

Electrical Impedance Tomography during Abdominal Laparoscopic Surgery: A Physiological Pilot Study
 , ,
, ,
Abstract
:1. Introduction
2. Methods
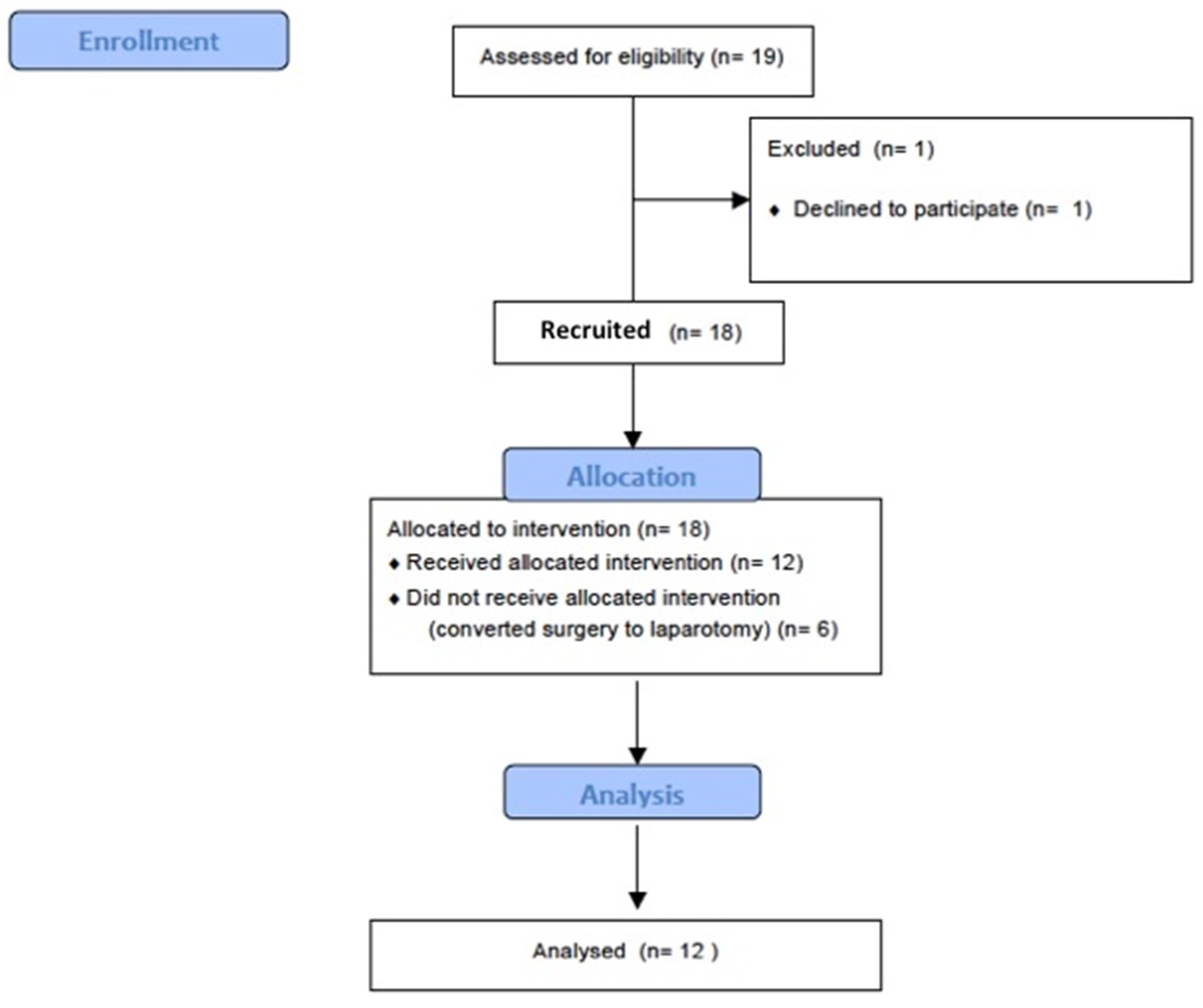
2.1. Patient Selection
2.2. Anesthesia Management
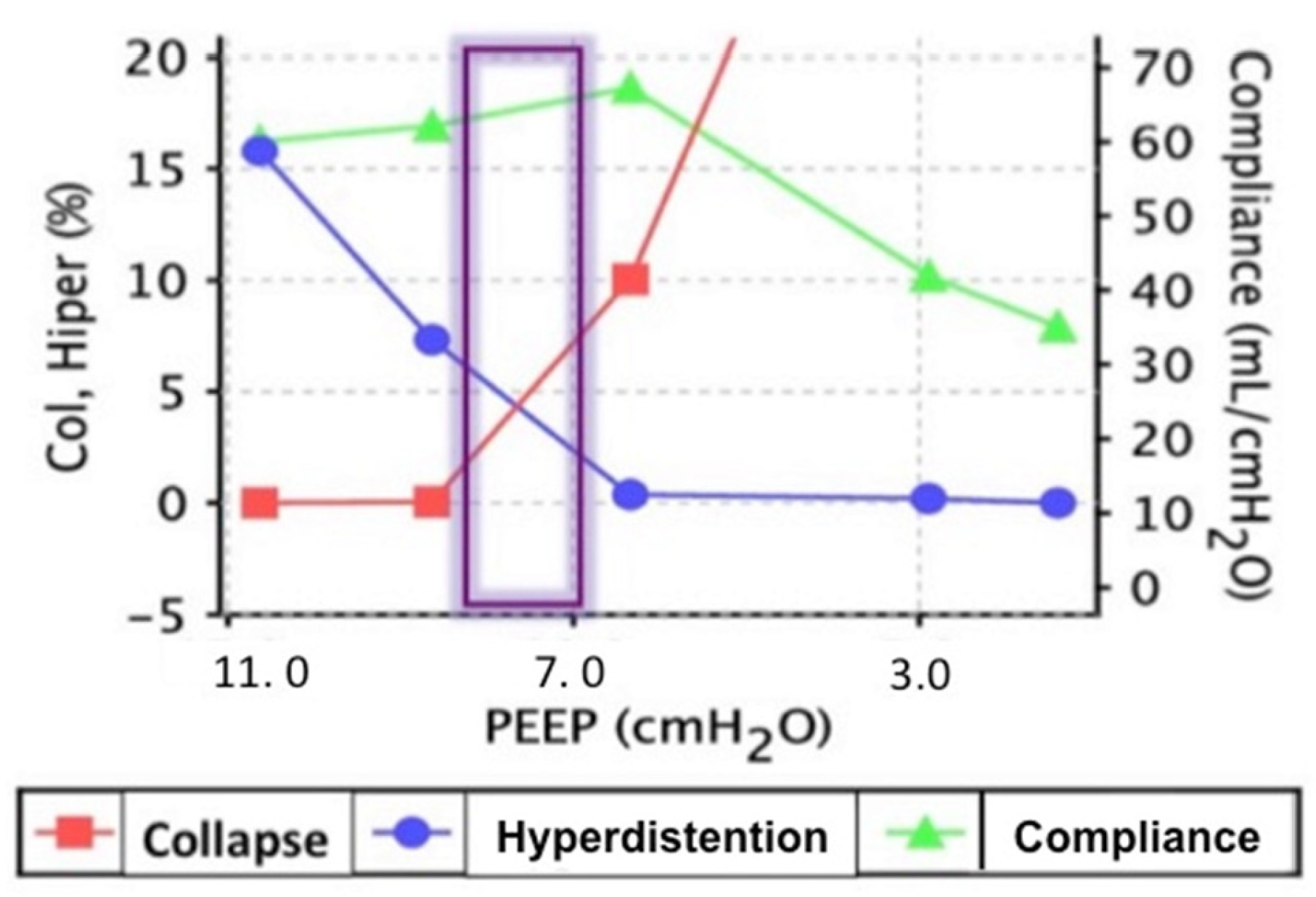
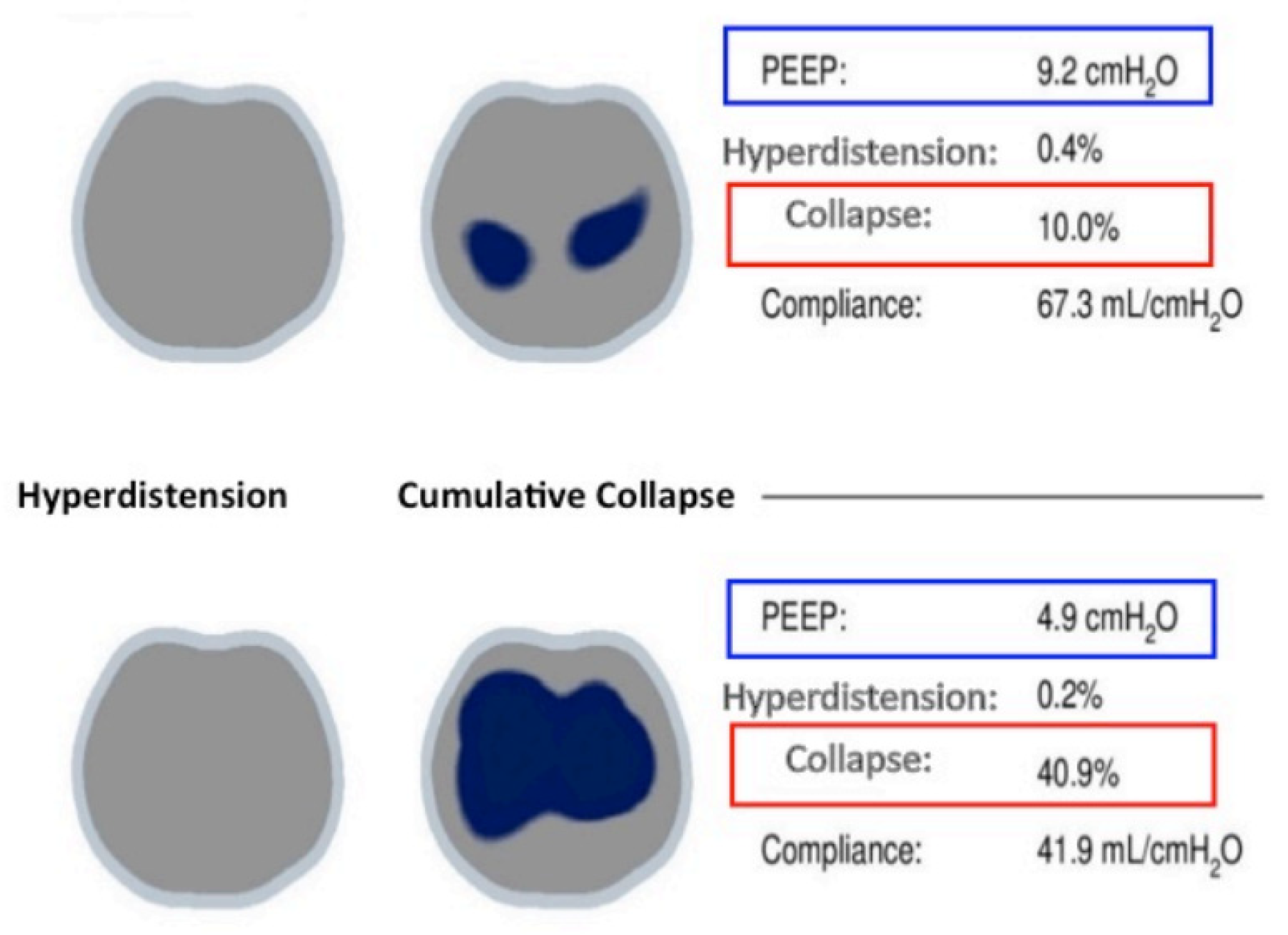
2.3. Respiratory Mechanics and Ventilation Setting
2.4. Sample Size and Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bendixen, H.H.; Hedley-Whyte, J.; Laver, M.B. Impaired oxygenation in surgical patients during general anesthesia with controlled ventilation. A concept of atelectasis. N. Engl. J. Med. 1963, 269, 991–996. [Google Scholar] [CrossRef]
- Brismar, B.; Hedenstierna, G.; Lundquist, H.; Strandberg, A.; Svensson, L.; Tokics, L. Pulmonary densities during anesthesia with muscular relaxation–a proposal of atelectasis. Anesthesiology 1985, 62, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Reinius, H.; Jonsson, L.; Gustafsson, S.; Sundbom, M.; Duvernoy, O.; Pelosi, P.; Hedenstierna, G.; Freden, F. Prevention of atelectasis inmorbidly obese patients during general anesthesia and paralysis: A computerized tomography study. Anesthesiology 2009, 111, 979–987. [Google Scholar] [CrossRef] [PubMed]
- Ranucci, M.; Ballotta, A.; La Rovere, M.T.; Castelvecchio, S. Postoperative hypoxia and length of intensive care unit stay after cardiac surgery: The underweight paradox? PLoS ONE 2014, 9, e93992. [Google Scholar] [CrossRef] [PubMed]
