
Visual Outcomes of Traumatic Lens Dislocations and Subluxations Managed by Pars Plana Vitrectomy and Lensectomy
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
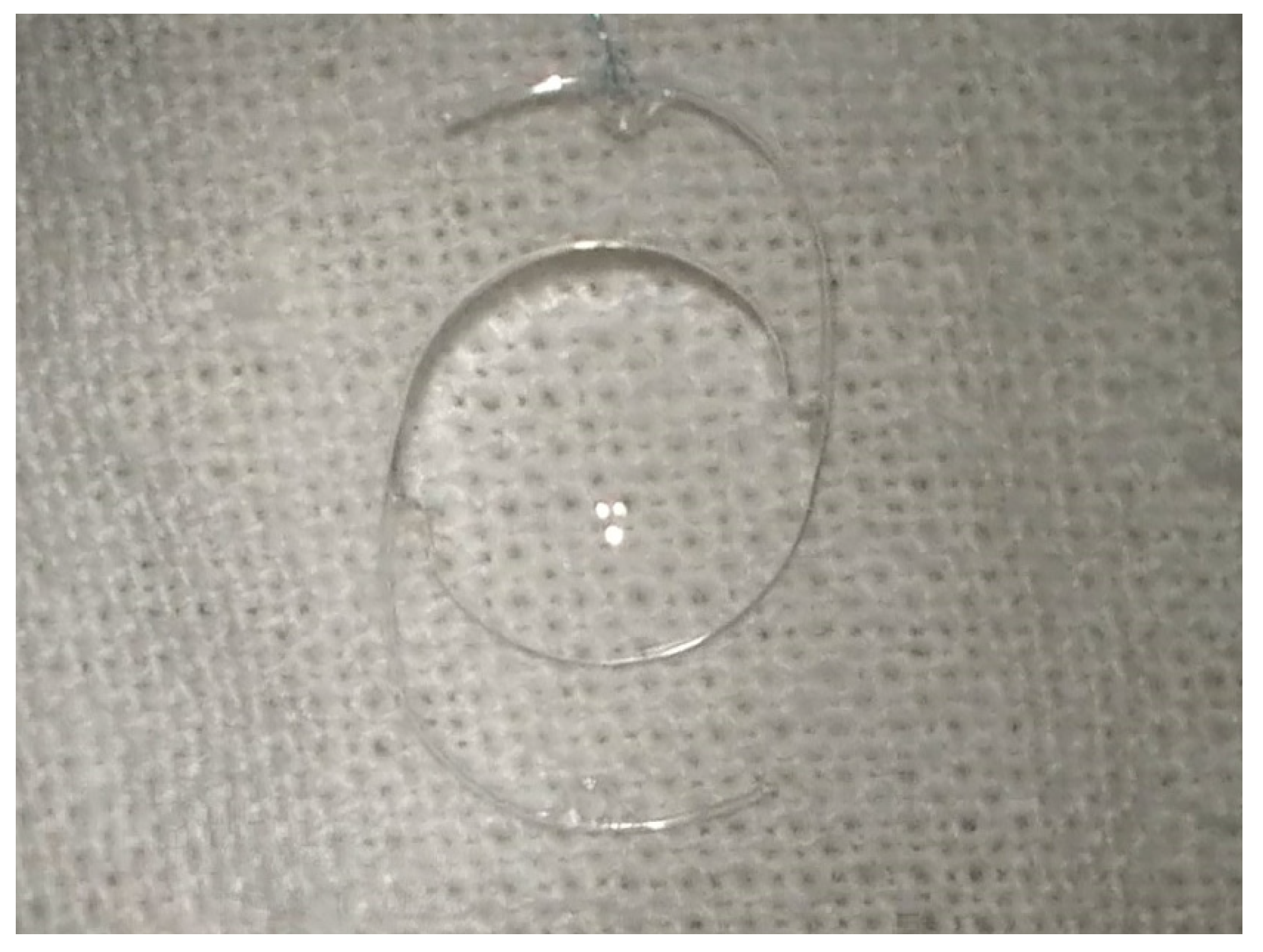
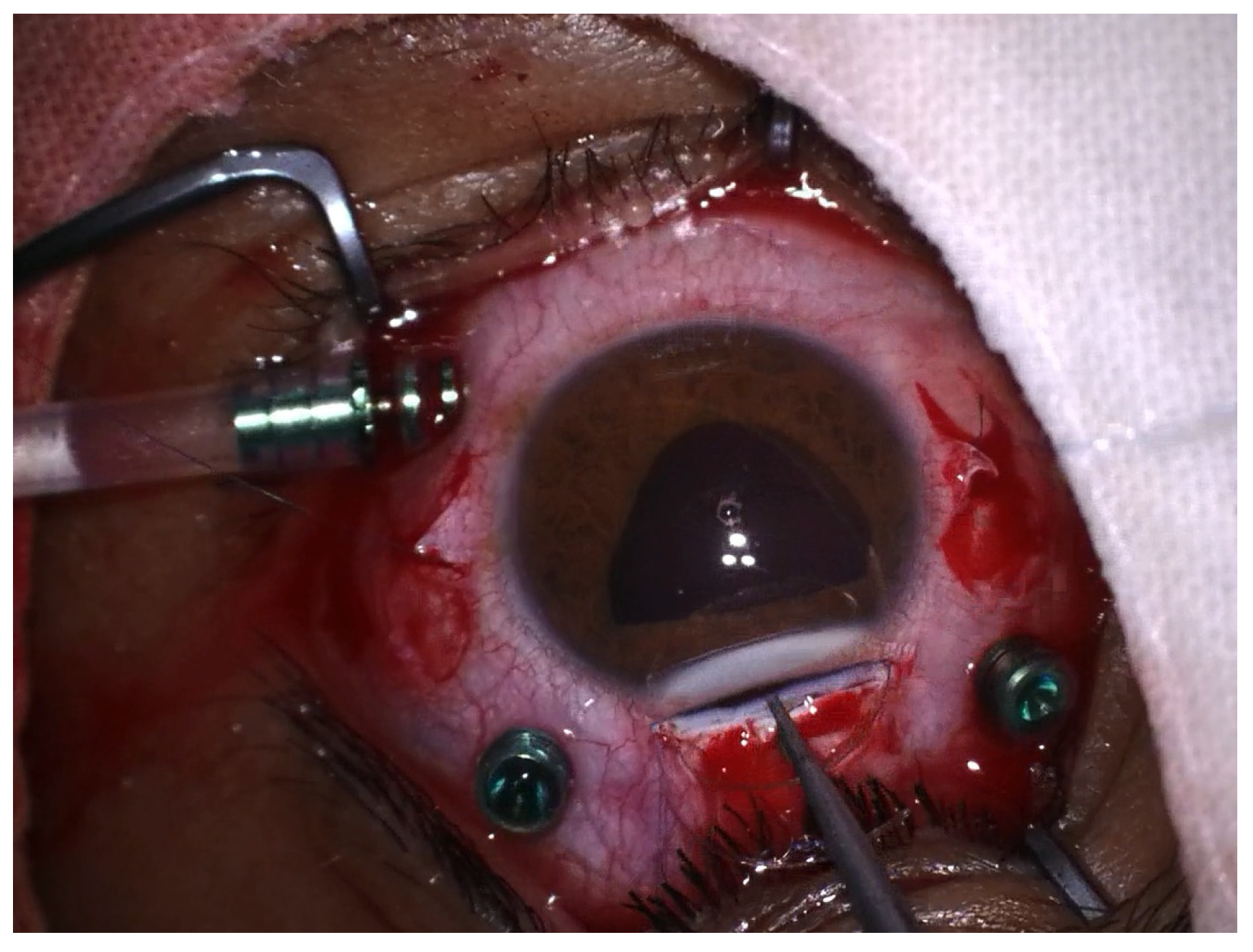
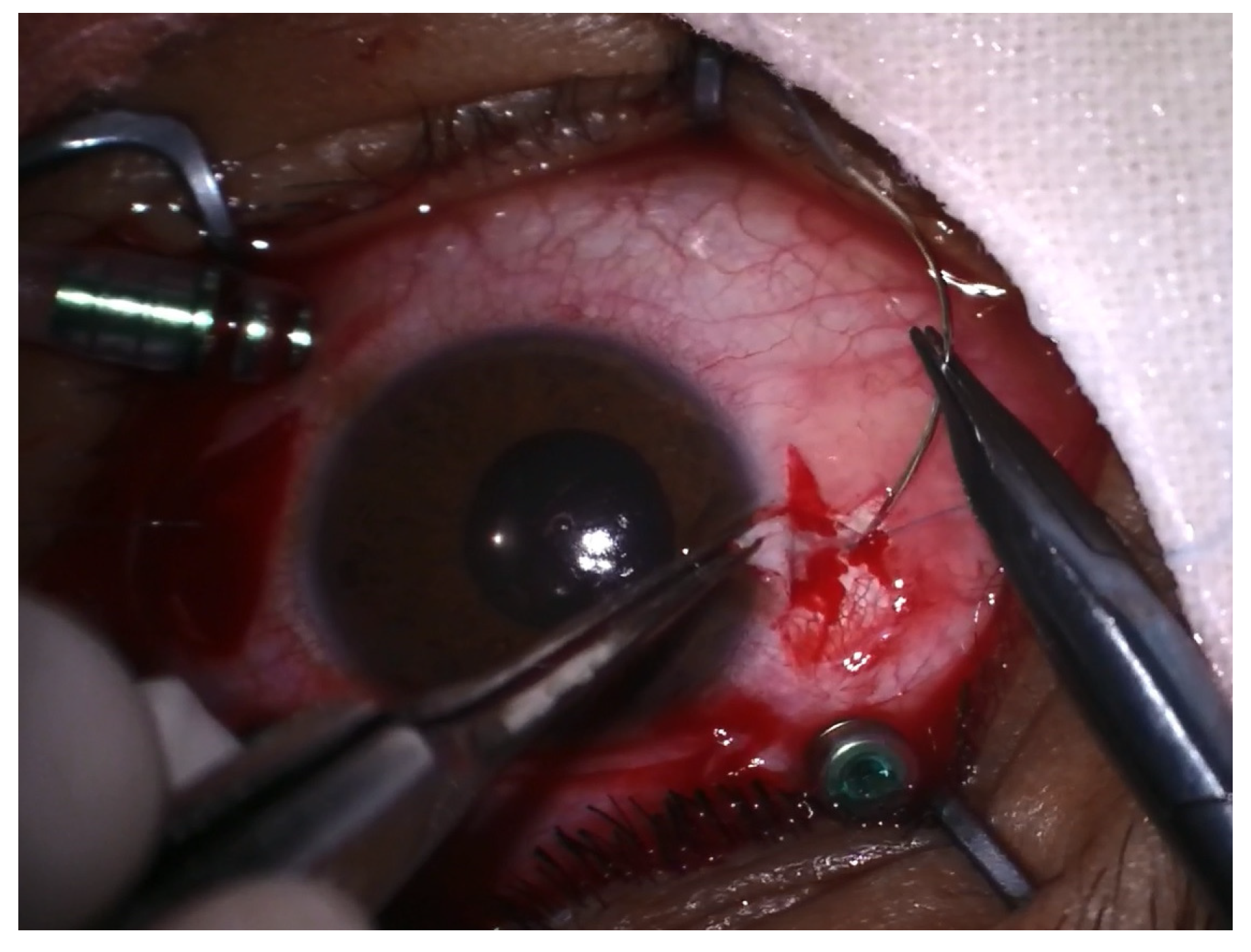
2.2. Surgical Technique
2.3. Statistical Analysis
3. Results
3.1. Demographic Results
3.2. Initial BCVA, Visual Outcome and Prognostic Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klopfer, J.; Tielsch, J.M.; Vitale, S.; See, L.C.; Canner, J.K. Ocular Trauma in the United States: Eye Injuries Resulting in Hospitalization, 1984 through 1987. Arch. Ophthalmol. 1992, 110, 838–842. [Google Scholar] [CrossRef]
- Négrel, A.D.; Thylefors, B. The Global Impact of Eye Injuries. Ophthalmic Epidemiol. 1998, 5, 143–169. [Google Scholar] [CrossRef]
- Bord, S.P.; Linden, J. Trauma to the Globe and Orbit. Emerg. Med. Clin. N. Am. 2008, 26, 97–123. [Google Scholar] [CrossRef]
- Salehi-Had, H.; Turalba, A. Management of Traumaticcrystalline Lens Subluxation and Dislocation. Int. Ophthalmol. Clin. 2010, 50, 167–179. [Google Scholar] [CrossRef]
- Kuhn, F.; Morris, R.; Witherspoon, C.D.; Mann, L. Blunt-Force Injuries Involving the Posterior Segment. Retin. Physician 2007, 20, 4. [Google Scholar]
- Spraul, C.W.; Grossniklaus, H.E. Vitreous Hemorrhage. Surv. Ophthalmol. 1997, 42, 3–39. [Google Scholar] [CrossRef]
- Nicoară, S.D.; Irimescu, I.; Călinici, T.; Cristian, C. Intraocular Foreign Bodies Extracted by Pars Plana Vitrectomy: Clinical Characteristics, Management, Outcomes and Prognostic Factors. BMC Ophthalmol. 2015, 15, 151. [Google Scholar] [CrossRef]
- Hapca, M.C.; Muntean, G.A.; Drăgan, I.A.N.; Vesa, Ș.C.; Nicoară, S.D. Outcomes and Prognostic Factors Following Pars Plana Vitrectomy for Intraocular Foreign Bodies—11-Year Retrospective Analysis in a Tertiary Care Center. J. Clin. Med. 2022, 11, 4482. [Google Scholar] [CrossRef]
- Yeh, S.; Colyer, M.H.; Weichel, E.D. Current Trends in the Management of Intraocular Foreign Bodies. Curr. Opin. Ophthalmol. 2008, 19, 225–233. [Google Scholar] [CrossRef]
- Liu, C.C.H.; Tong, J.M.K.; Li, P.S.H.; Li, K.K.W. Epidemiology and Clinical Outcome of Intraocular Foreign Bodies in Hong Kong: A 13-Year Review. Int. Ophthalmol. 2017, 37, 55–61. [Google Scholar] [CrossRef]
