
Epidemiology of Glucose-6-Phosphate Dehydrogenase Deficiency in Arab Countries: Insights from a Systematic Review
 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search Strategy
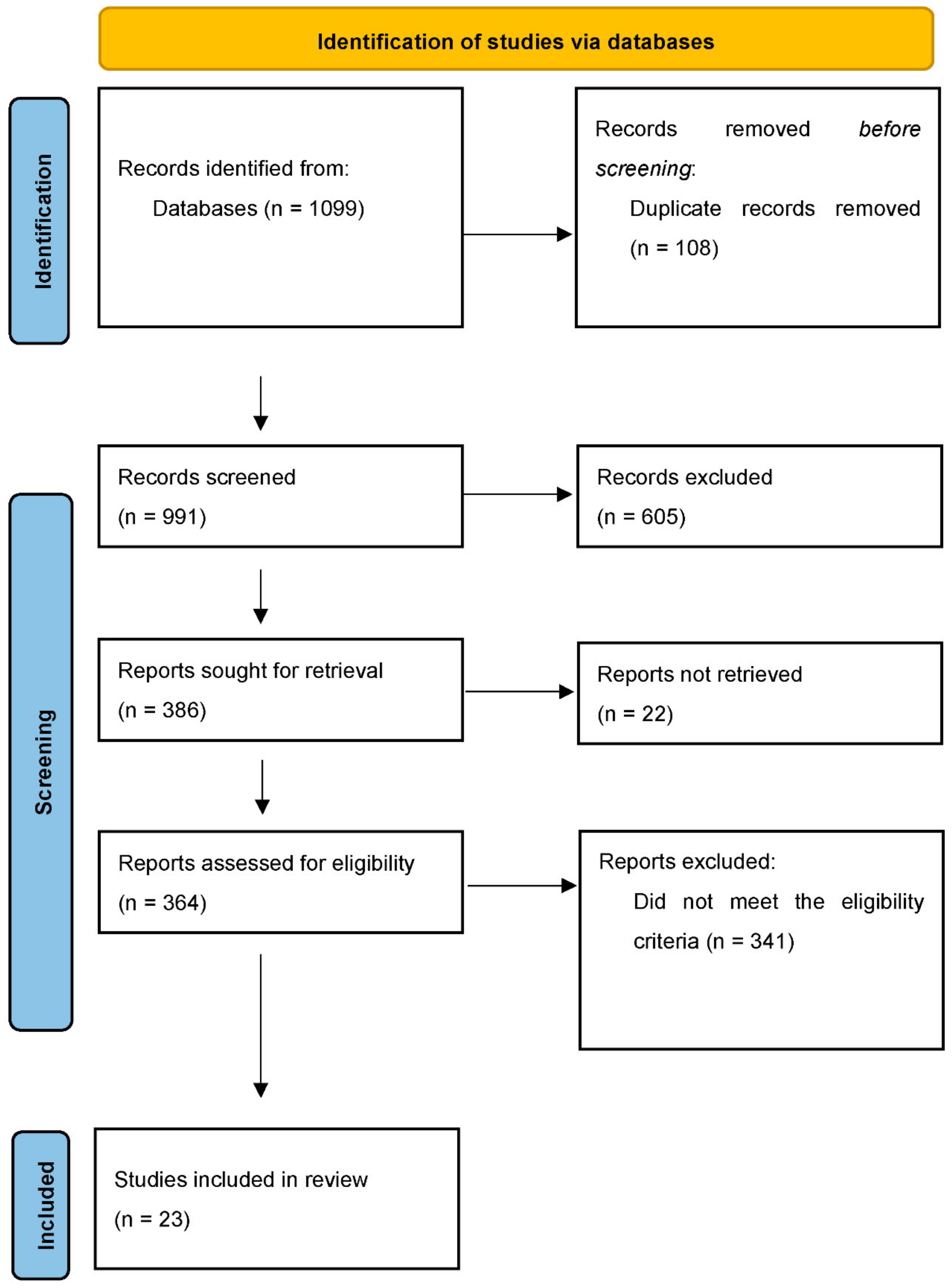
2.3. Study Selection
2.4. Process of Data Collection
3. Results
3.1. Study Characteristics
3.2. Epidemiology of G6PD Deficiency in Arab Countries: Key Findings
4. Discussion
Strengths and Limitations
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cappellini, M.D.; Fiorelli, G. Glucose-6-phosphate dehydrogenase deficiency. Lancet 2008, 371, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Luzzatto, L.; Arese, P. Favism and Glucose-6-Phosphate Dehydrogenase Deficiency. N. Engl. J. Med. 2018, 378, 1068–1069. [Google Scholar] [CrossRef] [PubMed]
- Luzzatto, L.; Nannelli, C.; Notaro, R. Glucose-6-Phosphate Dehydrogenase Deficiency. Hematol. Oncol. Clin. N. Am. 2016, 30, 373–393. [Google Scholar] [CrossRef]
- Luzzatto, L.; Ally, M.; Notaro, R. Glucose-6-phosphate dehydrogenase deficiency. Blood 2020, 136, 1225–1240. [Google Scholar] [CrossRef]
- Lee, H.Y.; Ithnin, A.; Azma, R.Z.; Othman, A.; Salvador, A.; Cheah, F.C. Glucose-6-Phosphate Dehydrogenase Deficiency and Neonatal Hyperbilirubinemia: Insights on Pathophysiology, Diagnosis, and Gene Variants in Disease Heterogeneity. Front. Pediatr. 2022, 10, 875877. [Google Scholar] [CrossRef] [PubMed]
- Mason, P.J. New insights into G6PD deficiency. Br. J. Haematol. 1996, 94, 585–591. [Google Scholar] [CrossRef]
- Nkhoma, E.T.; Poole, C.; Vannappagari, V.; Hall, S.A.; Beutler, E. The global prevalence of glucose-6-phosphate dehydrogenase deficiency: A systematic review and meta-analysis. Blood Cells Mol. Dis. 2009, 42, 267–278. [Google Scholar] [CrossRef]
- LaRue, N.; Kahn, M.; Murray, M.; Leader, B.T.; Bansil, P.; McGray, S.; Kalnoky, M.; Zhang, H.; Huang, H.; Jiang, H.; et al. Comparison of quantitative and qualitative tests for glucose-6-phosphate dehydrogenase deficiency. Am. J. Trop. Med. Hyg. 2014, 91, 854–861. [Google Scholar] [CrossRef]
- Fathi, A.; Barak, M.; Damandan, M.; Amani, F.; Moradpour, R.; Khalilova, I.; Valizadeh, M. Neonatal Screening for Glucose-6-phosphate dehydrogenase Deficiency in Ardabil Province, Iran, 2018–2019. Cell. Mol. Biomed. Rep. 2021, 1, 1–6. [Google Scholar] [CrossRef]
- DelFavero, J.J.; Jnah, A.J.; Newberry, D. Glucose-6-Phosphate Dehydrogenase Deficiency and the Benefits of Early Screening. Neonatal Netw. 2020, 39, 270–282. [Google Scholar] [CrossRef]
- Chiu, Y.H.; Chen, H.J.; Chang, Y.C.; Liu, Y.N.; Kao, S.M.; Liu, M.Y.; Weng, Y.Y.; Hsiao, K.J.; Liu, T.T. Applying a multiplexed primer extension method on dried blood spots increased the detection of carriers at risk of glucose-6-phosphate dehydrogenase deficiency in newborn screening program. Clin. Chim. Acta Int. J. Clin. Chem. 2019, 495, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- The EndNote Team. EndNote; EndNote 20; Clarivate: Philadelphia, PA, USA, 2013. [Google Scholar]