- Andersson, L.E.; Baath, M.; Thorne, A.; Aspelin, P.; Odeberg-Wernerman, S. Effect of carbon dioxide pneumoperitoneum on development of atelectasis during anesthesia, examined by spiral computed tomography. Anesthesiology 2005, 102, 293–2994. [Google Scholar] [CrossRef]
- Aldenkortt, M.; Lysakowski, C.; Elia, N.; Brochard, L.; Tramèr, M.R. Ventilation strategies in obese patients undergoing surgery: A quantitative systematic review and meta-analysis. Br. J. Anaesth. 2012, 109, 493–502. [Google Scholar] [CrossRef] [PubMed]
- D’Antini, D.; Rauseo, M.; Grasso, S.; Mirabella, L.; Camporota, L.; Cotoia, A.; Spadaro, S.; Fersini, A.; Petta, R.; Menga, R.; et al. Physiological effects of the open lung approach during laparoscopic cholecystectomy: Focus on driving pressure. Minerva Anestesiol. 2018, 84, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Cinnella, G.; Grasso, S.; Spadaro, S.; Rauseo, M.; Mirabella, M.; Salatto, P.; De Capraris, A.; Nappi, L.; Greco, P.; Dambrosio, M. Effects of Recruitment Maneuver and Positive End-expiratory Pressure on Respiratory Mechanics and Transpulmonary Pressure during Laparoscopic Surgery. Anesthesiology 2013, 118, 114–122. [Google Scholar] [CrossRef]
- Fogagnolo, A.; Montanaro, F.; Al-Husinat, L.; Turrini, C.; Rauseo, M.; Mirabella, L.; Ragazzi, R.; Ottaviani, I.; Cinnella, G.; Volta, C.A.; et al. Management of Intraoperative Mechanical Ventilation to Prevent Postoperative Complications after General Anesthesia: A Narrative Review. J. Clin. Med. 2021, 10, 2656. [Google Scholar] [CrossRef]
