
MRI Assessment of Cesarean Scar Pregnancies: A Case Series
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
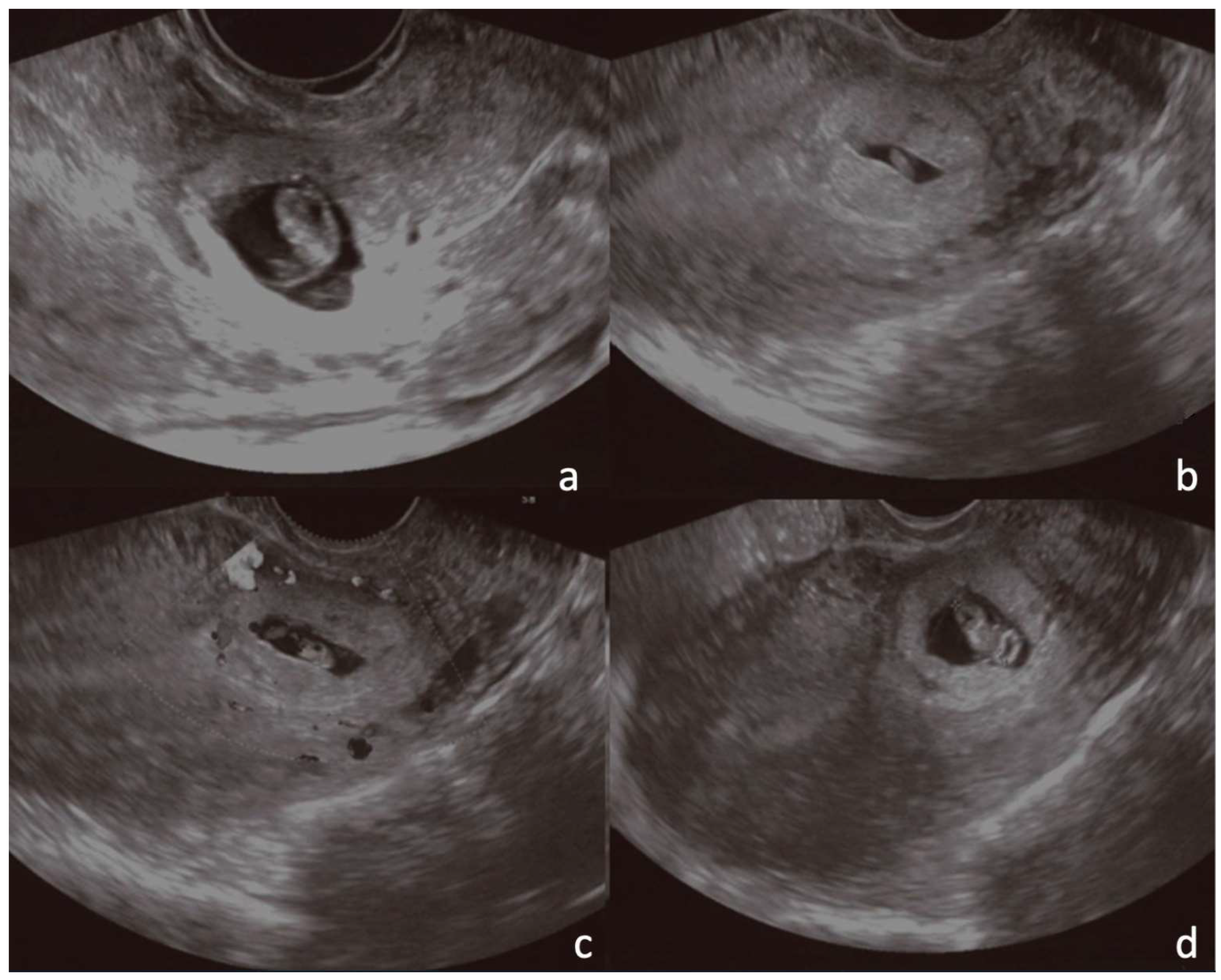
2.2. Transvaginal Ultrasonography
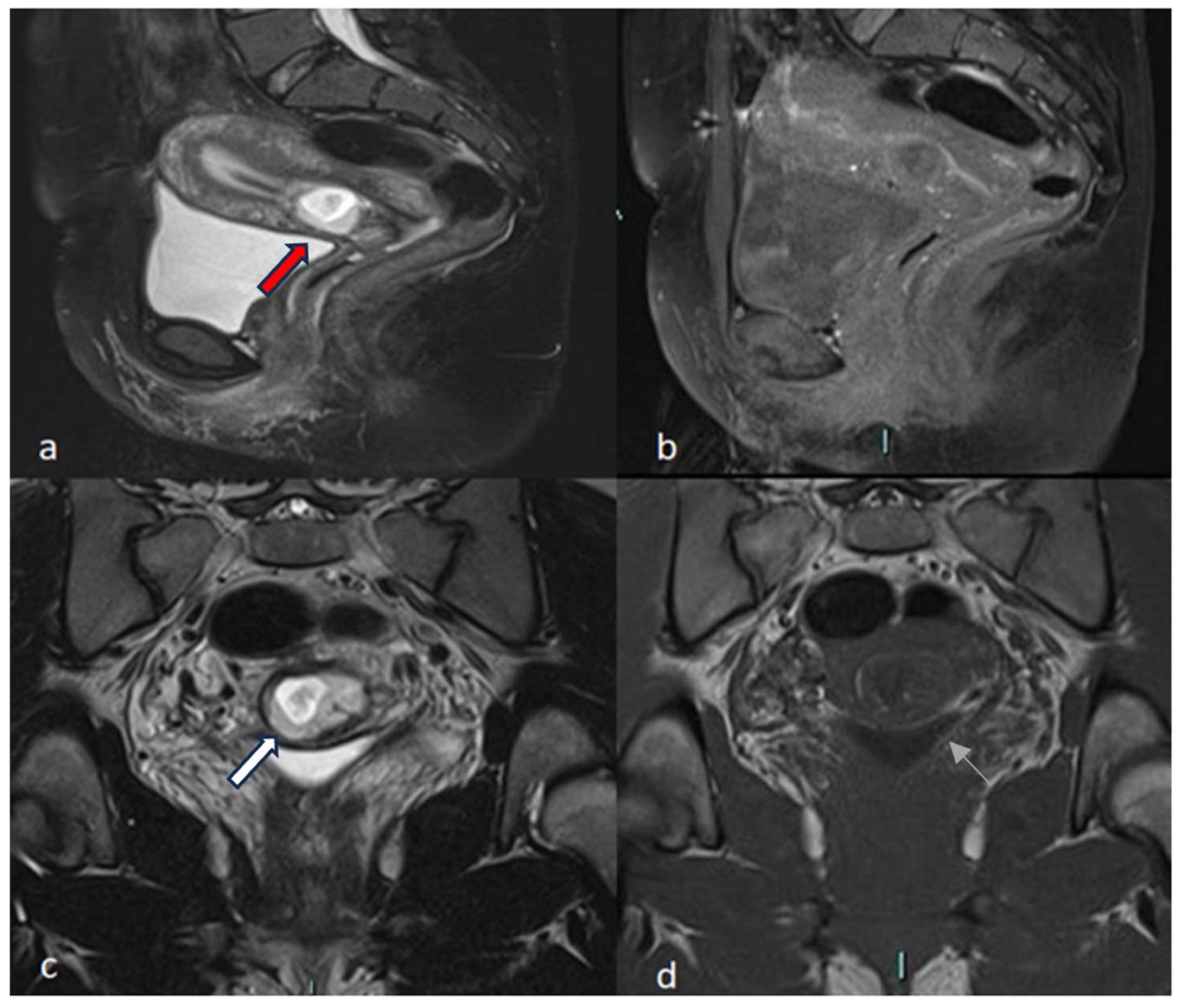
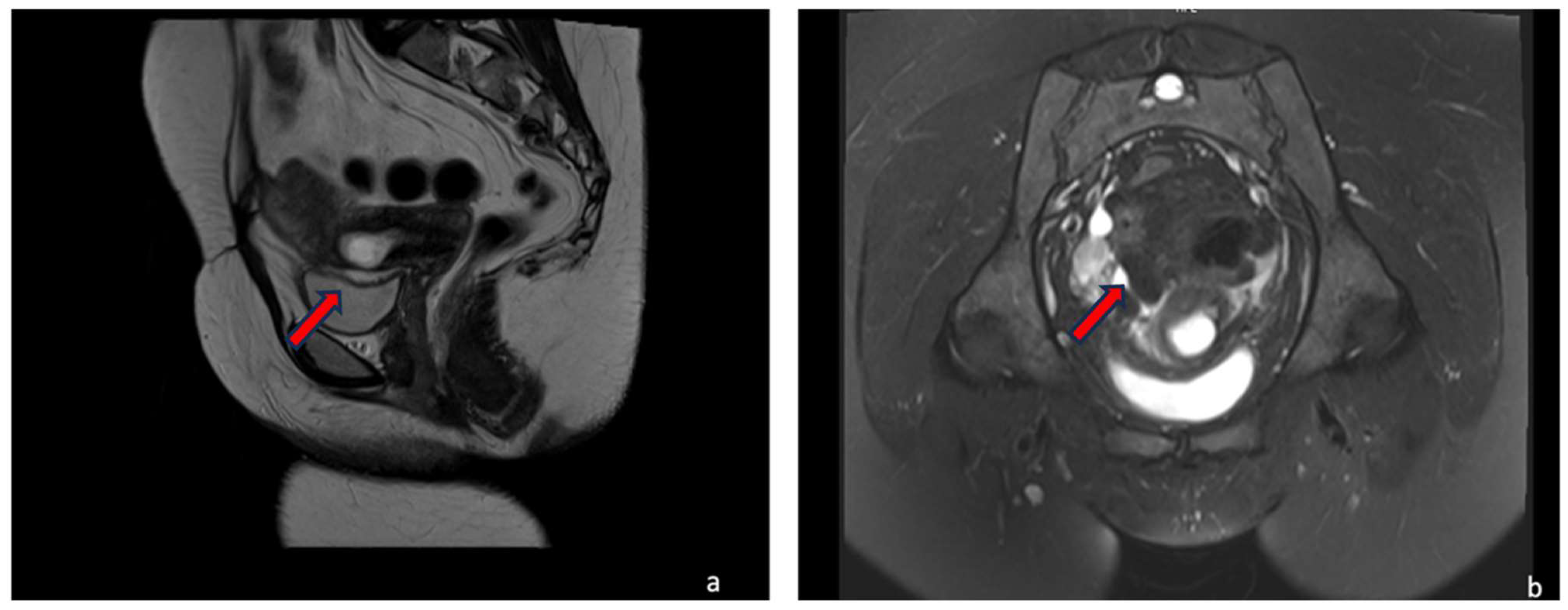
2.3. MRI
3. Results
4. Cases Presentation
4.1. Typical Cases
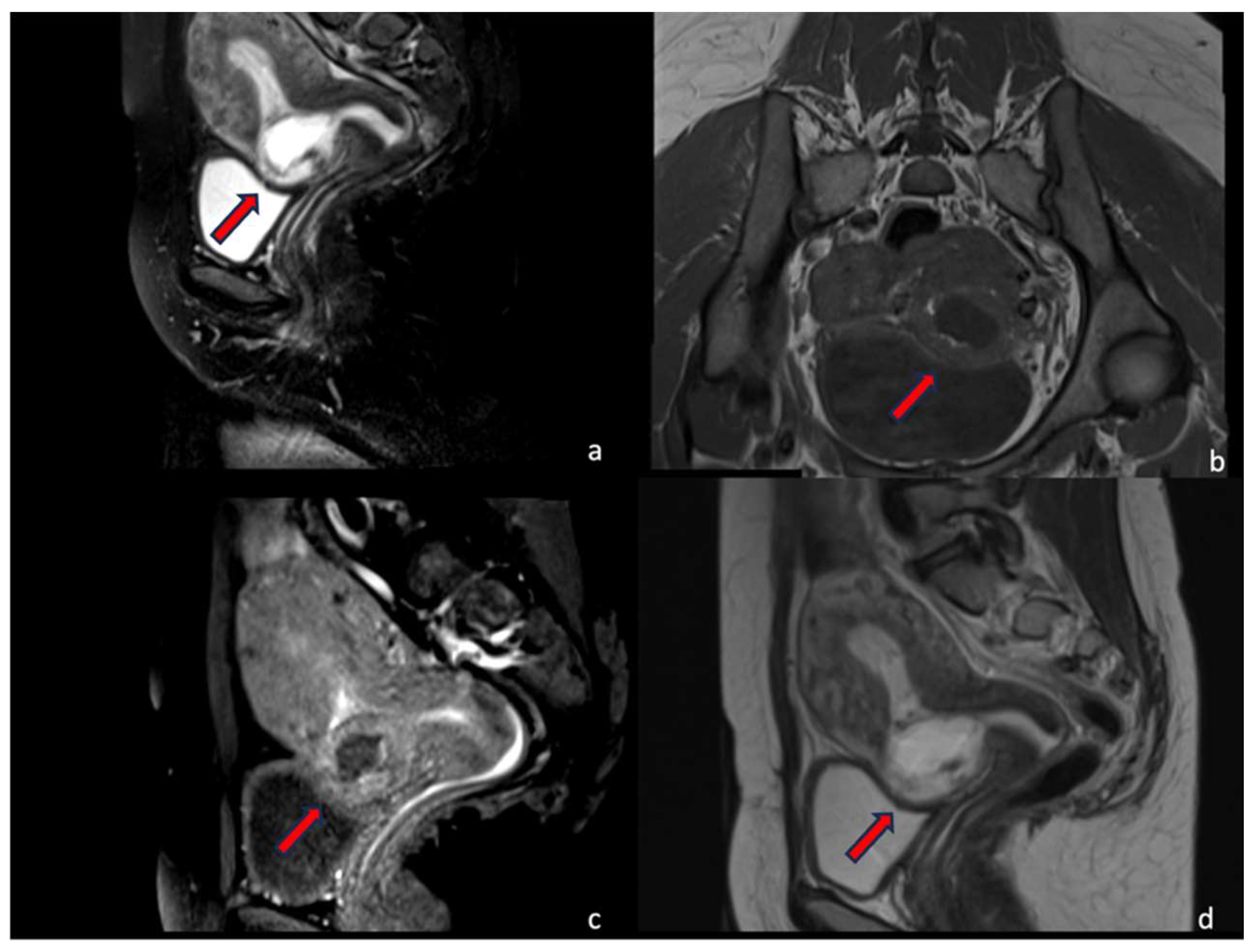
4.1.1. Case 1 (CSP Type I)
4.1.2. Case 2 (CSP Type II)
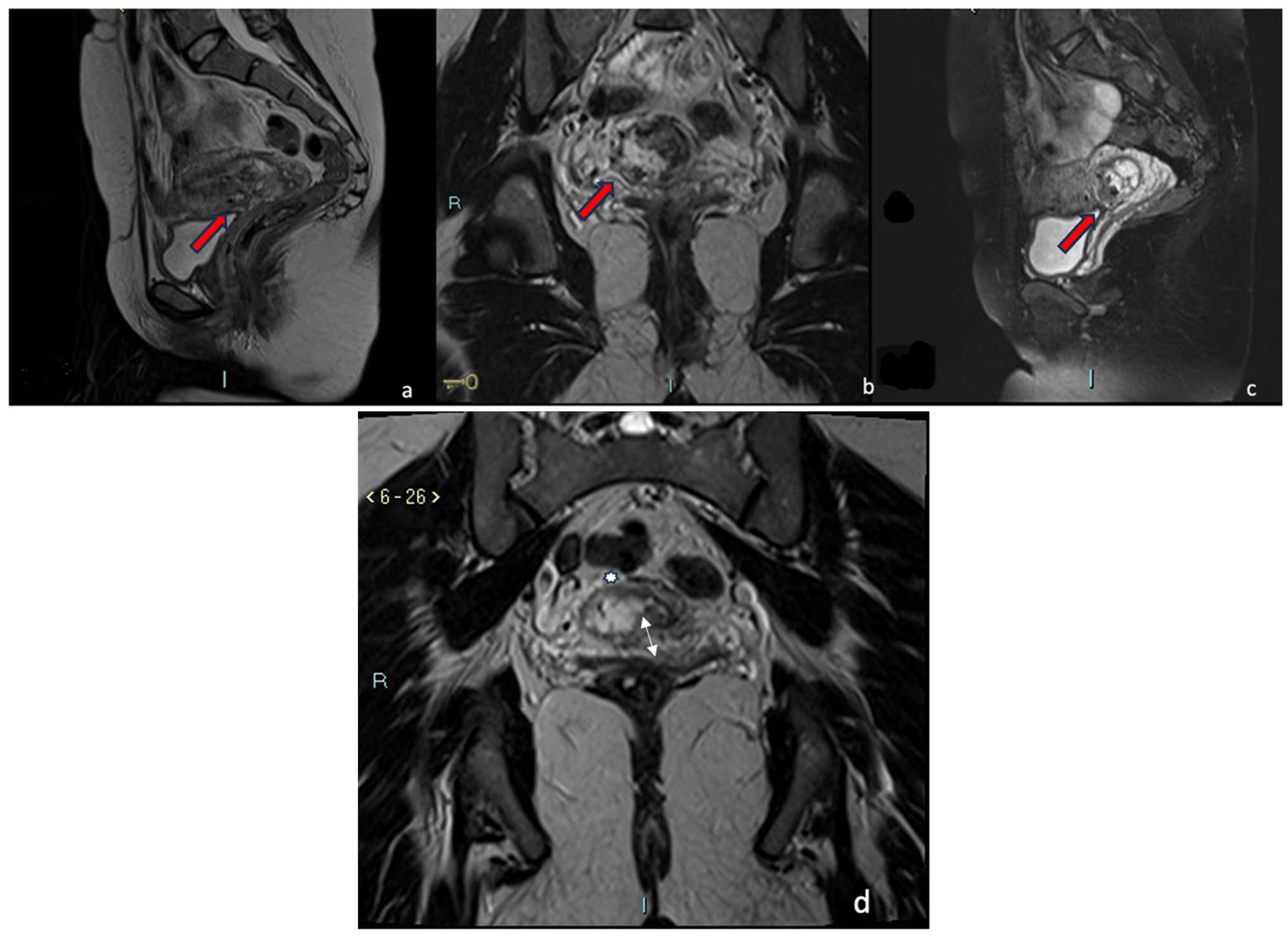
4.1.3. Case 3 (Low-Implanted Pregnancy)
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gonzalez, N.; Tulandi, T. Cesarean Scar Pregnancy: A Systematic Review. J. Minim. Invasive Gynecol. 2017, 24, 731–738. [Google Scholar] [CrossRef]
- Wong, W.S.F.; Fung, W.T. Magnetic Resonance Imaging in the Evaluation of Cesarean Scar Defect. Gynecol. Minim. Invasive Ther. 2018, 7, 104–107. [Google Scholar] [CrossRef]
- Timor-Tritsch, I.E.; Monteagudo, A.; Cali, G.; D’Antonio, F.; Kaelin Agten, A. Cesarean Scar Pregnancy: Diagnosis and Pathogenesis. Obstet. Gynecol. Clin. N. Am. 2019, 46, 797–811. [Google Scholar] [CrossRef]
- Selvaraj, N.; Thangarasu, M.; Prakash, S.; Raghavan, D.; Khakhar, A. Acquired post cesarean uretero-uterine fistula—A rare entity. Urol. Case Rep. 2020, 33, 101314. [Google Scholar] [CrossRef]
- Wang, K.; Jing, F. Comparison of Diagnostic Efficacy among Transvaginal Sonography, Transabdominal Sonography, and 3.0 T Magnetic Resonance Imaging in Early Cesarean Scar Pregnancy. J. Healthc. Eng. 2022, 2022, 9714369. [Google Scholar] [CrossRef]
