
Group A Streptococcus Infection in Neonatal Population: A Systematic Review of The Literature

 , , ,
, , ,  , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Protocol/Databases
2.2. Exclusion Criteria
- Studies that included neonates in the same group as children and adult patients and did not provide specific data regarding the neonatal population.
- Systematic reviews, meta-analyses, as well as studies coming from conference proceedings and those limited only to an abstract.
2.3. Study Outcome(s)
- Risk factors/characteristics of the affected neonates.
- Clinical presentation of GAS infection in neonates.
- Outcome of the neonates with GAS infection including mortality.
2.4. Data Synthesis and Presentation
2.5. Disagreement Resolution
3. Results
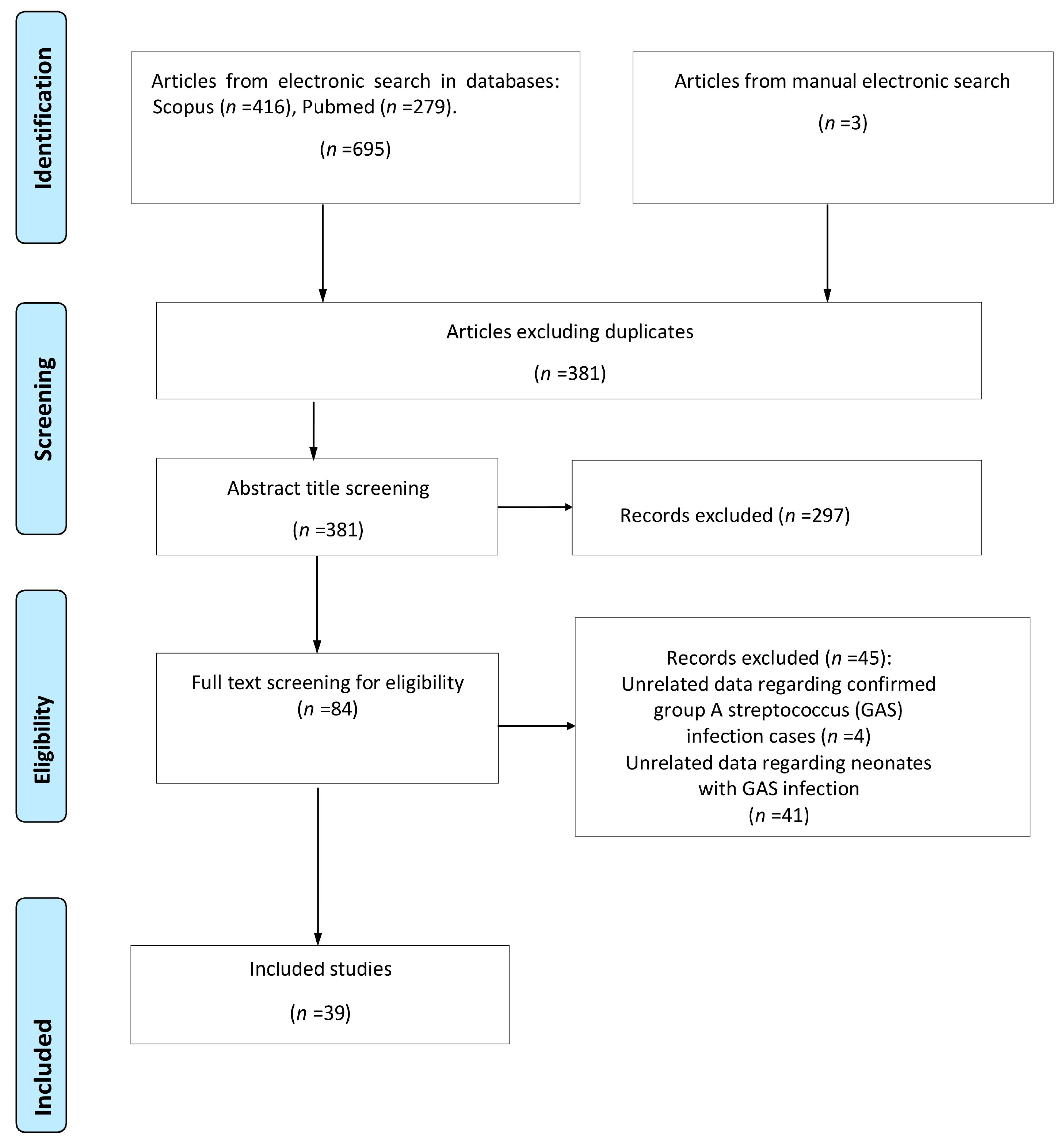
3.1. Study Selection
3.2. Study Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ershad, M.; Mostafa, A.; Dela Cruz, M.; Vearrier, D. Neonatal Sepsis. Curr. Emerg. Hosp. Med. Rep. 2019, 7, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Giannoni, E.; Agyeman, P.K.A.; Stocker, M.; Posfay-Barbe, K.M.; Heininger, U.; Spycher, B.D.; Bernhard-Stirnemann, S.; Niederer-Loher, A.; Kahlert, C.R.; Donas, A.; et al. Neonatal Sepsis of Early Onset, and Hospital-Acquired and Community-Acquired Late Onset: A Prospective Population-Based Cohort Study. J. Pediatr. 2018, 201, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Schrag, S.J.; Farley, M.M.; Petit, S.; Reingold, A.; Weston, E.J.; Pondo, T.; Hudson Jain, J.; Lynfield, R. Epidemiology of invasive early-onset neonatal sepsis, 2005 to 2014. Pediatrics 2016, 138, e20162013. [Google Scholar] [CrossRef] [PubMed]
