
The Use of Oral Anticoagulation Is Not Independently Associated with Mortality in Frail Older Patients with Repeated Falls

 , , and
, , and
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2020, 42, 373–498. [Google Scholar] [CrossRef]
- Cavallari, I.; Patti, G. Efficacy and safety of oral anticoagulation in elderly patients with atrial fibrillation. Anatol. J. Cardiol. 2018, 19, 67–71. [Google Scholar] [CrossRef]
- Zwart, L.; Germans, T.; Simsek, S.; Ruiter, J.; Jansen, R. Atrial Fibrillation, Anticoagulation, and Major Bleeding Episodes in Geriatric Patients at the Risk of Falling. OBM Geriatr. 2019, 3, 1. [Google Scholar] [CrossRef]
- Zwart, L.; Germans, T.; Vogels, R.; Simsek, S.; Hemels, M.; Jansen, R. Frail patients who fall and their risk on major bleeding and intracranial haemorrhage. Outcomes Fall Syncope Regist. BMC Geriatr. 2023, 23, 422. [Google Scholar]
- Zwart, L.A.; Jansen, R.W.; Ruiter, J.H.; Germans, T.; Simsek, S.; Hemels, M.E. Opportunistic screening for atrial fibrillation with a single lead device in geriatric patients. J. Geriatr. Cardiol. 2020, 17, 149–154. [Google Scholar] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Med. Sci. 2001, 56A, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Mitnitski, A. Frailty in Relation to the Accumulation of Deficits. J. Gerontol. Med. Sci. 2007, 62A, 722–727. [Google Scholar] [CrossRef]
- Singh, M.; Stewart, R.; White, H. Importance of frailty in patients with cardiovascular disease. Eur. Heart J. 2014, 35, 1726–1731. [Google Scholar] [CrossRef]
- Pialoux, T.; Goyard, J.; Lesourd, B. Screening tools for frailty in primary health care: A systematic review. Geriatr. Gerontol. Int. 2012, 12, 189–197. [Google Scholar] [CrossRef]
- Bamps, J.; Capouillez, B.; Rinaldi, R.; Patris, S. Frailty detection by healthcare professionals: A systematic review of the available English and French tools and their validation. Eur. Geriatr. Med. 2023, 14, 773–787. [Google Scholar] [CrossRef]