- Gokce, G.; Sobaci, G.; Ozgonul, C. Post-Traumatic Endophthalmitis: A Mini-Review. Semin. Ophthalmol. 2015, 30, 470–474. [Google Scholar] [CrossRef]
- Hapca, M.C.; Vesa, Ș.C.; Nicoară, S.D. Visual Outcomes and Prognostic Factors of Traumatic Endophthalmitis Treated by Pars Plana Vitrectomy: 11 Years Retrospective Analysis. J. Clin. Med. 2023, 12, 502. [Google Scholar] [CrossRef]
- Marcus, D.M.; Topping, T.M.; Frederick, A.R. Vitreoretinal Management of Traumatic Dislocation of the Crystalline Lens. Int. Ophthalmol. Clin. 1995, 35, 139–150. [Google Scholar] [CrossRef]
- Jarrett WH, I.I. Dislocation of the Lens. A Study of 166 Hospitalized Cases. Arch. Ophthalmol. 1967, 78, 289–296. [Google Scholar] [CrossRef]
- Robinson, D.H.; Leonard, B.N.; Scott, E.O. Harley’s Pediatric Ophthalmology, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005; ISBN 9780781750837. [Google Scholar]
- Chaudhry, N.A.; Belfort, A.; Flynn, H.W.J.; Tabandeh, H.; Smiddy, W.E.; Murray, T.G. Combined Lensectomy, Vitrectomy and Scleral Fixation of Intraocular Lens Implant after Closed-Globe Injury. Ophthalmic Surg. Lasers 1999, 30, 375–381. [Google Scholar] [CrossRef]
- Kuhn, F.; Morris, R.; Witherspoon, C.D.; Mann, L. Epidemiology of Blinding Trauma in the United States Eye Injury Registry. Ophthalmic Epidemiol. 2006, 13, 209–216. [Google Scholar] [CrossRef]
- Yaşa, D. Pars Plana Lensectomy Combined with Pars Plana Vitrectomy in Traumatic Ectopia Lentis. Beyoglu Eye J. 2017, 2, 81–84. [Google Scholar] [CrossRef]
- Singhal, A.; Sharma, A.; Sasirekha, M. Visual Outcome in Patients Operated for Traumatic Cataract: A Prospective Hospital Based Study. Indian J. Clin. Exp. Ophthalmol. 2020, 6, 563–567. [Google Scholar] [CrossRef]
- Peyman, G.A.; Raichand, M.; Goldberg, M.F.; Ritacca, D. Management of Subluxated and Dislocated Lenses with the Vitrophage. Br. J. Ophthalmol. 1979, 63, 771–778. [Google Scholar] [CrossRef]
- Kodjikian, L.; Beby, F.; Spire, M.; Gambrelle, J.; Hubert, I.; Burillon, C.; Grange, J.D.; Garweg, J.G. Combined Pars Plana Phacofragmentation, Vitrectomy, and Artisan Lens Implantation for Traumatic Subluxated Cataracts. Retina 2006, 26, 909–916. [Google Scholar] [CrossRef]