- Rothen, H.U.; Neumann, P.; Berglund, J.E.; Valtysson, J.; Magnusson, A.; Hedenstierna, G. Dynamics of reexpansion of atelectasis during general anaesthesia. Br. J. Anaesth. 1999, 82, 551–556. [Google Scholar] [CrossRef]
- Tusman, G.; Bohm, S.H.; Suarez-Sipmann, F.; Turchetto, E. Alveolar recruitment improves ventilatory efficiency of the lungs during anesthesia. Can. J. Anaesth. 2004, 51, 723–727. [Google Scholar] [CrossRef]
- Oba, Y.; Salzman, G.A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury. N. Engl. J. Med. 2000, 343, 813. [Google Scholar] [PubMed]
- Choi, G.; Wolthuis, E.K.; Bresser, P.; Levi, M.; Van Der Poll, T.; Dzoljic, M.; Vroom, M.B.; Schultz, M.J. Mechanical ventilation with lower tidal volumes and positive end-expiratory pressure prevents alveolar coagulation in patients without lung injury. Anesthesiology 2006, 105, 689–695. [Google Scholar] [CrossRef]
- Wolthuis, E.K.; Choi, G.; Dessing, M.C.; Bresser, P.; Lutter, R.; Dzoljic, M.; van der Poll, T.; Vroom, M.B.; Hollmann, M.; Schultz, M.J. Mechanical ventilation with lower tidal volumes and positive end-expiratory pressure prevents pulmonary inflammation in patients without preexisting lung injury. Anesthesiology 2008, 108, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Costa, E.L.; Borges, J.B.; Melo, A.; Suarez-Sipmann, F.; Toufen, C.; Bohm, S.H.; Amato, M.B. Bedside estimation of recruitable alveolar collapse and hyperdistension by electrical impedance tomography. Intensive Care Med. 2009, 35, 1132–1137. [Google Scholar] [CrossRef]
