.61−1.63) | 0.985 | 2.34 (0.89−6.15) | 0.082 |
| Sex (female), (reference) | 1 | 1 | |||||
| Male n (%) | 49 (74.2) | 187 (70.6) | 919 (69.6) | 1.04 (0.77−1.41) | 0.772 | 1.25 (0.61−2.58) | 0.533 |
| Active smokers, n (%) | |||||||
| No (reference) | 1 | ||||||
| Yes | 12 (18.2) | 58 (21.9) | 364 (27.6) | 0.73 (0.45−1.18) | 0.206 | 0.58 (0.36−0.92) | 0.023 |
| IPA (Pack-years), m (SD) | 42.7 (19.9) | 47.7 (24) | 49.4 (23.1) | 0.99 (0.98−1.00) | 0.454 | 0.98 (0.96−1.00) | 0.192 |
| BMI kg/m2, m (SD) | 26.4 (4.0) | 27.5 (5.2) | 27.1 (5.8) | 0.6 (0.98−1.03) | 0.426 | 0.97 (0.93−1.01) | 0.174 |
| >21 n (%) (reference) | 1 | 1 | |||||
| ≤21 n (%) | 5 (7.7) | 23 (9.1) | 144 (11.2) | 0.79 (0.48−1.28) | 0.347 | 0.66 (0.18−2.42) | 0.536 |
| Dyspnea (MRC-m), n (%) | |||||||
| <2 (reference) | 1 | 1 | |||||
| ≥2 | 46 (75.4) | 109 (51.4%) | 584 (54.4) | 0.88 (0.64−1.21) | 0.457 | 2.56 (1.67−3.94) | <0.001 |
| Charlson index, n (%) | |||||||
| <3 (reference) | 1 | ||||||
| ≥3 | 24 (36.4) | 45 (17) | 315 (23.9) | 0.65 (0.46−0.91) | 0.012 | 1.81 (0.99−3.33) | 0.053 |
| Chronic bronchitis criteria, n (%) | |||||||
| Not (reference) | 1 | ||||||
| Yes | 27 (40.9) | 78 (29.4) | 439 (33.3) | 0.83 (0.61−1.14) | 0.260 | 1.38 (0.52−3.69) | 0.510 |
| History of asthma, n (%) | |||||||
| Not (reference) | 1 | ||||||
| Yes | 3 (4.5) | 35 (13.6) | 167 (12.8) | 1.07 (0.67−1.68) | 0.768 | 0.32 (0.06−1.65) | 0.176 |
| GesEPOC Phenotype, n (%) | |||||||
| Non-exacerbator (reference) | 18 (33.3) | 89 (48.4) | 404 (43) | 1 | 1 | ||
| Exacerbator chronic bronchitis | 21 (38.9) | 25 (13.6) | 141 (15) | 0.80 (0.42−1.52) | 0.504 | 3.34 (1.21−9.20) | 0.020 |
| Exacerbator with emphysema | 12 (22.2) | 36 (19.6) | 228 (24.3) | 0.71 (0.45−1.11) | 0.143 | 1.18 (0.66−2.09) | 0.560 |
| Asthma-COPD | 3 (5.6) | 34 (18.5) | 166 (17.7) | 0.92 (0.53−1.62) | 0.798 | 0.40 (0.13−1.18) | 0.098 |
| Number of hospital admissions in the last year, n (%) | |||||||
| <1 (reference) | 1 | 1 | |||||
| ≥1 | 25 (37.9) | 46 (17.4) | 240 (18.2) | 0.94 (0.65−1.35) | 0.761 | 2.74 (0.84−8.87) | 0.092 |
| FEV1 (%), m (SD) | 52.8 (16.8) | 51.5 (17.6) | 50.4 (18.4) | 0.6 (0.99−1.00) | 0.335 | 1.00 (0.99−1.02) | 0.411 |
| ≥80, n (%) (reference) | 31 (47) | 14 (5.3) | 78 (5.9) | 1 | 1 | ||
| 50–79%, n (%) | 31 (47) | 125 (47.2) | 562 (42.6) | 1.23 (0.63−2.41) | 0.914 | 1.07 (0.24−4.78) | 0.924 |
| <50%, n (%) | 4 (6.1) | 126 (47.5) | 679 (51.5) | 1.03 (0.56−1.89) | 0.528 | 0.89 (0.33−2.33) | 0.813 |
