
Surgically Resected Cardiac Angiosarcoma: Survival Analysis from the National Cancer Database

 ,
,  , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Outcomes of Interest
2.3. Statistical Analysis
3. Results
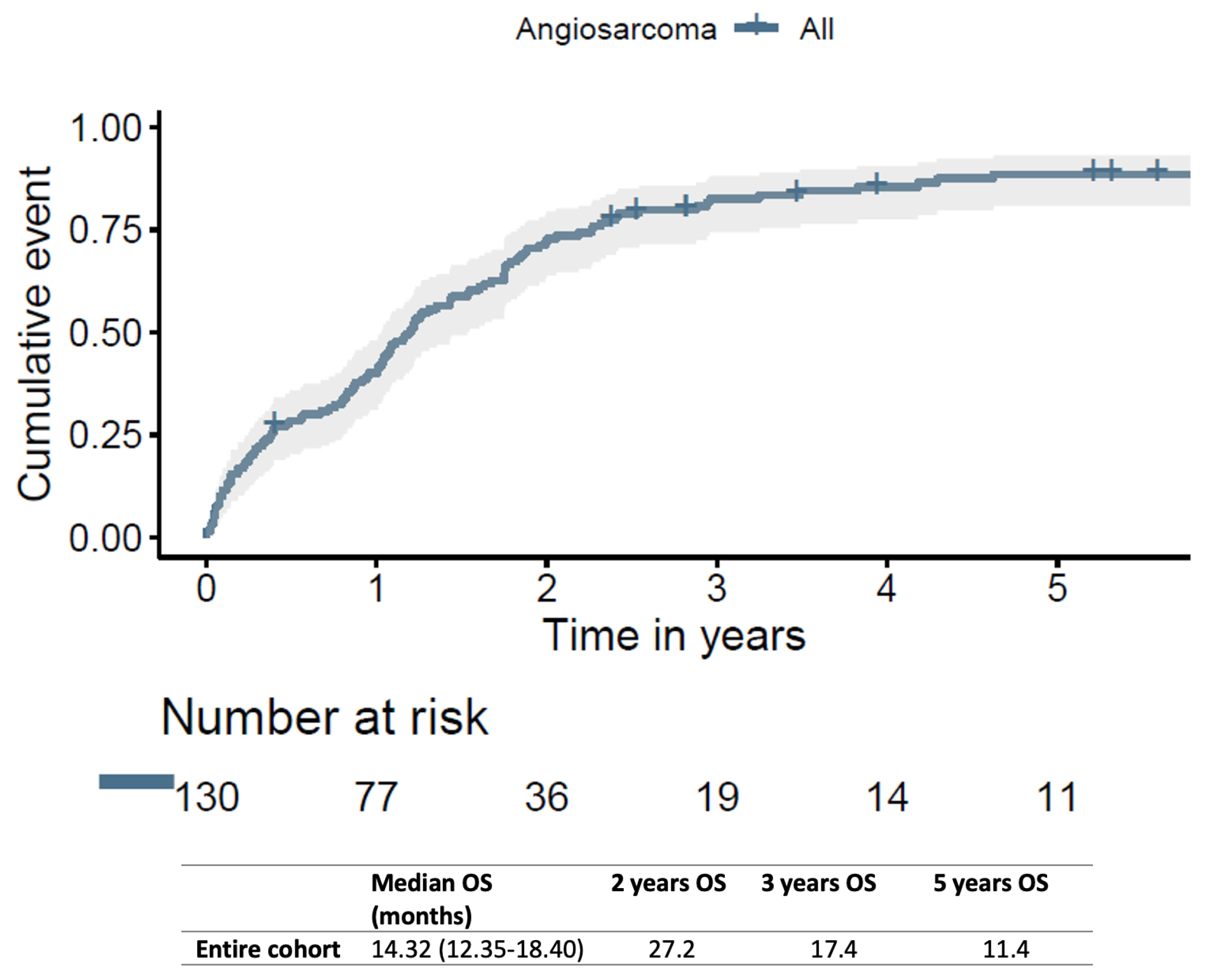
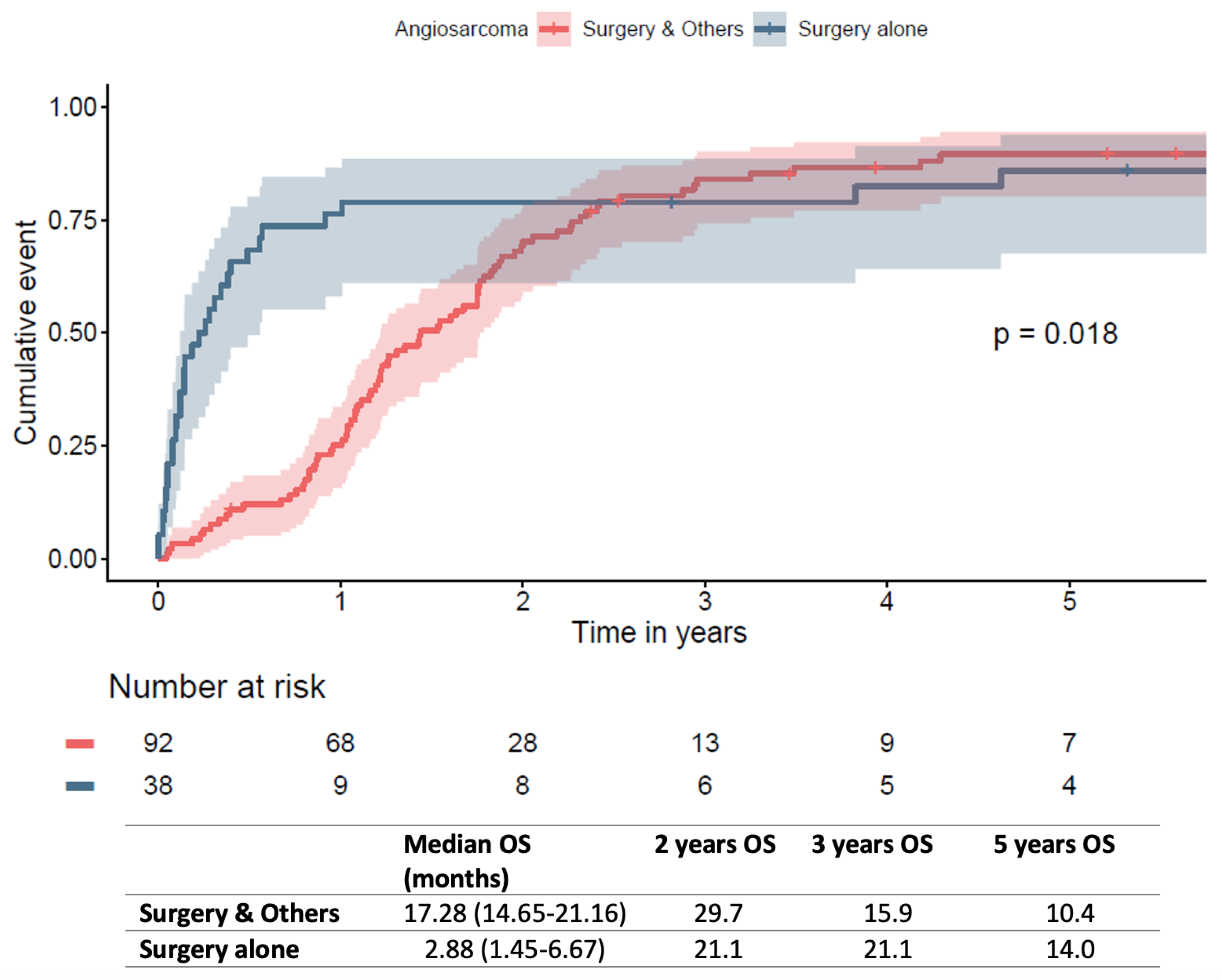
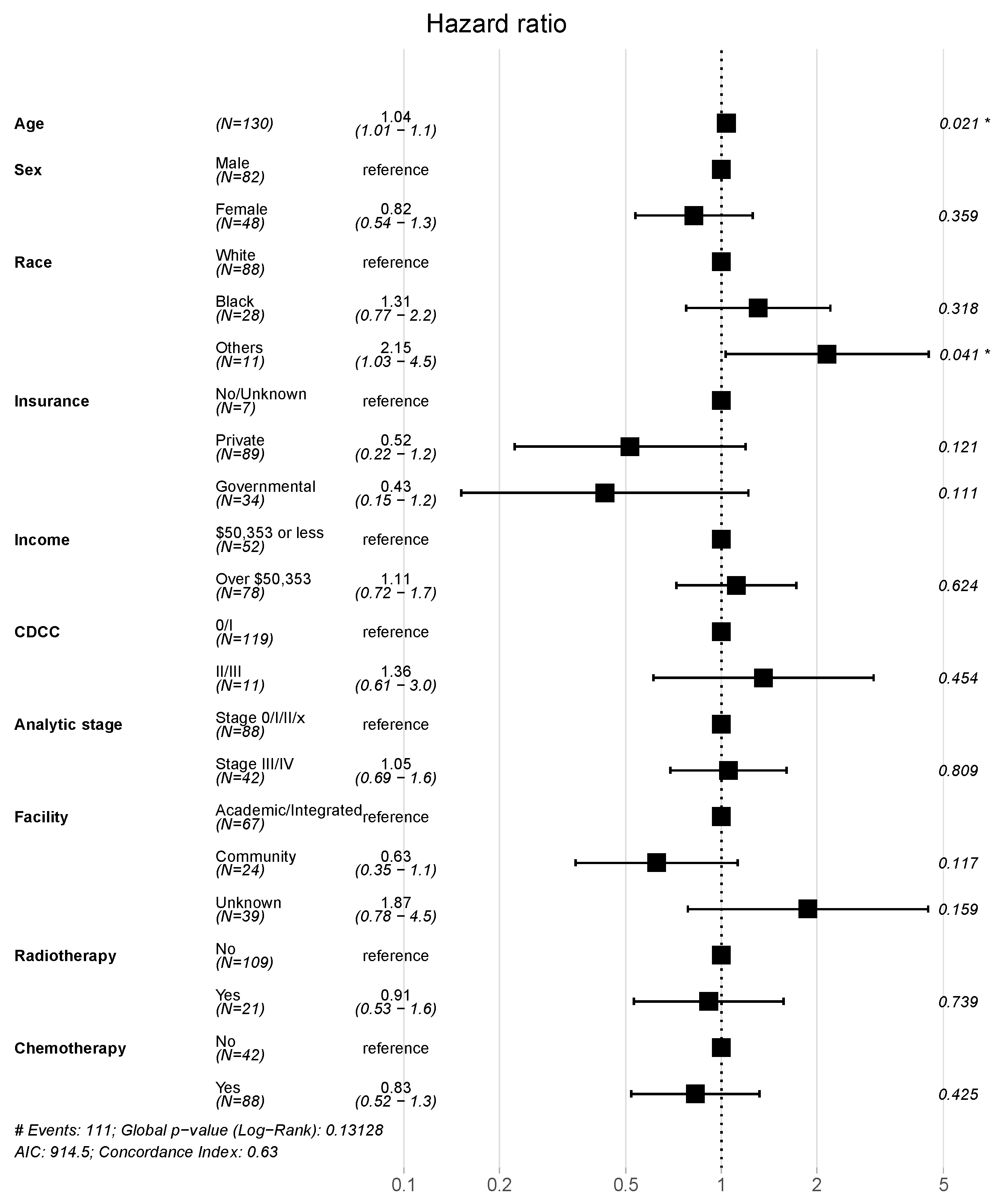
Survival Analysis
4. Discussion
Limitations

5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rahouma, M.; Arisha, M.J.; Elmously, A.; El-Sayed Ahmed, M.M.; Spadaccio, C.; Mehta, K.; Baudo, M.; Kamel, M.; Mansor, E.; Ruan, Y.; et al. Cardiac Tumors Prevalence and Mortality: A Systematic Review and Meta-Analysis. Int. J. Surg. 2020, 76, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Lima, N.d.A.; Byers-Spencer, K.; Cwikla, K.; Huffman, C.; Diaz, M.; Melgar, T.A.; Helmstetter, N. Benign Cardiac Neoplasms in the United States: A Thirteen-Year Review. Cardiology 2021, 146, 748–753. [Google Scholar] [CrossRef] [PubMed]
- Leja, M.J.; Shah, D.J.; Reardon, M.J. Primary Cardiac Tumors. Tex. Heart Inst. J. 2011, 38, 261–262. [Google Scholar] [PubMed]
- Butany, J.; Nair, V.; Naseemuddin, A.; Nair, G.M.; Catton, C.; Yau, T. Cardiac Tumours: Diagnosis and Management. Lancet Oncol. 2005, 6, 219–228. [Google Scholar] [CrossRef]
- Luo, L.; Zhao, W.; Wang, Y.; Liu, K. Cardiac Angiosarcoma: A Case Report and Review of the Literature. Echocardiography 2021, 38, 2083–2090. [Google Scholar] [CrossRef]
- Rahouma, M.; Baudo, M.; Dabsha, A.; Dimagli, A.; Mohamed, A.; Mick, S.L.; Girardi, L.; Gaudino, M.; Lorusso, R. Outcomes of Octogenarians with Primary Malignant Cardiac Tumors: National Cancer Database Analysis. J. Clin. Med. 2022, 11, 4899. [Google Scholar] [CrossRef]
