
Current Role of SLGT2 Inhibitors in the Management of the Whole Spectrum of Heart Failure: Focus on Dapagliflozin
 , , , and
, , , and 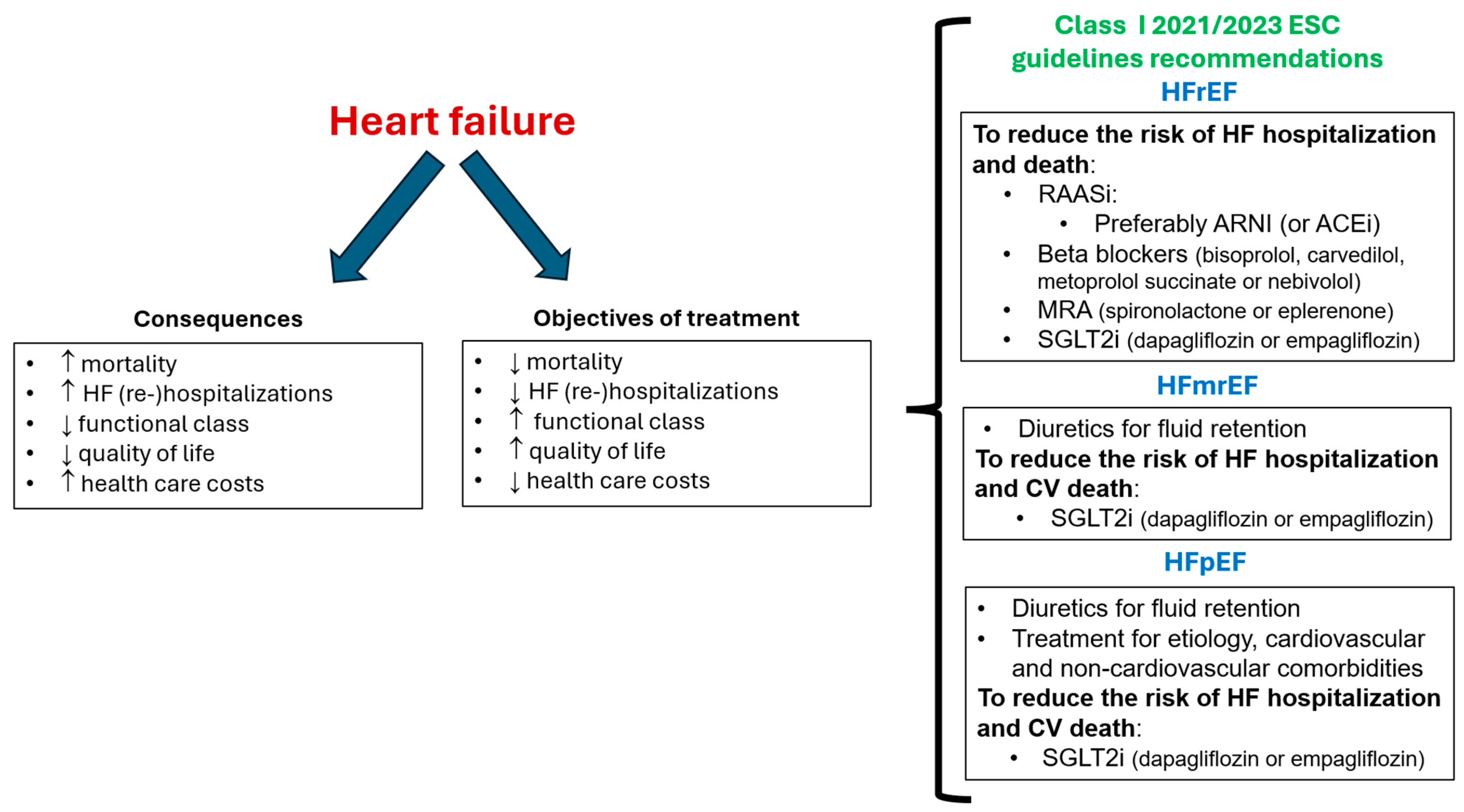{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Dapagliflozin: Beyond HF Protection
3. Dapagliflozin and HF
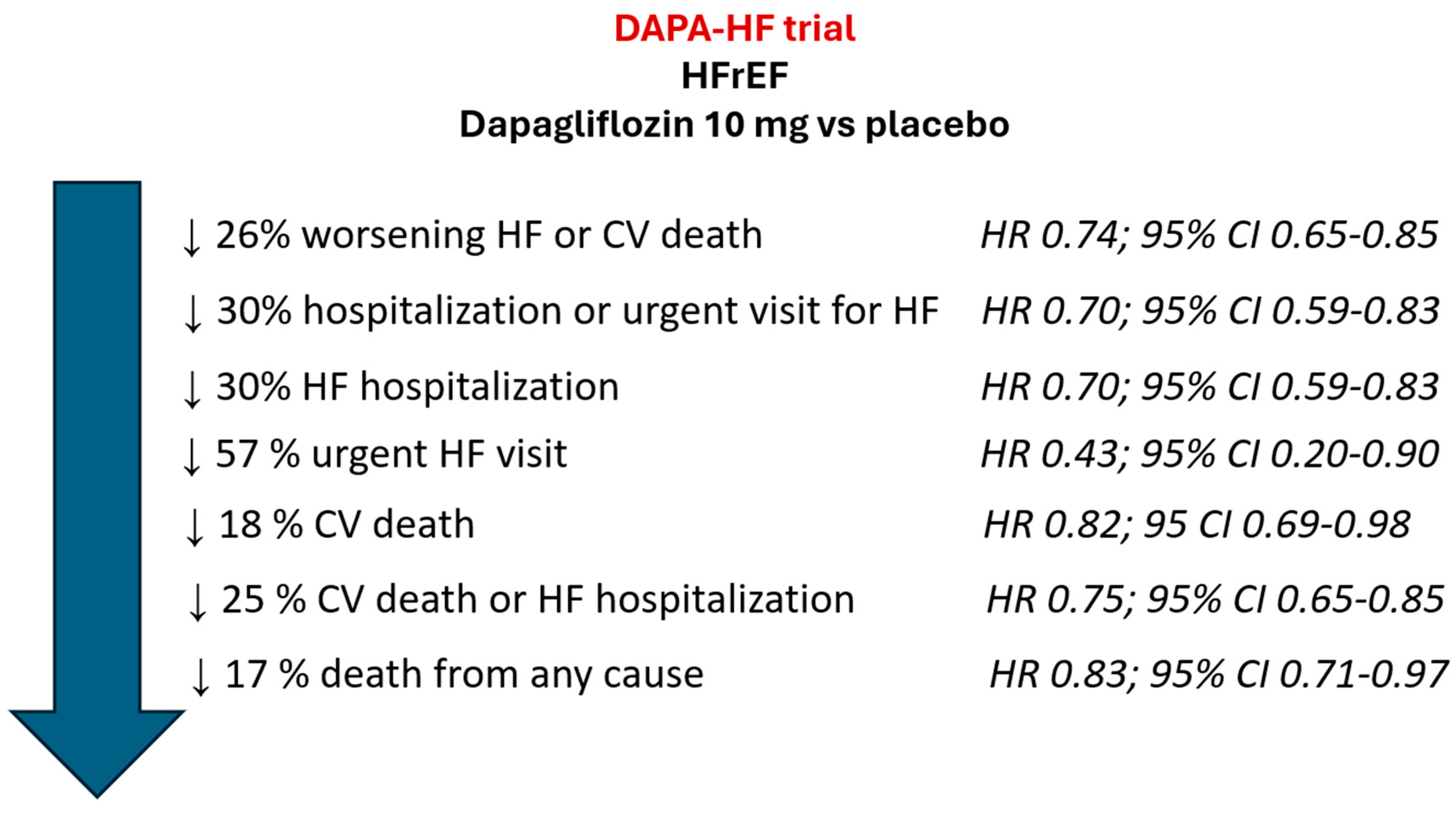
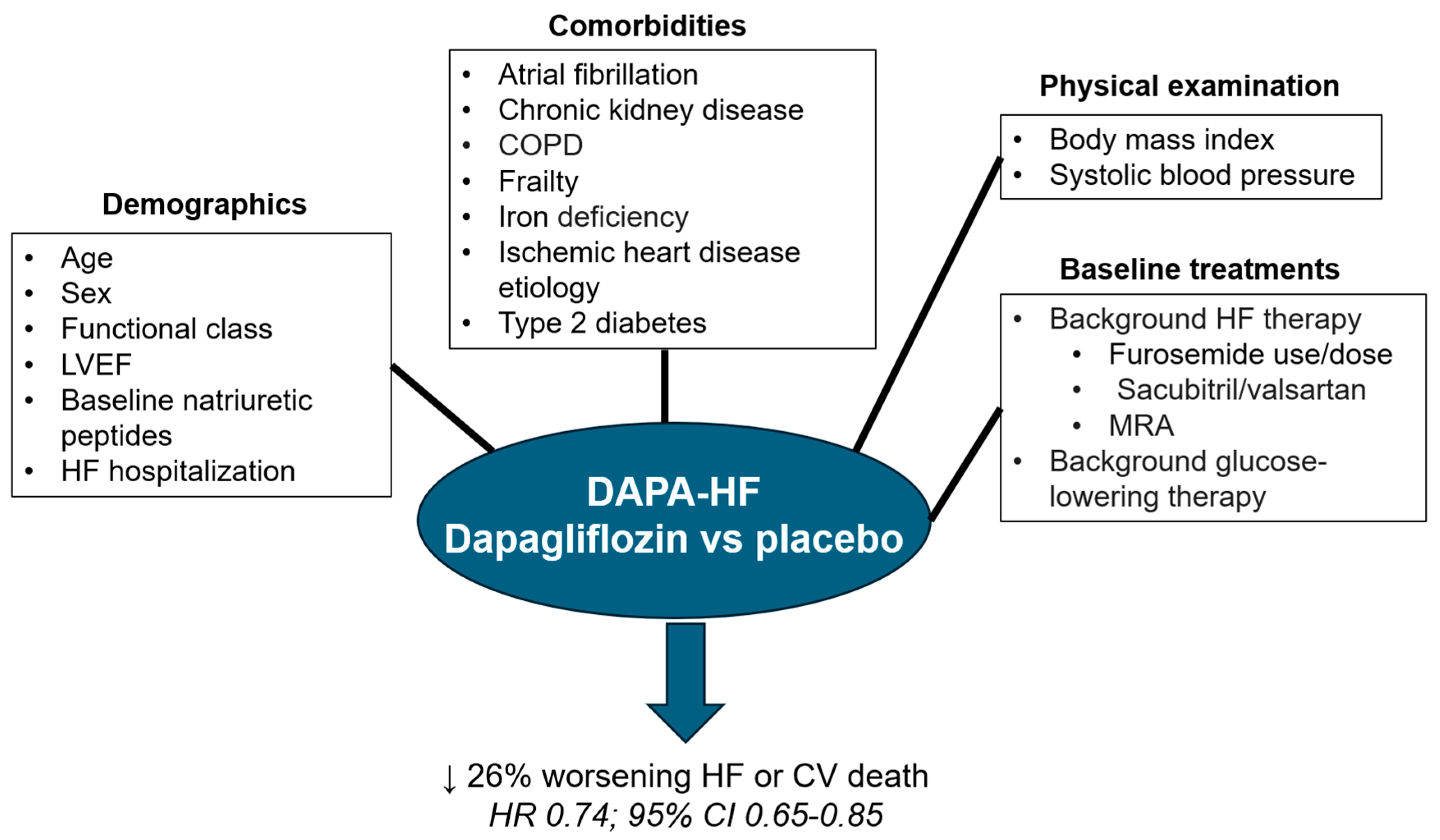
3.1. Dapagliflozin and HFrEF: The DAPA-HF Trial


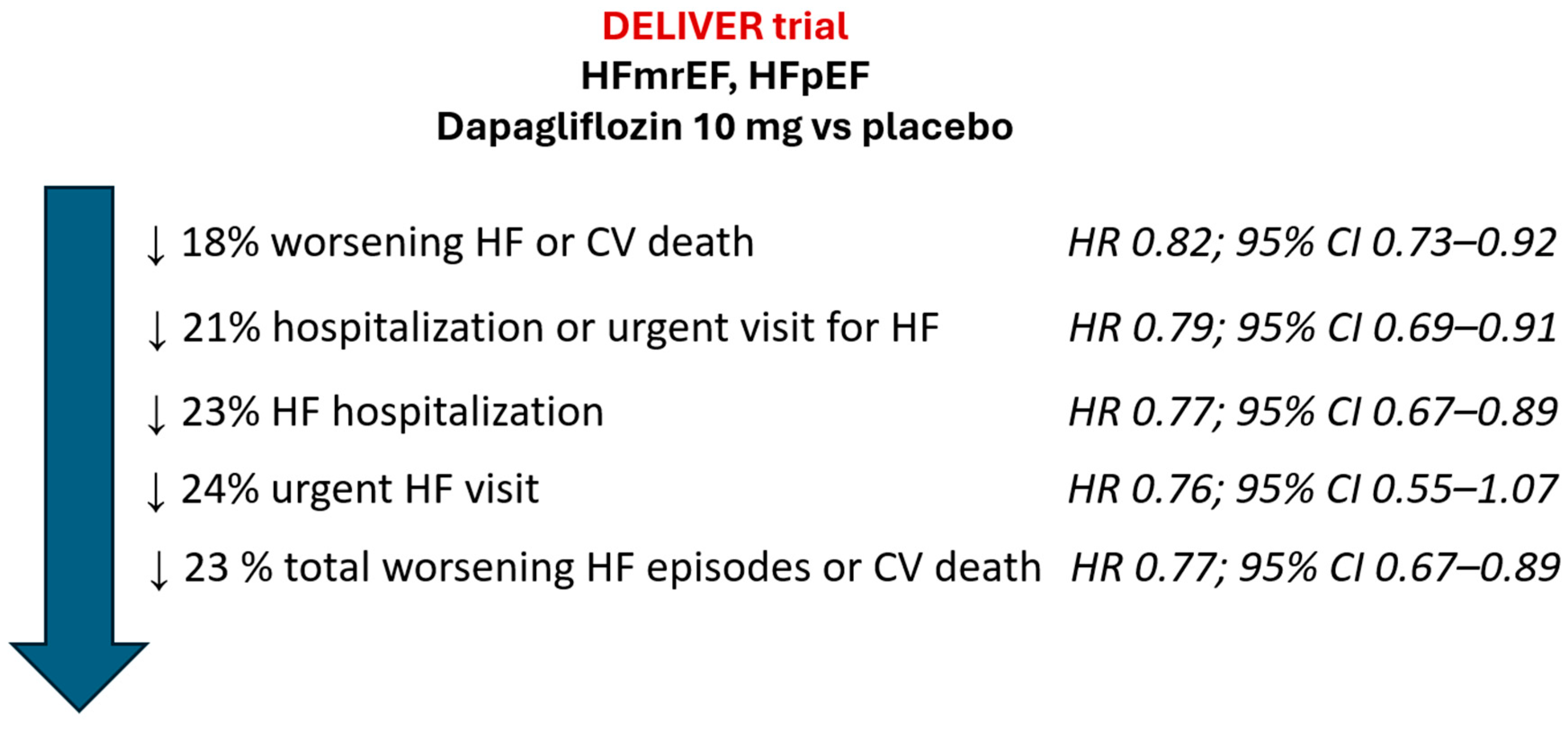
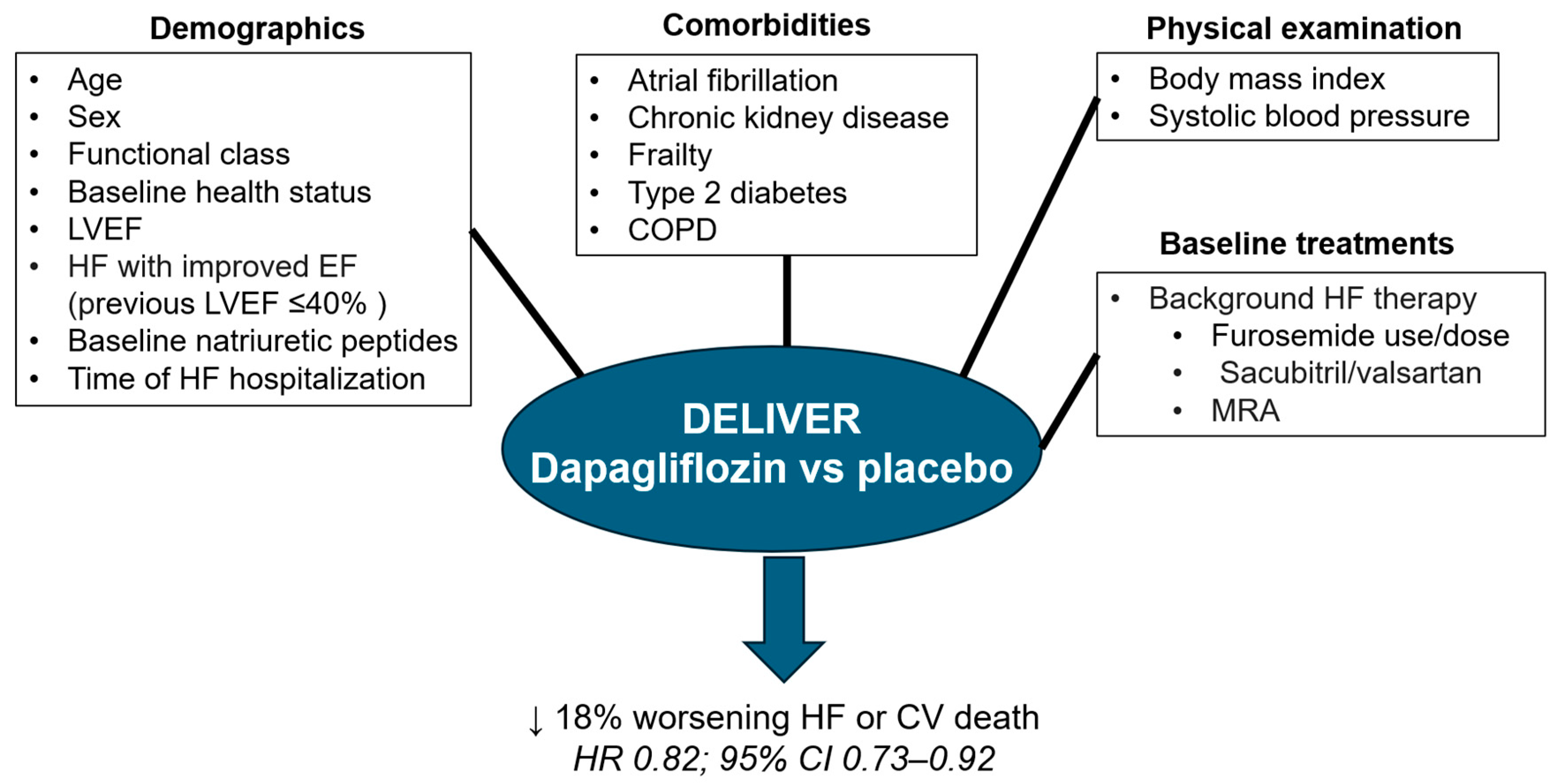
3.2. Dapagliflozin and HFmrEF and HFpEF: The DELIVER Trial
3.3. Dapagliflozin in the Whole Spectrum of HF
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Escobar, C.; Palacios, B.; Varela, L.; Gutiérrez, M.; Duong, M.; Chen, H.; Justo, N.; Cid-Ruzafa, J.; Hernández, I.; Hunt, P.R.; et al. Prevalence, Characteristics, Management and Outcomes of Patients with Heart Failure with Preserved, Mildly Reduced, and Reduced Ejection Fraction in Spain. J. Clin. Med. 2022, 11, 5199. [Google Scholar] [CrossRef]
- Lippi, G.; Sanchis-Gomarm, F. Global epidemiology and future trends of heart failure. AME. Med. J. 2020, 5, 15. [Google Scholar] [CrossRef]
- Fernández-Rodríguez, J.M.; Casado, J.; Formiga, F.; González-Franco, A.; Arévalo, J.C.; Beltrán, M.; Cerqueiro González, J.M.; Llàcer, P.; Manzano, L.; Morales-Rull, J.L.; et al. Executive summary of the 2023 update on the consensus regarding basic conduct during hospital admission for patients with acute heart failure. Rev. Clin. Esp. 2023, 223, 499–509. [Google Scholar] [CrossRef]
- van Riet, E.E.; Hoes, A.W.; Wagenaar, K.P.; Limburg, A.; Landman, M.A.; Rutten, F.H. Epidemiology of heart failure, the prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur. J. Heart Fail. 2016, 18, 242–252. [Google Scholar] [CrossRef]
- Pocock, S.J.; Ariti, C.A.; McMurray, J.J.; Maggioni, A.; Køber, L.; Squire, I.B.; Swedberg, K.; Dobson, J.; Poppe, K.K.; Whalley, G.A.; et al. Predicting survival in heart failure, a risk score based on 39,372 patients from 30 studies. Eur. Heart J. 2013, 34, 1404–1413. [Google Scholar] [CrossRef]
- Shahim, B.; Kapelios, C.J.; Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure: An Updated Review. Card Fail Rev. 2023, 9, e11. [Google Scholar] [CrossRef]
- Codina, P.; Zamora, E.; Levy, W.C.; Revuelta-López, E.; Borrellas, A.; Spitaleri, G.; Cediel, G.; Ruiz-Cueto, M.; Cañedo, E.; Santiago-Vacas, E.; et al. Mortality Risk Prediction Dynamics After Heart Failure Treatment Optimization: Repeat Risk Assessment Using Online Risk Calculators. Front. Cardiovasc. Med. 2022, 9, 836451. [Google Scholar] [CrossRef]
- Vaduganathan, M.; Claggett, B.L.; Jhund, P.S.; Cunningham, J.W.; Pedro Ferreira, J.; Zannad, F.; Packer, M.; Fonarow, G.C.; McMurray, J.J.V.; Solomon, S.D. Estimating lifetime benefits of comprehensive disease-modifying pharmacological therapies in patients with heart failure with reduced ejection fraction, a comparative analysis of three randomised controlled trials. Lancet 2020, 396, 121–128. [Google Scholar] [CrossRef]
- Chioncel, O.; Mebazaa, A.; Maggioni, A.P.; Harjola, V.P.; Rosano, G.; Laroche, C.; Piepoli, M.F.; Crespo-Leiro, M.G.; Lainscak, M.; Ponikowski, P.; et al. Acute heart failure congestion and perfusion status—Impact of the clinical classification on in-hospital and long-term outcomes, insights from the ESC-EORP-HFA heart failure long-term registry. Eur. J. Heart Fail. 2019, 21, 1338–1352. [Google Scholar] [CrossRef]
- Tomasoni, D.; Lombardi, C.M.; Sbolli, M.; Cotter, G.; Metra, M. Acute heart failure, more questions than answers. Prog. Cardiovasc. Dis. 2020, 63, 599–606. [Google Scholar] [CrossRef]
- Minana, G.; Bosch, M.J.; Nunez, E.; Mollar, A.; Santas, E.; Valero, E.; García-Blas, S.; Pellicer, M.; Bodí, V.; Chorro, F.J.; et al. Length of stay and risk of very early readmission in acute heart failure. Eur. J. Intern. Med. 2017, 42, 61–66. [Google Scholar] [CrossRef]
- Escobar, C.; Varela, L.; Palacios, B.; Capel, M.; Sicras, A.; Sicras, A.; Hormigo, A.; Alcázar, R.; Manito, N.; Botana, M. Costs and healthcare utilisation of patients with heart failure in Spain. BMC Health Serv. Res. 2020, 20, 964. [Google Scholar] [CrossRef]
- Escobar, C.; Palacios, B.; Varela, L.; Gutiérrez, M.; Duong, M.; Chen, H.; Justo, N.; Cid-Ruzafa, J.; Hernández, I.; Hunt, P.R.; et al. Healthcare resource utilization and costs among patients with heart failure with preserved; mildly reduced; and reduced ejection fraction in Spain. BMC Health Serv. Res. 2022, 22, 1241. [Google Scholar] [CrossRef]
- Redfield, M.M.; Borlaug, B.A. Heart Failure with Preserved Ejection Fraction, A Review. JAMA 2023, 329, 827–838. [Google Scholar] [CrossRef]
- Escobar, C.; Palacios, B.; Gonzalez, V.; Gutiérrez, M.; Duong, M.; Chen, H.; Justo, N.; Cid-Ruzafa, J.; Hernández, I.; Hunt, P.R.; et al. Burden of Illness beyond Mortality and Heart Failure Hospitalizations in Patients Newly Diagnosed with Heart Failure in Spain According to Ejection Fraction. J. Clin. Med. 2023, 12, 2410. [Google Scholar] [CrossRef]