- Rauseo, M.; Spinelli, E.; Sella, N.; Slobod, D.; Spadaro, S.; Longhini, F.; Giarratano, A.; Gilda, C.; Mauri, T.; Navalesi, P.; et al. Expert opinion document: “Electrical impedance tomography: Applications from the intensive care unit and beyond. J. Anesth. Analg. Crit. Care 2022, 2, 28. [Google Scholar] [CrossRef] [PubMed]
- Karsten, J.; Luepschen, H.; Grossherr, M.; Bruch, H.P.; Leonhardt, S.; Gehring, H.; Meier, T. Effect of PEEP on regional ventilation during laparoscopic surgery monitored by electrical impedance tomography. Acta Anaesthesiol. Scand. 2011, 55, 878–886. [Google Scholar] [CrossRef]
- Bikker, I.G.; Leonhardt, S.; Reis Miranda, D.; Bakker, J.; Gommers, D. Bedside measurement of changes in lung impedance to monitor alveolar ventilation in dependent and non-dependent parts by electrical impedance tomography during a positive end-expiratory pressure trial in mechanically ventilated intensive care unit patients. Crit. Care 2010, 14, R100. [Google Scholar] [CrossRef]
- Bikker, I.G.; Preis, C.; Egal, M.; Bakker, J.; Gommers, D. Electrical impedance tomography measured at two thoracic levels can visualize the ventilation distribution changes at the bedside during a decremental positive end-expiratory lung pressure trial. Crit. Care 2011, 15, R193. [Google Scholar] [CrossRef]
- Yang, F.; Patterson, R.P. The contribution of the lungs to thoracic impedance measurements: A simulation study based on a high resolution finite difference model. Physiol Meas. 2007, 28, S153–S161. [Google Scholar] [CrossRef]