- Stupak, A.; Kondracka, A.; Fronczek, A.; Kwasniewska, A. Scar Tissue after a Cesarean Section-The Management of Different Complications in Pregnant Women. Int. J. Environ. Res. Public. Health 2021, 18, 11998. [Google Scholar] [CrossRef]
- Timor-Tritsch, I.E.; Monteagudo, A.; Cali, G.; Vintzileos, A.; Viscarello, R.; Al-Khan, A.; Zamudio, S.; Mayberry, P.; Cordoba, M.M.; Dar, P. Cesarean scar pregnancy is a precursor of morbidly adherent placenta. Ultrasound Obstet. Gynecol. 2014, 44, 346–353. [Google Scholar] [CrossRef]
- Timor-Tritsch, I.E.; Monteagudo, A.; Cali, G.; Palacios-Jaraquemada, J.M.; Maymon, R.; Arslan, A.A.; Patil, N.; Popiolek, D.; Mittal, K.R. Cesarean scar pregnancy and early placenta accreta share common histology. Ultrasound Obstet. Gynecol. 2014, 43, 383–395. [Google Scholar] [CrossRef]
- Jordans, I.P.M.; Verberkt, C.; De Leeuw, R.A.; Bilardo, C.M.; Van Den Bosch, T.; Bourne, T.; Brolmann, H.A.M.; Dueholm, M.; Hehenkamp, W.J.K.; Jastrow, N.; et al. Definition and sonographic reporting system for Cesarean scar pregnancy in early gestation: Modified Delphi method. Ultrasound Obstet. Gynecol. 2022, 59, 437–449. [Google Scholar] [CrossRef]
- Liu, D.; Gu, X.; Liu, F.; Shi, F.; Yang, M. Contrast-enhanced ultrasound in uterine artery embolization treatment of cesarean scar pregnancy. J. Int. Med. Res. 2020, 48, 300060520980217. [Google Scholar] [CrossRef]