- Antoine, S.; Vaidya, G.; Imam, H.; Villarreal, D. Pathophysiologic mechanisms in heart failure, role of the sympathetic nervous system. Am. J. Med. Sci. 2017, 353, 27–30. [Google Scholar] [CrossRef]
- Sayer, G.; Bhat, G. The renin-angiotensin-aldosterone system and heart failure. Cardiol. Clin. 2014, 32, 21–32. [Google Scholar] [CrossRef]
- Hubers, S.A.; Brown, N.J. Combined angiotensin receptor antagonism and neprilysin inhibition. Circulation 2016, 133, 1115–1124. [Google Scholar] [CrossRef]
- Kansakar, S.; Guragain, A.; Verma, D.; Sharma, P.; Dhungana, B.; Bhattarai, B.; Yadav, S.; Gautam, N. Soluble guanylate cyclase stimulators in heart failure. Cureus 2021, 13, e17781. [Google Scholar] [CrossRef]
- Nightingale, B. A review of the proposed mechanistic actions of sodium glucose cotransporter-2 inhibitors in the treatment of heart failure. Cardiol. Res. 2021, 12, 60–66. [Google Scholar] [CrossRef]
- Severino, P.; D’Amato, A.; Prosperi, S.; Costi, B.; Angotti, D.; Birtolo, L.I.; Chimenti, C.; Lavalle, C.; Maestrini, V.; Mancone, M.; et al. Sodium-glucose cotransporter 2 inhibitors and heart failure, the best timing for the right patient. Heart Fail. Rev. 2023, 28, 709–721. [Google Scholar] [CrossRef] [PubMed]
- Velliou, M.; Polyzogopoulou, E.; Ventoulis, I.; Parissis, J. Clinical pharmacology of SGLT-2 inhibitors in heart failure. Expert Rev. Clin. Pharmacol. 2023, 16, 149–160. [Google Scholar] [CrossRef]
- Salah, H.M.; Verma, S.; Santos-Gallego, C.G.; Bhatt, A.S.; Vaduganathan, M.; Khan, M.S.; Lopes, R.D.; Al’Aref, S.J.; McGuire, D.K.; Fudim, M. Sodium-Glucose Cotransporter 2 Inhibitors and Cardiac Remodeling. J. Cardiovasc. Transl. Res. 2022, 15, 944–956. [Google Scholar] [CrossRef]
- Green, J.B.; McCullough, P.A. Roles for SGLT2 Inhibitors in Cardiorenal Disease. Cardiorenal Med. 2022, 12, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Gallardo, J.S.; Correa, A.; Contreras, J.P. Cardio-renal benefits of sodium-glucose co-transporter 2 inhibitors in heart failure with reduced ejection fraction, mechanisms and clinical evidence. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 8, 311–321. [Google Scholar] [CrossRef]
- Xie, Y.; Wei, Y.; Li, D.; Pu, J.; Ding, H.; Zhang, X. Mechanisms of SGLT2 Inhibitors in Heart Failure and Their Clinical Value. J. Cardiovasc. Pharmacol. 2023, 81, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Lytvyn, Y.; Bjornstad, P.; Udell, J.A.; Lovshin, J.A.; Cherney, D.Z.I. Sodium Glucose Cotransporter-2 Inhibition in Heart Failure, Potential Mechanisms; Clinical Applications; and Summary of Clinical Trials. Circulation 2017, 136, 1643–1658. [Google Scholar] [CrossRef]
- De Lorenzi, A.B.; Kaplinsky, E.; Zambrano, M.R.; Chaume, L.T.; Rosas, J.M. Emerging concepts in heart failure management and treatment, focus on SGLT2 inhibitors in heart failure with preserved ejection fraction. Drugs Context 2023, 12, 2022-7-1. [Google Scholar] [CrossRef]
- McDonagh, T.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- McDonagh, T.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure, Developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2023, 44, 3627–3639. [Google Scholar] [CrossRef]
- Kittleson, M.M.; Panjrath, G.S.; Amancherla, K.; Davis, L.L.; Deswal, A.; Dixon, D.L.; Januzzi, J.L., Jr.; Yancy, C.W. 2023 ACC Expert Consensus Decision Pathway on Management of Heart Failure with Preserved Ejection Fraction, A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2023, 81, 1835–1878. [Google Scholar] [CrossRef]
- Savarese, G.; Kishi, T.; Vardeny, O.; Adamsson Eryd, S.; Bodegård, J.; Lund, L.H.; Thuresson, M.; Bozkurt, B. Heart Failure Drug Treatment-Inertia; Titration; and Discontinuation, A Multinational Observational Study (EVOLUTION HF). JACC. Heart Fail. 2023, 11, 1–14. [Google Scholar] [CrossRef]
- Obaya, J.C.; Escobar, C.; Pallarés, V.; Egocheaga, I. Practical approach of dapagliflozin for the treatment of heart failure. Role of primary care physician. Semergen 2021, 47 (Suppl. 1), 5–10. [Google Scholar] [CrossRef] [PubMed]
- Forxiga (Dapagliflozin). Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/forxiga-epar-product-information_en.pdf (accessed on 26 August 2023).
- Escobar, C.; Anguita, M.; Barrios, V.; Fernández Rodríguez, J.M.; García Pinilla, J.M.; González-Costello, J.; González Franco, A.; Gómez Huelgas, R. Update on dapagliflozin for heart failure with reduced ejection fraction. Rev. Esp. Cardiol. Supl. 2021, 21(B), 1–9. [Google Scholar]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- Furtado, R.H.M.; Bonaca, M.P.; Raz, I.; Zelniker, T.A.; Mosenzon, O.; Cahn, A.; Kuder, J.; Murphy, S.A.; Bhatt, D.L.; Leiter, L.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Patients with Type 2 Diabetes Mellitus and Previous Myocardial Infarction. Circulation 2019, 139, 2516–2527. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef]