- Al Arrayed, S.; Hafadh, N.; Amin, S.; Al Mukhareq, H.; Sanad, H. Student screening for inherited blood disorders in Bahrain. EMHJ—East. Mediterr. Health J. 2003, 9, 344–352. [Google Scholar] [CrossRef]
- Dash, S. Hemoglobinopathies, G6PD deficiency, and hereditary elliptocytosis in Bahrain. Hum. Biol. 2004, 76, 779–783. [Google Scholar] [CrossRef]
- Abdel Fattah, M.; Abdel Ghany, E.; Adel, A.; Mosallam, D.; Kamal, S. Glucose-6-phosphate dehydrogenase and red cell pyruvate kinase deficiency in neonatal jaundice cases in egypt. Pediatr. Hematol. Oncol. 2010, 27, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Kasemy, Z.A.; Bahbah, W.A.; El Hefnawy, S.M.; Alkalash, S.H. Prevalence of and mothers’ knowledge, attitude and practice towards glucose-6-phosphate dehydrogenase deficiency among neonates with jaundice: A cross-sectional study. BMJ Open 2020, 10, e034079. [Google Scholar] [CrossRef]
- Elella, S.A.; Tawfik, M.; Barseem, N.; Moustafa, W. Prevalence of glucose-6-phosphate dehydrogenase deficiency in neonates in Egypt. Ann. Saudi Med. 2017, 37, 362–365. [Google Scholar] [CrossRef]
- Abo El Fotoh, M.W.M.; Rizk, M.S. Prevalence of glucose-6-phosphate dehydrogenase deficiency in jaundiced Egyptian neo-nates. J. Matern.-Fetal Neonatal Med. 2016, 29, 3834–3837. [Google Scholar] [CrossRef]
- Hagag, A.A.; Badraia, I.M.; Elfarargy, M.S.; Abd Elmageed, M.M.; Abo-Ali, E.A. Study of Glucose-6-Phosphate Dehydrogenase Deficiency: 5 Years Retrospective Egyptian Study. Endocr. Metab. Immune Disord. Drug Targets 2018, 18, 155–162. [Google Scholar] [CrossRef]
- Al-Mendalawi, M.D. Epidemiological, clinical and laboratory profile of glucose-6-phosphate dehydrogenase deficiency in the middle and north of Iraq: A comparative study. East. Mediterr. Health J. 2010, 16, 846–850. [Google Scholar] [CrossRef]
- Hilmi, F.A.; Al-Allawi, N.A.; Rassam, M.; Al-Shamma, G.; Al-Hashimi, A. Red cell glucose-6-phosphate dehydrogenase phenotypes in Iraq. East. Mediterr. Health J. 2002, 8, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.; Taha, J.; Al Naama, L.; Widad, N.; Jasim, S. Frequency of haemoglobinopathies and glucose-6-phosphate dehydrogenase deficiency in Basra. EMHJ—East. Mediterr. Health J. 2003, 9, 45–54. [Google Scholar] [CrossRef]
- Khneisser, I.; Adib, S.M.; Loiselet, J.; Mégarbané, A. Prevalence of G6PD deficiency and knowledge of diagnosis in a sample of previously unscreened Lebanese males: Clinical implications. J. Med. Screen. 2006, 13, 26–28. [Google Scholar] [CrossRef] [PubMed]
- Inati, A.; Abbas, H.A.; Boumitri, C.; Tecle, N. Prevalence of glucose-6-phosphate dehydrogenase deficiency among neonates at a tertiary care centre in Lebanon. J. Med. Screen. 2012, 19, 103–104. [Google Scholar] [CrossRef] [PubMed]