- Poterucha, T.J.; Kochav, J.; O’Connor, D.S.; Rosner, G.F. Cardiac Tumors: Clinical Presentation, Diagnosis, and Management. Curr. Treat. Options Oncol. 2019, 20, 66. [Google Scholar] [CrossRef]
- Torabi, S.; Arjomandi Rad, A.; Vardanyan, R.; Lopuszko, A.T.; Van den Eynde, J.; Zubarevich, A.; Sá, M.P.B.O.; Szczechowicz, M.; Weymann, A. Surgical and Multimodality Treatment of Cardiac Sarcomas: A Systematic Review and Meta-Analysis. J. Card. Surg. 2021, 36, 2476–2485. [Google Scholar] [CrossRef]
- Patel, S.D.; Peterson, A.; Bartczak, A.; Lee, S.; Chojnowski, S.; Gajewski, P.; Loukas, M. Primary Cardiac Angiosarcoma—A Review. Med. Sci. Monit. 2014, 20, 103–109. [Google Scholar] [CrossRef]
- Butany, J.; Yu, W. Cardiac Angiosarcoma: Two Cases and a Review of the Literature. Can. J. Cardiol. 2000, 16, 197–205. [Google Scholar]
- Ge, Y.; Ro, J.Y.; Kim, D.; Kim, C.H.; Reardon, M.J.; Blackmon, S.; Zhai, J.; Coffey, D.; Benjamin, R.S.; Ayala, A.G. Clinicopathologic and Immunohistochemical Characteristics of Adult Primary Cardiac Angiosarcomas: Analysis of 10 Cases. Ann. Diagn. Pathol. 2011, 15, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Rahouma, M.; Baudo, M.; Shmushkevich, S.; Chadow, D.; Mohamed, A.; Girardi, L.; Gaudino, M.; Lorusso, R. Sex Differences in Primary Malignant Cardiac Tumors: A Multi-Institutional Cohort Study from National Cancer Database. J. Card. Surg. 2022, 37, 1275–1286. [Google Scholar] [CrossRef]