- Greven, C.M.; Collins, A.S.; Slusher, M.M.; Weaver, R.G. Visual Results, Prognostic Indicators, and Posterior Segment Findings Following Surgery for Cataract/Lens Subluxation-Dislocation Secondary to Ocular Contusion Injuries. Retina 2002, 22, 575–580. [Google Scholar] [CrossRef]
- Moore, J.K.; Scott, I.U.; Flynn, H.W.; Smiddy, W.E.; Murray, T.G.; Kim, J.E.; Vilar, N.F.; Pereira, M.B.; Jorge, R. Retinal Detachment in Eyes Undergoing Pars Plana Vitrectomy for Removal of Retained Lens Fragments. Ophthalmology 2003, 110, 709–713. [Google Scholar] [CrossRef]
- Kazemi, S.; Wirostko, W.J.; Sinha, S.; Mieler, W.F.; Koenig, S.B.; Sheth, B.P. Combined Pars Plana Lensectomy-Vitrectomy with Open-Loop Flexible Anterior Chamber Intraocular Lens (AC IOL) Implantation for Subluxated Lenses. Trans. Am. Ophthalmol. Soc. 2000, 98, 247–251, discussion 251–253. [Google Scholar]
- Oh, J.; Smiddy, W.E. Pars Plana Lensectomy Combined with Pars Plana Vitrectomy for Dislocated Cataract. J. Cataract Refract. Surg. 2010, 36, 1189–1194. [Google Scholar] [CrossRef]
- Girard, L.J. Pars Plana Lensectomy by Ultrasonic Fragmentation. Surv. Ophthalmol. 1982, 27, 96–101. [Google Scholar] [CrossRef]
- Seo, M.S.; Yoon, K.C.; Lee, C.H. Phacofragmentation for the Treatment of a Completely Posterior Dislocation of the Total Crystalline Lens. Korean J. Ophthalmol. 2002, 16, 32. [Google Scholar] [CrossRef]
- Jurman, M.; Jones, W.L.; Harris, S.L. Traumatic Dislocation of the Crystalline Lens with Delayed Total Retinal Detachment. J. Am. Optom. Assoc. 1990, 61, 285–290. [Google Scholar]
- Zhang, H.; Dong, J.; Jin, K.; Wang, G.; Xu, D.; Huo, M. Efficacy of Removing Dislocated Lens Using Intravitreal Phacoemulsification. Eye Sci. 2012, 27, 8–10. [Google Scholar] [CrossRef]
- Tabatabaei, S.A.; Rajabi, M.B.; Tabatabaei, S.M.; Soleimani, M.; Rahimi, F.; Yaseri, M. Early versus Late Traumatic Cataract Surgery and Intraocular Lens Implantation. Eye 2017, 31, 1199–1204. [Google Scholar] [CrossRef]
- Agrawal, R.; Keane, P.A.; Singh, J.; Saihan, Z.; Kontos, A.; Pavesio, C.E. Classification of Semi-Automated Flare Readings Using the Kowa FM 700 Laser Cell Flare Meter in Patients with Uveitis. Acta Ophthalmol. 2016, 94, e135–e141. [Google Scholar] [CrossRef]
