
The Potential Benefic Effect of Nicotinamide Riboside in Treating a Murine Model of Monoiodoacetate-Induced Knee Osteoarthritis
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Study Design
2.3. Induction of Osteoarthritis
2.4. Blood Sampling
2.4.1. Cytokine Assessment
2.4.2. Assessment of Oxidative and Nitrosative Stress Biomarkers
2.5. Histopathological Analysis
2.6. Statistical Analysis
3. Results
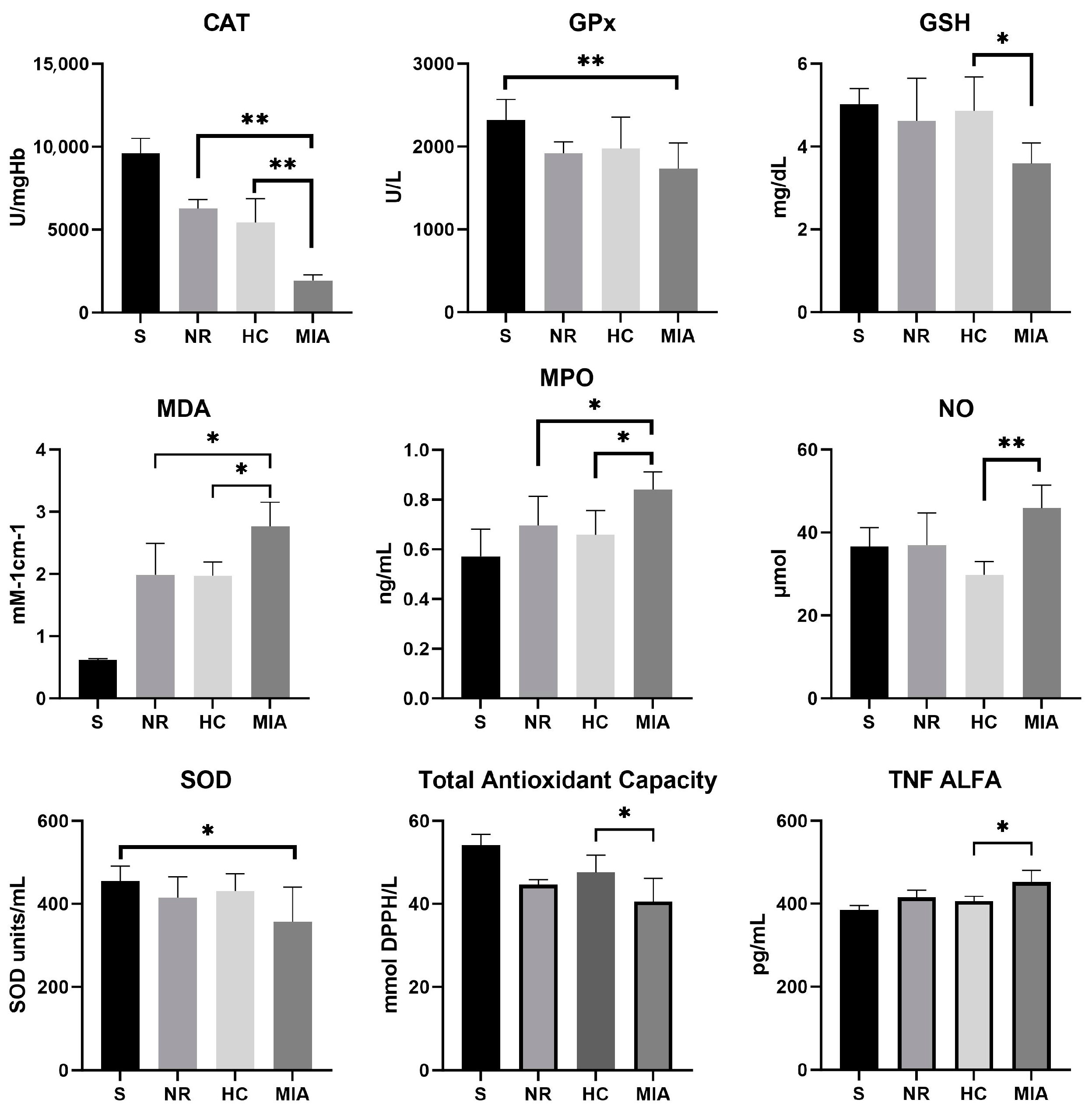
3.1. Cytokine and Oxidative and Nitrosative Stress Biomarkers
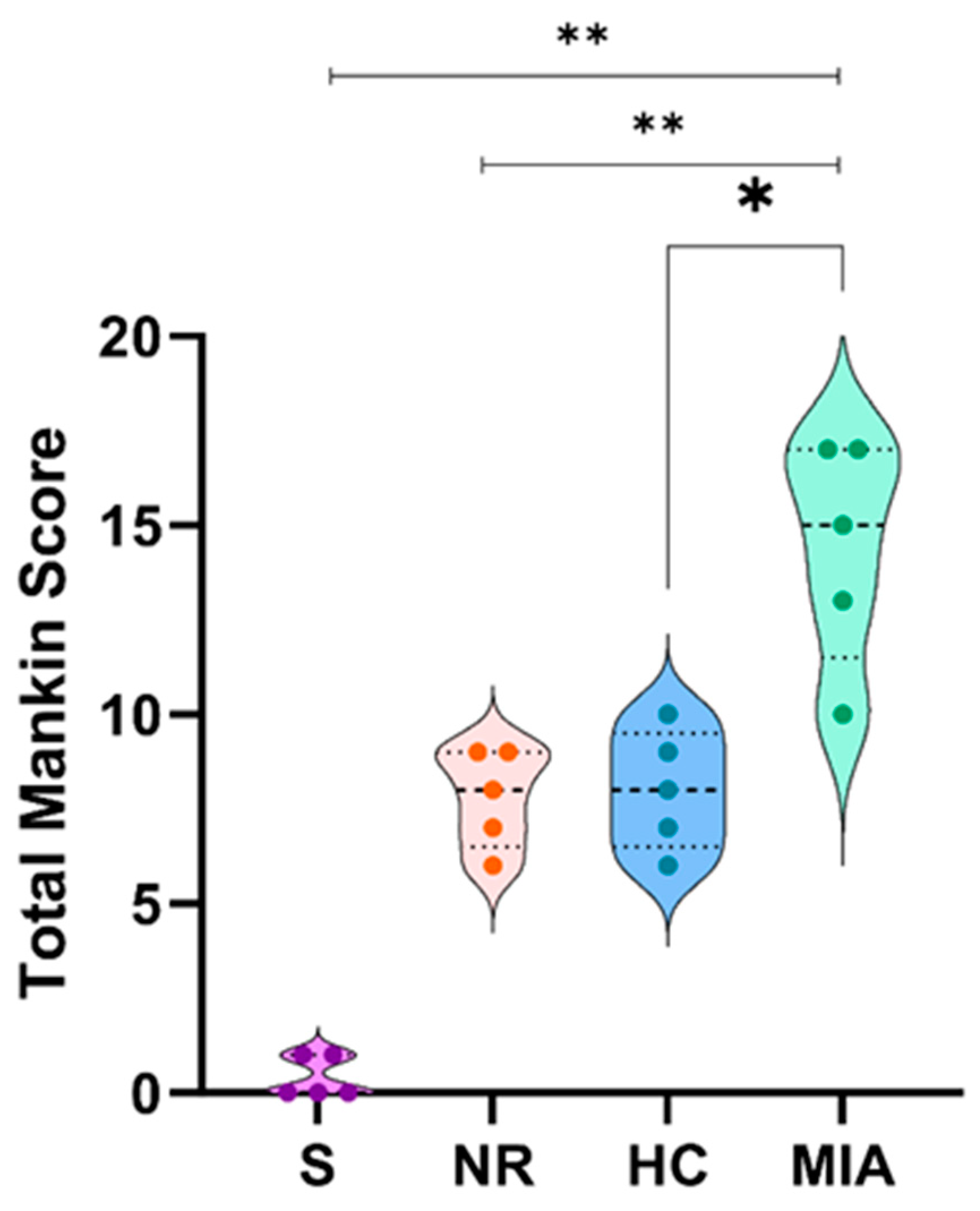
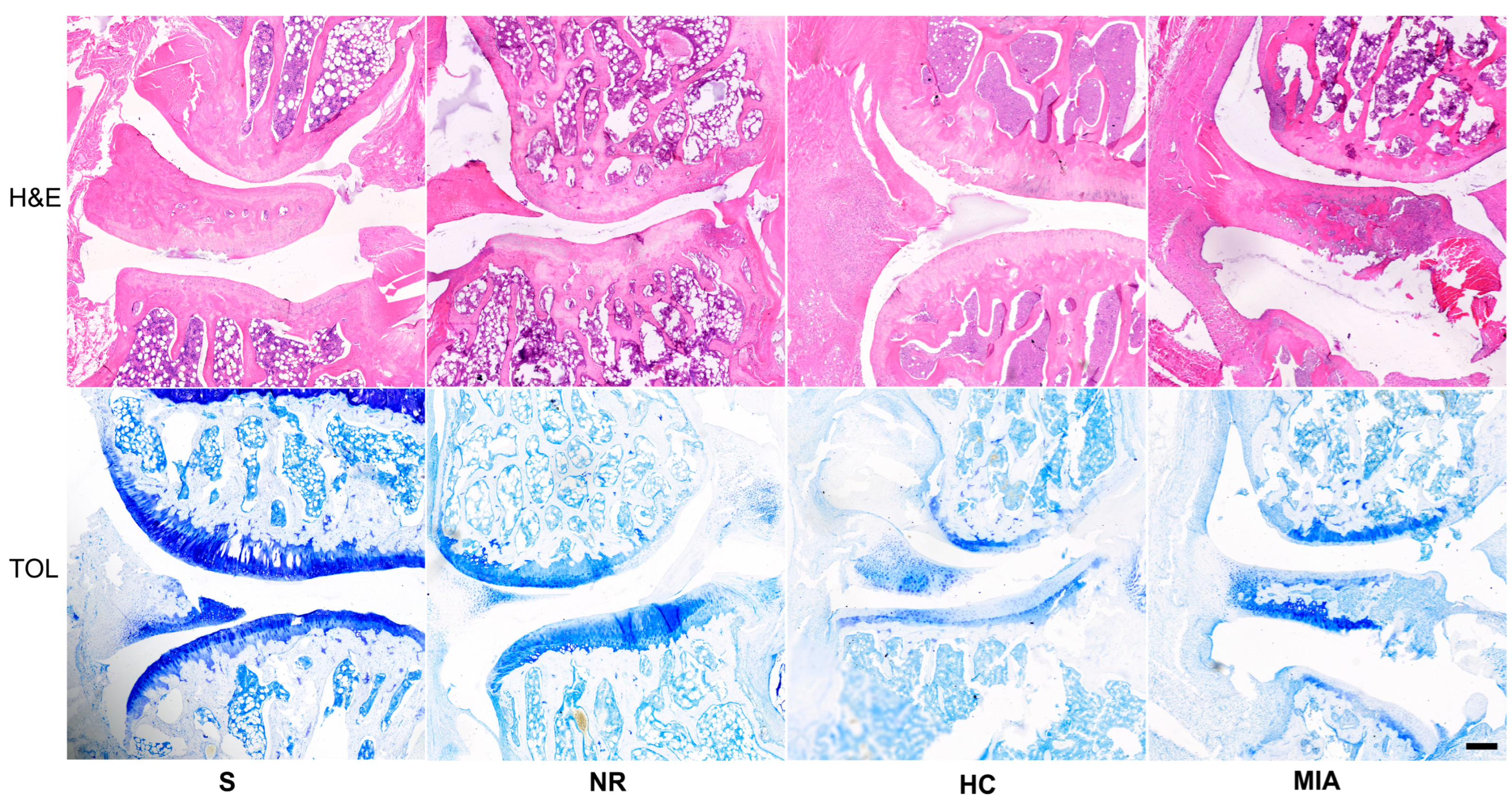
3.2. Histolopathological Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mallio, C.A.; Bernetti, C.; Agostini, F.; Mangone, M.; Paoloni, M.; Santilli, G.; Martina, F.M.; Quattrocchi, C.C.; Zobel, B.B.; Bernetti, A. Advanced MR Imaging for Knee Osteoarthritis: A Review on Local and Brain Effects. Diagnostics 2023, 13, 54. [Google Scholar] [CrossRef] [PubMed]
- Litwic, A.; Edwards, M.H.; Dennison, E.M.; Cooper, C. Epidemiology and Burden of Osteoarthritis. Br. Med. Bull. 2013, 105, 185–199. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, T.W.; Felson, D.T. Mechanisms of Osteoarthritis (OA) Pain. Curr. Osteoporos. Rep. 2018, 16, 611–616. [Google Scholar] [CrossRef] [PubMed]
- Michael, J.W.P.; Schlüter-Brust, K.U.; Eysel, P. Epidemiologie, Ätiologie, Diagnostik Und Therapie Der Gonarthrose. Dtsch. Arztebl. 2010, 107, 152–162. [Google Scholar]
- Lei, Y.; Zhang, Q.; Kuang, G.; Wang, X.; Fan, Q.; Ye, F. Functional Biomaterials for Osteoarthritis Treatment: From Research to Application. Smart Med. 2022, 1, e20220014. [Google Scholar] [CrossRef]
- Vincent, T.L.; Alliston, T.; Kapoor, M.; Loeser, R.F.; Troeberg, L.; Little, C.B. Osteoarthritis Pathophysiology: Therapeutic Target Discovery May Require a Multifaceted Approach. Clin. Geriatr. Med. 2022, 38, 193–219. [Google Scholar] [CrossRef]