- Dent, E.; Kowal, P.; Hoogendijk, E.O. Frailty measurement in research and clinical practice: A review. Eur. J. Intern. Med. 2016, 31, 3–10. [Google Scholar] [CrossRef]
- Rockwood, K.; Andrew, M.K.; Mitnitski, A. A comparison of two approaches to measuring frailty in elderly people. J. Gerontol. Med. Sci. 2007, 62A, 738–743. [Google Scholar] [CrossRef]
- Proietti, M.; Romiti, G.F.; Vitolo, M.; Harrison, S.L.; Lane, D.A.; Fauchier, L.; Marin, F.; Näbauer, M.; Potpara, T.S.; Dan, G.-A.; et al. Epidemiology and impact of frailty in patients with atrial fibrillation in Europe. Age Ageing 2022, 51, afac192. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Yang, P.-S.; Sung, J.-H.; Jang, E.; Yu, H.T.; Kim, T.-H.; Uhm, J.-S.; Kim, J.-Y.; Pak, H.-N.; Lee, M.-H.; et al. Effectiveness and Safety of Anticoagulation Therapy in Frail Patients with Atrial Fibrillation. Stroke 2022, 53, 1873–1882. [Google Scholar] [CrossRef] [PubMed]
- Perera, V.; Bajorek, B.V.; Matthews, S.; Hilmer, S.N. The impact of frailty on the utilisation of antithrombotic therapy in older patients with atrial fibrillation. Age Ageing 2009, 38, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, C.; Todd, O.; Clegg, A.; Gale, C.P.; Hall, M. Management of atrial fibrillation for older people with frailty: A systematic review and meta-analysis. Age Ageing 2019, 48, 196–203. [Google Scholar] [CrossRef]
- Tulner, L.R.; Van Campen, J.P.C.M.; Kuper, I.M.J.A.; Gijsen, G.J.P.T.; Koks, C.H.W.; Mac Gillavry, M.R.; van Tinteren, H.; Beijnen, J.H.; Brandjes, D.P.M. Reasons for Undertreatment with Oral Anticoagulants in Frail Geriatric Outpatients with Atrial Fibrillation. A Prospective, Descriptive Study. Drugs Aging 2010, 27, 39–50. [Google Scholar] [CrossRef]