| BODE index, m (DE) | 3.8 (2.2) | 3.1 (2.2) | 4.0 (2.0) | 0.83 (0.74−0.93) | 0.003 | 0.95 (0.76−1.19) | 0.689 |
| Long-term oxygen therapy, n (%) | |||||||
| Not (reference) | 1 | 1 | |||||
| Yes | 18 (27.3) | 56 (21.1) | 329 (24.9) | 0.80 (0.60−1.07) | 0.149 | 1.12 (0.53−2.36) | 0.747 |
| Diagnostic procedures conducted during the follow-up for COPD evaluation | |||||||
| Diffusion capacity measured on any occasion, n (%) | |||||||
| Not (reference) | 1 | 1 | |||||
| Yes | 51 (77.3) | 265 (80.1) | 996 (75.5) | 1.36 (0.94−1.97) | 0.100 | 1.10 (0.56−2.16) | 0.769 |
| Lung volumes measured on any occasion, n (%) | |||||||
| Not (reference) | 1 | 1 | |||||
| Yes | 21 (31.8) | 790 (58.8) | 970 (58.8) | 1.00 (0.72−1.39) | 0.970 | 0.31 (0.09−1.00) | 0.051 |
| 6-min walk test carried out on any occasion, n (%) | |||||||
| Not (reference) | 1 | 1 | |||||
| Yes | 27 (40.9) | 786 (59.5) | 962 (58.3) | 0.87 (0.62−1.22) | 0.431 | 0.47 (0.09−2.34) | 0.358 |
| BODE index calculated on any occasion, n (%) | |||||||
| Not (reference) | 1 | 1 | |||||
| Yes | 17 (25.8) | 565 (42.8) | 699 (42.3) | 1.05 (0.77−1.44) | 0.733 | 0.46 (0.08−2.63) | 0.386 |
| Chest CT carried on any occasion, n (%) | |||||||
| Not (reference) | 1 | 1 | |||||
| Yes | 65 (98.5) | 1091 (82.7) | 1381 (83.6) | 1.18 (0.85−1.63) | 0.320 | 13.6 (1.36−136.0) | 0.026 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calle Rubio, M.; Miravitlles, M.; López-Campos, J.L.; Soler-Cataluña, J.J.; Alcazar Navarrete, B.; Fuentes-Ferrer, M.E.; Rodriguez Hermosa, J.L. Detection of Alpha-1 Antitrypsin Levels in Chronic Obstructive Pulmonary Disease in Respiratory Clinics in Spain: Results of the EPOCONSUL 2021 Audit. J. Clin. Med. 2024, 13, 955. https://doi.org/10.3390/jcm13040955
Calle Rubio M, Miravitlles M, López-Campos JL, Soler-Cataluña JJ, Alcazar Navarrete B, Fuentes-Ferrer ME, Rodriguez Hermosa JL. Detection of Alpha-1 Antitrypsin Levels in Chronic Obstructive Pulmonary Disease in Respiratory Clinics in Spain: Results of the EPOCONSUL 2021 Audit. Journal of Clinical Medicine. 2024; 13(4):955. https://doi.org/10.3390/jcm13040955
Chicago/Turabian StyleCalle Rubio, Myriam, Marc Miravitlles, José Luis López-Campos, Juan J. Soler-Cataluña, Bernardino Alcazar Navarrete, Manuel E. Fuentes-Ferrer, and Juan Luis Rodriguez Hermosa. 2024. "Detection of Alpha-1 Antitrypsin Levels in Chronic Obstructive Pulmonary Disease in Respiratory Clinics in Spain: Results of the EPOCONSUL 2021 Audit" Journal of Clinical Medicine 13, no. 4: 955. https://doi.org/10.3390/jcm13040955