- Wheeler, D.C.; Stefánsson, B.V.; Jongs, N.; Chertow, G.M.; Greene, T.; Hou, F.F.; McMurray, J.J.V.; Correa-Rotter, R.; Rossing, P.; Toto, R.D.; et al. Effects of dapagliflozin on major adverse kidney and cardiovascular events in patients with diabetic and non-diabetic chronic kidney disease, a prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. 2021, 9, 22–31. [Google Scholar] [CrossRef]
- Chertow, G.M.; Vart, P.; Jongs, N.; Toto, R.D.; Gorriz, J.L.; Hou, F.F.; McMurray, J.J.V.; Correa-Rotter, R.; Rossing, P.; Sjöström, C.D.; et al. Effects of Dapagliflozin in Stage 4 Chronic Kidney Disease. J. Am. Soc. Nephrol. 2021, 32, 2352–2361. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Wheeler, D.C.; Stefánsson, B.V.; Jongs, N.; Postmus, D.; Correa-Rotter, R.; Chertow, G.M.; Hou, F.F.; Rossing, P.; Sjöström, C.D.; et al. Effects of Dapagliflozin in Patients with Kidney Disease; with and without Heart Failure. JACC Heart Fail. 2021, 9, 807–820. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; McMurray, J.J.V.; Claggett, B.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; et al. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N. Engl. J. Med. 2022, 387, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Nassif, M.E.; Windsor, S.L.; Tang, F.; Khariton, Y.; Husain, M.; Inzucchi, S.E.; McGuire, D.K.; Pitt, B.; Scirica, B.M.; Austin, B.; et al. Dapagliflozin Effects on Biomarkers; Symptoms; and Functional Status in Patients with Heart Failure with Reduced Ejection Fraction, The DEFINE-HF Trial. Circulation 2019, 140, 1463–1476. [Google Scholar] [CrossRef] [PubMed]
- Nassif, M.E.; Windsor, S.L.; Tang, F.; Husain, M.; Inzucchi, S.E.; McGuire, D.K.; Pitt, B.; Scirica, B.M.; Austin, B.; Fong, M.W.; et al. Dapagliflozin effects on lung fluid volumes in patients with heart failure and reduced ejection fraction, Results from the DEFINE-HF trial. Diabetes Obes. Metab. 2021, 23, 1426–1430. [Google Scholar] [CrossRef] [PubMed]
- Nassif, M.E.; Windsor, S.L.; Gosch, K.; Borlaug, B.A.; Husain, M.; Inzucchi, S.E.; Kitzman, D.W.; McGuire, D.K.; Pitt, B.; Scirica, B.M.; et al. Dapagliflozin Improves Heart Failure Symptoms and Physical Limitations Across the Full Range of Ejection Fraction, Pooled Patient-Level Analysis From DEFINE-HF and PRESERVED-HF Trials. Circ. Heart Fail. 2023, 16, e009837. [Google Scholar] [CrossRef]
- Palau, P.; Amiguet, M.; Domínguez, E.; Sastre, C.; Mollar, A.; Seller, J.; Garcia Pinilla, J.M.; Larumbe, A.; Valle, A.; Gómez Doblas, J.J.; et al. Short-term effects of dapagliflozin on maximal functional capacity in heart failure with reduced ejection fraction (DAPA-VO2), a randomized clinical trial. Eur. J. Heart Fail. 2022, 24, 1816–1826. [Google Scholar] [CrossRef]
- Petrie, M.C.; Verma, S.; Docherty, K.F.; Inzucchi, S.E.; Anand, I.; Belohlávek, J.; Böhm, M.; Chiang, C.E.; Chopra, V.K.; de Boer, R.A.; et al. Effect of Dapagliflozin on Worsening Heart Failure and Cardiovascular Death in Patients with Heart Failure with and without Diabetes. JAMA 2020, 323, 1353–1368. [Google Scholar] [CrossRef]
- Inzucchi, S.E.; Docherty, K.F.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Solomon, S.D.; Verma, S.; Bělohlávek, J.; et al. Dapagliflozin and the Incidence of Type 2 Diabetes in Patients with Heart Failure and Reduced Ejection Fraction, An Exploratory Analysis From DAPA-HF. Diabetes Care 2021, 44, 586–594. [Google Scholar] [CrossRef]
- Rossing, P.; Inzucchi, S.E.; Vart, P.; Jongs, N.; Docherty, K.F.; Jhund, P.S.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; et al. Dapagliflozin and new-onset type 2 diabetes in patients with chronic kidney disease or heart failure, pooled analysis of the DAPA-CKD and DAPA-HF trials. Lancet Diabetes Endocrinol. 2022, 10, 24–34. [Google Scholar] [CrossRef]
- Butt, J.H.; Nicolau, J.C.; Verma, S.; Docherty, K.F.; Petrie, M.C.; Inzucchi, S.E.; Schou, M.; Kosiborod, M.N.; Langkilde, A.M.; Martinez, F.A.; et al. Efficacy and safety of dapagliflozin according to aetiology in heart failure with reduced ejection fraction, insights from the DAPA-HF trial. Eur. J. Heart Fail. 2021, 23, 601–613. [Google Scholar] [CrossRef]
- Docherty, K.F.; Simpson, J.; Jhund, P.S.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Bengtsson, O.; et al. Effect of Dapagliflozin; Compared with Placebo; According to Baseline Risk in DAPA-HF. JACC Heart Fail. 2022, 10, 104–118. [Google Scholar] [CrossRef] [PubMed]
- Jhund, P.S.; Solomon, S.D.; Docherty, K.F.; Heerspink, H.J.L.; Anand, I.S.; Böhm, M.; Chopra, V.; de Boer, R.A.; Desai, A.S.; Ge, J.; et al. Efficacy of Dapagliflozin on Renal Function and Outcomes in Patients with Heart Failure with Reduced Ejection Fraction, Results of DAPA-HF. Circulation 2021, 143, 298–309. [Google Scholar] [CrossRef]
- Martinez, F.A.; Serenelli, M.; Nicolau, J.C.; Petrie, M.C.; Chiang, C.E.; Tereshchenko, S.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; et al. Efficacy and Safety of Dapagliflozin in Heart Failure with Reduced Ejection Fraction According to Age, Insights From DAPA-HF. Circulation 2020, 141, 100–111. [Google Scholar] [CrossRef]
