
Diagnostic Infrared Thermography of the Tongue and Taste Perception in Patients with Oral Lichen Planus: Case-Control Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Subjective Evaluation of Symptoms
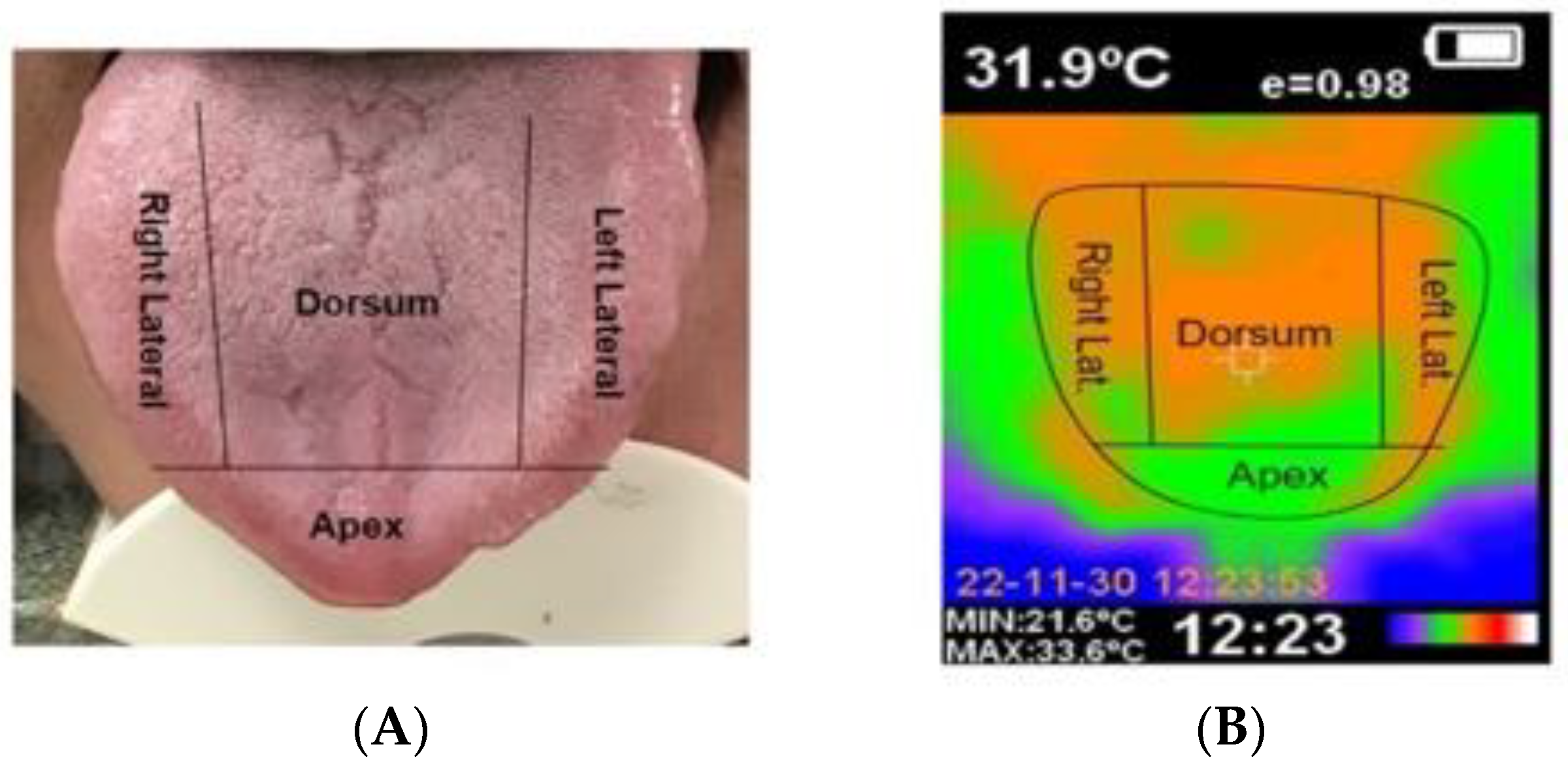
2.4. Recording of Thermographic Images
2.5. Statistical Analysis
3. Results
Study Sample
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Warnakulasuriya, S.; Kujan, O.; Aguirre-Urizar, J.M.; Bagan, J.V.; González-Moles, M.Á.; Kerr, A.R.; Lodi, G.; Mello, F.W.; Monteiro, L.; Ogden, G.R.; et al. Oral potentially malignant disorders: A consensus report from an international seminar on nomenclature and classification, convened by the WHO Collaborating Centre for Oral Cancer. Oral Dis. 2021, 27, 1862–1880. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S. Oral potentially malignant disorders: A comprehensive review on clinical aspects and management. Oral Oncol. 2020, 102, 104550. [Google Scholar] [CrossRef]
- González-Moles, M.Á.; Warnakulasuriya, S.; González-Ruiz, I.; González-Ruiz, L.; Ayén, Á.; Lenouvel, D.; Ruiz-Ávila, I.; Ramos-García, P. Worldwide prevalence of oral lichen planus: A systematic review and meta-analysis. Oral Dis. 2021, 27, 813–828. [Google Scholar] [CrossRef] [PubMed]
- Carrozzo, M.; Porter, S.; Mercadante, V.; Fedele, S. Oral lichen planus: A disease or a spectrum of tissue reactions? Types, causes, diagnostic algorhythms, prognosis, management strategies. Periodontology 2000 2019, 80, 105–125. [Google Scholar] [CrossRef] [PubMed]
- Alrashdan, M.S.; Cirillo, N.; McCullough, M. Oral lichen planus: A literature review and update. Arch. Dermatol. Res. 2016, 308, 539–551. [Google Scholar] [CrossRef]
- Bermejo-Fenoll, A.; Sánchez-Siles, M.; López-Jornet, P.; Camacho-Alonso, F.; Salazar-Sánchez, N. A retrospective clinicopathological study of 550 patients with oral lichen planus in south-eastern Spain. J. Oral Pathol. Med. 2010, 39, 491–496. [Google Scholar] [CrossRef]
- Iocca, O.; Sollecito, T.P.; Alawi, F.; Weinstein, G.S.; Newman, J.G.; De Virgilio, A.; Di Maio, P.; Spriano, G.; Pardiñas López, S.; Shanti, R.M. Potentially malignant disorders of the oral cavity and oral dysplasia: A systematic review and meta-analysis of malignant transformation rate by subtype. Head Neck 2020, 42, 539–555. [Google Scholar] [CrossRef] [PubMed]
- Louisy, A.; Humbert, E.; Samimi, M. Oral Lichen Planus: An Update on Diagnosis and Management. Am. J. Clin. Dermatol. 2023, in press. [Google Scholar] [CrossRef]
- Parlatescu, I.; Tovaru, M.; Nicolae, C.L.; Sfeatcu, R.; Didilescu, A.C. Oral health-related quality of life in different clinical forms of oral lichen planus. Clin. Oral Investig. 2020, 24, 301–308. [Google Scholar] [CrossRef]
- Eisenberg, E. Oral lichen planus: A benign lesion. J. Oral Maxillofac. Surg. 2000, 58, 1278–1285. [Google Scholar] [CrossRef] [PubMed]