- Proietti, M.; Romiti, G.F.; Raparelli, V.; Diemberger, I.; Boriani, G.; Vecchia, L.A.D.; Bellelli, G.; Marzetti, E.; Lip, G.Y.; Cesari, M. Frailty prevalence and impact on outcomes in patients with atrial fibrillation: A systematic review and meta-analysis of 1,187,000 patients. Ageing Res. Rev. 2022, 79, 101652. [Google Scholar] [CrossRef]
- Kojima, G.; Iliffe, S.; Walters, K. Frailty index as a predictor of mortality: A systematic review and meta-analysis. Age Ageing 2018, 47, 193–200. [Google Scholar] [CrossRef]
- Steffel, J.; Giugliano, R.P.; Braunwald, E.; Murphy, S.A.; Mercuri, M.; Choi, Y.; Aylward, P.; White, H.; Zamorano, J.L.; Antman, E.M.; et al. Edoxaban Versus Warfarin in Atrial Fibrillation Patients at Risk of Falling: ENGAGE AF-TIMI 48 Analysis. J. Am. Coll. Cardiol. 2016, 68, 1169–1178. [Google Scholar] [CrossRef]
- Wold, J.F.H.; Ruiter, J.H.; Cornel, J.H.; Vogels, R.L.C.; Jansen, R.W.W.M. A multidisciplinary care pathway for the evaluation of falls and syncope in geriatric paties. Eur. Geriatr. Med. 2015, 6, 7. [Google Scholar] [CrossRef]
- Searle, S.D.; Mitnitski, A.; Gahbauer, E.A.; Gill, T.M.; Rockwood, K. A standard procedure for creating a frailty index. BMC Geriatr. 2008, 8, 24. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation. N. Engl. J. Med. 2020, 383, 1305–1316. [Google Scholar]
- Oqap, Z.; Pournazari, P.; Sheldon, R.S. What is the Impact of Frailty on Prescription of Anticoagulation in Elderly Patients with Atrial Fibrillation?A Systematic Review and Meta-Analysis. J. Atr. Fibrillation 2018, 10, 1870. [Google Scholar] [CrossRef]
- Voorhout, L.; Pisters, R.; Geurts, C.H.P.H.; Oostindjer, A.; van Doorn, S.; Rila, H.; Fuijkschot, W.W.; Verheugt, F.; Hemels, M.E.W. Screening over 100,000 patients in 39 general practices in the Netherlands for anticoagulation underprescription in atrial fibrillation: A descriptive, cross-sectional study. BMJ Open 2023, 13, e072655. [Google Scholar] [CrossRef]