- Butt, J.H.; Dewan, P.; Merkely, B.; Belohlávek, J.; Drożdż, J.; Kitakaze, M.; Inzucchi, S.E.; Kosiborod, M.N.; Martinez, F.A.; Tereshchenko, S.; et al. Efficacy and Safety of Dapagliflozin According to Frailty in Heart Failure with Reduced Ejection Fraction, A Post Hoc Analysis of the DAPA-HF Trial. Ann. Intern. Med. 2022, 175, 820–830. [Google Scholar] [CrossRef] [PubMed]
- Serenelli, M.; Böhm, M.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Solomon, S.D.; DeMets, D.L.; et al. Effect of dapagliflozin according to baseline systolic blood pressure in the Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure trial (DAPA-HF). Eur. Heart J. 2020, 41, 3402–3418. [Google Scholar] [CrossRef] [PubMed]
- Butt, J.H.; Docherty, K.F.; Petrie, M.C.; Schou, M.; Kosiborod, M.N.; O’Meara, E.; Katova, T.; Ljungman, C.E.A.; Diez, M.; Ogunniyi, M.O.; et al. Efficacy and Safety of Dapagliflozin in Men and Women with Heart Failure with Reduced Ejection Fraction, A Prespecified Analysis of the Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure Trial. JAMA Cardiol. 2021, 6, 678–689. [Google Scholar] [CrossRef]
- Butt, J.H.; Docherty, K.F.; Jhund, P.S.; de Boer, R.A.; Böhm, M.; Desai, A.S.; Howlett, J.G.; Inzucchi, S.E.; Kosiborod, M.N.; Martinez, F.A.; et al. Dapagliflozin and atrial fibrillation in heart failure with reduced ejection fraction, insights from DAPA-HF. Eur. J. Heart Fail. 2022, 24, 513–525. [Google Scholar] [CrossRef]
- Curtain, J.P.; Docherty, K.F.; Jhund, P.S.; Petrie, M.C.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; et al. Effect of dapagliflozin on ventricular arrhythmias; resuscitated cardiac arrest; or sudden death in DAPA-HF. Eur. Heart J. 2021, 42, 3727–3738. [Google Scholar] [CrossRef]
- Adamson, C.; Jhund, P.S.; Docherty, K.F.; Bělohlávek, J.; Chiang, C.E.; Diez, M.; Drożdż, J.; Dukát, A.; Howlett, J.; Ljungman, C.E.A.; et al. Efficacy of dapagliflozin in heart failure with reduced ejection fraction according to body mass index. Eur. J. Heart Fail. 2021, 23, 1662–1672. [Google Scholar] [CrossRef]
- Dewan, P.; Docherty, K.F.; Bengtsson, O.; de Boer, R.A.; Desai, A.S.; Drozdz, J.; Hawkins, N.M.; Inzucchi, S.E.; Kitakaze, M.; Køber, L.; et al. Effects of dapagliflozin in heart failure with reduced ejection fraction and chronic obstructive pulmonary disease, an analysis of DAPA-HF. Eur. J. Heart Fail. 2021, 23, 632–643. [Google Scholar] [CrossRef]
- Docherty, K.F.; Welsh, P.; Verma, S.; De Boer, R.A.; O’Meara, E.; Bengtsson, O.; Køber, L.; Kosiborod, M.N.; Hammarstedt, A.; Langkilde, A.M.; et al. Iron Deficiency in Heart Failure and Effect of Dapagliflozin, Findings From DAPA-HF. Circulation 2022, 146, 980–994. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.M.; Dewan, P.; Anand, I.S.; Bělohlávek, J.; Bengtsson, O.; de Boer, R.A.; Böhm, M.; Boulton, D.W.; Chopra, V.K.; DeMets, D.L.; et al. Dapagliflozin and Diuretic Use in Patients with Heart Failure and Reduced Ejection Fraction in DAPA-HF. Circulation 2020, 142, 1040–1054. [Google Scholar] [CrossRef] [PubMed]
- Docherty, K.F.; Jhund, P.S.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; DeMets, D.L.; Sabatine, M.S.; Bengtsson, O.; et al. Effects of dapagliflozin in DAPA-HF according to background heart failure therapy. Eur. Heart J. 2020, 41, 2379–2392. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; Jhund, P.S.; Claggett, B.L.; Dewan, P.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Inzucchi, S.E.; et al. Effect of Dapagliflozin in Patients with HFrEF Treated with Sacubitril/Valsartan, The DAPA-HF Trial. JACC Heart Fail. 2020, 8, 811–818. [Google Scholar] [CrossRef]
- Shen, L.; Kristensen, S.L.; Bengtsson, O.; Böhm, M.; de Boer, R.A.; Docherty, K.F.; Inzucchi, S.E.; Katova, T.; Køber, L.; Kosiborod, M.N.; et al. Dapagliflozin in HFrEF Patients Treated with Mineralocorticoid Receptor Antagonists, An Analysis of DAPA-HF. JACC Heart Fail. 2021, 9, 254–264. [Google Scholar]
- Kristensen, S.L.; Docherty, K.F.; Jhund, P.S.; Bengtsson, O.; Demets, D.L.; Inzucchi, S.E.; Kober, L.; Kosiborod, M.N.; Langkilde, A.M.; Martinez, F.A.; et al. Dapagliflozin reduces the risk of hyperkalaemia in patients with heart failure and reduced ejection fraction, a secondary analysis DAPA-HF. Eur. Heart J. 2020, 41 (Suppl. 2), ehaa946.0939. [Google Scholar] [CrossRef]
- Docherty, K.F.; Jhund, P.S.; Bengtsson, O.; DeMets, D.L.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Langkilde, A.M.; Martinez, F.A.; Sabatine, M.S.; et al. Effect of Dapagliflozin in DAPA-HF According to Background Glucose-Lowering Therapy. Diabetes Care 2020, 43, 2878–2881. [Google Scholar] [CrossRef]
- Docherty, K.F.; Jhund, P.S.; Anand, I.; Bengtsson, O.; Böhm, M.; de Boer, R.A.; DeMets, D.L.; Desai, A.S.; Drozdz, J.; Howlett, J.; et al. Effect of Dapagliflozin on Outpatient Worsening of Patients with Heart Failure and Reduced Ejection Fraction, A Prespecified Analysis of DAPA-HF. Circulation 2020, 142, 1623–1632. [Google Scholar] [CrossRef]