- McLaren, R.; McCalla, S.; Irani, M. Conservative Management of Cesarean Scar Ectopic Pregnancy with Fetal Heart Activity and a Very High beta-hCG. Case Rep. Obstet. Gynecol. 2015, 2015, 959876. [Google Scholar] [PubMed]
- Huang, J.; Phillips, C.; Moshiri, M. Scarred for life: A review of cesarean section scar pregnancy and potential pitfalls in diagnosis. Abdom. Radiol. 2023, 48, 2672–2683. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Klein, M.A.; Mahboob, S.; Gupta, M.; Katz, D.S. Magnetic resonance imaging as an adjunct to ultrasound in evaluating cesarean scar ectopic pregnancy. J. Clin. Imaging Sci. 2013, 3, 16. [Google Scholar] [CrossRef] [PubMed]
- Birch Petersen, K.; Hoffmann, E.; Rifbjerg Larsen, C.; Svarre Nielsen, H. Cesarean scar pregnancy: A systematic review of treatment studies. Fertil. Steril. 2016, 105, 958–967. [Google Scholar] [CrossRef]
- Vial, Y.; Petignat, P.; Hohlfeld, P. Pregnancy in a cesarean scar. Ultrasound Obstet. Gynecol. 2000, 16, 592–593. [Google Scholar] [CrossRef]
- Timor-Tritsch, I.E.; Monteagudo, A.; Santos, R.; Tsymbal, T.; Pineda, G.; Arslan, A.A. The diagnosis, treatment, and follow-up of cesarean scar pregnancy. Am. J. Obstet. Gynecol. 2012, 207, 44.e1–44.e13. [Google Scholar] [CrossRef]
- Pan, Y.; Liu, M.B. The value of hysteroscopic management of cesarean scar pregnancy: A report of 44 cases. Taiwan J. Obstet. Gynecol. 2017, 56, 139–142. [Google Scholar] [CrossRef]