- Weston, E.J.; Pondo, T.; Lewis, M.M.; Martell-Cleary, P.; Morin, C.; Jewell, B.; Daily, P.; Apostol, M.; Petit, S.; Farley, M.; et al. The burden of invasive early-onset neonatal sepsis in the United States, 2005–2008. Pediatr. Infect. Dis. J. 2011, 30, 937–941. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, R.G.; Kandefer, S.; Do, B.T.; Smith, P.B.; Stoll, B.J.; Bell, E.F.; Carlo, W.A.; Laptook, A.R.; Sánchez, P.J.; Shankaran, S.; et al. Late-onset Sepsis in Extremely Premature Infants: 2000–2011. Pediatr. Infect. Dis. J. 2017, 36, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Stoll, B.J.; Hansen, N.I.; Bell, E.F.; Walsh, M.C.; Carlo, W.A.; Shankaran, S.; Laptook, A.R.; Sánchez, P.J.; Van Meurs, K.P.; Wyckoff, M.; et al. Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993–2012. JAMA 2015, 314, 1039–1051. [Google Scholar] [CrossRef] [PubMed]
- Mashau, R.C.; Meiring, S.T.; Dramowski, A.; Magobo, R.E.; Quan, V.C.; Perovic, O.; von Gottberg, A.; Cohen, C.; Velaphi, S.; van Schalkwyk, E.; et al. Culture-confirmed neonatal bloodstream infections and meningitis in South Africa, 2014-19: A cross-sectional study. Lancet Glob. Health 2022, 10, e1170–e1178. [Google Scholar] [CrossRef]
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000–15: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef]
- WHO. Sustainable Development Goals—The Goals within a Goal: Health Targets for SDG 3. Available online: https://www.who.int/sdg/targets/en/ (accessed on 11 September 2023).