- van der Meij, E.H.; van der Waal, I. Lack of clinicopathologic correlation in the diagnosis of oral lichen planus based on the presently available diagnostic criteria and suggestions for modifications. J. Oral Pathol. Med. 2003, 32, 507–512. [Google Scholar] [CrossRef]
- Schlosser, B.J. Lichen planus and lichenoid reactions of the oral mucosa. Dermatol. Ther. 2010, 23, 251–267. [Google Scholar] [CrossRef] [PubMed]
- Edwards, P.C.; Kelsch, R. Oral lichen planus: Clinical presentation and management. J. Can. Dent. Assoc. 2002, 68, 494–499. [Google Scholar]
- Giuliani, M.; Troiano, G.; Cordaro, M.; Corsalini, M.; Gioco, G.; Lo Muzio, L.; Pignatelli, P.; Lajolo, C. Rate of malignant transformation of oral lichen planus: A systematic review. Oral Dis. 2019, 25, 693–709. [Google Scholar] [CrossRef] [PubMed]
- White, B.A.; Lockhart, P.B.; Connolly, S.F.; Sonis, S.T. The use of infrared thermography in the evaluation of oral lesions. Int. J. Tissue React. 1987, 9, 105–114. [Google Scholar] [CrossRef]
- Lahiri, B.B.; Bagavathiappan, S.; Jayakumar, T.; Philip, J. Medical applications of infrared thermography: A review. Infrared Phys. Technol. 2012, 55, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Kesztyüs, D.; Brucher, S.; Kesztyüs, T. Use of infrared thermography in medical diagnostics: A scoping review protocol. BMJ Open 2022, 12, e059833. [Google Scholar] [CrossRef]
- Usamentiaga, R.; Venegas, P.; Guerediaga, J.; Vega, L.; Molleda, J.; Bulnes, F.G. Infrared thermography for temperature measurement and non-destructive testing. Sensors 2014, 14, 12305–12348. [Google Scholar] [CrossRef]
- Vergilio, M.M.; Gomes, G.; Aiello, L.M.; Fontana, M.; Aldred, A.; Ribeiro, J.A.S.; Gabbi, T.V.B.; Leonardi, G.R. Evaluation of skin using infrared thermal imaging for dermatology and aesthetic applications. J. Cosmet. Dermatol. 2022, 21, 895–904. [Google Scholar] [CrossRef]
- Zhihao, J.; Kai, Z.; Xiaozuo, L.; Li, X. Analysis of tongue information in coronary artery disease. In Proceedings of the 2008 IEEE International Symposium on IT in Medicine and Education, Xiamen, China, 12–14 December 2008; pp. 287–290. [Google Scholar]
- Feng, L.; Xiao, W.; Wen, C.; Deng, Q.; Guo, J.; Song, H. Objectification of Tongue Diagnosis in Traditional Medicine, Data Analysis, and Study Application. J. Vis. Exp. 2023, 194, e65140. [Google Scholar] [CrossRef]
- Baek, S.W.; Lee, J.M.; Park, Y.B.; Park, Y.J. Relationship between Tongue Temperature Estimated by Infrared Thermography, Tongue Color, and Cold-Heat Pathological Patterns: A Retrospective Chart Review Study. Evid.-Based Complement. Altern. Med. 2018, 27, 6841460. [Google Scholar] [CrossRef] [PubMed]
- Thirunavukkarasu, U.; Umapathy, S.; Krishnan, P.T.; Janardanan, K. Human Tongue Thermography Could Be a Prognostic Tool for Prescreening the Type II Diabetes Mellitus. Evid.-Based Complement. Altern. Med. 2020, 14, 3186208. [Google Scholar] [CrossRef]