- Slusher, M.M.; Greven, C.M.; Yu, D.D. Posterior Chamber Intraocular Lens Implantation Combined with Lensectomy-Vitrectomy and Intraretinal Foreign-Body Removal. Arch. Ophthalmol. 1992, 110, 127–129. [Google Scholar] [CrossRef] [PubMed]
- Rubsamen, P.E.; Irvine, W.D.; McCuen, B.W.; Smiddy, W.E.; Bowman, C.B. Primary Intraocular Lens Implantation in the Setting of Penetrating Ocular Trauma. Ophthalmology 1995, 102, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Lam, D.S.C.; Tham, C.C.Y.; Kwok, A.K.H.; Gopal, L. Combined Phacoemulsification, Pars Plana Vitrectomy, Removal of Intraocular Foreign Body (IOFB), and Primary Intraocular Lens Implantation for Patients with IOFB and Traumatic Cataract. Eye 1998, 12, 395–398. [Google Scholar] [CrossRef]
- Muga, R.; Maul, E. The Management of Lens Damage in Perforating Corneal Lacerations. Br. J. Ophthalmol. 1978, 62, 784–787. [Google Scholar] [CrossRef] [PubMed]
- Andenmatten, R.; Gonvers, M. Sophisticated Vitreoretinal Surgery in Patients with a Healthy Fellow Eye—An 11-Year Retrospective Study. Graefe’s Arch. Clin. Exp. Ophthalmol. 1993, 231, 495–499. [Google Scholar] [CrossRef]
- Assi, A.; Chacra, C.B.; Cherfan, G. Combined Lensectomy, Vitrectomy, and Primary Intraocular Lens Implantation in Patients with Traumatic Eye Injury. Int. Ophthalmol. 2008, 28, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Yalniz-Akkaya, Z.; Burcu, A.; Uney, G.O.; Abay, I.; Eksioglu, U.; Acar, M.A.; Ornek, F. Primary and Secondary Implantation of Scleral-Fixated Posterior Chamber Intraocular Lenses in Adult Patients. Middle East Afr. J. Ophthalmol. 2014, 21, 44–49. [Google Scholar] [CrossRef]
- Lee, V.Y.W.; Yuen, H.K.L.; Kwok, A.K.H. Comparison of Outcomes of Primary and Secondary Implantation of Scleral Fixated Posterior Chamber Intraocular Lens. Br. J. Ophthalmol. 2003, 87, 1459–1462. [Google Scholar] [CrossRef]
- Malbran, E.S.; Malbran, E.J.; Negri, I. Lens Guide Suture for Transport and Fixation in Secondary IOL Implantation after Intracapsular Extraction. Int. Ophthalmol. 1986, 9, 151–160. [Google Scholar] [CrossRef]
- Kumar, D.A.; Agarwal, A.; Packiyalakshmi, S.; Jacob, S.; Agarwal, A. Complications and Visual Outcomes after Glued Foldable Intraocular Lens Implantation in Eyes with Inadequate Capsules. J. Cataract Refract. Surg. 2013, 39, 1211–1218. [Google Scholar] [CrossRef]