- Dainese, P.; Wyngaert, K.V.; De Mits, S.; Wittoek, R.; Van Ginckel, A.; Calders, P. Association between Knee Inflammation and Knee Pain in Patients with Knee Osteoarthritis: A Systematic Review. Osteoarthr. Cartil. 2022, 30, 516–534. [Google Scholar] [CrossRef]
- Ansari, M.Y.; Ahmad, N.; Haqqi, T.M. Oxidative Stress and Inflammation in Osteoarthritis Pathogenesis: Role of Polyphenols. Biomed. Pharmacother. 2020, 129, 110452. [Google Scholar] [CrossRef]
- Tsokanos, A.; Livieratou, E.; Billis, E.; Tsekoura, M.; Tatsios, P.; Tsepis, E.; Fousekis, K. The Efficacy of Manual Therapy in Patients with Knee Osteoarthritis: A Systematic Review. Medicina 2021, 57, 696. [Google Scholar] [CrossRef]
- Kan, H.S.; Chan, P.K.; Chiu, K.Y.; Yan, C.H.; Yeung, S.S.; Ng, Y.L.; Shiu, K.W.; Ho, T. Non-Surgical Treatment of Knee Osteoarthritis. Hong Kong Med. J. 2019, 25, 127–133. [Google Scholar] [CrossRef]
- Primorac, D.; Molnar, V.; Matiši, V.; Hudetz, D.; Jeleč, Ž.; Rod, E.; Cukelj, F.; Vidovi, D.; Vrdoljak, T.; Dobriči, B.; et al. Comprehensive Review of Knee Osteoarthritis Pharmacological Treatment and the Latest Professional Societies’ Guidelines. Pharmaceuticals 2021, 14, 205. [Google Scholar] [CrossRef] [PubMed]
- Printz, J.O.; Lee, J.J.; Knesek, M.; Urquhart, A.G. Conflict of Interest in the Assessment of Hyaluronic Acid Injections for Osteoarthritis of the Knee: An Updated Systematic Review. J. Arthroplast. 2013, 28, 30–33.e1. [Google Scholar] [CrossRef] [PubMed]
- Peng, K.T.; Chiang, Y.C.; Huang, T.Y.; Chen, P.C.; Chang, P.J.; Lee, C.W. Curcumin Nanoparticles Are a Promising Anti-Bacterial and Anti-Inflammatory Agent for Treating Periprosthetic Joint Infections. Int. J. Nanomed. 2019, 14, 469–481. [Google Scholar] [CrossRef] [PubMed]