- Li, Y.Y.; Yin, Z.Y.; Li, S.; Xu, H.; Zhang, X.P.; Cheng, H.; Du, L.; Zhou, X.Y.; Zhang, B. Comparison of transvaginal surgery and methotrexate/mifepristone-combined transcervical resection in the treatment of cesarean scar pregnancy. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2957–2963. [Google Scholar]
- Pristavu, A.; Vinturache, A.; Mihalceanu, E.; Pintilie, R.; Onofriescu, M.; Socolov, D. Combination of medical and surgical management in successful treatment of caesarean scar pregnancy: A case report series. BMC Pregnancy Childbirth 2020, 20, 617. [Google Scholar] [CrossRef]
- Cali, G.; Timor-Tritsch, I.E.; Forlani, F.; Palacios-Jaraquemada, J.; Monteagudo, A.; Kaelin Agten, A.; Flacco, M.E.; Khalil, A.; Buca, D.; Manzoli, L.; et al. Value of first-trimester ultrasound in prediction of third-trimester sonographic stage of placenta accreta spectrum disorder and surgical outcome. Ultrasound Obstet. Gynecol. 2020, 55, 450–459. [Google Scholar] [CrossRef]
- Hsu, C.C.; Huang, K.G. Evolving Cesarean Scar Pregnancy into Morbidity Adherent Placenta-Evidence from Serial Ultrasound Examination. J. Med. Ultrasound 2017, 25, 47–51. [Google Scholar] [CrossRef]
- Kaelin Agten, A.; Cali, G.; Monteagudo, A.; Oviedo, J.; Ramos, J.; Timor-Tritsch, I. The clinical outcome of cesarean scar pregnancies implanted “on the scar” versus “in the niche”. Am. J. Obstet. Gynecol. 2017, 216, 510.e1–510.e6. [Google Scholar] [CrossRef] [PubMed]