- Yamane, S.; Sato, S.; Maruyama-Inoue, M.; Kadonosono, K. Flanged Intrascleral Intraocular Lens Fixation with Double-Needle Technique. Ophthalmology 2017, 124, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Wagoner, M.D.; Cox, T.A.; Ariyasu, R.G.; Jacobs, D.S.; Karp, C.L. Intraocular Lens Implantation in the Absence of Capsular Support: A Report by the American Academy of Ophthalmology. Ophthalmology 2003, 110, 840–859. [Google Scholar] [CrossRef]
- Jacob, S.; Kumar, D.A.; Rao, N.K. Scleral Fixation of Intraocular Lenses. Curr. Opin. Ophthalmol. 2020, 31, 50–60. [Google Scholar] [CrossRef]
- Kjeka, O.; Bohnstedt, J.; Meberg, K.; Seland, J.H. Implantation of Scleral-Fixated Posterior Chamber Intraocular Lenses in Adults. Acta Ophthalmol. 2008, 86, 537–542. [Google Scholar] [CrossRef]
- Tsatsos, M.; Vartsakis, G.; Athanasiadis, I.; Papavasileiou, E.; Yesilirmak, N.; Ziakas, N. Intraocular Lens Implantation in the Absence of Capsular Support: Iris Fixation. Eye 2022, 36, 1718–1720. [Google Scholar] [CrossRef] [PubMed]
- Calzetti, G.; Bellucci, C.; Tedesco, S.A.; Rossi, M.; Gandolfi, S.; Mora, P. Tilt and Decentration of Posterior and Anterior Iris-Claw Intraocular Lenses: A Pilot Study Using Anterior Segment Optical Coherence Tomography. BMC Ophthalmol. 2022, 22, 233. [Google Scholar] [CrossRef]
- Bellucci, C.; Perrella, A.; Rossi, M.; Papapicco, A.; Spadini, F.; Tedesco, S.A.; Gandolfi, S.; Mora, P. Light- and Drug-Induced Pupillary Dynamics in Eyes with a Retropupillary Iris-Claw Intraocular Lens. Graefe’s Arch. Clin. Exp. Ophthalmol. 2023, 261, 2301–2305. [Google Scholar] [CrossRef]
- Fujikawa, A.; Mohamed, Y.H.; Kinoshita, H.; Matsumoto, M.; Uematsu, M.; Tsuiki, E.; Suzuma, K.; Kitaoka, T. Visual Outcomes and Prognostic Factors in Open-Globe Injuries. BMC Ophthalmol. 2018, 18, 138. [Google Scholar] [CrossRef] [PubMed]
- Rofail, M.; Lee, G.A.; O’rourke, P. Prognostic Indicators for Open Globe Injury. Clin. Exp. Ophthalmol. 2006, 34, 783–786. [Google Scholar] [CrossRef] [PubMed]
