
Resection of a Solitary Right Ventricular Metastasis in Oligorecurrent Hepatocellular Carcinoma
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
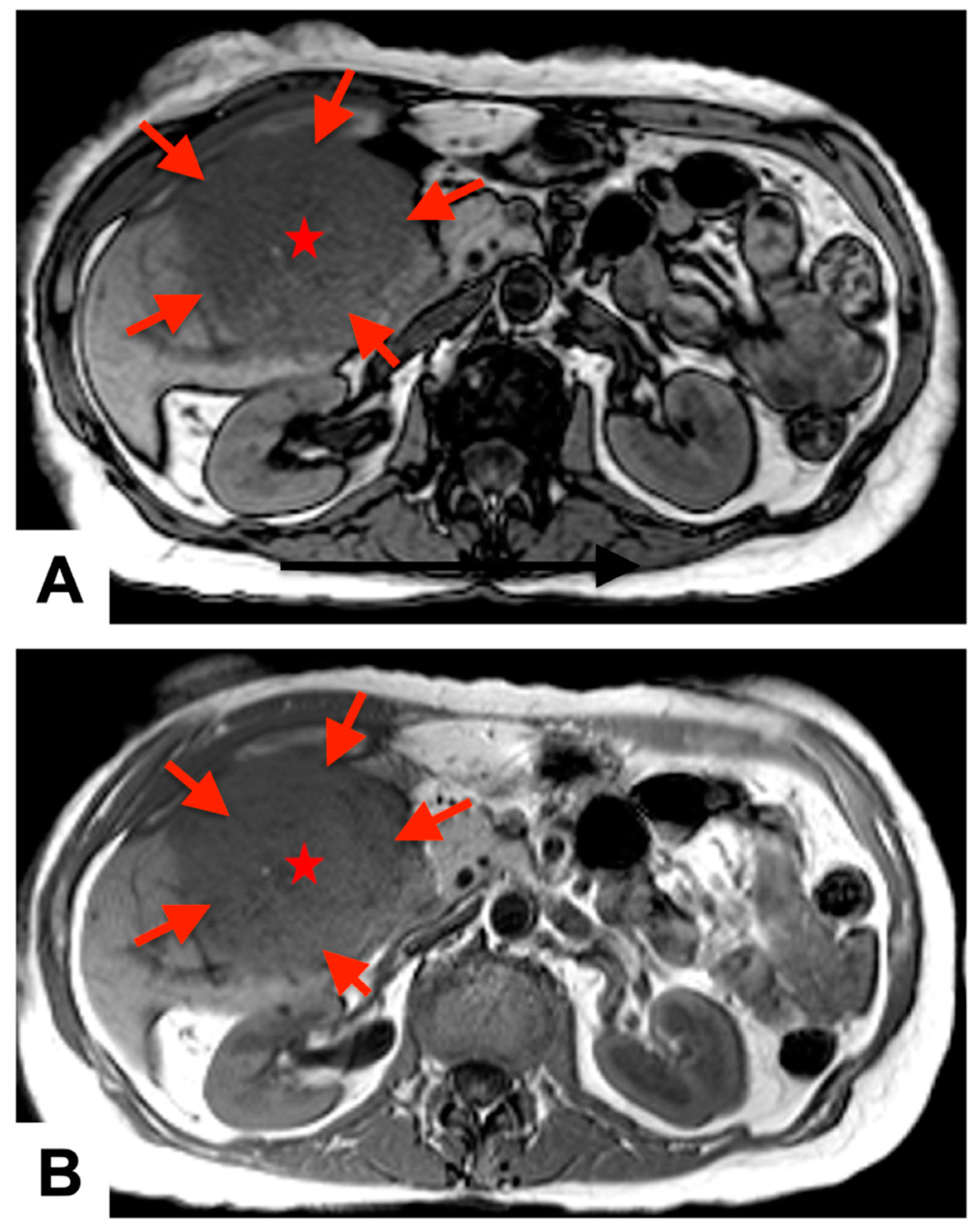
1.1. Case Report
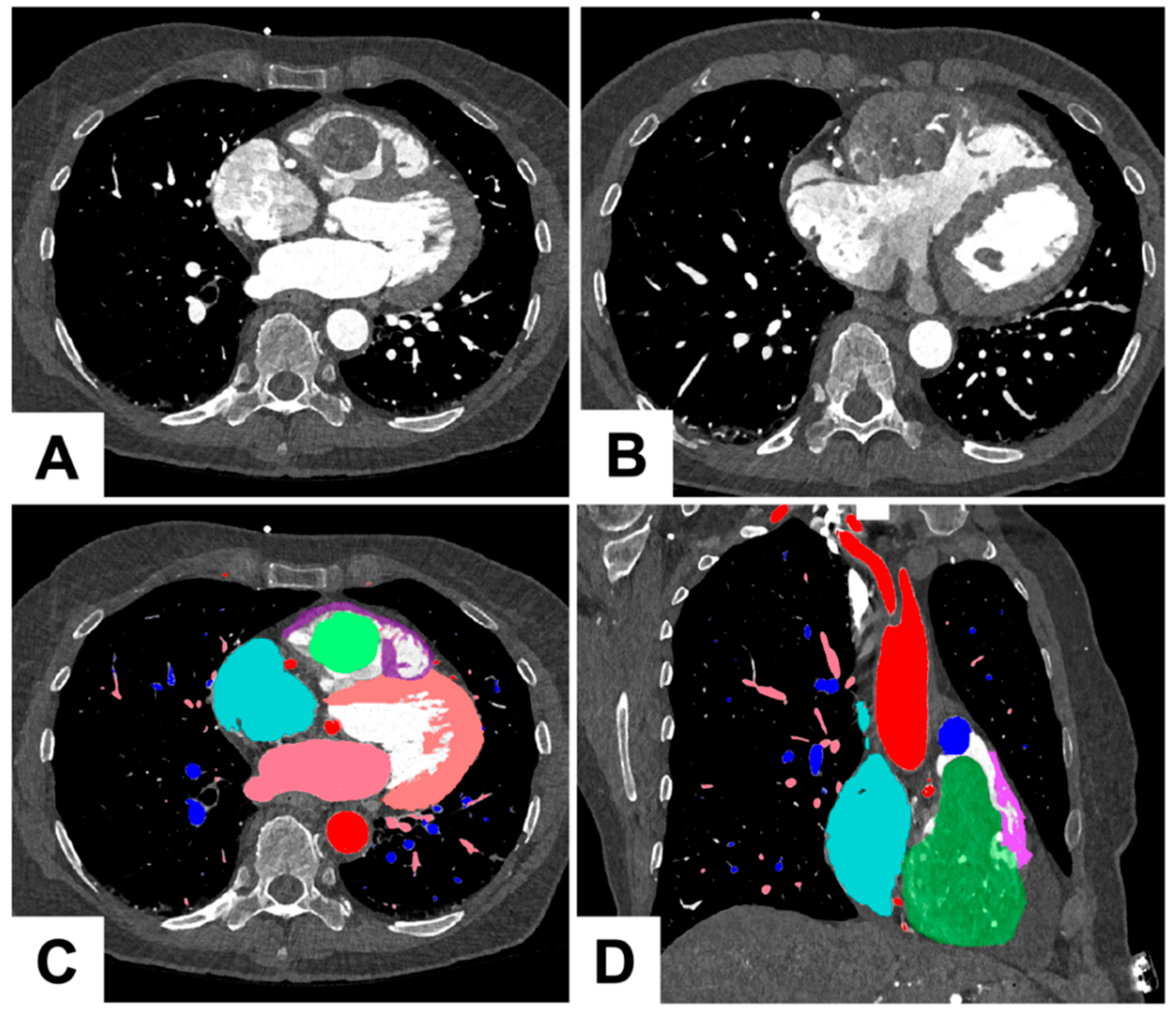
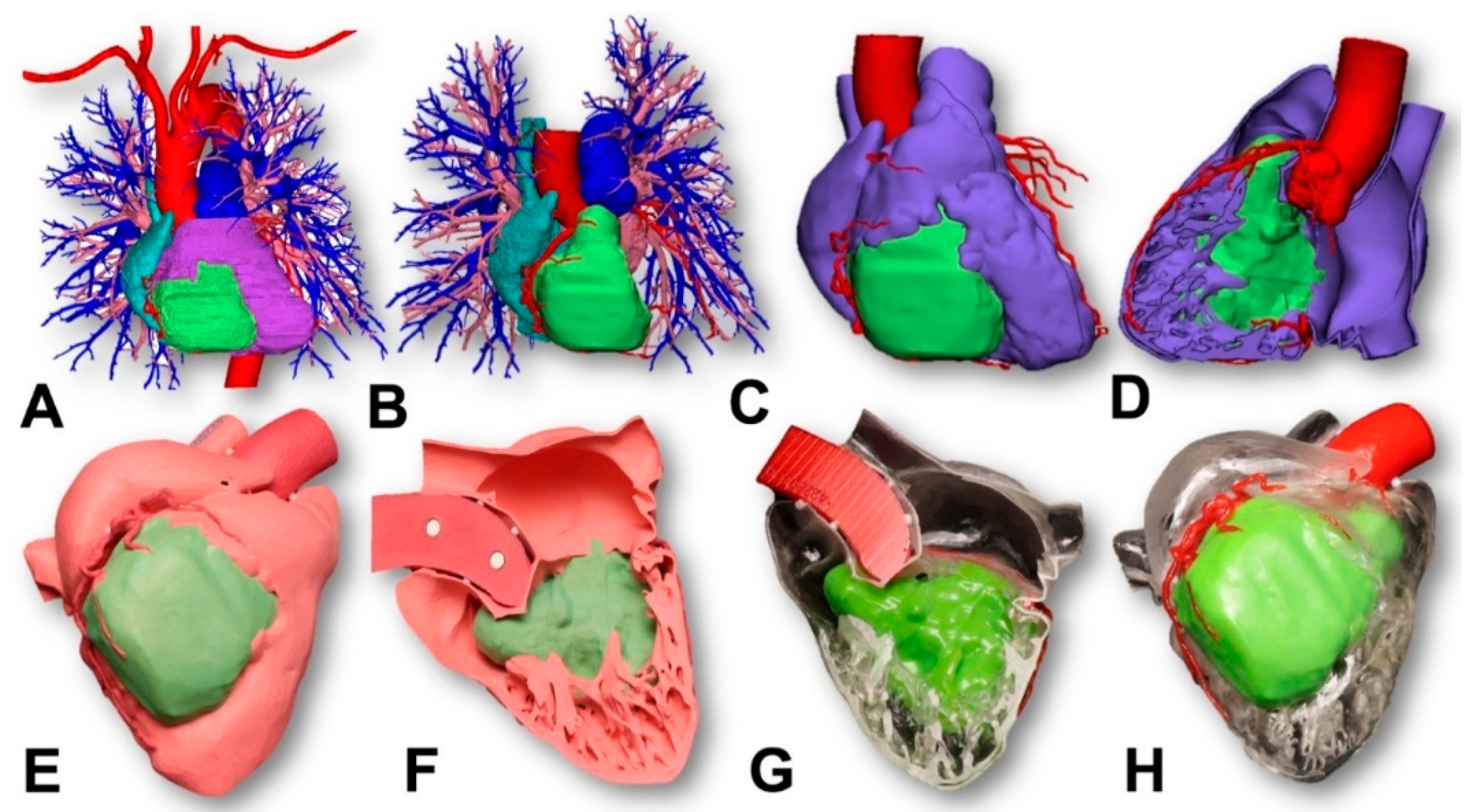
1.2. Three Dimensional Printing Process for the Tumor
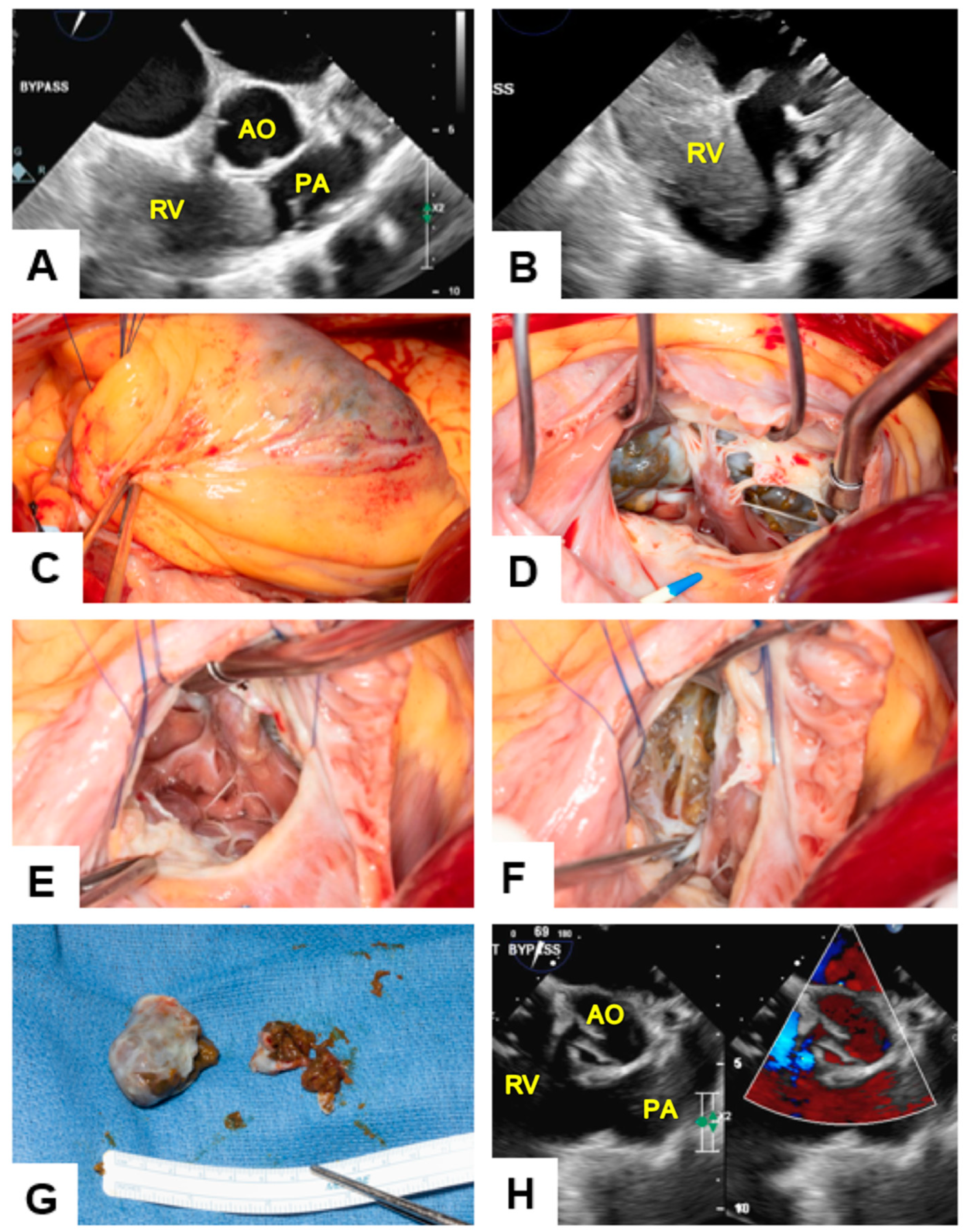
1.3. Surgical Procedure
2. Discussion
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HCC | Hepatocellular carcinoma |
| MRI | Magnetic resonance imaging |
| RV | Right ventricle |
| CT | Computed tomography |
| RVOT | Right ventricular outflow tract |
| RCA | Right coronary artery |
| TV | Tricuspid valve |
| TEE | Transesophageal echocardiogram |