- Arbel, R.; Sergienko, R.; Hammerman, A.; Dotan-Greenberg, S.; Batat, E.; Avnery, O.; Greenberg, D.; Ellis, M.H. Direct oral anticoagulation and mortality in moderate to high-risk atrial fibrillation. Heart 2019, 105, 1487–1492. [Google Scholar] [CrossRef]
- Poli, D.; Antonucci, E.; Ageno, W.; Bertù, L.; Migliaccio, L.; Martinese, L.; Pilato, G.; Testa, S.; Palareti, G. Oral anticoagulation in very elderly patients with atrial fibrillation: Results from the prospective multicenter START2-REGISTER study. PLoS ONE 2019, 14, e0216831. [Google Scholar] [CrossRef]
- Chai-Adisaksopha, C.; Hillis, C.; Isayama, T.; Lim, W.; Iorio, A.; Crowther, M. Mortality outcomes in patients receiving direct oral anticoagulants: A systematic review and meta-analysis of randomized controlled trials. J. Thromb. Haemost. 2015, 13, 2012–2020. [Google Scholar] [CrossRef]
- Joosten, L.P.; van Doorn, S.; van de Ven, P.M.; Köhlen, B.T.; Nierman, M.C.; Koek, H.L.; Hemels, M.E.; Huisman, M.V.; Kruip, M.; Faber, L.M.; et al. Safety of Switching from a Vitamin K Antagonist to a Non-Vitamin K Antagonist Oral Anticoagulant in Frail Older Patients with Atrial Fibrillation: Results of the FRAIL-AF Randomized Controlled Trial. Circulation 2023. Preprint. [Google Scholar] [CrossRef]
- Steverink, N.; Slaets, J.; Schuurmans, H.; Van Lis, M. Measuring frailty: Developing and testing the GFI (Groningen Frailty Indicator). Gerontologist 2001, 41, 236e237. [Google Scholar]
- Pastori, D.; Miyazawa, K.; Lip, G.Y.H. Dementia and Atrial Fibrillation: A Dangerous Combination for Ischemic Stroke and Mortality. J. Alzheimers Dis. 2018, 61, 1129–1132. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| General Characteristics | Total n = 663 | No Antithrombotic Medication, n = 298 | Antiplatelet Agents, n = 221 | Oral Anticoagulation, n = 144 |