- Milton, R.; Gillespie, D.; Dyer, C.; Taiyari, K.; Carvalho, M.J.; Thomson, K.; Sands, K.; Portal, E.A.R.; Hood, K.; Ferreira, A.; et al. Neonatal sepsis and mortality in low-income and middle-income countries from a facility-based birth cohort: An international multisite prospective observational study. Lancet Glob. Health 2022, 10, e661–e672. [Google Scholar] [CrossRef]
- Lim, W.H.; Lien, R.; Huang, Y.C.; Chiang, M.C.; Fu, R.H.; Chu, S.M.; Hsu, J.F.; Yang, P.H. Prevalence and pathogen distribution of neonatal sepsis among very-low-birth-weight infants. Pediatr. Neonatol. 2012, 53, 228–234. [Google Scholar] [CrossRef]
- Freedman, R.M.; Ingram, D.L.; Gross, I.; Ehrenkranz, R.A.; Warshaw, J.B.; Baltimore, R.S. A half century of neonatal sepsis at Yale: 1928 to 1978. Am. J. Dis. Child. 1981, 135, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Miyairi, I.; Berlingieri, D.; Protic, J.; Belko, J. Neonatal invasive group A streptococcal disease: Case report and review of the literature. Pediatr. Infect. Dis. J. 2004, 23, 161–165. [Google Scholar] [CrossRef] [PubMed]
- WHO. The Current Evidence for the Burden of Group A Streptococcal Diseases; Discussion papers on Child Health; Department of Child and Adolescent Health and Development: Geneva, Switzerland, 2005; Available online: https://www.who.int/publications/i/item/WHO-FCH-CAH-05.07 (accessed on 5 July 2023).
- Sherwood, E.; Vergnano, S.; Kakuchi, I.; Bruce, M.G.; Chaurasia, S.; David, S.; Dramowski, A.; Georges, S.; Guy, R.; Lamagni, T.; et al. Invasive group A streptococcal disease in pregnant women and young children: A systematic review and meta-analysis. Lancet Infect. Dis. 2022, 22, 1076–1088. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, M.W. Pathogenesis of group A streptococcal infections. Clin. Microbiol. Rev. 2000, 13, 470–511. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.; Greenhouse, P.; Donders, F.; Engel, U.; Paavonen, J.; Mendling, W. Genital Tract GAS Infection ISIDOG Guidelines. J. Clin. Med. 2021, 10, 2043. [Google Scholar] [CrossRef] [PubMed]
- Rimawi, B.H.; Soper, D.E.; Eschenbach, D.A. Group A streptococcal infections in obstetrics and gynecology. Clin. Obstet. Gynecol. 2012, 55, 864–874. [Google Scholar] [CrossRef] [PubMed]
- Hariri, S.H.M.; Ibrahim, N.R.; Ramli, M.; Ismail, A.A.; Zin, A.A.M.; Hajissa, K.; Mohamed, Z. Group A Streptococcus puerperal sepsis with invasive neonatal infection: A fatal case. Med. J. Malays. 2021, 76, 731–733. [Google Scholar]
- Spaulding, A.B.; Watson, D.; Dreyfus, J.; Heaton, P.; Grapentine, S.; Bendel-Stenzel, E.; Kharbanda, A.B. Epidemiology of Bloodstream Infections in Hospitalized Children in the United States, 2009–2016. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2019, 69, 995–1002. [Google Scholar] [CrossRef]
- WHO. Disease Outbreak News; Increased Incidence of Scarlet Fever and Invasive Group A Streptococcus Infection—Multi-country. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON429 (accessed on 11 September 2023).
- CDC. Increase in Pediatric Invasive Group A Streptococcal Infections. Available online: https://emergency.cdc.gov/han/2022/han00484.asp (accessed on 1 September 2023).