- Colletti, A.; Cicero, A.F.G. Nutraceutical Approach to Chronic Osteoarthritis: From Molecular Research to Clinical Evidence. Int. J. Mol. Sci. 2021, 22, 12920. [Google Scholar] [CrossRef]
- Campos, L.D.; Santos, V.D.A., Jr.; Pimentel, J.D.; Carregã, G.L.F.; Cazarin, C.B.B. Collagen Supplementation in Skin and Orthopedic Diseases: A Review of the Literature. Heliyon 2023, 9, e14961. [Google Scholar] [CrossRef]
- Elhassan, Y.S.; Kluckova, K.; Fletcher, R.S.; Schmidt, M.S.; Garten, A.; Doig, C.L.; Cartwright, D.M.; Oakey, L.; Burley, C.V.; Jenkinson, N.; et al. Nicotinamide Riboside Augments the Aged Human Skeletal Muscle NAD+ Metabolome and Induces Transcriptomic and Anti-Inflammatory Signatures. Cell Rep. 2019, 28, 1717–1728.e6. [Google Scholar] [CrossRef]
- Mehmel, M.; Jovanović, N.; Spitz, U. Nicotinamide Riboside—The Current State of Research and Therapeutic Uses. Nutrients 2020, 12, 1616. [Google Scholar] [CrossRef]
- Oh, H.; Kwak, J.S.; Yang, S.; Gong, M.K.; Kim, J.H.; Rhee, J.; Kim, S.K.; Kim, H.E.; Ryu, J.H.; Chun, J.S. Reciprocal Regulation by Hypoxia-Inducible Factor-2α and the NAMPT-NAD+-SIRT Axis in Articular Chondrocytes Is Involved in Osteoarthritis. Osteoarthr. Cartil. 2015, 23, 2288–2296. [Google Scholar] [CrossRef]
- Yoon, H.; Park, S.G.; Kim, H.J.; Shin, H.R.; Kim, K.T.; Cho, Y.D.; Moon, J.I.; Park, M.S.; Kim, W.J.; Ryoo, H.M. Nicotinamide Enhances Osteoblast Differentiation through Activation of the Mitochondrial Antioxidant Defense System. Exp. Mol. Med. 2023, 55, 1531–1543. [Google Scholar] [CrossRef]
- Docea, A.O.; Calina, D.; Buga, A.M.; Zlatian, O.; Paoliello, M.M.B.; Mogosanu, G.D.; Streba, C.T.; Popescu, E.L.; Stoica, A.E.; Bîrcă, A.C.; et al. The Effect of Silver Nanoparticles on Antioxidant/pro-Oxidant Balance in a Murine Model. Int. J. Mol. Sci. 2020, 21, 1233. [Google Scholar] [CrossRef]