|---|---|---|---|---|
| Female, n (%) | 438 (66.1) | 213 (71.5) | 142 (64.3) | 83 (57.6) |
| Age in years, median (sd) | 80 (6.5) | 79 (6.7) | 81 (6.0) | 81 (6.5) |
| Number of drugs, median (sd) | 7 (3.8) | 5 (3.3) | 8 (3.3) | 8 (3.8) |
| Number of morbidities, median (sd) | 10 (5.2) | 8 (4.4) | 10 (5.2) | 12 (5.6) |
| Multiple falls per year, n (%) | 584 (88.3) | 263 (87.9) | 196 (88.7) | 125 (87.4) |
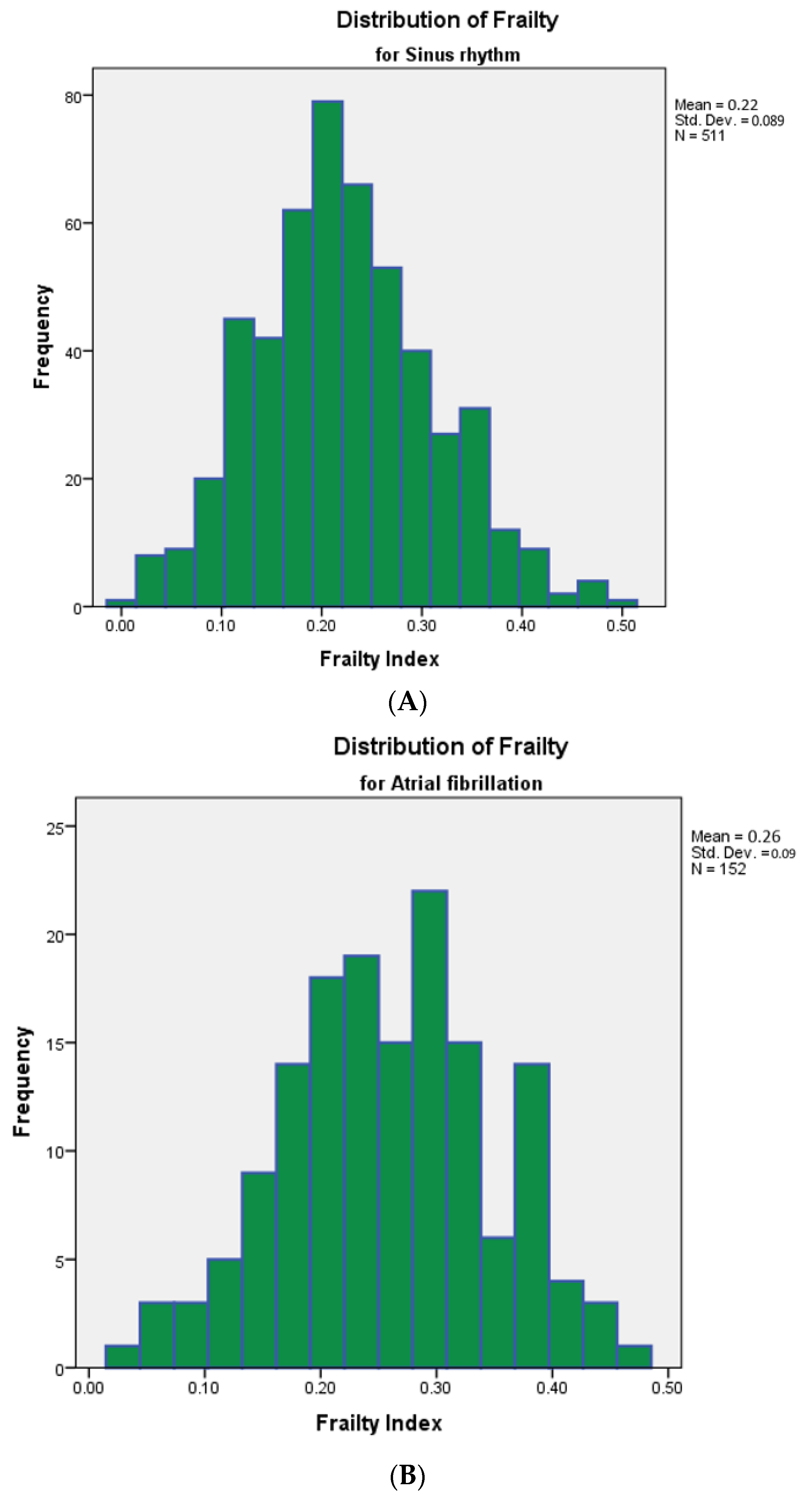
| Atrial fibrillation, n (%) | 152 (22.9) | 17 (5.7) | 17 (7.7) | 118 (81.9) |
| Hypertension, n (%) | 432 (65.2) | 163 (54.7) | 164 (74.2) | 105 (72.9) |
| Diabetes mellitus, n (%) | 150 (22.6) | 58 (19.5) | 53 (24.0) | 39 (27.1) |
| Creatinine clearance below 60 mL/min, n (%) | 139 (21.0) | 36 (12.1) | 55 (24.9) | 48 (33.3) |
| Heart failure, n (%) | 64 (9.7) | 7 (2.3) | 20 (9.0) | 37 (25.7) |
| Stroke in medical history, n (%) | 149 (22.5) | 13 (4.4) | 95 (43.0) | 41 (28.5) |
| Hypercholesterolemia, n (%) | 172 (25.9) | 49 (16.4) | 75 (33.9) | 48 (33.3) |
| Ischemic heart disease, n (%) | 160 (24.1) | 15 (5.0) | 94 (42.5) | 51 (35.4) |
| Geriatric features | ||||
| Frailty Index, mean (sd) | 0.23 (0.09) | 0.20 (0.08) | 0.26 (0.08) | 0.26 (0.09) |
| Moderately Frail, n (%) | 182 (27.5) | 83 (27.9) | 66 (29.9) | 33 (22.9) |
| Severe Frail, n (%) | 259 (39.1) | 73 (24.5) | 107 (48.4) | 79 (54.9) |
| Polypharmacy, n (%) | 484 (73.0) | 160 (53.7) | 196 (88.7) | 128 (88.9) |
| Orthostatic hypotension, n (%) | 195 (29.4) | 68 (22.8) | 79 (35.7) | 47 (32.6) |
| Post prandial hypotension, n (%) | 208 (31.4) | 91 (30.5) | 67 (30.3) | 50 (34.7) |
| Parkinsonism, n (%) | 63 (9.5) | 30 (10.1) | 22 (10.0) | 11 (7.6) |
| Gait disturbance, n (%) | 345 (52.0) | 153 (51.3) | 118 (53.4) | 74 (51.4) |
| ADL dependence, n (%) | 158 (23.8) | 59 (19.8) | 57 (25.8) | 42 (29.2) |
| iADL dependence, n (%) | 262 (39.5) | 103 (34.6) | 94 (42.5) | 65 (45.1) |