- Adler, A.; Arnold, J.H.; Bayford, R.; Borsic, A.; Brown, B.; Dixon, P.; Faes, T.J.; Frerichs, I.; Gagnon, H.; Gärber, Y. GREIT: A unified approach to 2D linear EIT reconstruction of lung images. Physiol Meas. 2009, 30, S35–S55. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, M.S.; Wania, V.; Bastin, B.; Schmalz, U.; Kienbaum, P.; Beiderlinden, M.; Treschan, T.A. Electrical impedance tomography during major open upper abdominal surgery: A pilot-study. BMC Anesthesiol. 2014, 14, 51. [Google Scholar] [CrossRef]
- Rothen, H.U.; Sporre, B.; Englberg, G.; Wegenius, G.; Hedenstierna, G. Re-expansion of atelectasis during general anaesthesia: A computed tomography study. Br. J. Anaesth. 1993, 71, 788–795. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Jiang, J.; Liu, Y.; Xu, H.; Zhou, S.; Yang, S.; Shi, X.; Yuan, H. Electrical Impedance Tomography guided PEEP Titration in Patients Undergoing Laparoscopic Abdominal Surgery. Medicine 2016, 95, e3306. [Google Scholar] [CrossRef] [PubMed]
- Erlandsson, K.; Odenstedt, H.; Lundin, S.; Stenqvist, O. Positive end-expiratory pressure optimization using electric impedance tomography in morbidly obese patients during laparoscopic gastric bypass surgery. Acta Anaesthesiol. Scand. 