

“It’s Like Listening to the Radio with a Little Interference”: A Qualitative Study Describing Pain Management among Patients with Psoriatic Arthritis

Abstract
:1. Introduction
2. Materials and Methods
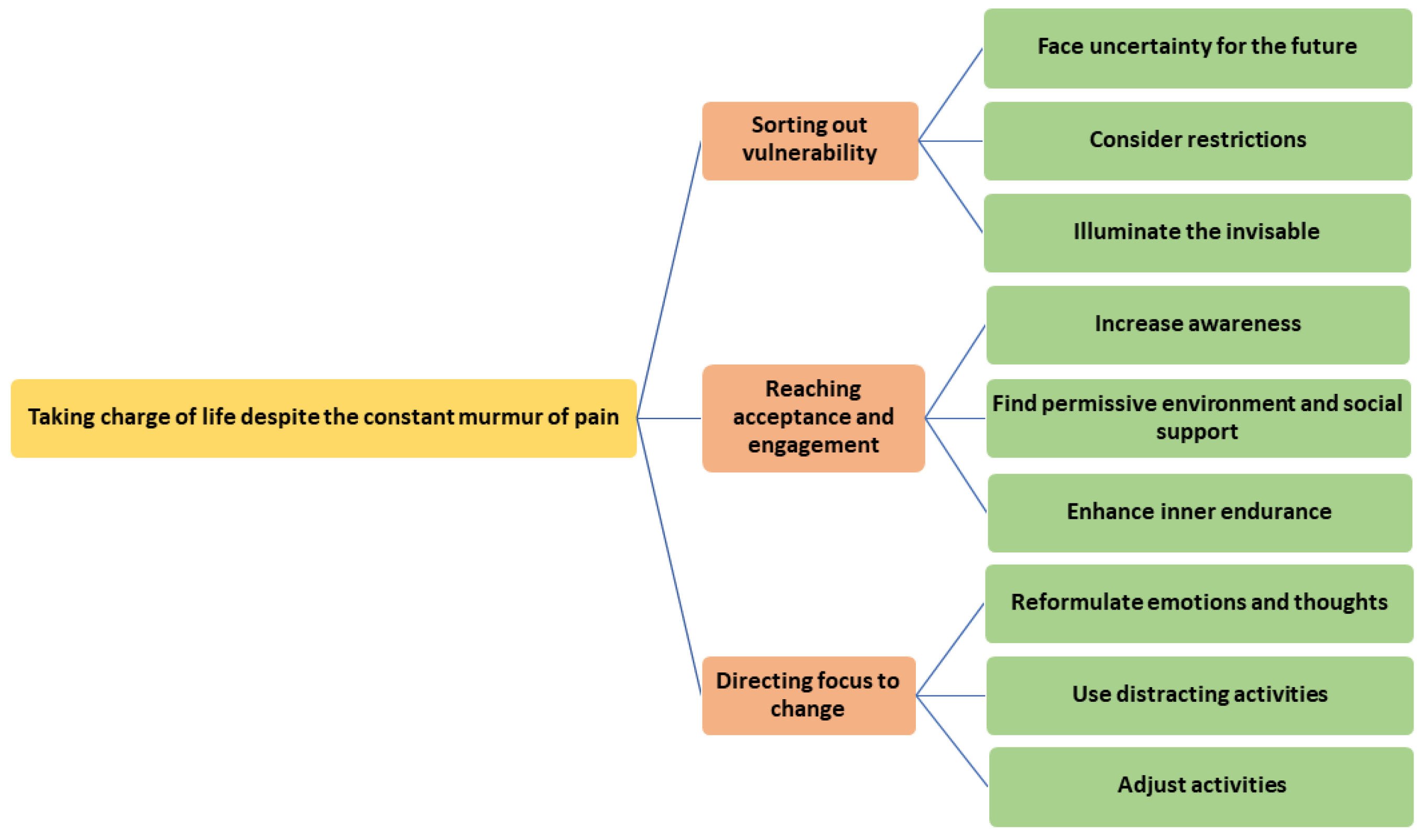
3. Results
3.1. Sorting out Vulnerability
3.1.1. Facing Uncertainty about the Future
3.1.2. Considering Restrictions
3.1.3. Illuminating the Invisible
3.2. Reaching Acceptance and Engagement
3.2.1. Increasing Awareness
3.2.2. Finding a Permissive Environment and Social Support
3.2.3. Enhancing Inner Endurance
3.3. Directing One’s Focus toward Change
3.3.1. Reformulating Emotions and Thoughts
3.3.2. Use of Distracting Activities
3.3.3. Adjusted Activities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gladman, D.D.; Antoni, C.; Mease, P.; Clegg, D.O.; Nash, P. Psoriatic arthritis: Epidemiology, clinical features, course, and outcome. Rheumatology 2005, 64, ii14–ii17. [Google Scholar] [CrossRef]
- Husni, M.E.; Merola, J.F.; Davin, S. The psychosocial burden of psoriatic arthritis. Semin. Arthritis Rheum. 2017, 47, 351–360. [Google Scholar] [CrossRef]
- Tezel, N.; Tasdelen, O.Y.; Bodur, H.; Gul, U.; Cakmak, S.K.; Oguz, I.D.; Karabulut, E. Is the health-related quality of life and functional status of patients with psoriatic arthritis worse than that of patients with psoriasis alone? Int. J. Rheum. Dis. 2014, 18, 63–69. [Google Scholar] [CrossRef]
- Dalal, D.S.; Lin, Y.C.; Brennan, D.M.; Borkar, N.; Korman, N.; Husni, M.E. Quantifying harmful effects of psoriatic diseases on quality of life: Cardio-metabolic outcomes in psoriatic arthritis study (COMPASS). Semin. Arthritis Rheum. 2015, 44, 641–645. [Google Scholar] [CrossRef]
- Edson-Heredia, E.; Zhu, B.; Guo, J.; Maeda-Chubachi, T.; Lebwohl, M. Disease burden and quality of life in psoriasis patients with and without comorbid psoriatic arthritis: Results from National Psoriasis Foundation panel surveys. Cutis 2015, 95, 173–178. [Google Scholar]
- Puig, L.; Strohal, R.; Husni, M.E.; Tsai, T.-F.; Noppakun, N.; Szumski, A.; Yang, S.; Robertson, D.; Boggs, R.; Koenig, A.S. Cardiometabolic profile, clinical features, quality of life and treatment outcomes in patients with moderate-to-severe psoriasis and psoriatic arthritis. J. Dermatol. Treat. 2015, 26, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Rich-Garg, N.; Truong, B.; Ehst, B.; Deodhar, A.; Ku, J.; Vakil-Gilani, K.; Danve, A.; Blauvelt, A. Demographics, clinical disease characteristics, and quality of life in a large cohort of psoriasis patients with and without psoriatic arthritis. Clin. Cosmet. Investig. Dermatol. 2015, 8, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Sumpton, D.; Kelly, A.; Tunnicliffe, D.J.; Craig, J.C.; Hassett, G.; Chessman, D.; Tong, A. Patients’ Perspectives and Experience of Psoriasis and Psoriatic Arthritis: A Systematic Review and Thematic Synthesis of Qualitative Studies. Arthritis Care Res. 2020, 72, 711–722. [Google Scholar] [CrossRef] [PubMed]