| Cognitive impairment | ||||
| MMSE < 26 points, n (%) | 177 (26.7) | 74 (24.8) | 57 (25.8) | 46 (31.9) |
| MoCA < 26 points, n (%) | 380 (57.3) | 172 (63.1) | 125 (56.6) | 83 (57.6) |
| Total, n = 196 (29.6%) | No Antithrombotics, n = 71 (23.8%) | Antiplatelet Agents, n = 67 (30.3%) | Oral Anticoagulation, n = 58 (40.3%) | |
|---|---|---|---|---|
| Infection, n (%) | 36 (18.4) | 8 (11.3) | 17 (25.4) | 11 (19.0) |
| Malignancy, n (%) | 21 (10.7) | 10 (14.1) | 8 (11.9) | 3 (5.2) |
| Cardiac, n (%) | 14 (7.1) | 3 (4.2) | 6 (9.0) | 5 (8.6) |
| Major bleeding, n (%) | 12 (6.1) | 8 (11.3) | 2 (3.0) | 2 (3.4) |
| Other, n (%) | 28 (14.3) | 8 (11.3) | 8 (11.9) | 12 (20.7) |
| Unknown, n (%) | 85 (43.4) | 34 (47.9) | 26 (38.8) | 25 (43.1) |
| General Characteristics | Hazard Ratio | 95% Confidence Interval | p |
|---|---|---|---|
| Female sex | 0.44 | 0.31–0.62 | <0.01 |
| Age, risk per year | 1.07 | 1.04–1.10 | <0.01 |
| Use of antithrombotic medication, as compared to no use | |||
| Antiplatelet agents | 1.55 | 1.04–2.31 | 0.03 |
| Oral anticoagulation | 2.14 | 1.38–3.32 | <0.01 |
| Number of prescription drugs | 1.06 | 1.01–1.10 | 0.02 |
| Number of morbidities | 1.07 | 1.03–1.10 | <0.01 |
| Multiple falls per year | 2.02 | 1.08–3.76 | 0.03 |
| Atrial fibrillation | 2.83 | 1.56–3.34 | <0.01 |
| Hypertension | 1.19 | 0.83–1.70 | 0.20 |
| Diabetes mellitus | 1.06 | 0.71–1.59 | 0.43 |
| Creatinine clearance 30–60 mL/min | 1.68 | 1.16–2.43 | <0.01 |
| Creatinine clearance 15–30 mL/min | 8.95 | 2.79–28.69 | <0.01 |
| Heart failure | 3.40 | 2.01–5.73 | <0.01 |
| History of stroke | 1.12 | 0.75–1.67 | 0.33 |
| Hypercholesterolemia | 1.18 | 0.81–1.73 | 0.23 |
| Ischemic heart disease | 1.98 | 1.36–2.88 | <0.01 |
| Geriatric features | |||
| Moderate Frailty | 2.47 | 1.50–4.05 | <0.01 |
| Severe Frailty | 3.94 | 2.50–6.20 | <0.01 |