| LVEF | Left ventricular ejection fraction |
| LV | Left ventricle |
| CAD | Computer-aided diagnosis |
References
- Ahmedin, J.; Ward, E.M.; Johnson, C.J.; Cronin, K.A.; Ma, J.; Ryerson, B.; Mariotto, A.; Lake, A.J.; Wilson, R.; Sherman, R.L.; et al. Annual Report to the Nation on the Status of Cancer, 1975–2014, Featuring Survival. J. Natl. Cancer Inst. 2017, 109, djx030. [Google Scholar]
- Zhang, X.T.; Li, Y.; Ren, S.H.; Ren, W.D.; Song, G.; Xiao, Y.J.; Sun, F.F.; Sun, L.; Yang, X.H.; Tan, X.Y. Isolated metastasis of hepatocellular carcinoma in the right ventricle. BMC Cardiovasc. Disord. 2019, 19, 287. [Google Scholar] [CrossRef] [PubMed]
- Kotani, E.; Kiuchi, K.; Takayama, M.; Takano, T.; Tabata, M.; Aramaki, T.; Kawamata, H. Effectiveness of transcoronary chemoembolization for metastatic right ventricular tumor derived from hepatocellular carcinoma. Chest 2000, 117, 287–289. [Google Scholar] [CrossRef] [PubMed]
- Gaurav, J.; Otto, M.; Abdul, M.K.M.; Chadha, M.; Sahajpal, A. Cardiac Metastasis After Curative Treatment of Hepatocellular Carcinoma: Assessment of Risk Factors, Treatment Options, and Prognosis. J. Patient Centered Res. Rev. 2022, 9, 181–184. [Google Scholar]
- Kawakami, M.; Koda, M.; Mandai, M.; Hosho, K.; Murawaki, Y.; Oda, W.; Hayashi, K. Isolated metastases of hepatocellular carcinoma in the right atrium: Case report and review of the literature. Oncol. Lett. 2013, 5, 1505–1508. [Google Scholar] [CrossRef]