- Rotas, M.A.; Haberman, S.; Levgur, M. Cesarean scar ectopic pregnancies: Etiology, diagnosis, and management. Obstet. Gynecol. 2006, 107, 1373–1381. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liu, X.; Xie, L.; Ye, Z.; Gan, L. Diagnostic accuracy and cut-off of contrast-enhanced ultrasound in caesarean scar pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 246, 117–122. [Google Scholar] [CrossRef]
- Park, B.H.; Marches, S.; Eichelberger, B.M.; Winter, M.D.; Pozzi, A.; Banks, S.A. Quantifying dog meniscal volume at 1.5T and 3.0T MRI. Res. Vet. Sci. 2020, 128, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Osborn, D.A.; Williams, T.R.; Craig, B.M. Cesarean scar pregnancy: Sonographic and magnetic resonance imaging findings, complications, and treatment. J. Ultrasound Med. 2012, 31, 1449–1456. [Google Scholar] [CrossRef]
- Maurea, S.; Romeo, V.; Mainenti, P.P.; Ginocchio, M.I.; Frauenfelder, G.; Verde, F.; Liuzzi, R.; D’Armiento, M.; Sarno, L.; Morlando, M.; et al. Diagnostic accuracy of magnetic resonance imaging in assessing placental adhesion disorder in patients with placenta previa: Correlation with histological findings. Eur. J. Radiol. 2018, 106, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Romeo, V.; Maurea, S. The new era of advanced placental tissue characterization using MRI texture analysis: Clinical implications. EBioMedicine 2020, 51, 102588. [Google Scholar] [CrossRef]