- Bieliński, P.; Jasielska, M.; Wyszyńska, A.; Winiarczyk, M.; Mackiewicz, J. Pars Plana Vitrectomy with Transscleral Fixation of Posterior Chamber Lens in the Treatment of Post-Traumatic Lens Dislocation. Int. Ophthalmol. 2019, 39, 455–460. [Google Scholar] [CrossRef]
- Mayer, C.S.; Hoffmann, A.M.; Prahs, P.; Reznicek, L.; Khoramnia, R. Functional Outcomes after Combined Iris and Intraocular Lens Implantation in Various Iris and Lens Defects. BMC Ophthalmol. 2020, 20, 370. [Google Scholar] [CrossRef] [PubMed]
- Duke-Elder, S. Text-Book of Ophthalmology, 3rd ed.; CV Mosby: St. Louis, MO, USA, 1954. [Google Scholar]
- Huang, H.M.; Kao, M.L.; Kuo, H.K.; Tsai, S.H.; Chen, Y.J.; Liu, C.C. Visual Results and Complications after Trans Pars Plana Vitrectomy and Lensectomy for Lens Dislocation. Chang Gung Med. J. 2004, 27, 429–435. [Google Scholar] [PubMed]
- Cox, M.S. Retinal Breaks Caused by Blunt Nonperforating Trauma at the Point of Impact. Trans. Am. Ophthalmol. Soc. 1980, 78, 414–466. [Google Scholar] [PubMed]
- Ke, G.; Zhou, E.; Zhu, K.; Wei, Y.; Wang, Z.; Jia, Y.; Wang, S.; Gu, Y. Retinal Break Associated with Traumatic Lens Dislocation or Subluxation Requiring Vitrectomy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 693–697. [Google Scholar] [CrossRef]
- Ghazi, N.G.; Green, W.R. Pathology and Pathogenesis of Retinal Detachment. Eye 2002, 16, 411–421. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.; Chung, H. Factors Contributing to Retinal Detachment after Transscleral Fixation of Posterior Chamber Intraocular Lenses. J. Cataract Refract. Surg. 1998, 24, 697–702. [Google Scholar] [CrossRef]
- Kuhn, F.; Maisiak, R.; Mann, L.; Mester, V.; Morris, R.; Witherspoon, C. The Ocular Trauma Score (OTS). Ophthalmol. Clin. N. Am. 2002, 15, 163–165. [Google Scholar] [CrossRef]
- Sobacı, G.; Akin, T.; Erdem, Ü.; Uysal, Y.; Karagül, S. Ocular Trauma Score in Deadly Weapon–Related Open-Globe Injuries. Am. J. Ophthalmol. 2006, 141, 760–761. [Google Scholar] [CrossRef]
- Unal, M.H.; Aydin, A.; Sonmez, M.; Ayata, A.; Ersanli, D. Validation of the Ocular Trauma Score for Intraocular Foreign Bodies in Deadly Weapon-Related Open-Globe Injuries. Ophthalmic Surg. Lasers Imaging Retin. 2008, 39, 121–124. [Google Scholar] [CrossRef]
- Uysal, Y.; Mutlu, F.M.; Sobac, G. Ocular Trauma Score in Childhood Open-Globe Injuries. J. Trauma Acute Care Surg. 2008, 65, 1284–1286. [Google Scholar] [CrossRef]