- Kavanaugh, A.; Helliwell, P.; Ritchlin, C.T. Psoriatic Arthritis and Burden of Disease: Patient Perspectives from the Population-Based Multinational Assessment of Psoriasis and Psoriatic Arthritis (MAPP) Survey. Rheumatol. Ther. 2016, 3, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Rifbjerg-Madsen, S.; Christensen, A.W.; Christensen, R.; Hetland, M.L.; Bliddal, H.; Kristensen, L.E.; Danneskiold-Samsøe, B.; Amris, K. Pain and pain mechanisms in patients with inflammatory arthritis: A Danish nationwide cross-sectional DANBIO registry survey. PLoS ONE 2017, 12, e0180014. [Google Scholar] [CrossRef] [PubMed]
- Orbai, A.-M.; de Wit, M.; Mease, P.; A Shea, J.; Gossec, L.; Leung, Y.Y.; Tillett, W.; Elmamoun, M.; Duffin, K.C.; Campbell, W.; et al. International patient and physician consensus on a psoriatic arthritis core outcome set for clinical trials. Rheumatology 2017, 76, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Pariser, D.; Schenkel, B.; Carter, C.; Farahi, K.; Brown, T.M.; Ellis, C.N.; For the Psoriasis Patient Interview Study Group. A multicenter, non-interventional study to evaluate patient-reported experiences of living with psoriasis. J. Dermatol. Treat. 2016, 27, 19–26. [Google Scholar] [CrossRef]
- Garrido-Cumbrera, M.; Hillmann, O.; Mahapatra, R.; Trigos, D.; Zajc, P.; Weiss, L.; Bostynets, G.; Gossec, L.; Coates, L.C. Improving the Management of Psoriatic Arthritis and Axial Spondyloarthritis: Roundtable Discussions with Healthcare Professionals and Patients. Rheumatol. Ther. 2017, 4, 219–231. [Google Scholar] [CrossRef]
- Dures, E.; For the PROMPT Study Group; Hewlett, S.; Lord, J.; Bowen, C.; McHugh, N.; Tillett, W. Important Treatment Outcomes for Patients with Psoriatic Arthritis: A Multisite Qualitative Study. Patient 2017, 10, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Geenen, R.; Overman, C.L.; Christensen, R.; Åsenlöf, P.; Capela, S.; Huisinga, K.L.; Husebø, M.E.P.; A Köke, A.J.; Paskins, Z.; A Pitsillidou, I.; et al. EULAR recommendations for the health professional’s approach to pain management in inflammatory arthritis and osteoarthritis. Rheumatology 2018, 77, 797–807. [Google Scholar] [CrossRef] [PubMed]
- Stålnacke, B.-M.; Bäckryd, E.; Roeck Hansen, E.; Novo, M.; Gerdle, B. Nationella registret över smärtrehabilitering, Smärtanalys och diagnossättning vid kroniska smärtor inom specialiserad smärtavård. Rapport 2014, 3. [Google Scholar]
- Craig, K.D.; MacKenzie, N.E. What is pain: Are cognitive and social features core components? Paediatr. Neonatal Pain 2021, 3, 106–118. [Google Scholar] [CrossRef]
- Evers, A.W.; Kraaimaat, F.W.; Geenen, R.; Jacobs, J.W.; Bijlsma, J.W. Pain coping and social support as predictors of long-term functional disability and pain in early rheumatoid arthritis. Behav. Res. Ther. 2003, 41, 1295–1310. [Google Scholar] [CrossRef]
- Spink, A.; Wagner, I.; Orrock, P. Common reported barriers and facilitators for self-management in adults with chronic musculoskeletal pain: A systematic review of qualitative studies. Musculoskelet. Sci. Pr. 2021, 56, 102433. [Google Scholar] [CrossRef]