- Djigo, O.K.M.; Bollahi, M.A.; Hasni Ebou, M.; Ould Ahmedou Salem, M.S.; Tahar, R.; Bogreau, H.; Basco, L.; Ould Mohamed Salem Boukhary, A. Assessment of glucose-6-phosphate dehydrogenase activity using CareStart G6PD rapid diagnostic test and associated genetic variants in Plasmodium vivax malaria endemic setting in Mauritania. PLoS ONE 2019, 14, e0220977. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, G.S.; Lemine, S.M.; Cheibetta, S.; Mohamed, A. Dépistage néonatal du déficit en glucose 6 phosphate déshydrogénase (G6PD) en Mauritanie. Pan Afr. Med. J. 2018, 30, 224. [Google Scholar] [CrossRef]
- Al Riyami, A.; Suleiman, A.; Afifi, M.; Al Lamki, Z.; Daar, S. A community-based study of common hereditary blood disorders in Oman. EMHJ—East. Mediterr. Health J. 2001, 7, 1004–1011. [Google Scholar] [CrossRef]
- Alharbi, K.K.; Khan, I.A. Prevalence of glucose-6-phosphate dehydrogenase deficiency and the role of the A- variant in a Saudi population. J. Int. Med. Res. 2014, 42, 1161–1167. [Google Scholar] [CrossRef]
- Muzaffer, M.A. Neonatal screening of glucose-6-phosphate dehydrogenase deficiency in Yanbu, Saudi Arabia. J. Med. Screen. 2005, 12, 170–171. [Google Scholar] [CrossRef]
- Albagshi, M.H.; Alomran, S.; Sloma, S.; Albagshi, M.; Alsuweel, A.; AlKhalaf, H. Prevalence of Glucose-6-Phosphate Dehydrogenase Deficiency Among Children in Eastern Saudi Arabia. Cureus 2020, 12, e11235. [Google Scholar] [CrossRef]
- Ali Albsheer, M.M.; Lover, A.A.; Eltom, S.B.; Omereltinai, L.; Mohamed, N.; Muneer, M.S.; Mohamad, A.O.; Abdel Hamid, M.M. Prevalence of glucose-6-phosphate dehydrogenase deficiency (G6PDd), CareStart qualitative rapid diagnostic test performance, and genetic variants in two malaria-endemic areas in Sudan. PLoS Neglected Trop. Dis. 2021, 15, e0009720. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.J.; Dunn, E.V.; Berg, B.; Abdouni, S.F. A hematological survey of preschool children of the United Arab Emirates. Saudi Med. J. 2003, 24, 609–613. [Google Scholar]
- UY, H.; Yusoff, N. Prevalence of Glucose-6-Phosphate Dehydrogenase (G6PD) Deficiency (Favism) in Thamar Province-Republic of Yemen. Biohealth Sci. Bull. 2011, 3, 12–19. [Google Scholar]
- Abdul-Ghani, R.; Mahdy, M.A.; Saif-Ali, R.; Alkubati, S.A.; Alqubaty, A.R.; Al-Mikhlafy, A.A.; Al-Eryani, S.M.; Al-Mekhlafi, A.M.; Alhaj, A. Glucose-6-phosphate dehydrogenase deficiency among Yemeni children residing in malaria-endemic areas of Hodeidah governorate and evaluation of a rapid diagnostic test for its detection. Malar. J. 2016, 15, 327. [Google Scholar] [CrossRef]
- Al-Nood, H.A. Thalassaemia and glucose-6-phosphate dehydrogenase deficiency in sickle-cell disorder patients in Taiz, Yemen. East. Mediterr. Health J. 2011, 17, 404–408. [Google Scholar] [CrossRef]
- Harcke, S.J.; Rizzolo, D.; Harcke, H.T. G6PD deficiency: An update. JAAPA Off. J. Am. Acad. Physician Assist. 2019, 32, 21–26. [Google Scholar] [CrossRef]