- Qi, Y.; Zhang, Y.F.; Zhu, Y.; Wan, M.G.; Du, S.S.; Yue, Z.Z. Prognostic Factors for Visual Outcome in Traumatic Cataract Patients. J. Ophthalmol. 2016, 2016, 1748583. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.F.; Deng, S.; Hammersmith, K.M.; Kuo, A.N.; Li, J.Y.; Weikert, M.P.; Shtein, R.M. Intraocular Lens Implantation in the Absence of Zonular Support: An Outcomes and Safety Update. Ophthalmology 2020, 127, 1234–1258. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | BCVA < 0.1 | BCVA ≥ 0.1 | p Value | |
|---|---|---|---|---|
| Gender | Female (n = 21) Male (n = 49) | 11 (28.9%) 27 (71.1%) | 10 (31.3%) 22 (68.7%) | 1.000 |
| Age | <50 (n = 18) ≥50 (n = 52) | 10 (26.3%) 28 (73.7%) | 8 (25.0%) 24 (75.0%) | 1.000 |
| Eye | Right (n = 37) Left (n = 33) | 20 (52.6%) 18 (47.4%) | 17 (53.1%) 15 (46.9%) | 1.000 |
| Eye protection | Yes (n = 0) No (n = 70) | - 38 (100%) | - 32 (100%) | |
| Location | Rural (n = 46) Urban (n = 24) | 27 (71.1%) 11 (28.9%) | 19 (59.4%) 13 (40.6%) | 0.440 |
| VA | Preoperative BCVA n (%) | Postoperative BCVA n (%) |
|---|---|---|
| ≥0.1 | 6 (8.57) | 32 (45.71) |
| <0.1 | 18 (25.71) | 19 (27.14) |
| CF | 20 (28.57) | 9 (12.85) |
| HM | 20 (28.57) | 5 (7.14) |
| LP | 4 (5.71) | 2 (2.85) |
| NLP | 2 (2.85) | 3 (4.28) |
| Total | 70 | 70 |
| Factor | Final VA, n (%) | p Value | |
|---|---|---|---|
| <0.1 | ≥0.1 | ||
| Age | |||
| <50 | 10 (26.3) | 8 (25.0) | 1.000 |
| ≥50 | 28 (73.7) | 24 (75.0) | |
| Initial VA | |||
| <0.1 | 37 (97.4) | 26 (81.3) | 0.000 |
| ≥0.1 | 1 (2.6) | 6 (18.7) | |
| Iridodonesis | |||
| Yes | 7 (18.4) | 16 (50.0) | 0.011 |
| No | 31 (81.6) | 16 (50.0) | |
| Phacodonesis | |||
| Yes | 2 (5.3) | 5 (15.6) | 0.234 |
| No | 36 (94.7) | 27 (84.4) | |
| RD | |||
| Yes | 11 (28.9) | 2 (6.2) | 0.014 |
| No | 27 (71.1) | 30 (93.8) | |
| IOFB | |||
| Yes | 3 (7.9) | 3 (9.4) | 1.000 |
| No | 35 (92.1) | 29 (90.6) | |
| VH | |||
| Yes | 8 (21.1) | 10 (31.3) | 0.485 |
| No | 30 (78.9) | 22 (68.7) | |
| Secondary glaucoma | |||
| Yes | 13 (34.2) | 4 (12.5) | 0.067 |
| No | 25 (65.8) | 28 (87.5) | |
| Dislocation mechanism | |||
| PC rupture | 7 (18.4) | 4 (12.5) | 0.727 |
| Zonular rupture | 31 (81.6) | 28 (87.5) | |
| Hyphema | |||