- Meca, A.D.; Turcu-Stiolica, A.; Stanciulescu, E.C.; Andrei, A.M.; Nitu, F.M.; Banita, I.M.; Matei, M.; Pisoschi, C.G. Variations of Serum Oxidative Stress Biomarkers under First-Line Antituberculosis Treatment: A Pilot Study. J. Pers. Med. 2021, 11, 112. [Google Scholar] [CrossRef] [PubMed]
- Gerwin, N.; Bendele, A.M.; Glasson, S.; Carlson, C.S. The OARSI Histopathology Initiative—Recommendations for Histological Assessments of Osteoarthritis in the Rat. Osteoarthr. Cartil. 2010, 18, S24–S34. [Google Scholar] [CrossRef] [PubMed]
- Kraus, V.B.; Huebner, J.L.; DeGroot, J.; Bendele, A. The OARSI Histopathology Initiative—Recommendations for Histological Assessments of Osteoarthritis in the Guinea Pig. Osteoarthr. Cartil. 2010, 18, S35–S52. [Google Scholar] [CrossRef]
- Pitcher, T.; Sousa-Valente, J.; Malcangio, M. The Monoiodoacetate Model of Osteoarthritis Pain in the Mouse. J. Vis. Exp. 2016, 2016, e53746. [Google Scholar] [CrossRef]
- De Sousa Valente, J. The Pharmacology of Pain Associated with the Monoiodoacetate Model of Osteoarthritis. Front. Pharmacol. 2019, 10, 974. [Google Scholar] [CrossRef] [PubMed]
- Ashford, S.; Williard, J. Osteoarthritis: A review. Nurse Pract. 2014, 39, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nedunchezhiyan, U.; Varughese, I.; Sun, A.R.J.; Wu, X.; Crawford, R.; Prasadam, I. Obesity, Inflammation, and Immune System in Osteoarthritis. Front. Immunol. 2022, 13, 907750. [Google Scholar] [CrossRef]
- Lepetsos, P.; Papavassiliou, A.G. ROS/Oxidative Stress Signaling in Osteoarthritis. Biochim. Biophys. Acta Mol. Basis Dis. 2016, 1862, 576–591. [Google Scholar] [CrossRef]
- Li, D.; Xie, G.; Wang, W. Reactive Oxygen Species: The 2-Edged Sword of Osteoarthritis. Am. J. Med. Sci. 2012, 344, 486–490. [Google Scholar] [CrossRef]
- Galasso, M.; Gambino, S.; Romanelli, M.G.; Donadelli, M.; Scupoli, M.T. Browsing the Oldest Antioxidant Enzyme: Catalase and Its Multiple Regulation in Cancer. Free Radic. Biol. Med. 2021, 172, 264–272. [Google Scholar] [CrossRef]
