
Extracorporeal Membrane Oxygenation for Pulmonary Embolism: A Systematic Review and Meta-Analysis
 , , , , , and
, , , , , and 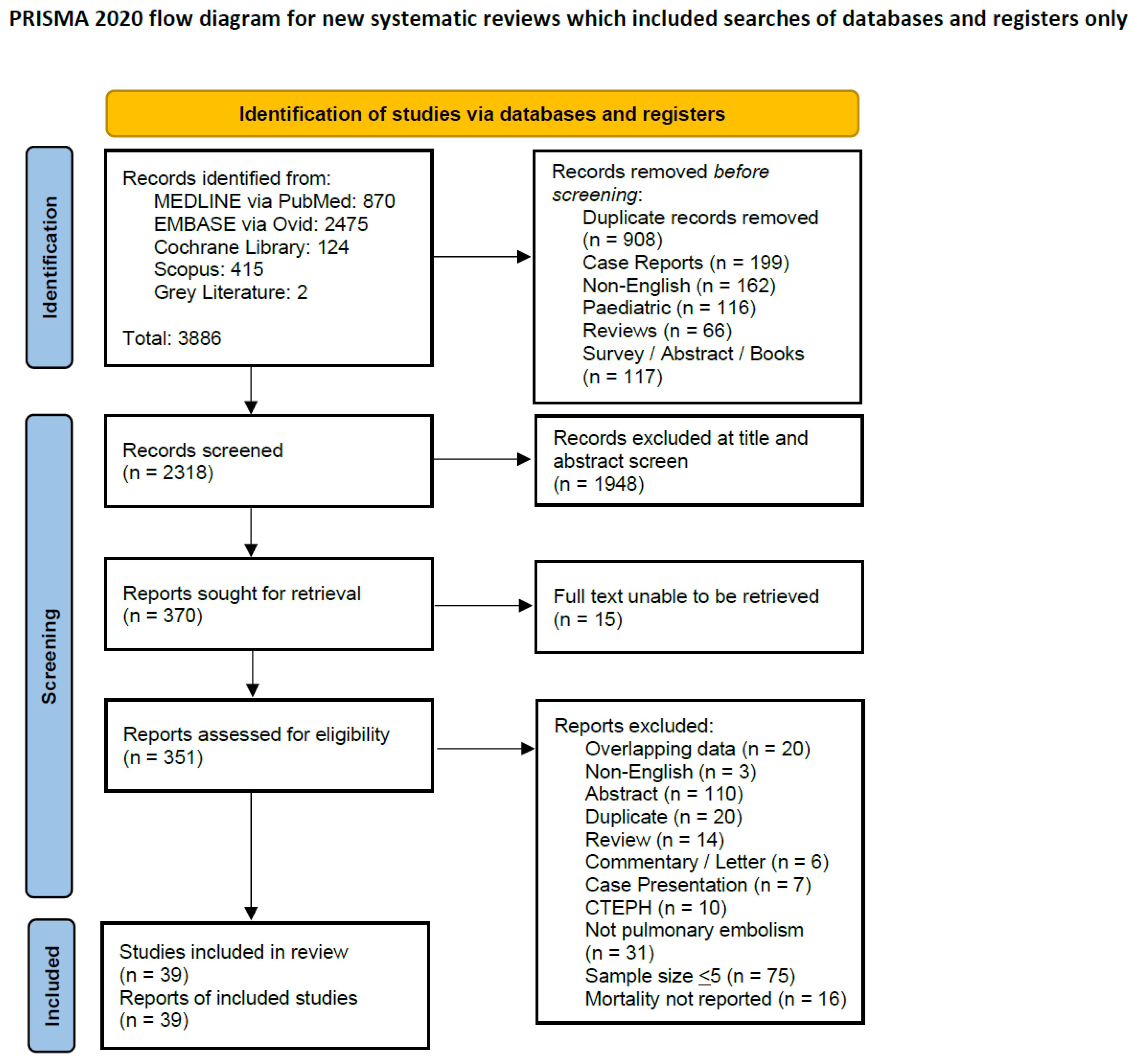{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Collection and Risk of Bias Assessment
2.3. Data Synthesis
2.4. Role of the Funding Source
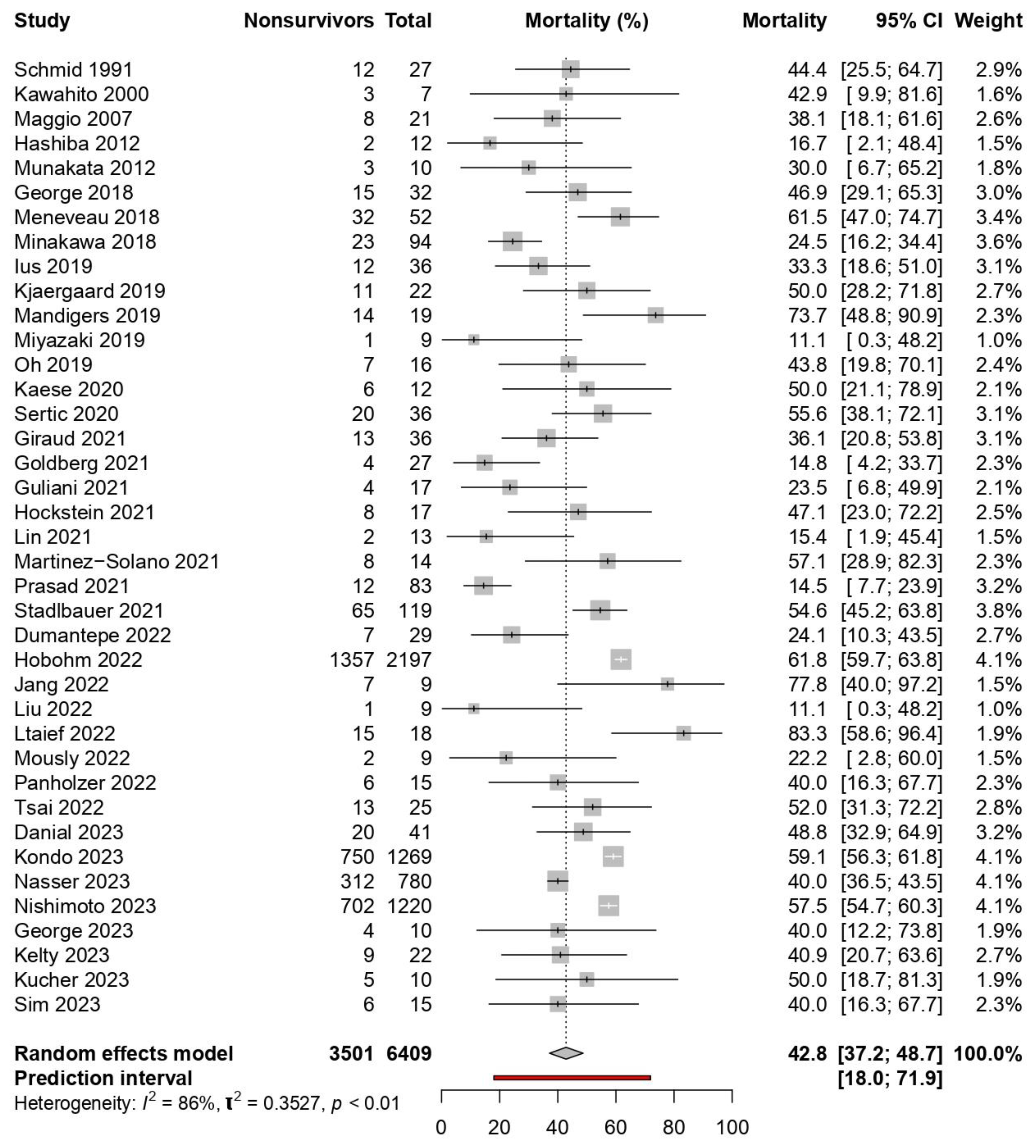
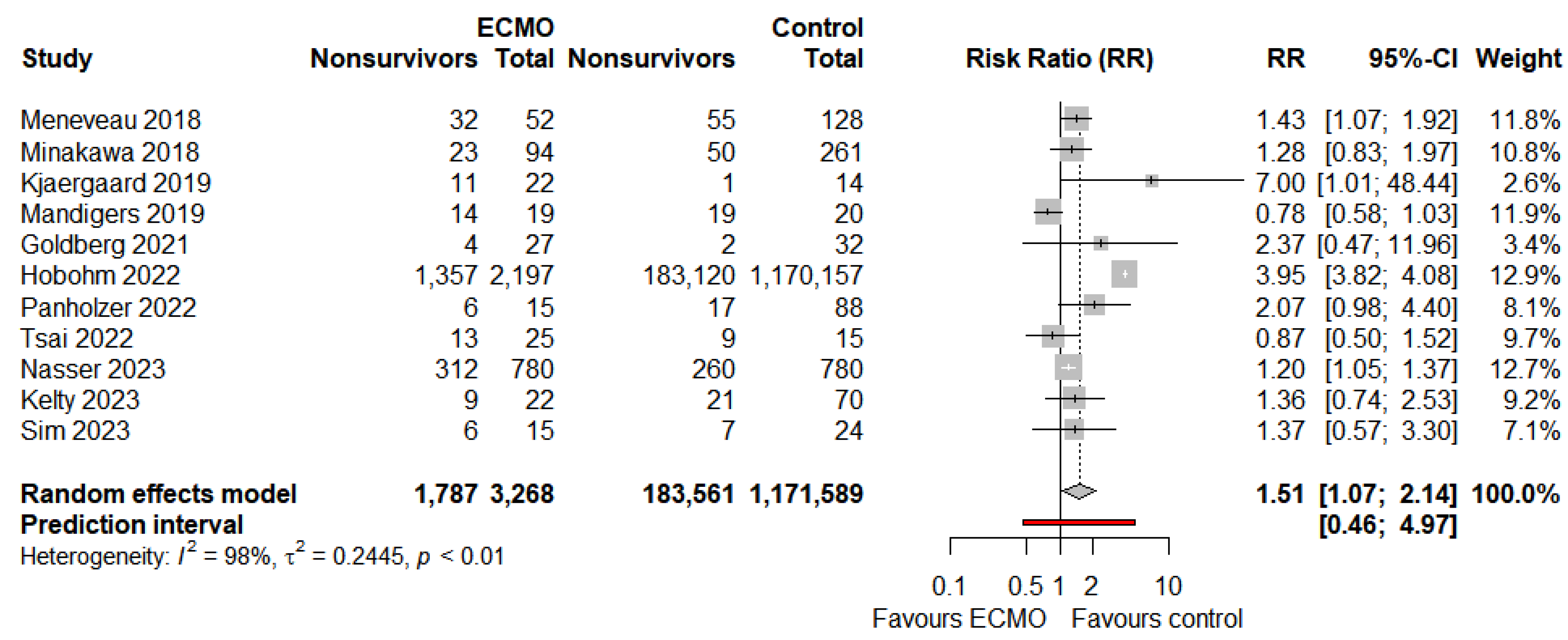
3. Results
3.1. Secondary Outcomes
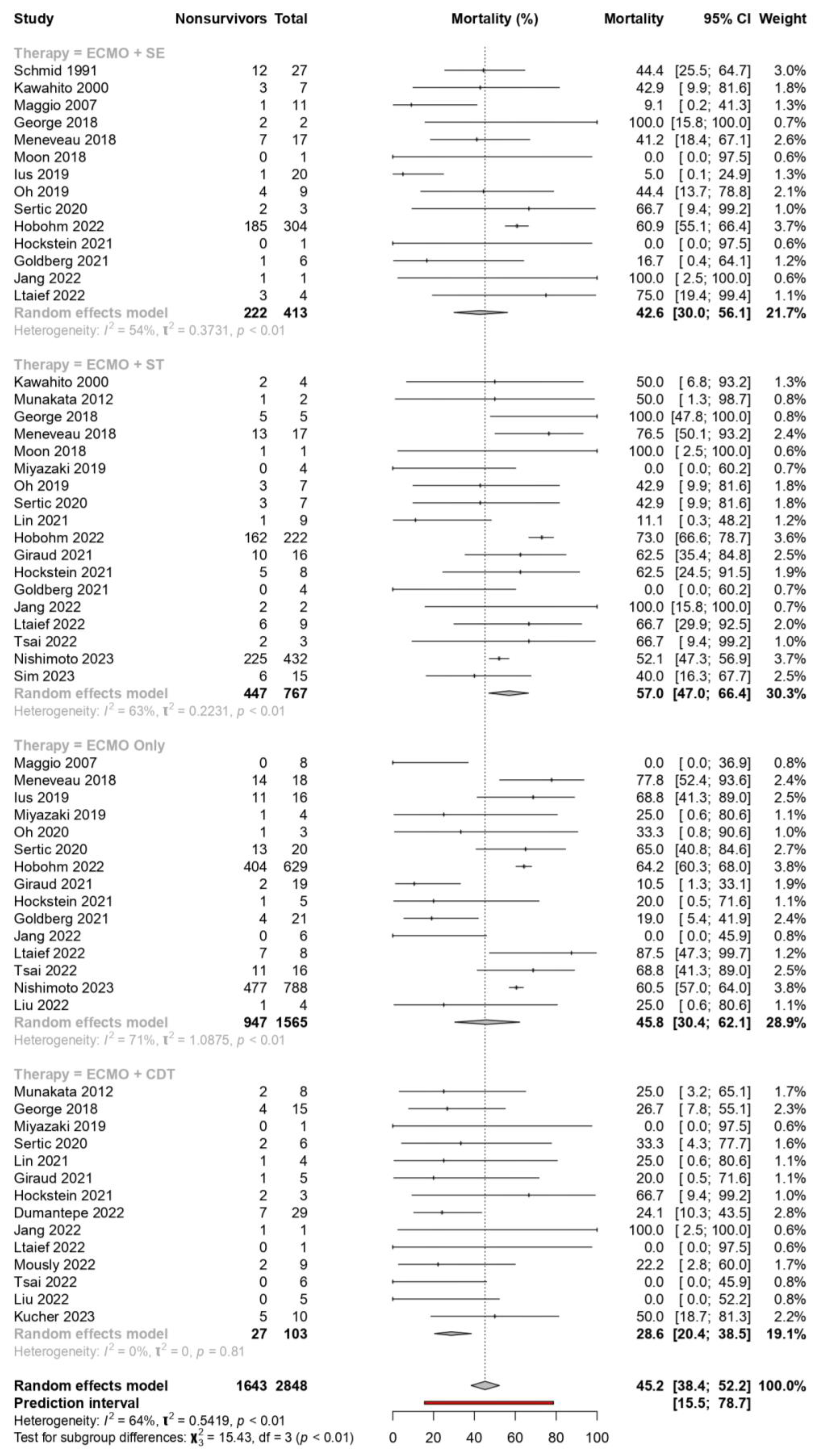
3.2. Post Hoc Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CI | Confidence intervals |
| ECMO | Extracorporeal membrane oxygenation |
| GRADE | Grading of Recommendations, Assessment, Development and Evaluations |
| HRPE | High-risk pulmonary embolism |
| ICU | Intensive care unit |
| JBI | Joanna Briggs Institute |
| PE | Pulmonary embolism |
| PROSPERO | International prospective register of systematic reviews |
| RR | Risk ratio |
| VA | Venoarterial |
| VV | Venovenous |
References
- Horlander, K.T.; Mannino, D.M.; Leeper, K.V. Pulmonary embolism mortality in the United States, 1979-1998: An analysis using multiple-cause mortality data. Arch. Intern. Med. 2003, 163, 1711–1717. [Google Scholar] [CrossRef] [PubMed]
- Lassila, R.; Jula, A.; Pitkäniemi, J.; Haukka, J. The association of statin use with reduced incidence of venous thromboembolism: A population-based cohort study. BMJ Open 2014, 4, e005862. [Google Scholar] [CrossRef] [PubMed]
- Kucher, N.; Rossi, E.; De Rosa, M.; Goldhaber, S.Z. Massive pulmonary embolism. Circulation 2006, 113, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Pasrija, C.; Kronfli, A.; George, P.; Raithel, M.; Boulos, F.; Herr, D.L.; Gammie, J.S.; Pham, S.M.; Griffith, B.P.; Kon, Z.N. Utilization of veno-arterial extracorporeal membrane oxygenation for massive pulmonary embolism. Ann. Thorac. Surg. 2018, 105, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.-J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef]
- Alba, A.C.; Foroutan, F.; Buchan, T.A.; Alvarez, J.; Kinsella, A.; Clark, K.; Zhu, A.; Lau, K.; McGuinty, C.; Aleksova, N.; et al. Mortality in patients with cardiogenic shock supported with VA ECMO: A systematic review and meta-analysis evaluating the impact of etiology on 29,289 patients. J. Heart Lung Transplant. 2021, 40, 260–268. [Google Scholar] [CrossRef]
- Corsi, F.; Lebreton, G.; Bréchot, N.; Hekimian, G.; Nieszkowska, A.; Trouillet, J.L.; Luyt, C.E.; Leprince, P.; Chastre, J.; Combes, A.; et al. Life-threatening massive pulmonary embolism rescued by venoarterial-extracorporeal membrane oxygenation. Crit. Care 2017, 21, 76. [Google Scholar] [CrossRef]