- Sparrow, R.L. Red blood cell components: Time to revisit the sources of variability. Blood Transfus. 2017, 15, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Ainoon, O.; Alawiyah, A.; Yu, Y.H.; Cheong, S.K.; Hamidah, N.H.; Boo, N.Y.; Zaleha, M. Semiquantitative screening test for G6PD deficiency detects severe deficiency but misses a substantial proportion of partially-deficient females. Southeast Asian J. Trop. Med. Public Health 2003, 34, 405–414. [Google Scholar]
- Gómez-Manzo, S.; Marcial-Quino, J.; Vanoye-Carlo, A.; Serrano-Posada, H.; Ortega-Cuellar, D.; González-Valdez, A.; Castillo-Rodríguez, R.A.; Hernández-Ochoa, B.; Sierra-Palacios, E.; Rodríguez-Bustamante, E.; et al. Glucose-6-Phosphate Dehydrogenase: Update and Analysis of New Mutations around the World. Int. J. Mol. Sci. 2016, 17, 2069. [Google Scholar] [CrossRef] [PubMed]
- Bener, A.; Alali, K.A. Consanguineous marriage in a newly developed country: The Qatari population. J. Biosoc. Sci. 2006, 38, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Bittles, A.H.; Hamamy, H.A. Endogamy and consanguineous marriage in Arab populations. In Genetic Disorders among Arab Populations; Springer: Berlin/Heidelberg, Germany, 2010; pp. 85–108. [Google Scholar]
- Akrami, S.M.; Osati, Z. Is consanguineous marriage religiously encouraged? Islamic and Iranian considerations. J. Biosoc. Sci. 2007, 39, 313–316. [Google Scholar] [CrossRef] [PubMed]
- WHO Working Group. Glucose-6-phosphate dehydrogenase deficiency. Bull. World Health Organ. 1989, 67, 601–611. [Google Scholar]


{kind=link}
| Author | Year | Country | Study Design | Sample Size | Target Population | Age |
|---|---|---|---|---|---|---|
| Al-Arrayed et al. | 2003 | Bahrain | Cross-sectional | 5686 | 11th-grade students from 38 schools | 16–17 years |
| Dash et al. | 2004 | Bahrain | Hospital-based study | 4173 newborns, 15,827 adults | Bahrainis visiting the Salmaniya Medical Complex and various health centers of the Ministry of Health. | Not specified |
| Fattah et al. | 2010 | Egypt | Case-series study | 69 | Neonates with pathological indirect hyperbilirubinemia | 36.78 ± 1.92 weeks |
| Kasemy et al. | 2019 | Egypt | Cross-sectional | 487 | Neonates with Jaundice | 4.45 ± 0.86 days |
| Elella et al. | 2017 | Egypt | Cross-sectional | 2782 | Infants born during 2015 | Under one year |
| El Fotoh et al. | 2016 | Egypt | Prospective cross-sectional | 202 | Neonates with indirect hyperbilirubinemia | 3.7 ± 2.5 days |
| Hagag et al. | 2017 | Egypt | Retrospective study | 1000 | Patients with G6PD deficiency anemia | 22.8 ± 15.54 |
| Al-Mendalawi et al. | 2010 | Iraq | Cross-sectional | 156 | Children under 5 years | 2.8 ± 1.2 years |
| Hilmi et al. | 2002 | Iraq | Cross-sectional | 758 | 121 medical students and 69 hospital staff members (All males) | 18–60 years |
| Hassan et al. | 2003 | Iraq | Cross-sectional | 1064 | Couples aged 14–60 years attending a primary health care department | 14–60 years |
| Khneisser et al. | 2006 | Lebanon | Community-based survey | 3000 | Men | 14 years and above |