- Zhou, B.; Zhao, G.; Zhu, Y.; Chen, X.; Zhang, N.; Yang, J.; Lin, H. Protective Effects of Nicotinamide Riboside on H2O2-Induced Oxidative Damage in Lens Epithelial Cells. Curr. Eye Res. 2021, 46, 961–970. [Google Scholar] [CrossRef] [PubMed]
- de Castro, J.M.; Assumpção, J.A.F.; Stein, D.J.; Toledo, R.S.; da Silva, L.S.; Caumo, W.; Carraro, C.C.; da Rosa Araujo, A.S.; Torres, I.L.S. Nicotinamide Riboside Reduces Cardiometabolic Risk Factors and Modulates Cardiac Oxidative Stress in Obese Wistar Rats under Caloric Restriction. Life Sci. 2020, 263, 118596. [Google Scholar] [CrossRef]
- Tudorachi, N.B.; Totu, E.E.; Fifere, A.; Ardeleanu, V.; Mocanu, V.; Mircea, C.; Isildak, I.; Smilkov, K.; Cărăuşu, E.M. The Implication of Reactive Oxygen Species and Antioxidants in Knee Osteoarthritis. Antioxidants 2021, 10, 985. [Google Scholar] [CrossRef] [PubMed]
- Gheita, T.A.; Kenawy, S.A. Measurement of Malondialdehyde, Glutathione, and Glutathione Peroxidase in SLE Patients. Methods Mol. Biol. 2014, 1134, 193–199. [Google Scholar] [CrossRef]
- Li, J.; Li, Y.; Li, Y.; Yang, Z.; Jin, H. Physicochemical Properties of Collagen from Acaudina Molpadioides and Its Protective Effects against H2O2-Induced Injury in RAW264.7 Cells. Mar. Drugs 2020, 18, 370. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Alsahli, M.A.; Rahmani, A.H. Myeloperoxidase as an Active Disease Biomarker: Recent Biochemical and Pathological Perspectives. Med. Sci. 2018, 6, 33. [Google Scholar] [CrossRef]
- Jiang, H.; Ji, P.; Shang, X.; Zhou, Y. Connection between Osteoarthritis and Nitric Oxide: From Pathophysiology to Therapeutic Target. Molecules 2023, 28, 1683. [Google Scholar] [CrossRef]