- Yusuff, H.; Zochios, V.; Vuylsteke, A. Extracorporeal membrane oxygenation in acute massive pulmonary embolism: A systematic review. Perfusion 2015, 30, 611–616. [Google Scholar] [CrossRef]
- Oh, Y.N.; Oh, D.K.; Koh, Y.; Lim, C.-M.; Huh, J.-W.; Lee, J.S.; Jung, S.-H.; Kang, P.-J.; Hong, S.-B. Use of extracorporeal membrane oxygenation in patients with acute high-risk pulmonary embolism: A case series with literature review. Acute Crit. Care 2019, 34, 148–154. [Google Scholar] [CrossRef]
- Maggio, P.; Hemmila, M.; Haft, J.; Bartlett, R. Extracorporeal Life Support for Massive Pulmonary Embolism. J. Trauma Acute Care Surg. 2007, 62, 570–576. [Google Scholar] [CrossRef]
- Jia, D.; Yang, I.X.; Ling, R.R.; Syn, N.; Poon, W.H.; Murughan, K.; Tan, C.S.; Choong, A.M.T.L.; MacLaren, G.; Ramanathan, K. Vascular Complications of Extracorporeal Membrane Oxygenation: A Systematic Review and Meta-Regression Analysis. Crit. Care Med. 2020, 48, e1269–e1277. [Google Scholar] [CrossRef]
- Mitra, S.; Ling, R.R.; Yang, I.X.; Poon, W.H.; Tan, C.S.; Monagle, P.; MacLaren, G.; Ramanathan, K. Severe COVID-19 and coagulopathy: A systematic review and meta-analysis. Ann. Acad. Med. Singap. 2021, 50, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Baldetti, L.; Beneduce, A.; Cianfanelli, L.; Falasconi, G.; Pannone, L.; Moroni, F.; Venuti, A.; Sacchi, S.; Gramegna, M.; Pazzanese, V.; et al. Use of extracorporeal membrane oxygenation in high-risk acute pulmonary embolism: A systematic review and meta-analysis. Artif. Organs 2021, 45, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.H.; Gordon, M.; Vender, R.; Pettigrew, S.; Desai, P.; Marchetti, N.; Mamary, A.J.; Panaro, J.; Cohen, G.; Bashir, R.; et al. Venoarterial Extracorporeal Membrane Oxygenation in Massive Pulmonary Embolism-Related Cardiac Arrest: A Systematic Review. Crit. Care Med. 2021, 49, 760–769. [Google Scholar] [CrossRef] [PubMed]
- Chopard, R.; Nielsen, P.; Ius, F.; Cebotari, S.; Ecarnot, F.; Pilichowski, H.; Schmidt, M.; Kjaergaard, B.; Sousa-Casasnovas, I.; Ghoreishi, M.; et al. Optimal reperfusion strategy in acute high-risk pulmonary embolism requiring extracorporeal membrane oxygenation support: A systematic review and meta-analysis. Eur. Respir. J. 2022, 60, 2102977. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Peters, M.D.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef]