- Kosiborod, M.N.; Jhund, P.S.; Docherty, K.F.; Diez, M.; Petrie, M.C.; Verma, S.; Nicolau, J.C.; Merkely, B.; Kitakaze, M.; DeMets, D.L.; et al. Effects of Dapagliflozin on Symptoms; Function; and Quality of Life in Patients with Heart Failure and Reduced Ejection Fraction, Results From the DAPA-HF Trial. Circulation 2020, 141, 90–99. [Google Scholar] [CrossRef]
- Berg, D.D.; Jhund, P.S.; Docherty, K.F.; Murphy, S.A.; Verma, S.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Langkilde, A.M.; Martinez, F.A.; et al. Time to Clinical Benefit of Dapagliflozin and Significance of Prior Heart Failure Hospitalization in Patients with Heart Failure with Reduced Ejection Fraction. JAMA Cardiol. 2021, 6, 499–507. [Google Scholar] [CrossRef]
- Docherty, K.F.; Jhund, P.S.; Claggett, B.; Ferreira, J.P.; Bengtsson, O.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Langkilde, A.M.; Martinez, F.A.; et al. Extrapolating Long-term Event-Free and Overall Survival with Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction, An Exploratory Analysis of a Phase 3 Randomized Clinical Trial. JAMA Cardiol. 2021, 6, 1298–1305. [Google Scholar] [CrossRef]
- Inzucchi, S.E.; Claggett, B.L.; Vaduganathan, M.; Desai, A.S.; Jhund, P.S.; de Boer, R.A.; Hernandez, A.F.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; et al. Efficacy and safety of dapagliflozin in patients with heart failure with mildly reduced or preserved ejection fraction by baseline glycaemic status (DELIVER), a subgroup analysis from an international; multicentre; double-blind; randomised; placebo-controlled trial. Lancet Diabetes Endocrinol. 2022, 10, 869–881. [Google Scholar]
- Mc Causland, F.R.; Claggett, B.L.; Vaduganathan, M.; Desai, A.S.; Jhund, P.; de Boer, R.A.; Docherty, K.; Fang, J.; Hernandez, A.F.; Inzucchi, S.E.; et al. Dapagliflozin and Kidney Outcomes in Patients with Heart Failure with Mildly Reduced or Preserved Ejection Fraction, A Prespecified Analysis of the DELIVER Randomized Clinical Trial. JAMA Cardiol. 2023, 8, 56–65. [Google Scholar] [CrossRef]
- Peikert, A.; Martinez, F.A.; Vaduganathan, M.; Claggett, B.L.; Kulac, I.J.; Desai, A.S.; Jhund, P.S.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; et al. Efficacy and Safety of Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction According to Age, The DELIVER Trial. Circ. Heart Fail. 2022, 15, e010080. [Google Scholar] [CrossRef]
- Butt, J.H.; Jhund, P.S.; Belohlávek, J.; de Boer, R.A.; Chiang, C.E.; Desai, A.S.; Drożdż, J.; Hernandez, A.F.; Inzucchi, S.E.; Katova, T.; et al. Efficacy and Safety of Dapagliflozin According to Frailty in Patients with Heart Failure, A Prespecified Analysis of the DELIVER Trial. Circulation 2022, 146, 1210–1224. [Google Scholar] [CrossRef]
- Selvaraj, S.; Vaduganathan, M.; Claggett, B.L.; Miao, Z.M.; Fang, J.C.; Vardeny, O.; Desai, A.S.; Shah, S.J.; Lam, C.S.P.; Martinez, F.A.; et al. Blood Pressure and Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction, DELIVER. JACC Heart Fail. 2023, 11, 76–89. [Google Scholar] [CrossRef]
- Chatur, S.; Cunningham, J.W.; Vaduganathan, M.; Mc Causland, F.R.; Claggett, B.L.; Desai, A.S.; Miao, Z.M.; Jhund, P.S.; de Boer, R.A.; Hernandez, A.F.; et al. Renal and blood pressure effects of dapagliflozin in recently hospitalized patients with heart failure with mildly reduced or preserved ejection fraction, Insights from the DELIVER trial. Eur. J. Heart Fail. 2023, 25, 1170–1175. [Google Scholar] [CrossRef]
- Butt, J.H.; Kondo, T.; Jhund, P.S.; Comin-Colet, J.; de Boer, R.A.; Desai, A.S.; Hernandez, A.F.; Inzucchi, S.E.; Janssens, S.P.; Kosiborod, M.N.; et al. Atrial Fibrillation and Dapagliflozin Efficacy in Patients with Preserved or Mildly Reduced Ejection Fraction. J. Am. Coll. Cardiol. 2022, 80, 1705–1717. [Google Scholar] [CrossRef]
- Adamson, C.; Kondo, T.; Jhund, P.S.; de Boer, R.A.; Cabrera Honorio, J.W.; Claggett, B.; Desai, A.S.; Alcocer Gamba, M.A.; Al Habeeb, W.; Hernandez, A.F.; et al. Dapagliflozin for heart failure according to body mass index, the DELIVER trial. Eur. Heart J. 2022, 43, 4406–4417. [Google Scholar] [CrossRef]
- Chatur, S.; Vaduganathan, M.; Claggett, B.; Vardeny, O.; Desai, A.S.; Jhund, P.S.; de Boer, R.A.; Lam, C.S.P.; Kosiborod, M.N.; Shah, S.J.; et al. Dapagliflozin and diuretic utilization in heart failure with mildly reduced or preserved ejection fraction, the DELIVER trial. Eur. Heart J. 2023, 44, 2930–2943. [Google Scholar] [CrossRef]
- Yang, M.; Butt, J.H.; Kondo, T.; Jering, K.S.; Docherty, K.F.; Jhund, P.S.; de Boer, R.A.; Claggett, B.L.; Desai, A.S.; Hernandez, A.F.; et al. Dapagliflozin in patients with heart failure with mildly reduced and preserved ejection fraction treated with a mineralocorticoid receptor antagonist or sacubitril/valsartan. Eur. J. Heart Fail. 2022, 24, 2307–2319. [Google Scholar] [CrossRef] [PubMed]
- Vardeny, O.; Fang, J.C.; Desai, A.S.; Jhund, P.S.; Claggett, B.; Vaduganathan, M.; de Boer, R.A.; Hernandez, A.F.; Lam, C.S.P.; Inzucchi, S.E.; et al. Dapagliflozin in heart failure with improved ejection fraction, a prespecified analysis of the DELIVER trial. Nat. Med. 2022, 28, 2504–2511. [Google Scholar] [CrossRef] [PubMed]