| Polypharmacy | 1.15 | 0.78–1.70 | 0.27 |
| Orthostatic hypotension | 1.20 | 0.78–1.85 | 0.24 |
| Post prandial hypotension | 1.79 | 1.13–2.83 | 0.01 |
| Parkinsonism | 2.83 | 1.67–4.79 | <0.01 |
| Gait disturbance | 1.54 | 1.09–2.18 | 0.01 |
| ADL dependence | 2.63 | 1.80–3.83 | <0.01 |
| iADL dependence | 2.19 | 1.55–3.09 | <0.01 |
| Cognitive impairment | |||
| MMSE < 26 points | 1.66 | 1.14–2.40 | 0.01 |
| MoCA < 26 points | 1.41 | 0.94–2.12 | 0.06 |
| Hazard Ratio | 95% Confidence Interval | p | |
|---|---|---|---|
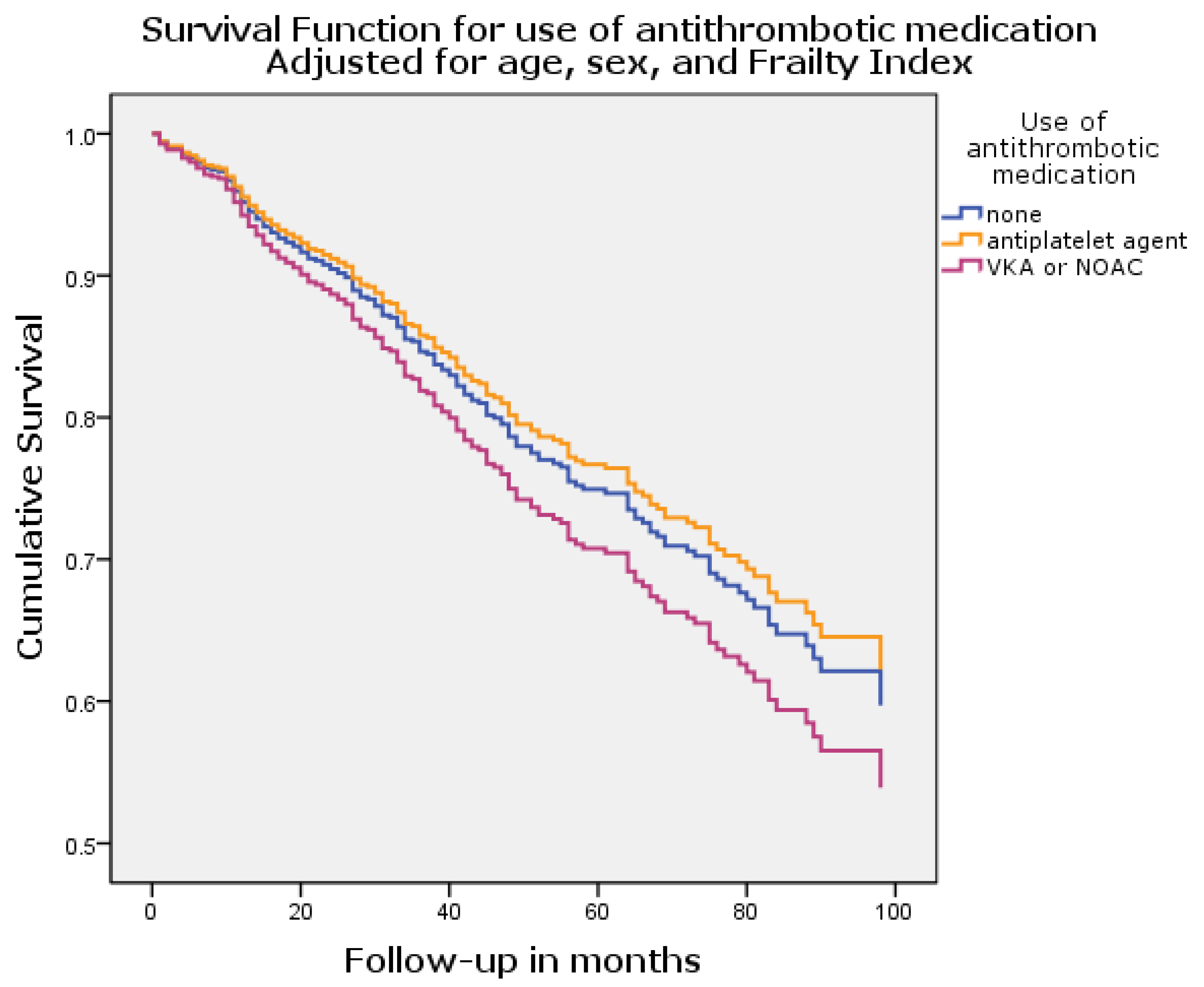
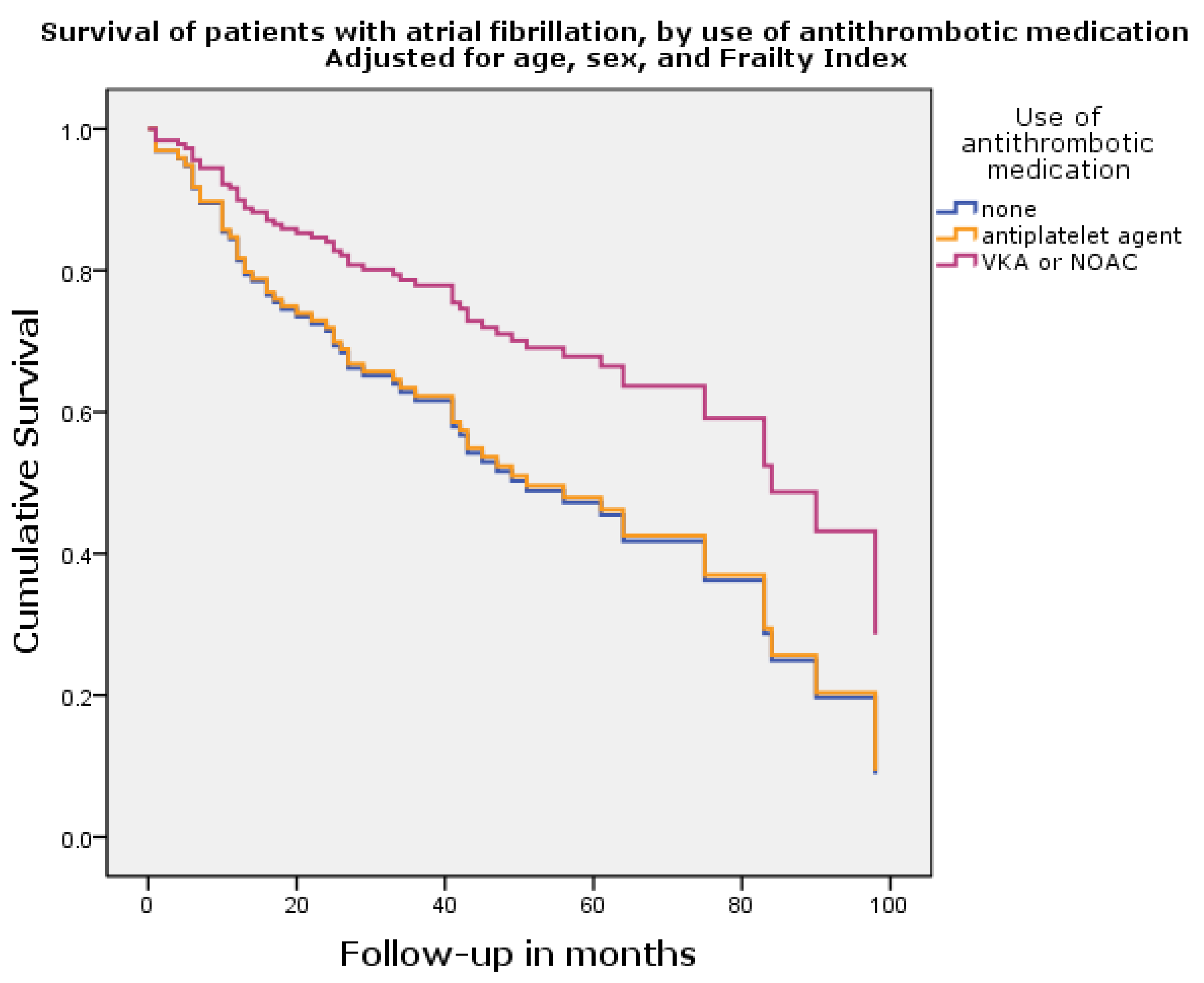
| Use of antithrombotic medication, as compared to no use | |||
| Antiplatelet agents | 0.89 | 0.62–1.29 | 0.54 |
| Oral anticoagulation | 1.22 | 0.83–1.80 | 0.31 |
| Female sex | 0.46 | 0.34–0.62 | <0.01 |
| Age, risk per year | 1.05 | 1.03–1.08 | <0.01 |
| Frailty Index | 74.0 | 13.1–417.3 | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zwart, L.A.R.; Walgers, J.J.; Hemels, M.E.W.; Germans, T.; de Groot, J.R.; Jansen, R.W.M.M. The Use of Oral Anticoagulation Is Not Independently Associated with Mortality in Frail Older Patients with Repeated Falls. J. Clin. Med. 2023, 12, 7388. https://doi.org/10.3390/jcm12237388
Zwart LAR, Walgers JJ, Hemels MEW, Germans T, de Groot JR, Jansen RWMM. The Use of Oral Anticoagulation Is Not Independently Associated with Mortality in Frail Older Patients with Repeated Falls. Journal of Clinical Medicine. 2023; 12(23):7388. https://doi.org/10.3390/jcm12237388
Chicago/Turabian StyleZwart, Lennaert A. R., Jeske J. Walgers, Martin E. W. Hemels, Tjeerd Germans, Joris R. de Groot, and René W. M. M. Jansen. 2023. "The Use of Oral Anticoagulation Is Not Independently Associated with Mortality in Frail Older Patients with Repeated Falls" Journal of Clinical Medicine 12, no. 23: 7388. https://doi.org/10.3390/jcm12237388