- Lassoued, Y.; Assad, Z.; Ouldali, N.; Caseris, M.; Mariani, P.; Birgy, A.; Bonacorsi, S.; Bidet, P.; Faye, A. Unexpected Increase in Invasive Group A Streptococcal Infections in Children After Respiratory Viruses Outbreak in France: A 15-Year Time-Series Analysis. Open Forum Infect. Dis. 2023, 10, ofad188. [Google Scholar] [CrossRef]
- Cobo-Vázquez, E.; Aguilera-Alonso, D.; Carrasco-Colom, J.; Calvo, C.; Saavedra-Lozano, J. Increasing incidence and severity of invasive Group A streptococcal disease in Spanish children in 2019-2022. Lancet Reg. Health Eur. 2023, 27, 100597. [Google Scholar] [CrossRef]
- Ladhani, S.N.; Guy, R.; Bhopal, S.S.; Brown, C.S.; Lamagni, T.; Sharp, A. Paediatric group A streptococcal disease in England from October to December, 2022. Lancet Child Adolesc. Health 2023, 7, e2–e4. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Germont, Z.; Bidet, P.; Plainvert, C.; Bonacorsi, S.; Poyart, C.; Biran, V.; Frérot, A.; Faye, A.; Basmaci, R. Invasive Streptococcus pyogenes Infections in <3-Month-Old Infants in France: Clinical and Laboratory Features. Front. Pediatr. 2020, 8, 204. [Google Scholar] [CrossRef]
- Holden, R.; Wilmer, A.; Kollman, T. Primary peritonitis due to group A Streptococcus in a previously healthy pediatric patient. Can. J. Infect. Dis. Med. Microbiol. J. Can. Mal. Infect. Microbiol. Med. 2012, 23, e69–e70. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.X.; Dang, N.T.; Phan, H.T.; Pham, N.H.; Vu, H.A. Perforated Acute Appendicitis in a Six-Day-Old Neonate: A Rare Differential Diagnosis of Neonatal Peritonitis. Case Rep. Gastroenterol. 2021, 15, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Rangel, S.; Moss, R. Principles and Practice of Pediatric Infectious Diseases; Elsevier Health Sciences: Amsterdam, The Netherlands, 2009. [Google Scholar]
- Manalo, R.; Mirza, H.; Opal, S. Streptococcus pyogenes tuboovarian abscess: A potential sexually transmitted disease? Sex. Transm. Dis. 2002, 29, 606–607. [Google Scholar] [CrossRef] [PubMed]
- Gisser, J.M.; Fields, M.C.; Pick, N.; Moses, A.E.; Srugo, I. Invasive group a streptococcus associated with an intrauterine device and oral sex. Sex. Transm. Dis. 2002, 29, 483–485. [Google Scholar] [CrossRef] [PubMed]
- Gherardi, G.; Vitali, L.A.; Creti, R. Prevalent emm Types among Invasive GAS in Europe and North America since Year 2000. Front. Public Health 2018, 6, 59. [Google Scholar] [CrossRef]
- Stevens, D.L.; Tanner, M.H.; Winship, J.; Swarts, R.; Ries, K.M.; Schlievert, P.M.; Kaplan, E. Severe group A streptococcal infections associated with a toxic shock-like syndrome and scarlet fever toxin A. N. Engl. J. Med. 1989, 321, 1–7. [Google Scholar] [CrossRef]
- Moses, A.E.; Ziv, A.; Harari, M.; Rahav, G.; Shapiro, M.; Englehard, D. Increased incidence and severity of Streptococcus pyogenes bacteremia in young children. Pediatr. Infect. Dis. J. 1995, 14, 767–770. [Google Scholar] [CrossRef]
- WHO. WHO Recommendations for Prevention and Treatment of Maternal Peripartum Infections; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Lehtonén, O.P.J.; Kero, P.; Ruuskanen, O.; Gaworzewska, E.T.; Hollo, O.; Erkkola, R.; Salmi, T. A nursery outbreak of group A streptococcal infection. J. Infect. 1987, 14, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.R.; Arango, C.A.; Garcia-Prats, J.A.; Baker, C.J. An outbreak of M serotype 1 group A streptococcus in a neonatal intensive care unit. J. Pediatr. 