- Devan, H.; Hale, L.; Hempel, D.; Saipe, B.; Perry, M.A. What Works and Does Not Work in a Self-Management Intervention for People with Chronic Pain? Qualitative Systematic Review and Meta-Synthesis. Phys. Ther. 2018, 98, 381–397. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The “What” and “Why” of Goal Pursuits: Human Needs and the Self-Determination of Behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Lindgren, B.-M.; Lundman, B.; Graneheim, U.H. Abstraction and interpretation during the qualitative content analysis process. Int. J. Nurs. Stud. 2020, 108, 103632. [Google Scholar] [CrossRef]
- Crowe, M.; Whitehead, L.; Seaton, P.; Jordan, J.; Mccall, C.; Maskill, V.; Trip, H. Qualitative meta-synthesis: The experience of chronic pain across conditions. J. Adv. Nurs. 2017, 73, 1004–1016. [Google Scholar] [CrossRef]
- Dures, E.; Bowen, C.; Brooke, M.; Lord, J.; Tillett, W.; McHugh, N.; Hewlett, S. Diagnosis and initial management in psoriatic arthritis: A qualitative study with patients. Rheumatol. Adv. Pr. 2019, 3, rkz022. [Google Scholar] [CrossRef]
- Ogdie, A.; Michaud, K.; Nowak, M.; Bruce, R.; Cantor, S.; Hintzen, C.; Mease, P.J. Patient’s experience of psoriatic arthritis: A conceptual model based on qualitative interviews. RMD Open 2020, 6, e001321. [Google Scholar] [CrossRef] [PubMed]
- Moverley, A.R.; Vinall-Collier, K.A.; Helliwell, P.S. It’s not just the joints, it’s the whole thing: Qualitative analysis of patients’ experience of flare in psoriatic arthritis. Rheumatology 2015, 54, 1448–1453. [Google Scholar] [CrossRef]
- Bergström, M.; Ahlstrand, I.; Thyberg, I.; Falkmer, T.; Börsbo, B.; Björk, M. ‘Like the worst toothache you’ve had’—How people with rheumatoid arthritis describe and manage pain. Scand. J. Occup. Ther. 2017, 24, 468–476. [Google Scholar] [CrossRef]
- Murray, A.; Hall, A.M.; Williams, G.C.; McDonough, S.M.; Ntoumanis, N.; Taylor, I.M.; Jackson, B.; Matthews, J.; Hurley, D.A.; Lonsdale, C. Effect of a Self-Determination Theory–Based Communication Skills Training Program on Physiotherapists’ Psychological Support for Their Patients with Chronic Low Back Pain: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2015, 96, 809–816. [Google Scholar] [CrossRef]
- Arnott, R.; Park, V.; Rhind, N.; Cooper, K. Exploring the experiences and perceptions of participating in a peer-support intervention for adults with chronic non-cancer pain: A qualitative systematic review. JBI Évid. Synth. 2023, 21, 1509–1548. [Google Scholar] [CrossRef]
- Uysal, A.; Ascigil, E.; Turunc, G. Spousal autonomy support, need satisfaction, and well-being in individuals with chronic pain: A longitudinal study. J. Behav. Med. 2017, 40, 281–292. [Google Scholar] [CrossRef]
- Kindt, S.; Vansteenkiste, M.; Loeys, T.; Goubert, L. Helping motivation and well-being of chronic pain couples: A daily diary study. Pain 2016, 157, 1551–1562. [Google Scholar] [CrossRef]
- Kvale, S. InterViews: Learning the Craft of Qualitative Research Interviewing, 2nd ed.; Sage Publications: Los Angeles, CA, USA, 2009. [Google Scholar]