2006, 50, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Radke, O.C.; Schneider, T.; Heller, A.R.; Koch, T. Spontaneous breathing during general anesthesia prevents the ventral redistribution of ventilation as detected by electrical impedance tomography: A randomized trial. Anesthesiology 2012, 116, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Bordes, J.; Mazzeo, C.; Gourtobe, P.; Cungi, P.J.; Antonini, F.; Bourgoin, S.; Kaiser, E. Impact of extraperitoneal dioxyde carbon insufflation on respiratory function in anesthetized adults: A Preliminary Study Using Electrical Impedance Tomography and Wash-out/Wash-in Technic. Anesthesiol. Pain Med. 2015, 5, e22845. [Google Scholar] [CrossRef] [PubMed]
- Mols, G.; Priebe, H.; Guttmann, J. Alveolar recruitment in acute lung injury. Br. J. Anaesth. 2006, 96, 156–166. [Google Scholar] [CrossRef]
- Sprung, J.; Whalley, D.G.; Falcone, T.; Warner, D.; Hubmayr, R.; Hammel, J. The impact of morbid obesity, pneumoperitoneum, and posture on respiratory system mechanics and oxygenation during laparoscopy. Anesth. Analg. 2002, 94, 1345–1350. [Google Scholar] [CrossRef]
- Casati, A.; Comotti, L.; Tommasino, C.; Leggieri, C.; Bignami, E.; Tarantino, F.; Torri, G. Effects of pneumoperitoneum and reverse Trendelenburg position on cardiopulmonary function in morbidly obese patients receiving laparoscopic gastric banding. Eur. J. Anaesthesiol. 2000, 17, 300–305. [Google Scholar] [CrossRef]
- Futier, E.; Jaber, S. Lung-protective ventilation in abdominal surgery. Curr. Opin. Crit. Care 2014, 20, 426–430. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient (n.) | Age (yrs) | Sex (M/F) | BMI (Kg/m2) | Comorbidities | ASA | Type of Surgery | Duration of Surgery (min) |