- Santesso, N.; Glenton, C.; Dahm, P.; Garner, P.; Akl, E.A.; Alper, B.; Brignardello-Petersen, R.; Carrasco-Labra, A.; De Beer, H.; Hultcrantz, M.; et al. GRADE guidelines 26: Informative statements to communicate the findings of systematic reviews of interventions. J. Clin. Epidemiol. 2020, 119, 126–135. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Clopper, C.J.; Pearson, E.S. The use of confidence or fiducial limits illustrated in the case of the binomial. Biometrika 1934, 26, 404–413. [Google Scholar] [CrossRef]
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata command to perform meta-analysis of binomial data. Arch. Public Health 2014, 72, 39. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, G.; Chemaitelly, H.; Abu-Raddad, L.J.; Rücker, G. Seriously misleading results using inverse of Freeman-Tukey double arcsine transformation in meta-analysis of single proportions. Res. Synth. Methods 2019, 10, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A. GRADE guidelines: 7. Rating the quality of evidence—Inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef] [PubMed]
- Iorio, A.; Spencer, F.A.; Falavigna, M.; Alba, C.; Lang, E.; Burnand, B.; McGinn, T.; Hayden, J.; Williams, K.; Shea, B. Use of GRADE for assessment of evidence about prognosis: Rating confidence in estimates of event rates in broad categories of patients. BMJ 2015, 350, h870. [Google Scholar] [CrossRef] [PubMed]
- Danial, P.; Olivier, M.E.; Bréchot, N.; Ponnaiah, M.; Schoell, T.; D’Alessandro, C.; Demondion, P.; Clément, M.; Juvin, C.; Carillion, A.; et al. Association Between Shock Etiology and 5-Year Outcomes After Venoarterial Extracorporeal Membrane Oxygenation. J. Am. Coll. Cardiol. 2023, 81, 897–909. [Google Scholar] [CrossRef] [PubMed]
- Kondo, T.; Araki, T.; Imaizumi, T.; Sumita, Y.; Nakai, M.; Tanaka, A.; Okumura, T.; Butt, J.H.; Petrie, M.C.; McMurray, J.J.V.; et al. Prognosis in Patients with Cardiogenic Shock Who Received Temporary Mechanical Circulatory Support. JACC Asia 2023, 3, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Chen, J.; Xu, X.; Lan, F.; He, M.; Shao, C.; Xu, Y.; Han, P.; Chen, Y.; Zhu, Y.; et al. Extracorporeal Membrane Oxygenation-First Strategy for Acute Life-Threatening Pulmonary Embolism. Front. Cardiovasc. Med. 2022, 9, 875021. [Google Scholar] [CrossRef]
- Nasser, M.F.; Jabri, A.; Sharma, S.; Alhuneafat, L.; Omar, Y.A.; Krishnan, V.; Cameron, S.J. Outcomes with use of extra-corporeal membrane oxygenation in high-risk pulmonary embolism: A national database perspective. J. Thromb. Thrombolysis 2023, 55, 499–505. [Google Scholar] [CrossRef]