- Janigan, D.T.; Husain, A.; Robinson, N.A. Cardiac Angiosarcomas. A Review and a Case Report. Cancer 1986, 57, 852–859. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, A.; Ferlosio, A.; Roselli, M.; Chiariello, L.; Spagnoli, L.G. Cardiac Sarcomas: An Update. J. Thorac. Oncol. 2010, 5, 1483–1489. [Google Scholar] [CrossRef] [PubMed]
- Rahouma, M.; Tafuni, A.; Dabsha, A.; Baudo, M.; Khairallah, S.; Corradi, D.; Gaudino, M.; Lorusso, R. Outcomes of Surgery in Cardiac Angiosarcoma. JACC Cardio Oncol. 2023, 5, 259–261. [Google Scholar] [CrossRef] [PubMed]
- Yanagawa, B.; Mazine, A.; Chan, E.Y.; Barker, C.M.; Gritti, M.; Reul, R.M.; Ravi, V.; Ibarra, S.; Shapira, O.M.; Cusimano, R.J.; et al. Surgery for Tumors of the Heart. Semin. Thorac. Cardiovasc. Surg. 2018, 30, 385–397. [Google Scholar] [CrossRef] [PubMed]
- Simpson, L.; Kumar, S.K.; Okuno, S.H.; Schaff, H.V.; Porrata, L.F.; Buckner, J.C.; Moynihan, T.J. Malignant Primary Cardiac Tumors: Review of a Single Institution Experience. Cancer 2008, 112, 2440–2446. [Google Scholar] [CrossRef]
- Antonuzzo, L.; Rotella, V.; Mazzoni, F.; Doni, L.; Bianchini, D.; Garbini, F.; Maio, V.; Di Costanzo, F. Primary Cardiac Angiosarcoma: A Fatal Disease. Case Rep. Med. 2009, 2009, 591512. [Google Scholar] [CrossRef]
- Hendriksen, B.S.; Stahl, K.A.; Hollenbeak, C.S.; Taylor, M.D.; Vasekar, M.K.; Drabick, J.J.; Conte, J.V.; Soleimani, B.; Reed, M.F. Postoperative Chemotherapy and Radiation Improve Survival Following Cardiac Sarcoma Resection. J. Thorac. Cardiovasc. Surg. 2021, 161, 110–119.e4. [Google Scholar] [CrossRef]
- Engelhardt, K.E.; DeCamp, M.M.; Yang, A.D.; Bilimoria, K.Y.; Odell, D.D. Treatment Approaches and Outcomes for Primary Mediastinal Sarcoma: Analysis of 976 Patients. Ann. Thorac. Surg. 2018, 106, 333–339. [Google Scholar] [CrossRef]