1996, 129, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.F.; Rybak, A.; Werner, A.; Kochert, F.; Cahn-Sellem, F.; Gelbert, N.; Vié Le Sage, F.; Batard, C.; Béchet, S.; Corbaux, H.; et al. Surveillance of noninvasive group A Streptococcus infections in French ambulatory pediatrics before and during the COVID-19 pandemic: A prospective multicenter study from 2018–2022. Int. J. Infect. Dis. 2023, 134, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Harris, K.; Proctor, L.K.; Shinar, S.; Philippopoulos, E.; Yudin, M.H.; Murphy, K.E. Outcomes and management of pregnancy and puerperal group A streptococcal infections: A systematic review. Acta Obstet. Gynecol. Scand. 2023, 102, 138–157. [Google Scholar] [CrossRef] [PubMed]
- Kohli-Lynch, M.; Russell, N.J.; Seale, A.C.; Dangor, Z.; Tann, C.J.; Baker, C.J.; Bartlett, L.; Cutland, C.; Gravett, M.G.; Heath, P.T.; et al. Neurodevelopmental Impairment in Children After Group B Streptococcal Disease Worldwide: Systematic Review and Meta-analyses. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2017, 65, S190–S199. [Google Scholar] [CrossRef] [PubMed]
- Leonard, A.; Wright, A.; Saavedra-Campos, M.; Lamagni, T.; Cordery, R.; Nicholls, M.; Domoney, C.; Sriskandan, S.; Balasegaram, S. Severe group A streptococcal infections in mothers and their newborns in London and the South East, 2010–2016: Assessment of risk and audit of public health management. BJOG Int. J. Obstet. Gynaecol. 2019, 126, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.T.V.; Lau, S.Y.F.; Hui, S.Y.A.; Ma, T.; Kong, C.W.; Kwong, L.T.; Chan, D.; Lee, D.; Mok, S.L.; Ma, V.; et al. Incidence of neonatal sepsis after universal antenatal culture-based screening of group B streptococcus and intrapartum antibiotics: A multicentre retrospective cohort study. BJOG Int. J. Obstet. Gynaecol. 2023, 130, 24–31. [Google Scholar] [CrossRef]
- Rosa-Fraile, M.; Alós, J.I. Group B Streptococcus neonatal infections, the ongoing history. Enfermedades Infecc. Y Microbiol. Clin. (Engl. Ed.) 2022, 40, 349–352. [Google Scholar] [CrossRef]
- Chuan, I.; Van Beneden, C.; Beall, B.; Schuchat, A.; Active Bacterial Core Surveillance/Emerging Infections Program Network. Population-based surveillance for postpartum invasive group a streptococcus infections, 1995–2000. Clin. Infect. Dis. 2002, 35, 665–670. [Google Scholar] [CrossRef]
- Ventura, A.; Rúbio, C.; Rodrigues, D.; Silva, I.; Peres, A.; Cunha, F. Late-onset neonatal sepsis caused by group A Streptococcus—An unlikely agent. Nascer Crescer-Birth Growth Med. J. 2019, 28, 26–29. [Google Scholar] [CrossRef]
- Martic, J.; Mijac, V.; Jankovic, B.; Sekulovic, L.K.; Vasiljevic, Z.; Vuksanovic, J. Neonatal cellulitis and sepsis caused by group A streptococcus. Pediatr. Dermatol. 2010, 27, 528–530. [Google Scholar] [CrossRef] [PubMed]
- Mearkle, R.; Saavedra-Campos, M.; Lamagni, T.; Usdin, M.; Coelho, J.; Chalker, V.; Sriskandan, S.; Cordery, R.; Rawlings, C.; Balasegaram, S. Household transmission of invasive group A Streptococcus infections in England: A population-based study, 2009, 2011 to 2013. Euro Surveill. Bull. Eur. Mal. Transm. Eur. Commun. Dis. Bull. 2017, 22, 30532. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, A.; Bielicki, J.; Mathur, S.; Sharland, M.; Van Den Anker, J.N. Reviewing the WHO guidelines for antibiotic use for sepsis in neonates and children. Paediatr. Int. Child Health 2018, 38, S3–S15. [Google Scholar] [CrossRef] [PubMed]