| Yes | 6 (15.8) | 4 (12.5) | 0.745 |
| No | 32 (84.2) | 28 (87.5) | |
| Timing of PPV | |||
| <1 month | 29 (76.3) | 24 (75.0) | 1.000 |
| >1 month | 9 (23.7) | 8 (25.0) | |
| Final Lens Position | Number (%) |
|---|---|
| PC IOL scleral fixation | 51 (72.9%) |
| PC IOL in sulcus | 1 (1.4%) |
| PC IOL in the bag | 3 (4.3%) |
| Aphakia | 15 (21.4%) |
| OTS | Final VA Group | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NLP | HM/LP | CF-<0.1 | 0.1–0.4 | ≥0.5 | ||||||||
| OTS | (%) | p Value | (%) | p Value | (%) | p Value | (%) | p Value | (%) | p Value | Total p Value | |
| Our Study (70) | N (%) | N (%) | N (%) | N (%) | N (%) | |||||||
| 1 | OTS Our Study (2) | (73) 0 (0) | 0.02 | (17) 2 (100) | 0.002 | (7) 0 (0) | 0.69 | (2) 0 (0) | 0.83 | (1) 0 (0) | 0.88 | <0.001 |
| 2 | OTS Our Study (16) | (28) 3 (18.75) | 0.43 | (26) 3 (18.75) | 0.53 | (18) 7 (43.75) | 0.02 | (13) 2 (12.5) | 0.95 | (15) 1 (6.25) | 0.34 | 0.001 |
| 3 | OTS Our Study (47) | (2) 0 (0) | 0.32 | (11) 2 (4.25) | 0.18 | (15) 22 (46.81) | <0.001 | (28) 18 (38.3) | 0.2 | (44) 5 (10.64) | <0.001 | <0.001 |
| 4 | OTS Our Study (5) | (1) 0 (0) | 0.82 | (2) 0 (0) | 0.74 | (2) 0 (0) | 0.74 | (21) 0 (0) | 0.25 | (74) 5 (100) | 0.18 | <0.001 |
| 5 | OTS Our Study | (0) 0 (0) | - | (1) 0 (0) | - | (2) 0 (0) | - | (5) 0 (0) | - | (92) 0 (0) | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hapca, M.-C.; Muntean, G.-A.; Nemeș-Drăgan, I.-A.; Vesa, Ș.C.; Nicoară, S.-D. Visual Outcomes of Traumatic Lens Dislocations and Subluxations Managed by Pars Plana Vitrectomy and Lensectomy. J. Clin. Med. 2023, 12, 6981. https://doi.org/10.3390/jcm12226981
Hapca M-C, Muntean G-A, Nemeș-Drăgan I-A, Vesa ȘC, Nicoară S-D. Visual Outcomes of Traumatic Lens Dislocations and Subluxations Managed by Pars Plana Vitrectomy and Lensectomy. Journal of Clinical Medicine. 2023; 12(22):6981. https://doi.org/10.3390/jcm12226981
Chicago/Turabian StyleHapca, Mădălina-Claudia, George-Adrian Muntean, Iulia-Andrada Nemeș-Drăgan, Ștefan Cristian Vesa, and Simona-Delia Nicoară. 2023. "Visual Outcomes of Traumatic Lens Dislocations and Subluxations Managed by Pars Plana Vitrectomy and Lensectomy" Journal of Clinical Medicine 12, no. 22: 6981. https://doi.org/10.3390/jcm12226981