- Reardon, M.J.; Walkes, J.-C.; Benjamin, R. Therapy Insight: Malignant Primary Cardiac Tumors. Nat. Clin. Pract. Cardiovasc. Med. 2006, 3, 548–553. [Google Scholar] [CrossRef] [PubMed]
- Molina, J.E.; Edwards, J.E.; Ward, H.B. Primary Cardiac Tumors: Experience at the University of Minnesota. Thorac. Cardiovasc. Surg. 1990, 38 (Suppl. 2), 183–191. [Google Scholar] [CrossRef] [PubMed]
- Sultan, I.; Bianco, V.; Habertheuer, A.; Kilic, A.; Gleason, T.G.; Aranda-Michel, E.; Harinstein, M.E.; Martinez-Meehan, D.; Arnaoutakis, G.; Okusanya, O. Long-Term Outcomes of Primary Cardiac Malignancies: Multi-Institutional Results From the National Cancer Database. J. Am. Coll. Cardiol. 2020, 75, 2338–2347. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Overall | Short Survivors | Intermediate Survivors | Late Survivors ** | p | p (≥3 vs. <3 Years) | |
|---|---|---|---|---|---|---|
| N | 130 | 94 | 17 | 19 | ||
| Age (median [IQR]) | 50.5 [37.0, 62.0] | 51.5 [37.0, 62.75] | 48.0 [43.0, 58.0] | 45.0 [35.5, 56.5] | 0.510 | 0.264 |
| Female sex | 48 (36.9) | 35 (73%) | 6 (13%) | 7 (15%) | 0.999 | 0.999 |
| Race (%) | 0.487 | 0.375 | ||||
| · White | 88 (69.3) | 60 (68%) | 14 (16%) | 14 (16%) | ||
| · Black | 28 (22.0) | 21 (75%) | 2 (7.1%) | 5 (18%) | ||
| · Others | 11 (8.7) | 10 (91%) | 1 (9.1%) | 0 (0%) | ||
| Insurance status | 0.319 | 0.329 | ||||
| · No insurance/unknown | 7 (5.4) | 5 (71%) | 2 (29%) | 0 (0%) | ||
| · Private | 89 (68.5) | 61 (69%) | 12 (13%) | 16 (18%) | ||
| · Governmental | 34 (26.2) | 28 (82%) | 3 (8.8%) | 3 (8.8%) | ||
| Median income quartile (%) | 0.898 | 0.924 | ||||
| · Less than USD 40,227 | 16 (12.9) | 11 (69%) | 2 (13%) | 3 (19%) | ||