- Downie, L.; Armiento, R.; Subhi, R.; Kelly, J.; Clifford, V.; Duke, T. Community-acquired neonatal and infant sepsis in developing countries: Efficacy of WHO’s currently recommended antibiotics--systematic review and meta-analysis. Arch. Dis. Child. 2013, 98, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Karaky, N.M.; Araj, G.F.; Tokajian, S.T. Molecular characterization of Streptococcus pyogenes group A isolates from a tertiary hospital in Lebanon. J. Med. Microbiol. 2014, 63, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Seale, A.C.; Davies, M.R.; Anampiu, K.; Morpeth, S.C.; Nyongesa, S.; Mwarumba, S.; Smeesters, P.R.; Efstratiou, A.; Karugutu, R.; Mturi, N.; et al. Invasive Group A Streptococcus Infection among Children, Rural Kenya. Emerg. Infect. Dis. 2016, 22, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Kaur, J.; Singhi, P.; Singhi, S.; Malhi, P.; Saini, A.G. Neurodevelopmental and Behavioral Outcomes in Children with Sepsis-Associated Encephalopathy Admitted to Pediatric Intensive Care Unit: A Prospective Case Control Study. J. Child Neurol. 2016, 31, 683–690. [Google Scholar] [CrossRef]
- Ching, N.S.; Crawford, N.; McMinn, A.; Baker, C.; Azzopardi, K.; Brownlee, K.; Lee, D.; Gibson, M.; Smeesters, P.; Gonis, G.; et al. Prospective Surveillance of Pediatric Invasive Group A Streptococcus Infection. J. Pediatr. Infect. Dis. Soc. 2019, 8, 46–52. [Google Scholar] [CrossRef]
- Reeves, B.C.; Deeks, J.J.; Higgins, J.P.; Shea, B.; Tugwell, P.; Wells, G.A.; on behalf of the Cochrane Non-Randomized Studies of Interventions Methods Group. Including Non-Randomized Studies on Intervention Effects. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2019; pp. 595–620. [Google Scholar]
- Loke, Y.K.; Price, D.; Herxheimer, A. Systematic reviews of adverse effects: Framework for a structured approach. BMC Med. Res. Methodol. 2007, 7, 32. [Google Scholar] [CrossRef]
- Nambiema, A.; Sembajwe, G.; Lam, J.; Woodruff, T.; Mandrioli, D.; Chartres, N.; Fadel, M.; Le Guillou, A.; Valter, R.; Deguigne, M.; et al. A Protocol for the Use of Case Reports/Studies and Case Series in Systematic Reviews for Clinical Toxicology. Front. Med. 2021, 8, 708380. [Google Scholar] [CrossRef]
- Middleton, B.; Morris, P.; Carapetis, J. Invasive group A streptococcal infection in the Northern Territory, Australia: Case report and review of the literature. J. Paediatr. Child Health 2014, 50, 869–873. [Google Scholar] [CrossRef]
- Crum, N.F.; Chun, H.M.; Gaylord, T.G.; Hale, B.R. Group A streptococcal toxic shock syndrome developing in the third trimester of pregnancy. Infect. Dis. Obstet. Gynecol. 2002, 10, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Mahieu, L.M.; Holm, S.E.; Goossens, H.J.; Van Acker, K.J. Congenital streptococcal toxic shock syndrome with absence of antibodies against streptococcal pyrogenic exotoxins. J. Pediatr. 1995, 127, 987–989. [Google Scholar] [CrossRef] [PubMed]
- Nieburg, P.I.; Williams, M.L. Group A beta hemolytic streptococcal sepsis in mother and infant twins. J. Pediatr. 1975, 87, 453. [Google Scholar] [CrossRef] [PubMed]
- Lequier, L.; Vaudry, W.L. Puerperal fever and neonatal pleural empyema and bacteremia caused by group A streptococcus. Can. J. Infect. Dis. J. Can. Des Mal. Infect. 1998, 9, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Shinoda, Y.; Hori, T.; Sasai, H.; Ikebe, T.; Ohnishi, H. Neonatal bacteremia caused by emm type 80 group A Streptococcus: A case report. Pediatr. Int. Off. J. Jpn. Pediatr. Soc. 2020, 62, 1305–1306. [Google Scholar] [CrossRef] [PubMed]
- Verboon-Maciolek, M.A.; Krediet, T.G.; van Ertbruggen, I.; Gerards, L.J.; Fleer, A. Severe neonatal group A streptococcal disease. Eur. J. Pediatr. 2000, 159, 450–452. [Google Scholar] [CrossRef] [PubMed]