- Nicolas-Rodriguez, E.; Garcia-Martinez, A.; Molino-Pagan, D.; Marin-Martinez, L.; Pons-Fuster, E.; López-Jornet, P. Thermography as a Non-Ionizing Quantitative Tool for Diagnosing Burning Mouth Syndrome: Case-Control Study. Int. J. Environ. Res. Public Health 2022, 19, 8903. [Google Scholar] [CrossRef]
- Jung, C.J.; Jeon, Y.J.; Kim, J.Y.; Kim, K.H. Review on the current trends in tongue diagnosis systems. Integr. Med. Res. 2012, 1, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.; Zhang, Y. Relationship between dynamic infrared thermal images and blood perfusion rate of the tongue in anaemia patients. Infrared Phys. Technol. 2018, 89, 27–34. [Google Scholar] [CrossRef]
- Lv, C.; Wang, X.; Chen, J.; Yang, N.; Fisk, I. A non-invasive measurement of tongue surface temperature. Food Res. Int. 2022, 116, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Suter, V.G.A.; Negoias, S.; Friedrich, H.; Landis, B.N.; Caversaccio, M.D.; Bornstein, M.M. Impaired Taste Perception in Li-chen Planus Patients with Tongue Involvement. Oral Health Prev. Dent. 2021, 19, 287–294. [Google Scholar] [CrossRef]
- Dominguez-Lara, S. Magnitud del efecto para pruebas de normalidad en investigación en salud. Investig. Educ. Med. 2018, 7, 92–93. [Google Scholar] [CrossRef]
- Gzawi, M.; Warawreh, A.; Hijazin, R.; Jafar, H. Clinical evaluation of thermography as a diagnostic tool in oral and maxillo-facial lesions. J. R. Med. Serv. 2018, 25, 45–49. [Google Scholar]
- Aboushady, M.A.; Talaat, W.; Hamdoon, Z.; Elshazly, M.T.; Ragy, N.; Bourauel, C.; Talaat, S. Thermography as a non-ionizing quantitative tool for diagnosing periapical inflammatory lesions. BMC Oral Health 2021, 21, 260. [Google Scholar] [CrossRef]
- de Almeida, A.N.S.; de Souza Ferreira, S.L.; Balata, P.M.M.; da Cunha, D.A.; Pernambuco, L.; da Silva, H.J. Thermography in complementary assessments of head and neck muscles: A scoping review. J. Oral Rehabil. 2022, 49, 1188–1196. [Google Scholar] [CrossRef] [PubMed]
- Wziątek-Kuczmik, D.; Niedzielska, I.; Mrowiec, A.; Bałamut, K.; Handzel, M.; Szurko, A. Is Thermal Imaging a Helpful Tool in Diagnosis of Asymptomatic Odontogenic Infection Foci-A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 16325. [Google Scholar] [CrossRef] [PubMed]
- Bermejo-Fenoll, A.; López-Jornet, P.; Camacho-Alonso, F.; Saura-Ingles, A.; Panchon-Ruiz, A. Morphometric analysis of the dorsum linguae in patients with Oral Lichen Planus. Med. Oral Patol. Oral Cirugía Bucal 2009, 14, e388-92. [Google Scholar]
- Suter, V.G.; Negoias, S.; Friedrich, H.; Landis, B.N.; Caversaccio, M.D.; Bornstein, M.M. Gustatory function and taste perception in patients with oral lichen planus and tongue involvement. Clin. Oral Investig. 2017, 21, 957–964. [Google Scholar] [CrossRef]