- Little, M.P.; Azizova, T.V.; Richardson, D.B.; Tapio, S.; Bernier, M.O.; Kreuzer, M.; Cucinotta, F.A.; Bazyka, D.; Chumak, V.; Ivanov, V.K.; et al. Ionising radiation and cardiovascular disease: Systematic review and meta-analysis. BMJ 2023, 380, e072924. [Google Scholar] [CrossRef]
- Darby, S.C.; Ewertz, M.; McGale, P.; Bennet, A.M.; Blom-Goldman, U.; Brønnum, D.; Correa, C.; Cutter, D.; Gagliardi, G.; Gigante, B.; et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N. Engl. J. Med. 2013, 368, 987–998. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ergi, D.G.; Klarich, K.W.; Dearani, J.A.; Crestanello, J.A.; Maleszewski, J.J.; Morris, J.M.; Young, P.M.; Callaghan, C.M.; Pitot, H.C.; Arghami, A. Resection of a Solitary Right Ventricular Metastasis in Oligorecurrent Hepatocellular Carcinoma. J. Clin. Med. 2023, 12, 7530. https://doi.org/10.3390/jcm12247530
Ergi DG, Klarich KW, Dearani JA, Crestanello JA, Maleszewski JJ, Morris JM, Young PM, Callaghan CM, Pitot HC, Arghami A. Resection of a Solitary Right Ventricular Metastasis in Oligorecurrent Hepatocellular Carcinoma. Journal of Clinical Medicine. 2023; 12(24):7530. https://doi.org/10.3390/jcm12247530
Chicago/Turabian StyleErgi, Defne Gunes, Kyle W. Klarich, Joseph A. Dearani, Juan A. Crestanello, Joseph J. Maleszewski, Jonathan M. Morris, Phillip M. Young, Cameron M. Callaghan, Henry C. Pitot, and Arman Arghami. 2023. "Resection of a Solitary Right Ventricular Metastasis in Oligorecurrent Hepatocellular Carcinoma" Journal of Clinical Medicine 12, no. 24: 7530. https://doi.org/10.3390/jcm12247530