- Sorrentino, F.; De Feo, V.; Stabile, G.; Tinelli, R.; D’Alterio, M.N.; Ricci, G.; Angioni, S.; Nappi, L. Cesarean Scar Pregnancy Treated by Artery Embolization Combined with Diode Laser: A Novel Approach for a Rare Disease. Medicina 2021, 57, 411. [Google Scholar] [CrossRef]
- Wang, Y.; Zhou, Y.; Zeng, L.; Chen, L.; Zhao, Y. Analysis of risk factors for massive intraoperative bleeding in patients with placenta accreta spectrum. BMC Pregnancy Childbirth 2022, 22, 116. [Google Scholar] [CrossRef]
- Polat, I.; Alkis, I.; Sahbaz, A.; Sahin, O.; Ekiz, A.; Gulac, B.; Tekirdag, A.I. Diagnosis and management of cesarean scar pregnancy. Clin. Exp. Obstet. Gynecol. 2012, 39, 365–368. [Google Scholar] [PubMed]
- Al-Nazer, A.; Omar, L.; Wahba, M.; Abbas, T.; Abdulkarim, M. Ectopic intramural pregnancy developing at the site of a cesarean section scar: A case report. Cases J. 2009, 2, 9404. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, J.; Exner, M.; Bremicker, K.; Grothoff, M.; Stumpp, P.; Schrey-Petersen, S.; Stepan, H. Cesarean section scar in 3 T magnetic resonance imaging and ultrasound: Image characteristics and comparison of the methods. Arch. Gynecol. Obstet. 2019, 299, 439–449. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | Ages | Previous Pregnancies | Previous Cesarian Section | GA (Weeks) at TVUS Exam | Final Diagnosis |