- Nishimoto, Y.; Ohbe, H.; Matsui, H.; Nakajima, M.; Sasabuchi, Y.; Sato, Y.; Watanabe, T.; Yamada, T.; Fukunami, M.; Yasunaga, H. Effectiveness of systemic thrombolysis on clinical outcomes in high-risk pulmonary embolism patients with venoarterial extracorporeal membrane oxygenation: A nationwide inpatient database study. J. Intensive Care 2023, 11, 4. [Google Scholar] [CrossRef]
- Panholzer, B.; Gravert, H.; Borzikowsky, C.; Huenges, K.; Schoettler, J.; Schoeneich, F.; Attmann, T.; Haneya, A.; Frank, D.; Cremer, J.; et al. Outcome after surgical embolectomy for acute pulmonary embolism. J. Cardiovasc. Med. 2022, 23, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Schmid, C.; Zietlow, S.; Wagner, T.O.; Laas, J.; Borst, H.G. Fulminant pulmonary embolism: Symptoms, diagnostics, operative technique, and results. Ann. Thorac. Surg. 1991, 52, 1102–1105; discussion 1105–1107. [Google Scholar] [CrossRef] [PubMed]
- Kawahito, K.; Murata, S.; Adachi, H.; Ino, T.; Fuse, K. Resuscitation and circulatory support using extracorporeal membrane oxygenation for fulminant pulmonary embolism. Artif. Organs. 2000, 24, 427–430. [Google Scholar] [CrossRef] [PubMed]
- Hashiba, K.; Okuda, J.; Maejima, N.; Iwahashi, N.; Tsukahara, K.; Tahara, Y.; Hibi, K.; Kosuge, M.; Ebina, T.; Endo, T. Percutaneous cardiopulmonary support in pulmonary embolism with cardiac arrest. Resuscitation 2012, 83, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Munakata, R.; Yamamoto, T.; Hosokawa, Y.; Tokita, Y.; Akutsu, K.; Sato, N.; Murata, S.; Tajima, H.; Mizuno, K.; Tanaka, K. Massive pulmonary embolism requiring extracorporeal life support treated with catheter-based interventions. Int. Heart J. 2012, 53, 370–374. [Google Scholar] [CrossRef] [PubMed]
- George, B.; Parazino, M.; Omar, H.R.; Davis, G.; Guglin, M.; Gurley, J.; Smyth, S. A retrospective comparison of survivors and non-survivors of massive pulmonary embolism receiving veno-arterial extracorporeal membrane oxygenation support. Resuscitation 2018, 122, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Meneveau, N.; Guillon, B.; Planquette, B.; Piton, G.; Kimmoun, A.; Gaide-Chevronnay, L.; Aissaoui, N.; Neuschwander, A.; Zogheib, E.; Dupont, H.; et al. Outcomes after extracorporeal membrane oxygenation for the treatment of high-risk pulmonary embolism: A multicentre series of 52 cases. Eur. Heart J. 2018, 39, 4196–4204. [Google Scholar] [CrossRef] [PubMed]
- Minakawa, M.; Fukuda, I.; Miyata, H.; Motomura, N.; Takamoto, S.; Taniguchi, S.; Daitoku, K.; Kondo, N. Outcomes of Pulmonary Embolectomy for Acute Pulmonary Embolism. Circ. J. 2018, 82, 2184–2190. [Google Scholar] [CrossRef]