- Fernandes, M.S.; Castelo, P.M.; Chaves, G.N.; Fernandes, J.P.S.; Fonseca, F.L.A.; Zanato, L.E.; Gavião, M.B.D. Relationship between polypharmacy, xerostomia, gustatory sensitivity, and swallowing complaints in the elderly: A multidisciplinary approach. J. Texture Stud. 2021, 52, 187–196. [Google Scholar] [CrossRef]
- Mollaoglu, N. Oral lichen planus: A review. Br. J. Oral Maxillofac. Surg. 2000, 38, 370–377. [Google Scholar] [CrossRef]
- López-Pintor, R.M.; Diniz-Freitas, M.; Ramesh, S.S.K.; Valdéz, J.A.; Dan, H.; Bissonnette, C.; Dan, H.; Brennan, M.T.; Burkhart, N.W.; Greenberg, M.S.; et al. World Workshop on Oral Medicine VIII: Development of a core outcome set for oral lichen planus: A systematic review of outcome domains. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2023, 135, 772–780. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total | Control | OLP | OLP Tongue | p Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n 43 | 49.4% | n 24 | 27.3% | n 20 | 23% | |||
| Sex | Female | 66 | 75.9 | 34 | 79.1 | 15 | 62.5 | 17 | 85.0 | 0.164 |
| Male | 21 | 24.1 | 9 | 20.9 | 9 | 37.5 | 3 | 15.0 | ||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||
| Age | 60.43 | 10.7 | 57.02 | 10.5 | 63.58 | 6.4 | 63.95 | 13.3 | 0.012 * | |
| OLP Evolution | <6 months | 11 | 25.0 | - | - | 1 | 4.2 | 10 | 50.0 | 0.001 *** |
| 6 months–2 years | 11 | 25.0 | - | - | 6 | 25.0 | 5 | 25.0 | ||
| 3–5 Years | 7 | 15.9 | - | - | 7 | 29.2 | 0 | 0 | ||
| 6–10 Years | 6 | 13.6 | - | - | 6 | 25.0 | 0 | 0 | ||
| >10 Years | 9 | 20.5 | - | - | 4 | 16.6 | 5 | 25.0 | ||
| OLP Clinical form | Reticular/ | 14 | 31.8 | - | - | 9 | 37.5 | 5 | 25.0 | 0.111 |
| Atrophic/Erosive | 11 | 25.0 | - | - | 8 | 33.3 | 3 | 15.0 | ||
| Mixes | 19 | 43.2 | - | - | 7 | 29.2 | 12 | 60.0 | ||
| Variables | Control | OLP | OLP Lingual | F(gl) | p Value | η2 | |||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||||
| Tª M Dorsum | 33.27 | 1.0 | 32.85 | 0.9 | 33.28 | 0.7 | 1.97(2) | 0.146 | 0.045 |
| Tª M Lateral right | 32.79 | 1.0 | 32.54 | 0.7 | 32.71 | 0.7 | 0.67(2) | 0.515 | 0.016 |
| Tª M Lateral Left | 32.61 | 1.0 | 32.12 | 0.8 | 32.17 | 0.7 | 2.97(2) | 0.057 | 0.066 |
| Tª M Apex | 31.37 | 1.2 | 31.01 | 0.8 | 31.43 | 0.8 | 1.18(2) | 0.313 | 0.027 |
| Variables | n | % | |
|---|---|---|---|
| Dorsum | No lesion | 11 | 55.0 |
| Reticular/plaque | 3 | 15.0 | |
| Atrophic/Erosive | 3 | 15.0 | |
| Mixed | 3 | 15.0 | |
| Lateral right | No lesion | 5 | 25.0 |
| Reticular/plaque | 5 | 25.0 | |
| Atrophic/Erosive | 5 | 25.0 | |
| Mixed | 5 | 25.0 | |
| Lateral left | No lesion | 6 | 30.0 |
| Reticular/Plaque | 5 | 25.0 | |
| Atrophic/Erosive | 5 | 25.0 | |
| Mixed | 4 | 20.0 | |
| Tip | No lesion | 18 | 90.0 |
| Reticular/Plaque | 1 | 5.0 | |
| Atrophic/Erosive | 1 | 5.0 | |
| Mixed | - | - | |