| · USD 40,227–USD 50,353 | 30 (24.2) | 21 (70%) | 5 (17%) | 4 (13%) | ||
| · USD 50,354–USD 63,332 | 34 (27.4) | 26 (76%) | 2 (5.9%) | 6 (18%) | ||
| · USD 63,333 or more | 44 (35.5) | 33 (75%) | 5 (11%) | 6 (14%) | ||
| Urban/rural counties (%) | 0.313 | 0.194 | ||||
| · Metropolitan | 110 (87.3) | 82 (75%) | 13 (12%) | 15 (14%) | ||
| · Urban | 11 (8.7) | 9 (82%) | 1 (9.1%) | 1 (9.1%) | ||
| · Rural | 5 (4.0) | 2 (40%) | 1 (20%) | 2 (40%) | ||
| No high school graduate quartile (%) | 0.923 | 0.675 | ||||
| · 17.6% or more | 21 (16.9) | 15 (71%) | 3 (14%) | 3 (14%) | ||
| · 10.9%–17.5% | 36 (29.0) | 26 (72%) | 4 (11%) | 6 (17%) | ||
| · 6.3%–10.8% | 32 (25.8) | 26 (81%) | 3 (9.4%) | 3 (9.4%) | ||
| · Less than 6.3% | 35 (28.2) | 24 (69%) | 4 (11%) | 7 (20%) | ||
| Great circle distance (miles; median [IQR]) | 18.30 [7.70, 50.80] | 11.90 [6.50, 42.30] | 38.50 [19.77, 629.75] | 25.70 [5.65, 72.35] | 0.057 | 0.874 |
| CDCC (0 or 1/2 or 3) (%) * | 119/11 (91.5/8.5) | 85/9 (90.4/9.6) | 15/2 (88.2/11.8) | 19/0 (100/0) | 0.357 | 0.366 |
| Year of diagnosis (median [IQR]) | 2010 [2007, 2013] | 2010 [2007, 2013] | 2013 [2008, 2015] | 2010 [2008.5, 2012] | 0.112 | 0.560 |
| Grade (poorly differentiated/anaplastic) (%) | 63 (48.5) | 46 (73%) | 10 (16%) | 7 (11%) | 0.458 | 0.326 |
| Tumor size (in mm; median [IQR]) | 60.0 [45.0, 85.0] | 60.0 [48.5, 87.0] | 48.0 [40.0, 74.75] | 70.0 [50.25, 81.5] | 0.437 | 0.606 |
| Analytic stage group (%) | 0.146 | 0.121 | ||||
| · Stage x/0/I | 73 (56.2) | 55 (75%) | 11 (15%) | 7 (9.6%) | ||
| · Stage II | 15 (11.5) | 8 (53%) | 3 (20%) | 4 (27%) | ||