- Ius, F.; Hoeper, M.M.; Fegbeutel, C.; Kühn, C.; Olsson, K.; Koigeldiyev, N.; Tudorache, I.; Warnecke, G.; Optenhöfel, J.; Puntigam, J.O. Extracorporeal membrane oxygenation and surgical embolectomy for high-risk pulmonary embolism. Eur. Respir. J. 2019, 53, 1801773. [Google Scholar] [CrossRef]
- Kjaergaard, B.; Kristensen, J.H.; Sindby, J.E.; de Neergaard, S.; Rasmussen, B.S. Extracorporeal membrane oxygenation in life-threatening massive pulmonary embolism. Perfusion 2019, 34, 467–474. [Google Scholar] [CrossRef]
- Mandigers, L.; Scholten, E.; Rietdijk, W.J.R.; den Uil, C.A.; van Thiel, R.J.; Rigter, S.; Heijnen, B.; Gommers, D.; Dos Reis Miranda, D. Survival and neurological outcome with extracorporeal cardiopulmonary resuscitation for refractory cardiac arrest caused by massive pulmonary embolism: A two center observational study. Resuscitation 2019, 136, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, K.; Hikone, M.; Kuwahara, Y.; Ishida, T.; Sugiyama, K.; Hamabe, Y. Extracorporeal CPR for massive pulmonary embolism in a “hybrid 2136 emergency department”. Am. J. Emerg. Med. 2019, 37, 2132–2135. [Google Scholar] [CrossRef] [PubMed]
- Kaese, S.; Lebiedz, P. Extracorporeal life support after failure of thrombolysis in pulmonary embolism. Adv. Respir. Med. 2020, 88, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Sertic, F.; Diagne, D.; Chavez, L.; Richards, T.; Berg, A.; Acker, M.; Giri, J.S.; Szeto, W.Y.; Khandhar, S.; Gutsche, J.; et al. Mid-term outcomes with the use of extracorporeal membrane oxygenation for cardiopulmonary failure secondary to massive pulmonary embolism. Eur. J. Cardiothorac. Surg. 2020, 58, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Giraud, R.; Laurencet, M.; Assouline, B.; De Charrière, A.; Banfi, C.; Bendjelid, K. Can VA-ECMO be used as an adequate treatment in massive pulmonary embolism? J. Clin. Med. 2021, 10, 3376. [Google Scholar] [CrossRef]
- Goldberg, J.B.; Spevack, D.M.; Ahsan, S.; Rochlani, Y.; Ohira, S.; Spencer, P.; Kai, M.; Malekan, R.; Spielvogel, D.; Lansman, S. Comparison of Surgical Embolectomy and Veno-arterial Extracorporeal Membrane Oxygenation for Massive Pulmonary Embolism. Semin. Thorac. Cardiovasc. Surg. 2021, 34, 934–942. [Google Scholar] [CrossRef]
- Guliani, S.; Das Gupta, J.; Osofsky, R.; Kraai, E.P.; Mitchell, J.A.; Dettmer, T.S.; Wray, T.C.; Tawil, I.; Rana, M.A.; Marinaro, J. Venoarterial extracorporeal membrane oxygenation is an effective management strategy for massive pulmonary embolism patients. J. Vasc. Surg. Venous. Lymphat. Disord. 2021, 9, 307–314. [Google Scholar] [CrossRef]