|---|---|---|---|---|---|---|---|
| 1 | 72 | M | 25.9 | DM II | II | Left hemicolectomy | 105 |
| 2 | 79 | F | 28.1 | HTN | II | Right hemicolecthomy | 120 |
| 3 | 69 | F | 25.4 | HTN | II | Left hemicolectomy | 120 |
| 4 | 67 | F | 30.5 | HTN, COPD | II | Ileo-cholic resection | 250 |
| 5 | 68 | F | 23.3 | I | Left hemicolectomy | 315 | |
| 6 | 73 | F | 29.3 | HTN | II | Left hemicolectomy | 180 |
| 7 | 69 | F | 23.9 | HTN | II | Left hemicolectomy | 180 |
| 8 | 77 | F | 26.6 | HTN | II | Right Total colectomy | 240 |
| 9 | 64 | F | 19.3 | CHF | II | Left Total colectomy | 270 |
| 10 | 55 | F | 27.7 | I | Right hemicolecthomy | 210 | |
| 11 | 57 | F | 21.7 | I | Left hemicolectomy | 180 | |
| 12 | 65 | M | 26.5 | HTN | II | Left hemicolectomy | 255 |
| T0 (Baseline) | T1 (IOT) | T2 (Pneumo) | T3 (Pneumo-RM) | T4 (End Surgery) | p Value | |
|---|---|---|---|---|---|---|
| pH | 7.38 ± 0.026 | 7.41 ± 0.06 | 7.37 ± 0.07 | 7.42 ± 0.05 | 7.35 ± 0.05 | 0.182 |
| PaO2 mmHg | 78.1 ± 9.49 | 130 ± 48.1 | 138 ± 42.5 | 149 ± 43.5 | 188 ± 66.7 | <0.001 |
| PaCO2 mmHg | 39.1 ± 3.18 | 37.9 ± 4.44 | 42.4 ± 5.89 | 44.8 ± 5.19 | 40.3 ± 6.85 | 0.075 |
| PaO2/FiO2 | 372 ± 45 | 313 ± 130 | 335 ± 116 | 367 ± 111 | 371 ± 80.4 | 0.819 |
| PAM mmHg | 95.8 ± 15 | 84.2 ± 12.7 | 84.2 ± 14.5 | 81.8 ± 13.5 | 78.5 ± 11.4 | 0.100 |
| HR bpm | 81 ± 11.6 | 75.8 ± 9.86 | 77 ± 9.40 | 72.3 ± 5.06 | 70.6 ± 8.18 | 0.279 |
| Vt mL | 452 ± 74.7 | 426 ± 104 | 425 ± 61.2 | 447 ± 69.5 | 0.747 | |