- Nohara, F.; Nagaya, K.; Asai, H.; Tsuchida, E.; Okamoto, T.; Hayashi, T.; Sakata, H.; Terao, Y.; Azuma, H. Neonatal pleural empyema caused by emm type 6 group A streptococcus. Pediatr. Int. Off. J. Jpn. Pediatr. Soc. 2013, 55, 519–521. [Google Scholar] [CrossRef]
- Nutman, J.; Henig, E.; Wilunsky, E.; Reisner, S.H. Acute necrotising fasciitis due to streptococcal infection in a newborn infant. Arch. Dis. Child. 1979, 54, 637–639. [Google Scholar] [CrossRef]
- Thaarup, J.; Ellermann-Eriksen, S.; Stjernholm, J. Neonatal pleural empyema with group A Streptococcus. Acta Pædiatrica 1997, 86, 769–771. [Google Scholar] [CrossRef]
- Ross, L.; Tong, J. Concurrent neonatal and maternal sepsis due to invasive group A Streptococcus infection within 48 hours of birth. J. Paediatr. Child Health 2021, 57, 1698–1700. [Google Scholar] [CrossRef] [PubMed]
- Sakata, H. Susceptibility and emm type of Streptococcus pyogenes isolated from children with severe infection. J. Infect. Chemother. Off. J. Jpn. Soc. Chemother. 2013, 19, 1042–1046. [Google Scholar] [CrossRef] [PubMed]
- Sakata, H. Pediatric invasive streptococcal infection in northern and eastern regions of Hokkaido, Japan from 2010 to 2012. Pediatr. Int. Off. J. Jpn. Pediatr. Soc. 2014, 56, 360–363. [Google Scholar] [CrossRef] [PubMed]
- Timmis, A.; Parkins, K.; Kustos, I.; Riordan, F.A.; Efstratiou, A.; Carrol, E.D. Invasive group A streptococcal infections in children presenting to a paediatric intensive care unit in the North West of England. J. Infect. 2010, 60, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Barnham, M.R.; Weightman, N.C. Bacteraemic Streptococcus pyogenes infection in the peri-partum period: Now a rare disease and prior carriage by the patient may be important. J. Infect. 2001, 43, 173–176. [Google Scholar] [CrossRef]
- Saito, R.; Kerr-Liddell, R.; Paul, S.P. Late onset neonatal sepsis caused by group A streptococcus. Br. J. Hosp. Med. 2017, 78, 170–171. [Google Scholar] [CrossRef] [PubMed]
- Huber, B.M. Cellulitis-adenitis in a neonate with group a streptococcal sepsis. Klin. Padiatr. 2014, 226, 82–83. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Naqvi, S.H. Neonatal group A streptococcal septicemia. Pediatr. Infect. Dis. J. 1990, 9, 528–529. [Google Scholar] [CrossRef]
- Wilschanski, M.; Faber, J.; Abramov, A.; Isacsohn, M.; Erlichman, M. Neonatal septicemia caused by group A beta-hemolytic Streptococcus. Pediatr. Infect. Dis. J. 1989, 8, 536–537. [Google Scholar] [CrossRef]
- Cartwright, R.Y. Neonatal septicaemia due to group A beta-haemolytic streptococcus. Br. Med. J. 1977, 1, 146–147. [Google Scholar] [CrossRef]
- Barnham, M. Invasive streptococcal infections in the era before the acquired immune deficiency syndrome: A 10 years’ compilation of patients with streptococcal bacteraemia in North Yorkshire. J. Infect. 1989, 18, 231–248. [Google Scholar] [CrossRef] [PubMed]
- Umadevi, S.; Kali, A.; Sreenivasan, S.; Pramodhini, S.; Charles, M.V. Septic Arthritis caused by Group A Streptococcus in Newborn: An Unusual Presentation. J. Clin. Diagn. Res. 2013, 7, 1143–1144. [Google Scholar] [CrossRef] [PubMed]