- Hobohm, L.; Sagoschen, I.; Habertheuer, A.; Barco, S.; Valerio, L.; Wild, J.; Schmidt, F.P.; Gori, T.; Münzel, T.; Konstantinides, S.; et al. Clinical use and outcome of extracorporeal membrane oxygenation in patients with pulmonary embolism. Resuscitation 2021, 170, 285–292. [Google Scholar] [CrossRef]
- Hockstein, M.A.; Creel-Bulos, C.; Appelstein, J.; Jabaley, C.S.; Stentz, M.J. Institutional Experience With Venoarterial Extracorporeal Membrane Oxygenation for Massive Pulmonary Embolism: A Retrospective Case Series. J. Cardiothorac. Vasc. Anesth. 2021, 35, 2681–2685. [Google Scholar] [CrossRef]
- Lin, T.W.; Tsai, M.T.; Hu, Y.N.; Wang, Y.C.; Wen, J.S.; Wu, H.Y.; Luo, C.Y.; Roan, J.N. Simultaneous Thrombolysis and Extracorporeal Membrane Oxygenation for Acute Massive Pulmonary Emboli. Ann. Thorac. Surg. 2021, 111, 923–929. [Google Scholar] [CrossRef]
- Martínez-Solano, J.; Sousa-Casasnovas, I.; Bellón-Cano, J.M.; García-Carreño, J.; Juárez-Fernández, M.; Díez-Delhoyo, F.; Sanz-Ruiz, R.; Devesa-Cordero, C.; Elízaga-Corrales, J.; Fernández-Avilés, F.; et al. Lactate levels as a prognostic predict in cardiogenic shock under venoarterial extracorporeal membrane oxygenation support. Rev. Esp. Cardiol. 2021, 75, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Prasad, N.K.; Boyajian, G.; Tran, D.; Shah, A.; Jones, K.M.; Madathil, R.J.; Deatrick, K.B.; Cires-Drouet, R.; Kaczorowski, D.J. Veno-Arterial Extracorporeal Membrane Oxygenation for Pulmonary Embolism after Systemic Thrombolysis. Semin. Thorac. Cardiovasc. Surg. 2021, 34, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Dumantepe, M.; Ozturk, C. Acoustic pulse thrombolysis complemented by ECMO improved survival in patients with high-risk pulmonary embolism. J. Card. Surg. 2022, 37, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.; Koo, S.M.; Kim, K.U.; Kim, Y.K.; Uh, S.T.; Jang, G.E.; Chang, W.; Lee, B.Y. Clinical experiences of high-risk pulmonary thromboembolism receiving extracorporeal membrane oxygenation in single institution. Tuberc. Respir. Dis. 2022, 85, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Ltaief, Z.; Lupieri, E.; Bonnemain, J.; Ben-Hamouda, N.; Rancati, V.; Kobbe, S.S.; Kirsch, M.; Chiche, J.-D.; Liaudet, L. Venoarterial Extracorporeal Membrane Oxygenation in High-Risk Pulmonary Embolism: A Case Series and Literature Review. Rev. Cardiovasc. Med. 2022, 23, 193. [Google Scholar] [CrossRef]