| Ve L/min | 5.85 ± 0.71 | 5.5 ± 1.16 | 5.85 ± 0.96 | 5.96 ± 1.13 | 0.715 | |
| PEEPext cmH2O | 5.08 ± 0.7 | 5.67 ± 1.23 | 7.91 ± 2.6 | 6.83 ± 2.5 | 0.027 | |
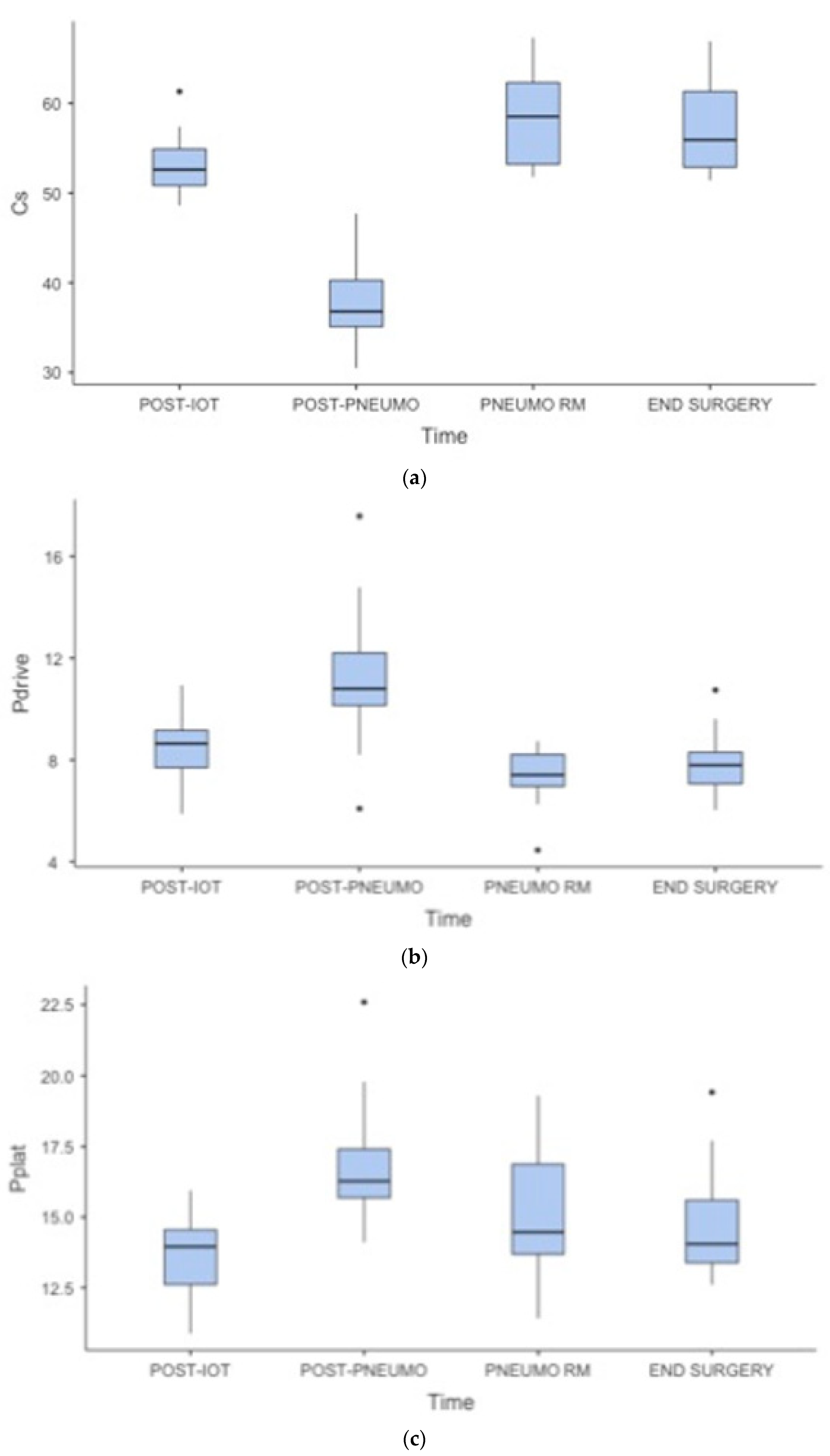
| Pplat cmH2O | 13.6 ± 1.51 | 17 ± 2.3 | 15.2 ± 2.36 | 14.7 ± 2.07 | 0.003 | |
| Pdrive cmH2O | 8.5 ± 1.45 | 11.3 ± 2.96 | 7.33 ± 1.21 | 7.87 ± 1.34 | <0.001 | |
| Cs mL/cmH2O | 53.3 ± 3.54 | 38 ± 4.99 | 58.4 ± 5.43 | 57 ± 5.10 | <0.001 | |
| RR bpm | 12.7 | 13 | 14.3 | 13.6 | 0.174 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rauseo, M.; Spadaro, S.; Mirabella, L.; Cotoia, A.; Laforgia, D.; Gaudino, G.; Vinella, F.; Ferrara, G.; Gattullo, A.; Tullo, L.; et al. Electrical Impedance Tomography during Abdominal Laparoscopic Surgery: A Physiological Pilot Study. J. Clin. Med. 2023, 12, 7467. https://doi.org/10.3390/jcm12237467
Rauseo M, Spadaro S, Mirabella L, Cotoia A, Laforgia D, Gaudino G, Vinella F, Ferrara G, Gattullo A, Tullo L, et al. Electrical Impedance Tomography during Abdominal Laparoscopic Surgery: A Physiological Pilot Study. Journal of Clinical Medicine. 2023; 12(23):7467. https://doi.org/10.3390/jcm12237467
Chicago/Turabian StyleRauseo, Michela, Savino Spadaro, Lucia Mirabella, Antonella Cotoia, Donato Laforgia, Gennaro Gaudino, Francesca Vinella, Giuseppe Ferrara, Adriana Gattullo, Livio Tullo, and et al. 2023. "Electrical Impedance Tomography during Abdominal Laparoscopic Surgery: A Physiological Pilot Study" Journal of Clinical Medicine 12, no. 23: 7467. https://doi.org/10.3390/jcm12237467