- Coulter, J.B.; Buchannon, C.R.; Vellodi, A.; Hart, C.A.; Sills, J.A. Group-A streptococcal infection in the newborn. Lancet 1984, 2, 355–356. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.S.; Ribeiro, G.S.; Oliveira, T.Q.; Santos, R.C.; Gouveia, E.; Salgado, K.; Takahashi, D.; Fontes, C.; Campos, L.C.; Reis, M.G.; et al. Burden of group A streptococcal meningitis in Salvador, Brazil: Report of 11 years of population-based surveillance. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2009, 13, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Shanks, G.D.; Anderson, R.T.; Lazoritz, S.; Hemming, V.G. Bilateral neonatal group A streptococcal hydrocele infection associated with maternal puerperal sepsis. Pediatr. Infect. Dis. 1986, 5, 107–108. [Google Scholar] [CrossRef] [PubMed]
- Torres-Martínez, C.; Mehta, D.; Butt, A.; Levin, M. Streptococcus associated toxic shock. Arch. Dis. Child. 1992, 67, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Givner, L.B.; Abramson, J.S.; Wasilauskas, B. Apparent increase in the incidence of invasive group A beta-hemolytic streptococcal disease in children. J. Pediatr. 1991, 118, 341–346. [Google Scholar] [CrossRef]
- Johnson, M.P.; Rand, K.H. Group A beta-hemolytic streptococcal bacteremia and HIV infection. South. Med. J. 1990, 83, 146–149. [Google Scholar] [CrossRef]
- Davey, C.; Moore, A.M. Necrotizing fasciitis of the scalp in a newborn. Obstet. Gynecol. 2006, 107, 461–463. [Google Scholar] [CrossRef]
- Pius, S.; Bello, M.; Galadima, G.B.; Ibrahim, H.A.; Yerima, S.T.; Ambe, J.P. Neonatal septicaemia, bacterial isolates and antibiogram sensitivity in Maiduguri North-Eastern Nigeria. Niger. Postgrad. Med. J. 2016, 23, 146–151. [Google Scholar] [CrossRef]
- Wheeler, M.C.; Roe, M.H.; Kaplan, E.L.; Schlievert, P.M.; Todd, J.K. Outbreak of group A streptococcus septicemia in children. Clinical, epidemiologic, and microbiological correlates. JAMA 1991, 266, 533–537. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Reported Data | Missing Data | ||
|---|---|---|---|
| Gestational age (weeks) | Preterm | 30/43 (69.8) | 151/194 (77.8) |
| Term | 13/43 (30.2) | ||
| Gender | Male | 35/59 (59.3) | 135/194 (69.6) |
| Female | 24/59 (40.7) | ||
| Delivery mode | Vaginal | 17/26 (65.4) | 168/194 (86.6) |
| Cesarean section | 9/26 (34.6) |
| EOS | LOS | |
|---|---|---|
| Respiratory distress | 12/20 (60) | 7/49 (14.2) |
| Fever | 6/20 (30) | 15/49 (30.6) |
| Rash | 6/19 (30) | 23/49 (46.9) |
| Gastrointestinal disturbances | 4/20 (20) | 22/49 (44.9) |
| All Cases (n = 194) | EOS (n = 20) | LOS (n = 49) | |
|---|---|---|---|
| Meningitis | 10 | - | 5 |
| Pneumonia (empyema) | 5 (4) | 5 (3) | - |
| Omphalitis | 18 | - | - |
| Peritonitis | 9 | - | 8 |
| Skin lesions | 5 | - | 1 |
| Osteomyelitis/arthritis | 2 | - | 2 |
| TSS | 5 | 4 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sokou, R.; Filippatos, F.; Daniil, V.; Bikouli, E.-D.; Tsantes, A.G.; Piovani, D.; Bonovas, S.; Iliodromiti, Z.; Boutsikou, T.; Tsantes, A.E.; et al. Group A Streptococcus Infection in Neonatal Population: A Systematic Review of The Literature. J. Clin. Med. 2023, 12, 6974. https://doi.org/10.3390/jcm12226974
Sokou R, Filippatos F, Daniil V, Bikouli E-D, Tsantes AG, Piovani D, Bonovas S, Iliodromiti Z, Boutsikou T, Tsantes AE, et al. Group A Streptococcus Infection in Neonatal Population: A Systematic Review of The Literature. Journal of Clinical Medicine. 2023; 12(22):6974. https://doi.org/10.3390/jcm12226974
Chicago/Turabian StyleSokou, Rozeta, Filippos Filippatos, Vasiliki Daniil, Efstathia-Danai Bikouli, Andreas G. Tsantes, Daniele Piovani, Stefanos Bonovas, Zoi Iliodromiti, Theodora Boutsikou, Argirios E. Tsantes, and et al. 2023. "Group A Streptococcus Infection in Neonatal Population: A Systematic Review of The Literature" Journal of Clinical Medicine 12, no. 22: 6974. https://doi.org/10.3390/jcm12226974