- Carames, B.; López-Armada, M.; Cillero-Pastor, B.; Lires-Dean, M.; Vaamonde-García, C.; Galdo, F.; Blanco, F. Differential effects of tumor necrosis factor-α and interleukin-1β on cell death in human articular chondrocytes. Osteoarthr. Cartil. 2008, 16, 715–722. [Google Scholar] [CrossRef]
- Hamza, R.Z.; Al-Salmi, F.A.; El-Shenawy, N.S. Chitosan and Lecithin Ameliorate Osteoarthritis Symptoms Induced by Monoiodoacetate in a Rat Model. Molecules. 2020, 25, 5738. [Google Scholar] [CrossRef]
- Nikniaz, Z.; Mahdavi, R.; Ostadrahimi, A.; Ebrahimi, A.; Nikniaz, L.; Vatankhah, A. Effects of Elaeagnus Angustifolia L. Powder Supplementation on Serum Total Antioxidant Capacity and Malondialdehyde Levels in Females with Knee Osteoarthritis. J. Herb. Med. 2015, 5, 177–183. [Google Scholar] [CrossRef]
- Abdel Jaleel, G.A.; Saleh, D.O.; Al-Awdan, S.W.; Hassan, A.; Asaad, G.F. Impact of Type III Collagen on Monosodium Iodoacetate-Induced Osteoarthritis in Rats. Heliyon 2020, 6, e04083. [Google Scholar] [CrossRef] [PubMed]
- Biţă, A.; Scorei, I.R.; Ciocîlteu, M.V.; Nicolaescu, O.E.; Pîrvu, A.S.; Bejenaru, L.E.; Rău, G.; Bejenaru, C.; Radu, A.; Neamţu, J.; et al. Nicotinamide Riboside, a Promising Vitamin B3 Derivative for Healthy Aging and Longevity: Current Research and Perspectives. Molecules 2023, 28, 6078. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, F.M.; Angelinetta, C.; Rizzi, G.; Praticò, A.; Villa, R. Evaluation of the Efficacy of a Hydrolyzed Collagen Supplement for Improving Skin Moisturization, Smoothness, and Wrinkles. J. Clin. Aesthet. Dermatol. 2022, 15, 48–52. [Google Scholar]
- Conze, D.B.; Crespo-Barreto, J.; Kruger, C.L. Safety Assessment of Nicotinamide Riboside, a Form of Vitamin B3. Hum. Exp. Toxicol. 2016, 35, 1149–1160. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| S | NR | HC | MIA | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | S.D. | Mean | S.D. | Mean | S.D. | Mean | S.D. | |