- Malterud, K. Qualitative research: Standards, challenges, and guidelines. Lancet 2001, 358, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W. Qualitative Inquiry and Research Design: Choosing among Five Approaches, 3rd ed.; Sage Publications: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Thomas, D.R. Feedback from research participants: Are member checks useful in qualitative research? Qual. Res. Psychol. 2017, 14, 23–41. [Google Scholar] [CrossRef]
- Staller, K.M. Big enough? Sampling in qualitative inquiry. Qual. Soc. Work. 2021, 20, 897–904. [Google Scholar] [CrossRef]
- Sebele-Mpofu, F.Y. Saturation controversy in qualitative research: Complexities and underlying assumptions. A literature review. Cogent Soc. Sci. 2020, 6, 1838706. [Google Scholar] [CrossRef]
- Gialouri, C.G.; Fragoulis, G.E. Disease activity indices in psoriatic arthritis: Current and evolving concepts. Clin. Rheumatol. 2021, 40, 4427–4435. [Google Scholar] [CrossRef] [PubMed]
- Gossec, L.; Walsh, J.A.; Michaud, K.; Holdsworth, E.; Peterson, S.; Meakin, S.; Yang, F.; Booth, N.; Chakravarty, S.D.; Piercy, J.; et al. Effect of Fatigue on Health-Related Quality of Life and Work Productivity in Psoriatic Arthritis: Findings from a Real-World Survey. J. Rheumatol. 2022, 49, 1221–1228. [Google Scholar] [CrossRef] [PubMed]
- Conaghan, P.G.; Alten, R.; Deodhar, A.; Sullivan, E.; Blackburn, S.; Tian, H.; Gandhi, K.; Jugl, S.M.; Strand, V. Relationship of pain and fatigue with health-related quality of life and work in patients with psoriatic arthritis on TNFi: Results of a multi-national real-world study. RMD Open 2020, 6, e001240. [Google Scholar] [CrossRef] [PubMed]
- Osborne, N.R.; Davis, K.D. Chapter Eight-Sex and gender differences in pain. In International Review of Neurobiology; Moro, E., Arabia, G., Tartaglia, M.C., Ferretti, M.T., Eds.; Academic Press: Cambridge, MA, USA, 2022; Volume 164, pp. 277–307. [Google Scholar] [CrossRef]
- Stlund, G.; Björk, M.; Thyberg, I.; Valtersson, E.; Sverker, A. Women’s situation-specific strategies in managing participation re-strictions due to early rheumatoid arthritis: A gender comparison. Musculoskelet. Care 2018, 16, 251–259. [Google Scholar] [CrossRef]


{kind=link}
| Main Areas of Inquiry |
|---|
| Times in life when pain has been highly present (challenging to manage, easy to manage) |
| Thoughts about reasons for pain |
| Factors affecting pain (personal, behavioral, social, environmental, and psychological factors) |
| How pain is managed |
| Expectations of the future in relation to pain |
| Demographic and Health-Related Data | |
|---|---|
| Gender, female/male (n) | 8/3 |
| Age, years, md (range) | 52 (40–67) |
| Disease duration, years, md (range) | 4 (1–24) |
| Level of education, n | |
| High school | 6 |
| University | 5 |
| Occupational status, n | |
| Full-time work | 8 |
| Part-time work | 3 |
| Married/partner, n | 10 |
| Children at home, n | 4 |
| Pain, VAS 1 mm, md (range) | 40 (20–70) |
| Fatigue, VAS 2 mm, md (range) | 60 (0–90) |
| General health, VAS 3 mm, md (range) | 70 (30–90) |
| Activity limitations, | |
| HAQ-DI 4, md (range), n = 9 | 0.875 (0–1.5) |
| BASFI 5, n = 1 | 2.7 |
| Steps of Analysis | Authors Involved |