| Inati et al. | 2012 | Lebanon | Cross-sectional | 3009 | neonates | <1 month |
| Djigo et al. | 2019 | Mauritania | Cross-sectional | 443 | Healthy blood donors | Median age: 30 years (18–61) |
| Mohamed et al. | 2018 | Mauritania | Cross-sectional | 523 | Newborns | <1 month |
| AL-Riyami et al. | 2001 | Oman | Community-based study | 6342 | The general population (children) | 0–5 years |
| Alharbi et al. | 2014 | Saudi Arabia | Cross-sectional | 2100 | Saudi Men | 43 ± 10.05 |
| Muzaffer et al. | 2005 | Saudi Arabia | Hospital-based study | 2505 | Newborns | <1 month |
| Albagshi et al. | 2020 | Saudi Arabia | Retrospective study | 48,889 | Children 0–14 years | 1.93 ± 3.98 |
| Albsheer et al. | 2021 | Sudan | Cross-sectional | 557 | The general population from New Halfa and Khartum | 34.2 ±15.6 |
| Miller et al. | 2000 | UAE | Cross-sectional community-based survey | 496 | Emirati children | 12–71 months |
| Hussein et al. | 2011 | Yemen | Cross-sectional | 90 | Adult individuals | 22 years |
| Ghani et al. | 2016 | Yemen | Cross-sectional | 400 | Children residing in the malaria endemic areas of the Hodeidah governate | Eight years (6–11 years) |
| Al Nood | 2009 | Yemen | Pilot study | 31 | Patients with sickle cell trait | 6 months–18 years |
| Author | Prevalence | Gender-Specific Prevalence | Risk Factors | Key Findings |
|---|---|---|---|---|
| Al-Arrayed et al. | 23.2% for G6PD deficiency and 1.9% G6PD deficiency carriers | Males: 11.4% | Not studied | Prevalence was higher among geographic regions such as Sitara (45%), the western region (36%), Jidhafs (34%), the northern region (31%), and the central region (31%). Prevalence was lower in areas such as Isa (17%), Muharraq (11%), Riffa (8%), and Hidd (5%). Among those who were G6PD deficient, 55% were females, compared to 45% were males. |
| Females: 11.9% | ||||
| Dash et al. | G6PD deficiency was detected in 31.3% of the sample | G6PD deficiency among males: 40.6% | Gender and sickle cell anemia | The prevalence in Bahrain is the highest reported prevalence in the region, with twice the prevalence in males than females and 1.4 times more in study subjects with sickle hemoglobin. |
| Females: 23.1% | ||||
| G6PD deficiency M: F ratio: 1.8:1 | ||||
| Fattah et al. | 14.40% | 21.2% in males, with a significantly higher proportion in males than females (0.01). Male to female ratio was 2.33:1. | Gender | Isolated G6PD deficiency was detected in 10% of neonates, mild deficiency was found in one patient, and three patients each had moderate and severe deficiency. |
| Kasemy et al. | 10.10% | Males were 9.54 times more likely to develop deficiency than females. | Male gender, family history, and consanguinity | Mothers’ perceptions of G6PD deficiency were very low, and 17.10% had knowledge about G6PD deficiency. About 45% had a positive attitude toward G6PD deficiency, and 19.9% had good practice toward G6PD deficiency. |