- Mously, H.; Hajjari, J.; Chami, T.; Hammad, T.; Schilz, R.; Carman, T.; Elgudin, Y.; Abu-Omar, Y.; Pelletier, M.P.; Shishehbor, M.H.; et al. Percutaneous mechanical thrombectomy and extracorporeal membranous oxygenation: A case series. Catheter. Cardiovasc. Interv. 2022, 100, 274–278. [Google Scholar] [CrossRef]
- Stadlbauer, A.; Philipp, A.; Blecha, S.; Lubnow, M.; Lunz, D.; Li, J.; Terrazas, A.; Schmid, C.; Lange, T.J.; Camboni, D. Long-term follow-up and quality of life in patients receiving extracorporeal membrane oxygenation for pulmonary embolism and cardiogenic shock. Ann. Intensive Care 2021, 11, 181. [Google Scholar] [CrossRef]
- Tsai, H.Y.; Wang, Y.T.; Lee, W.C.; Yen, H.T.; Lo, C.M.; Wu, C.C.; Huang, K.R.; Chen, Y.C.; Sheu, J.J.; Chen, Y.Y. Efficacy and Safety of Veno-Arterial Extracorporeal Membrane Oxygenation in the Treatment of High-Risk Pulmonary Embolism: A Retrospective Cohort Study. Front. Cardiovasc. Med. 2022, 9, 799488. [Google Scholar] [CrossRef]
- George, T.J.; Sheasby, J.; Sawhney, R.; DiMaio, J.M.; Afzal, A.; Gable, D.; Sayfo, S. Extracorporeal membrane oxygenation for large pulmonary emboli. Bayl. Univ. Med. Cent. Proc. 2023, 36, 314–317. [Google Scholar] [CrossRef]
- Kelty, C.E.; Berjaoui, W.; Shrestha, N.K.; Fitch, S.; Jovinge, S.M.; Rendon, R.L. Veno-Arterial Extracorporeal Membrane Oxygenation versus Standard Medical Management for Massive Pulmonary Embolism. Perfusion, 2023; online ahead of print. [Google Scholar] [CrossRef]
- Kucher, N.; Ouda, A.; Voci, D.; Barco, S.; Micieli, E.; Münger, M.; Pleming, W.; Grigorean, A.; Sromicki, J.; Schmiady, M.O.; et al. Percutaneous large-bore aspiration embolectomy with veno-arterial extracorporal membrane oxygenation support or standby in patients with high-risk pulmonary embolism and contraindications to thrombolysis: A preliminary single centre experience. Eur. Heart J. Acute Cardiovasc. Care. 2023, 12, 232–236. [Google Scholar] [CrossRef]
- Sim, H.T.; Jo, M.S.; Chang, Y.J.; Cho, D.G.; Kim, J.W. Outcome of Massive Pulmonary Embolism Treated Only with Extracorporeal Membrane Oxygenation and Anticoagulation without Thrombolytic Therapy or Surgical Embolectomy. Perfusion, 2023; online ahead of print. [Google Scholar] [CrossRef]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Performance of the trim and fill method in the presence of publication bias and between-study heterogeneity. Stat. Med. 2007, 26, 4544–4562. [Google Scholar] [CrossRef] [PubMed]
- Tanimoto, A.; Sugiyama, K.; Tanabe, M.; Kitagawa, K.; Kawakami, A.; Hamabe, Y. Out-of-hospital cardiac arrest patients with an initial non-shockable rhythm could be candidates for extracorporeal cardiopulmonary resuscitation: A retrospective study. Scand. J. Trauma Resusc. Emerg. Med. 2020, 28, 101. [Google Scholar] [CrossRef] [PubMed]