- Ostrominski, J.W.; Vaduganathan, M.; Claggett, B.L.; de Boer, R.A.; Desai, A.S.; Dobreanu, D.; Hernandez, A.F.; Inzucchi, S.E.; Jhund, P.S.; Kosiborod, M.; et al. Dapagliflozin and New York Heart Association functional class in heart failure with mildly reduced or preserved ejection fraction, the DELIVER trial. Eur. J. Heart Fail. 2022, 24, 1892–1901. [Google Scholar] [CrossRef] [PubMed]
- Peikert, A.; Chandra, A.; Kosiborod, M.N.; Claggett, B.L.; Desai, A.S.; Jhund, P.S.; Lam, C.S.P.; Inzucchi, S.E.; Martinez, F.A.; de Boer, R.A.; et al. Association of Dapagliflozin vs Placebo with Individual Kansas City Cardiomyopathy Questionnaire Components in Patients with Heart Failure with Mildly Reduced or Preserved Ejection Fraction, A Secondary Analysis of the DELIVER Trial. JAMA Cardiol. 2023, 8, 684–690. [Google Scholar] [CrossRef] [PubMed]
- Nassif, M.E.; Windsor, S.L.; Borlaug, B.A.; Kitzman, D.W.; Shah, S.J.; Tang, F.; Khariton, Y.; Malik, A.O.; Khumri, T.; Umpierrez, G.; et al. The SGLT2 inhibitor dapagliflozin in heart failure with preserved ejection fraction, a multicenter randomized trial. Nat. Med. 2021, 27, 1954–1960. [Google Scholar] [CrossRef]
- Myhre, P.L.; Vaduganathan, M.; Claggett, B.L.; Miao, Z.M.; Jhund, P.S.; de Boer, R.A.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; et al. Influence of NT-proBNP on Efficacy of Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. JACC Heart Fail. 2022, 10, 902–913. [Google Scholar] [CrossRef]
- Jhund, P.S.; Claggett, B.L.; Talebi, A.; Butt, J.H.; Gasparyan, S.B.; Wei, L.J.; McCaw, Z.R.; Wilderäng, U.; Bengtsson, O.; Desai, A.S.; et al. Effect of Dapagliflozin on Total Heart Failure Events in Patients with Heart Failure with Mildly Reduced or Preserved Ejection Fraction, A Prespecified Analysis of the DELIVER Trial. JAMA Cardiol. 2023, 8, 554–563. [Google Scholar] [CrossRef]
- Jhund, P.S.; Ponikowski, P.; Docherty, K.F.; Gasparyan, S.B.; Böhm, M.; Chiang, C.E.; Desai, A.S.; Howlett, J.; Kitakaze, M.; Petrie, M.C.; et al. Dapagliflozin and Recurrent Heart Failure Hospitalizations in Heart Failure with Reduced Ejection Fraction, An Analysis of DAPA-HF. Circulation 2021, 143, 1962–1972. [Google Scholar] [CrossRef]
- Cunningham, J.W.; Vaduganathan, M.; Claggett, B.L.; Kulac, I.J.; Desai, A.S.; Jhund, P.S.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; et al. Dapagliflozin in Patients Recently Hospitalized with Heart Failure and Mildly Reduced or Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2022, 80, 1302–1310. [Google Scholar] [CrossRef]
- Vaduganathan, M.; Claggett, B.L.; Jhund, P.; de Boer, R.A.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; Shah, S.J.; et al. Time to Clinical Benefit of Dapagliflozin in Patients with Heart Failure with Mildly Reduced or Preserved Ejection Fraction, A Prespecified Secondary Analysis of the DELIVER Randomized Clinical Trial. JAMA Cardiol. 2022, 7, 1259–1263. [Google Scholar] [CrossRef]
- Vaduganathan, M.; Claggett, B.L.; Jhund, P.; de Boer, R.A.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; Shah, S.J.; et al. Estimated Long-Term Benefit of Dapagliflozin in Patients with Heart Failure. J. Am. Coll. Cardiol. 2022, 80, 1775–1784. [Google Scholar] [CrossRef] [PubMed]
- Jhund, P.S.; Kondo, T.; Butt, J.H.; Docherty, K.F.; Claggett, B.L.; Desai, A.S.; Vaduganathan, M.; Gasparyan, S.B.; Bengtsson, O.; Lindholm, D.; et al. Dapagliflozin across the range of ejection fraction in patients with heart failure, a patient-level; pooled meta-analysis of DAPA-HF and DELIVER. Nat. Med. 2022, 28, 1956–1964. [Google Scholar] [CrossRef]
- Wang, X.; Vaduganathan, M.; Claggett, B.L.; Hegde, S.M.; Pabon, M.; Kulac, I.J.; Vardeny, O.; O’Meara, E.; Zieroth, S.; Katova, T.; et al. Sex Differences in Characteristics; Outcomes; and Treatment Response with Dapagliflozin Across the Range of Ejection Fraction in Patients with Heart Failure, Insights From DAPA-HF and DELIVER. Circulation 2023, 147, 624–634. [Google Scholar] [CrossRef] [PubMed]
- Amiguet, M.; Palau, P.; Domínguez, E.; Seller, J.; Pinilla, J.M.G.; de la Espriella, R.; Miñana, G.; Valle, A.; Sanchis, J.; Górriz, J.L.; et al. Dapagliflozin and short-term changes on circulating antigen carbohydrate 125 in heart failure with reduced ejection fraction. Sci. Rep. 2023, 13, 10591. [Google Scholar] [CrossRef]
- Charaya, K.; Shchekochikhin, D.; Andreev, D.; Dyachuk, I.; Tarasenko, S.; Poltavskaya, M.; Mesitskaya, D.; Bogdanova, A.; Ananicheva, N.; Kuzub, A. Impact of dapagliflozin treatment on renal function and diuretics use in acute heart failure: A pilot study. Open Heart 2022, 9, e001936. [Google Scholar] [CrossRef]
- Yeoh, S.E.; Osmanska, J.; Petrie, M.C.; Brooksbank, K.J.M.; Clark, A.L.; Docherty, K.F.; Foley, P.W.X.; Guha, K.; Halliday, C.A.; Jhund, P.S.; et al. Dapagliflozin vs. metolazone in heart failure resistant to loop diuretics. Eur. Heart J. 2023, 44, 2966–2977. [Google Scholar] [CrossRef] [PubMed]