|---|---|
| To familiarize themselves with and obtain an overview of the material, all the transcribed individual interviews were first read carefully by one of the authors | E.S. |
| Open coding was performed with all the material through writing notes and headings describing approaches to pain in the text while reading it. Parts of the interviews connected to the headings were also identified. The material was read through several times while headings and related parts were identified. The headings were then moved/collected from the margins into a coding mind map. The first step of the open coding (writing notes and headings) was also performed with four of the interviews by a second author. | E.S., N.B. |
| The various codes were compared regarding differences and similarities. Codes with related meanings were grouped together in categories in the mind map. To ensure trustworthiness, two of the authors repeatedly discussed and compared the emerging categories with the content of the original interviews, until a negotiated consensus was reached. | E.S., N.B. |
| The last step of the analysis, identifying a meaningful underlying essence that runs through the material, resulted in an overarching theme of meaning and descriptive subthemes. Discussions with the author who acted as a peer expert, to compare the emerging categories and themes, were held during the final phase of the analytic procedure until a negotiated consensus was reached. | E.S., N.B., M.B. |
| Quotes are provided in the results for illustration and trustworthiness. | Supplementary File S1. |
| Management of Pain in PsA | Needs Satisfaction + or Frustration − | ||
|---|---|---|---|
| Category in the Present Study’s Results (Action Component) | Competence | Autonomy | Relatedness |
| Face uncertainty for the future | − | ||
| Consider restrictions | − | − | − |
| Illuminate the invisible | − | − | |
| Increase awareness | + | ||
| Find a permissive environment and social support | + | ± | |
| Enhance inner endurance | + | + | |
| Reformulate emotions and thoughts | + | ± | |
| Use distracting activities | + | + | |
| Adjusted activities | + | + |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brodin, N.; Sundström, B.; Björk, M.; Swärdh, E. “It’s Like Listening to the Radio with a Little Interference”: A Qualitative Study Describing Pain Management among Patients with Psoriatic Arthritis. J. Clin. Med. 2023, 12, 7348. https://doi.org/10.3390/jcm12237348
Brodin N, Sundström B, Björk M, Swärdh E. “It’s Like Listening to the Radio with a Little Interference”: A Qualitative Study Describing Pain Management among Patients with Psoriatic Arthritis. Journal of Clinical Medicine. 2023; 12(23):7348. https://doi.org/10.3390/jcm12237348
Chicago/Turabian StyleBrodin, Nina, Björn Sundström, Mathilda Björk, and Emma Swärdh. 2023. "“It’s Like Listening to the Radio with a Little Interference”: A Qualitative Study Describing Pain Management among Patients with Psoriatic Arthritis" Journal of Clinical Medicine 12, no. 23: 7348. https://doi.org/10.3390/jcm12237348