|---|---|---|---|---|---|
| 1 | 30 | 4 | 3 | 8 w and 4 d | CSP I |
| 2 | 35 | 3 | 2 | 6 w and 6 d | CSP II |
| 3 | 43 | 3 | 1 | 8 w and 3 d | CSP I |
| 4 | 31 | 1 | 1 | 7 weeks | Low-implanted pregnancy |
| 5 | 35 | 1 | 1 | 7 w and 4 d | CSP I |
| 6 | 28 | 2 | 2 | 10 w | Low-implanted pregnancy |
| 7 | 32 | 2 | 2 | 9 w and 5 d | Cervico-isthmic pregnancy |
| Empty Uterus | Empty Endocervical Canal | Trophoblast within the CS | GS Ovoid and Regularly Shaped | Vascularity of GS at CD | Myometrium (Measured between the Gestation Sac and Bladder Wall) (1–4 mm) or Discontinuous or Absent | Cleavage Points between the Uterus and Bladder | Negative “Sliding Organ Sign” | Diagnosis | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Patient 1 | TVUS | + | + | + | + | + | + | − | + | CSP I |
| MRI | + | + | + | + | − | + | + | − | ||
| Patient 2 | TVUS | + | + | + | + | + | + | − | + | CSP II |
| MRI | + | + | + | + | − | + | + | − | ||
| Patient 3 | TVUS | + | + | + | + | + | + | − | + | CSP I |
| MRI | + | + | + | + | − | + | + | − | ||
| Patient 4 | TVUS | + | + | − | + | + | + | − | + | Low-implanted pregnancy |
| MRI | + | + | − | + | − | + | + | − | ||
| Patient 5 | TVUS | + | + | + | + | + | + | − | + | CSP I |
| MRI | + | + | + | + | − | + | + | − | ||
| Patient 6 | TVUS | + | + | − | + | + | + | − | + | Low-implanted pregnancy |
| MRI | + | + | − | + | − | + | + | − | ||
| Patient 7 | TVUS | + | − | − | + | + | + | − | − | Cervico-isthmic pregnancy |