| Variables | No Lesion (n = 40) | Reticular/ Plaque (n = 14) | Atrophic/Erosive (n = 14) | Mixed (n = 12) | Sig. | η2 |
|---|---|---|---|---|---|---|
| Temperature | 32.12 (1.0) | 32.51 (0.9) | 32.50 (1.1) | 33.07 (1.0) | 0.032 | 0.109 |
| Variable | OLP | OLP Lingual | χ2(gl) | p Value | V | |||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | |||||
| Taste alteration | Never | 16 | 66.7% | 13 | 65.0% | 1.83(3) | 0.609 | 0.204 |
| Sometimes | 3 | 12.5% | 2 | 10.0% | ||||
| From time to time | 4 | 16.7% | 2 | 10.0% | ||||
| Often | 1 | 4.2% | 3 | 15.0% | ||||
| Sweet | Never | 18 | 75.0% | 15 | 75.0% | 0.24(3) | 0.97 | 0.075 |
| Sometimes | 2 | 8.3% | 1 | 5.0% | ||||
| From time to time | 3 | 12.5% | 3 | 15.0% | ||||
| Often | 1 | 4.2% | 1 | 5.0% | ||||
| Salty | Never | 18 | 75.0% | 14 | 70.0% | 0.68(3) | 0.879 | 0.124 |
| Sometimes | 1 | 4.2% | 2 | 10.0% | ||||
| From time to time | 3 | 12.5% | 2 | 10.0% | ||||
| Often | 2 | 8.3% | 2 | 10.0% | ||||
| Sour | Never | 18 | 75.0% | 14 | 70.0% | 0.62(3) | 0.892 | 0.118 |
| Sometimes | 2 | 8.3% | 1 | 5.0% | ||||
| From time to time | 3 | 12.5% | 4 | 20.0% | ||||
| Often | 1 | 4.2% | 1 | 5.0% | ||||
| Bitter | Never | 17 | 70.8% | 15 | 75.0% | 2.93(3) | 0.403 | 0.258 |
| Sometimes | 3 | 12.5% | 0 | 0.0% | ||||
| From time to time | 3 | 12.5% | 4 | 20.0% | ||||
| Often | 1 | 4.2% | 1 | 5.0% | ||||
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Taste alteration | -- | ||||||||
| 2. Sweet | 0.875 ** | -- | |||||||
| 3. Salty | 0.927 ** | 0.925 ** | -- | ||||||
| 4. Sour | 0.936 ** | 0.934 ** | 0.990 ** | -- | |||||
| 5. Bitter | 0.884 ** | 0.996 ** | 0.919 ** | 0.937 ** | -- | ||||
| 6. Dorsum | 0.140 | 0.133 | 0.086 | 0.046 | 0.119 | -- | |||
| 7. Lateral right | −0.146 | 0.010 | −0.077 | −0.120 | −0.010 | 0.230 | -- | ||
| 8. Lateral left | 0.040 | 0.287 | 0.192 | 0.149 | 0.256 | 0.080 | 0.661 ** | -- | |
| 9. Apex | 0.149 | 0.099 | 0.057 | 0.125 | 0.154 | −0.286 | 0.022 | −0.089 | -- |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicolas-Rodriguez, E.; Pons-Fuster, E.; López-Jornet, P. Diagnostic Infrared Thermography of the Tongue and Taste Perception in Patients with Oral Lichen Planus: Case-Control Study. J. Clin. Med. 2024, 13, 435. https://doi.org/10.3390/jcm13020435
Nicolas-Rodriguez E, Pons-Fuster E, López-Jornet P. Diagnostic Infrared Thermography of the Tongue and Taste Perception in Patients with Oral Lichen Planus: Case-Control Study. Journal of Clinical Medicine. 2024; 13(2):435. https://doi.org/10.3390/jcm13020435
Chicago/Turabian StyleNicolas-Rodriguez, Elena, Eduardo Pons-Fuster, and Pia López-Jornet. 2024. "Diagnostic Infrared Thermography of the Tongue and Taste Perception in Patients with Oral Lichen Planus: Case-Control Study" Journal of Clinical Medicine 13, no. 2: 435. https://doi.org/10.3390/jcm13020435