- Belohlavek, J.; Rohn, V.; Jansa, P.; Tosovsky, J.; Kunstyr, J.; Semrad, M.; Horak, J.; Lips, M.; Mlejnsky, F.; Balik, M.; et al. Veno-arterial ECMO in severe acute right ventricular failure with pulmonary obstructive hemodynamic pattern. J. Invasive Cardiol. 2010, 22, 365–369. Available online: https://pubmed.ncbi.nlm.nih.gov/20679672/ (accessed on 29 October 2023). [PubMed]
- Kmiec, L.; Philipp, A.; Floerchinger, B.; Lubnow, M.; Unterbuchner, C.; Creutzenberg, M.; Lunz, D.; Mueller, T.; Schmid, C.; Camboni, D. Extracorporeal membrane oxygenation for massive pulmonary embolism as bridge to therapy. ASAIO J. 2020, 66, 146–152. [Google Scholar] [CrossRef]
- Gangaraju, R.; Klok, F.A. Advanced therapies and extracorporeal membrane oxygenation for the management of high-risk pulmonary embolism. Hematol. Am. Soc. Hematol. Educ. Program. 2020, 2020, 195–200. [Google Scholar] [CrossRef]
- Goldberg, J.B.; Giri, J.; Kobayashi, T.; Ruel, M.; Mittnacht, A.J.C.; Rivera-Lebron, B.; DeAnda, A., Jr.; Moriarty, J.M.; MacGillivray, T.E. Surgical Management and Mechanical Circulatory Support in High-Risk Pulmonary Embolisms: Historical Context, Current Status, and Future Directions: A Scientific Statement from the American Heart Association. Circulation 2023, 147, e628–e647. [Google Scholar] [CrossRef]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis with R: A Hands-On Guide; Chapman and Hall/CRC: Boca Raton, FL, USA, 2021. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boey, J.J.E.; Dhundi, U.; Ling, R.R.; Chiew, J.K.; Fong, N.C.-J.; Chen, Y.; Hobohm, L.; Nair, P.; Lorusso, R.; MacLaren, G.; et al. Extracorporeal Membrane Oxygenation for Pulmonary Embolism: A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 64. https://doi.org/10.3390/jcm13010064
Boey JJE, Dhundi U, Ling RR, Chiew JK, Fong NC-J, Chen Y, Hobohm L, Nair P, Lorusso R, MacLaren G, et al. Extracorporeal Membrane Oxygenation for Pulmonary Embolism: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(1):64. https://doi.org/10.3390/jcm13010064
Chicago/Turabian StyleBoey, Jonathan Jia En, Ujwal Dhundi, Ryan Ruiyang Ling, John Keong Chiew, Nicole Chui-Jiet Fong, Ying Chen, Lukas Hobohm, Priya Nair, Roberto Lorusso, Graeme MacLaren, and et al. 2024. "Extracorporeal Membrane Oxygenation for Pulmonary Embolism: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 1: 64. https://doi.org/10.3390/jcm13010064