- Cox, Z.L.; Collins, S.P.; Aaron, M.; Hernandez, G.A.; Iii, A.T.M.; Davidson, B.T.; Fowler, M.; Lindsell, C.J.; Jr, F.E.H.; Jenkins, C.A.; et al. Efficacy and safety of dapagliflozin in acute heart failure: Rationale and design of the DICTATE-AHF trial. Am. Heart J. 2021, 232, 116–124. [Google Scholar] [CrossRef]
- Cox, Z. DICTATE-AHF trial. Presented in a Hot Line Session today at ESC Congress 2023. Available online: https://www.escardio.org/The-ESC/Press-Office/Press-releases/DICTATE-AHF-trial-fails-to-meet-primary-endpoint-with-dapagliflozin-in-acute-heart-failure (accessed on 2 September 2023).
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner-La Rocca, H.P.; Choi, D.J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Talha, K.M.; Butler, J.; Greene, S.J.; Aggarwal, R.; Anker, S.D.; Claggett, B.L.; Solomon, S.D.; McMurray, J.J.V.; Vaduganathan, M.; Fonarow, G.C. Population-Level Implications of Sodium-Glucose Cotransporter-2 Inhibitors for Heart Failure with Preserved Ejection Fraction in the US. JAMA Cardiol. 2023, 8, 66–73. [Google Scholar] [CrossRef]
- Håkansson, E.; Norberg, H.; Själander, S.; Lindmark, K. Eligibility of Dapagliflozin and Empagliflozin in a Real-World Heart Failure Population. Cardiovasc. Ther. 2021, 2021, 1894155. [Google Scholar] [CrossRef]
- Thorvaldsen, T.; Ferrannini, G.; Mellbin, L.; Benson, L.; Cosentino, F.; McMurray, J.J.V.; Dahlström, U.; Lund, L.H.; Savarese, G. Eligibility for Dapagliflozin and Empagliflozin in a Real-world Heart Failure Population. J. Card. Fail. 2022, 28, 1050–1062. [Google Scholar] [CrossRef]
- Maltês, S.; Cunha, G.J.L.; Rocha, B.M.L.; Presume, J.; Guerreiro, R.; Henriques, C.; Rodrigues, C.; Araújo, I.; Fonseca, C. Dapagliflozin in a Real-World Chronic Heart Failure Population: How Many Are Actually Eligible? Cardiology 2021, 146, 201–206. [Google Scholar] [CrossRef]
- Montero-Pérez-Barquero, M.; Escobar-Cervantes, C.; Arévalo-Lorido, J.C.; Conde-Martel, A.; Salamanca-Bautista, P.; Manzano-Espinosa, L.; Formiga, F.; Díez-Manglano, J.; Cepeda, J.M.; González-Franco, A.; et al. Projected effectiveness of dapagliflozin in heart failure with reduced ejection fraction in clinical practice. Future Cardiol. 2023, 19, 343–351. [Google Scholar] [CrossRef]
- Montero-Pérez-Barquero, M.; Escobar-Cervantes, C.; Llàcer, P.; Quirós-López, R.; Trullás, J.C.; Cerqueiro, J.M.; Epelde-Gonzálo, F.; Carrera-Izquierdo, M.; Formiga, F.; González-Franco, A.; et al. Projected clinical benefits of dapagliflozin in patients with heart failure with preserved ejection fraction. Future Cardiol. 2023, 19, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Montero-Pérez-Barquero, M.; Escobar-Cervantes, C.; Dávila-Ramos, M.F.; Suárez-Pedreira, I.; Pérez-Silvestre, J.; Ceresuela-Eito, L.M.; Muela-Molinero, A.; Quesada-Simón, M.A.; Formiga, F.; González-Franco, A.; et al. Benefits of dapagliflozin in the whole spectrum of heart failure in clinical practice: The RICA registry. Future Cardiol. 2023, 19, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Ma, Y. Dapagliflozin Inhibits Ventricular Remodeling in Heart Failure Rats by Activating Autophagy through AMPK/mTOR Pathway. Comput. Math. Methods Med. 2022, 2022, 6260202. [Google Scholar] [CrossRef]
- Zhang, N.; Feng, B.; Ma, X.; Sun, K.; Xu, G.; Zhou, Y. Dapagliflozin improves left ventricular remodeling and aorta sympathetic tone in a pig model of heart failure with preserved ejection fraction. Cardiovasc. Diabetol. 2019, 18, 107. [Google Scholar] [CrossRef] [PubMed]
- Withaar, C.; Meems, L.M.G.; Markousis-Mavrogenis, G.; Boogerd, C.J.; Silljé, H.H.W.; Schouten, E.M.; Dokter, M.M.; Voors, A.A.; Westenbrink, B.D.; Lam, C.S.P.; et al. The effects of liraglutide and dapagliflozin on cardiac function and structure in a multi-hit mouse model of heart failure with preserved ejection fraction. Cardiovasc. Res. 2021, 117, 2108–2124. [Google Scholar] [CrossRef]
- Lee, S.G.; Kim, D.; Lee, J.J.; Lee, H.J.; Moon, R.K.; Lee, Y.J.; Lee, S.J.; Lee, O.H.; Kim, C.; Oh, J.; et al. Dapagliflozin attenuates diabetes-induced diastolic dysfunction and cardiac fibrosis by regulating SGK1 signaling. BMC Med. 2022, 20, 309. [Google Scholar] [CrossRef] [PubMed]
- Ren, F.F.; Xie, Z.Y.; Jiang, Y.N.; Guan, X.; Chen, Q.Y.; Lai, T.F.; Li, L. Dapagliflozin attenuates pressure overload-induced myocardial remodeling in mice via activating SIRT1 and inhibiting endoplasmic reticulum stress. Acta Pharmacol. Sin. 2022, 43, 1721–1732. [Google Scholar] [CrossRef]
- Bao, N.; Liu, X.; Zhong, X.; Jia, S.; Hua, N.; Zhang, L.; Mo, G. Dapagliflozin-affected endothelial dysfunction and altered gut microbiota in mice with heart failure. PeerJ 2023, 11, e15589. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.; Chen, L.; Yan, J.; Shen, M.; Zhang, R.; Li, M.; He, M.; Chen, K.; Zhu, Y.; Lin, H.; et al. Dapagliflozin attenuates residual cardiac remodeling after surgical ventricular reconstruction in mice with an enlarged heart after myocardial infarction. Biomed. Pharmacother. 2022, 156, 113765. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lin, X.; Chu, Y.; Chen, X.; Du, H.; Zhang, H.; Xu, C.; Xie, H.; Ruan, Q.; Lin, J.; et al. Dapagliflozin: A sodium-glucose cotransporter 2 inhibitor; attenuates angiotensin II-induced cardiac fibrotic remodeling by regulating TGFβ1/Smad signaling. Cardiovasc. Diabetol. 2021, 20, 121. [Google Scholar] [CrossRef]