| MRI | + | − | − | + | − | + | + | − |
| Patient Number | Depth of Scar mm (d) | Width of Scar (w) | Scar Myometrial Thickness (t) | Adjacent Myometrial Thickness (T) |
|---|---|---|---|---|
| #1 | 13 mm | 25 mm | <1 mm | 9 mm |
| #2 | 29 mm | 38 mm | <1 mm | 18 mm |
| #3 | 10 mm | 26 mm | <1 mm | 3 mm |
| #4 | 12 mm | 23 mm | <1 mm | 8 mm |
| #5 | 9 mm | 18 mm | 2 mm | 10 mm |
| #6 | 6 mm | 22 mm | <1 mm | 9 mm |
| #7 | 15 mm | 49 mm | <1 mm | 8 mm |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Comune, R.; Liguori, C.; Tamburrini, S.; Arienzo, F.; Gallo, L.; Dell’Aversana, F.; Pezzullo, F.; Tamburro, F.; Affinito, P.; Scaglione, M. MRI Assessment of Cesarean Scar Pregnancies: A Case Series. J. Clin. Med. 2023, 12, 7241. https://doi.org/10.3390/jcm12237241
Comune R, Liguori C, Tamburrini S, Arienzo F, Gallo L, Dell’Aversana F, Pezzullo F, Tamburro F, Affinito P, Scaglione M. MRI Assessment of Cesarean Scar Pregnancies: A Case Series. Journal of Clinical Medicine. 2023; 12(23):7241. https://doi.org/10.3390/jcm12237241
Chicago/Turabian StyleComune, Rosita, Carlo Liguori, Stefania Tamburrini, Francesco Arienzo, Luigi Gallo, Federica Dell’Aversana, Filomena Pezzullo, Fabio Tamburro, Pietro Affinito, and Mariano Scaglione. 2023. "MRI Assessment of Cesarean Scar Pregnancies: A Case Series" Journal of Clinical Medicine 12, no. 23: 7241. https://doi.org/10.3390/jcm12237241