| · Stage III/IV | 42 (32.3) | 31 (74%) | 3 (7.1%) | 8 (19%) | ||
| Facility type (%) | 0.173 | 0.797 | ||||
| · Academic/integrated | 67 (51.5) | 51 (76%) | 7 (10%) | 9 (13%) | ||
| · Community | 24 (18.5) | 14 (58%) | 7 (29%) | 3 (13%) | ||
| · Unknown | 39 (30.0) | 29 (74%) | 3 (7.7%) | 7 (18%) | ||
| Radiation (%) | 21 (16.2) | 15 (71%) | 1 (4.8%) | 5 (24%) | 0.251 | 0.192 |
| Chemotherapy (%) | 88 (67.7) | 62 (70%) | 15 (17%) | 11 (13%) | 0.107 | 0.426 |
| 30-day mortality (alive/dead) (%) | 116/14 (89.2/10.8) | 80/14 (85.1/14.9) | 17/0 (100/0) | 19/0 (100/0) | 0.055 | 0.221 |
| Vital status (alive/dead) (%) | 16/114 (12.3/87.7) | 1/93 (1.1/98.9) | 4/13 (23.5/76.5) | 11/8 (57.9/42.1) | <0.001 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahouma, M.; Baudo, M.; Khairallah, S.; Lau, C.; Gaudino, M.; El-Sayed Ahmed, M.M.; Kumar, A.; Lorusso, R.; Mick, S.L. Surgically Resected Cardiac Angiosarcoma: Survival Analysis from the National Cancer Database. J. Clin. Med. 2023, 12, 7764. https://doi.org/10.3390/jcm12247764
Rahouma M, Baudo M, Khairallah S, Lau C, Gaudino M, El-Sayed Ahmed MM, Kumar A, Lorusso R, Mick SL. Surgically Resected Cardiac Angiosarcoma: Survival Analysis from the National Cancer Database. Journal of Clinical Medicine. 2023; 12(24):7764. https://doi.org/10.3390/jcm12247764
Chicago/Turabian StyleRahouma, Mohamed, Massimo Baudo, Sherif Khairallah, Christopher Lau, Mario Gaudino, Magdy M. El-Sayed Ahmed, Akshay Kumar, Roberto Lorusso, and Stephanie L. Mick. 2023. "Surgically Resected Cardiac Angiosarcoma: Survival Analysis from the National Cancer Database" Journal of Clinical Medicine 12, no. 24: 7764. https://doi.org/10.3390/jcm12247764