- Wang, C.; Qin, Y.; Zhang, X.; Yang, Y.; Wu, X.; Liu, J.; Qin, S.; Chen, K.; Xiao, W. Effect of Dapagliflozin on Indicators of Myocardial Fibrosis and Levels of Inflammatory Factors in Heart Failure Patients. Dis. Markers 2022, 2022, 5834218. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; She, Q.; Du, J. Dapagliflozin attenuates myocardial remodeling in hypertension by activating the circadian rhythm signaling pathway. Arch. Pharm. Res. 2023, 46, 117–130. [Google Scholar] [CrossRef]
- Pascual-Figal, D.A.; Zamorano, J.L.; Domingo, M.; Morillas, H.; Nuñez, J.; Cobo Marcos, M.; Riquelme-Pérez, A.; Teis, A.; Santas, E.; Caro-Martinez, C.; et al. Impact of dapagliflozin on cardiac remodelling in patients with chronic heart failure: The DAPA-MODA study. Eur. J. Heart Fail. 2023, 25, 1352–1360. [Google Scholar] [CrossRef]
- Escobar, C.; Luis-Bonilla, J.; Crespo-Leiro, M.G.; Esteban-Fernández, A.; Farré, N.; Garcia, A.; Nuñez, J. Individualizing the treatment of patients with heart failure with reduced ejection fraction; a journey from hospitalization to long-term outpatient care. Expert. Opin. Pharmacother. 2022, 23, 1589–1599. [Google Scholar] [CrossRef]
- Rosano, G.M.C.; Moura, B.; Metra, M.; Böhm, M.; Bauersachs, J.; Ben Gal, T.; Adamopoulos, S.; Abdelhamid, M.; Bistola, V.; Čelutkienė, J.; et al. Patient profiling in heart failure for tailoring medical therapy. A consensus document of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2021, 23, 872–881. [Google Scholar] [CrossRef]
- Isaza, N.; Calvachi, P.; Raber, I.; Liu, C.L.; Bellows, B.K.; Hernandez, I.; Shen, C.; Gavin, M.C.; Garan, A.R.; Kazi, D.S. Cost-effectiveness of Dapagliflozin for the Treatment of Heart Failure with Reduced Ejection Fraction. JAMA Netw. Open 2021, 4, e2114501. [Google Scholar] [CrossRef]
- Wu, M.; Qin, S.; Wang, L.; Tan, C.; Peng, Y.; Zeng, X.; Luo, X.; Yi, L.; Wan, X. Economic Evaluation of Dapagliflozin in the Treatment of Patients with Heart Failure: A Systematic Review. Front. Pharmacol. 2022, 13, 860109. [Google Scholar] [CrossRef]
- Tang, Y.; Sang, H. Cost-utility analysis of add-on dapagliflozin in heart failure with preserved or mildly reduced ejection fraction. ESC Heart Fail. 2023, 10, 2524–2533. [Google Scholar] [CrossRef]
- Alnsasra, H.; Tsaban, G.; Solomon, A.; Khalil, F.; Aboalhasan, E.; Weinstein, J.M.; Azuri, J.; Hammerman, A.; Arbel, R. Effect of Dapagliflozin Versus Empagliflozin on Cardiovascular Death in Patients with Heart Failure Across the Spectrum of Ejection Fraction: Cost per Outcome Analysis. Am. J. Cardiovasc. Drugs 2023, 23, 323–328. [Google Scholar] [CrossRef]
- Parizo, J.T.; Goldhaber-Fiebert, J.D.; Salomon, J.A.; Khush, K.K.; Spertus, J.A.; Heidenreich, P.A.; Sandhu, A.T. Cost-effectiveness of Dapagliflozin for Treatment of Patients with Heart Failure with Reduced Ejection Fraction. JAMA Cardiol. 2021, 6, 926–935. [Google Scholar] [CrossRef] [PubMed]
- McEwan, P.; Darlington, O.; McMurray, J.J.V.; Jhund, P.S.; Docherty, K.F.; Böhm, M.; Petrie, M.C.; Bergenheim, K.; Qin, L. Cost-effectiveness of dapagliflozin as a treatment for heart failure with reduced ejection fraction: A multinational health-economic analysis of DAPA-HF. Eur. J. Heart Fail. 2020, 22, 2147–2156. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.J.H.; Chew, D.S.; Qin, L.; Fine, N.M.; Chen, J.; McMurray, J.J.V.; Howlett, J.G.; McEwan, P. Cost-effectiveness of immediate initiation of dapagliflozin in patients with a history of heart failure. Eur. J. Heart Fail. 2023, 25, 238–247. [Google Scholar] [CrossRef]
- Nguyen, B.N.; Mital, S.; Bugden, S.; Nguyen, H.V. Cost-effectiveness of dapagliflozin and empagliflozin for treatment of heart failure with reduced ejection fraction. Int. J. Cardiol. 2023, 376, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Escobar, C.; Barrios, V. SGLT 2 inhibitors: Searching for the best in class. Int. J. Cardiol. 2023, 384, 48–49. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Escobar, C.; Pascual-Figal, D.; Manzano, L.; Nuñez, J.; Camafort, M. Current Role of SLGT2 Inhibitors in the Management of the Whole Spectrum of Heart Failure: Focus on Dapagliflozin. J. Clin. Med. 2023, 12, 6798. https://doi.org/10.3390/jcm12216798
Escobar C, Pascual-Figal D, Manzano L, Nuñez J, Camafort M. Current Role of SLGT2 Inhibitors in the Management of the Whole Spectrum of Heart Failure: Focus on Dapagliflozin. Journal of Clinical Medicine. 2023; 12(21):6798. https://doi.org/10.3390/jcm12216798
Chicago/Turabian StyleEscobar, Carlos, Domingo Pascual-Figal, Luis Manzano, Julio Nuñez, and Miguel Camafort. 2023. "Current Role of SLGT2 Inhibitors in the Management of the Whole Spectrum of Heart Failure: Focus on Dapagliflozin" Journal of Clinical Medicine 12, no. 21: 6798. https://doi.org/10.3390/jcm12216798