| CAT [U/mg Hb] | 9618.00 | 888.40 | 6286.00 | 536.30 | 5425.00 | 1445.00 | 1940.00 | 333.50 |
| GPx [U/L] | 2319.00 | 250.50 | 1922.00 | 134.30 | 1975.00 | 377.70 | 1736.00 | 307.00 |
| GSH [mg/dL] | 5.02 | 0.38 | 4.62 | 1.02 | 4.86 | 0.81 | 3.59 | 0.50 |
| MDA [mM−1cm−1] | 0.62 | 0.02 | 1.98 | 0.51 | 1.97 | 0.22 | 2.76 | 0.39 |
| MPO [ng/mL] | 0.57 | 0.11 | 0.70 | 0.12 | 0.66 | 0.10 | 0.84 | 0.07 |
| NO [μmol] | 36.64 | 4.54 | 36.96 | 7.76 | 29.76 | 3.29 | 45.92 | 5.57 |
| SOD [units/mL] | 454.50 | 36.36 | 414.60 | 50.92 | 430.60 | 41.71 | 356.60 | 84.21 |
| TAC [mmol DPPH/L] | 54.18 | 2.06 | 44.66 | 0.99 | 47.60 | 3.37 | 40.50 | 4.58 |
| TNF Alfa [pg/mL] | 385.20 | 10.26 | 414.80 | 17.58 | 406.80 | 11.10 | 452.20 | 28.52 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gherghina, F.-L.; Mîndrilă, I.; Buteică, S.-A.; Bică, G.; Pisoschi, C.-G.; Biță, C.-E.; Paliu, I.-A.; Rogoveanu, O.-C. The Potential Benefic Effect of Nicotinamide Riboside in Treating a Murine Model of Monoiodoacetate-Induced Knee Osteoarthritis. J. Clin. Med. 2023, 12, 6920. https://doi.org/10.3390/jcm12216920
Gherghina F-L, Mîndrilă I, Buteică S-A, Bică G, Pisoschi C-G, Biță C-E, Paliu I-A, Rogoveanu O-C. The Potential Benefic Effect of Nicotinamide Riboside in Treating a Murine Model of Monoiodoacetate-Induced Knee Osteoarthritis. Journal of Clinical Medicine. 2023; 12(21):6920. https://doi.org/10.3390/jcm12216920
Chicago/Turabian StyleGherghina, Florin-Liviu, Ion Mîndrilă, Sandra-Alice Buteică, George Bică, Cătălina-Gabriela Pisoschi, Cristina-Elena Biță, Iulia-Alexandra Paliu, and Otilia-Constantina Rogoveanu. 2023. "The Potential Benefic Effect of Nicotinamide Riboside in Treating a Murine Model of Monoiodoacetate-Induced Knee Osteoarthritis" Journal of Clinical Medicine 12, no. 21: 6920. https://doi.org/10.3390/jcm12216920