| Elella et al. | 4.3% (119 infants) had G6PD deficiency, and 0.6% had an intermediate deficiency | Male to female ratio of 3.2:1. | Not studied | About 6% (91) of males and 2.1% (28) of females had G6PD deficiency. Enzyme activity was significantly higher among males than females (p < 0.01) |
| El Fotoh et al. | 8.9% had G6PD deficiency | All males were G6PD deficient (100%) | Gender | The mean serum bilirubin of G6PD deficient cases was 17.2 ±4.4. A significant positive correlation was found between the time of appearance of jaundice in days and G6PD levels in deficient cases. |
| Hagag et al. | 93.2% in males and 6.8% in females. | Males (932) were more commonly affected than females (68) | Gender. Diet and infections were the common causes of hemolysis | A high prevalence of hemolytic crisis in g6PD deficiency was found among children 1–3 years old with a mean age of 22.8 ± 15.54 months. Fava beans and falafel were the most common foods causing hemolysis, followed by chickpeas, broad beans, and green peas |
| Al-Mendalawi et al. | Not applicable, as all patients included had G6PD deficiency | The ratio of males to females was 1.6:1 in Baghdad and 3.4:1 in Mosul | Family history and male gender | Family history was positive in 19.2% of the patients in Baghdad and 13.6% in Mosul. |
| Hilmi et al. | 6.10% | Not applicable, as all were males | Not studied | The prominent non-deficient G6PD phenotype was G6PD B (92.6%), and 1.3% had G6PD A+. The presence of a substantial number of the non-Mediterranean variant was unexpected and perhaps related to the more heterogenous background of the Iraqi people. With respect to ethnicity, 6% of Arabs, 8.8% of Kurds, and 5.6% of Turkomans were G6PD-deficient. |
| Hassan et al. | 12.50% | Males: 15.3% | Not studied | The prevalence of G6PD deficiency ranged from 11.4% in Al-Madina to 16.1% in Abua al-Khasib. |
| Khneisser et al. | Cumulative incidence rate: 12/1000 or 1.2% | Not applicable, as all were males | Not studied | Cases of G6PD deficiency were younger than the rest of the participants. |
| Of those who were affected, 77.8% were aware of their problem since they were affected, and 22.2% were not aware of their problem. | ||||
| Inati et al. | 2.10% | Males: 3.1% | Male gender and Muslims | There was a higher prevalence of G6PD deficiency among Muslims (2.6%) than among Christians (1.3%), as consanguinity is more common in Muslims. |
| Females: 0.9% | ||||
| Djigo et al. | 11.30% | Males: 11.8% | Not studied | Among males, Black Africans had the highest prevalence of G6PD deficiency (15%), and 5.9% of White Moors were deficient. |
| Females: 3.7% | ||||
| Mohamed et al. | 11.09% | Males: 15% | Black children and males | G6PD deficiency was more common in males than females (p = 0.007); also, Black children (15%) had a higher prevalence of G6PD deficiency than White children (8%). |
| Females: 7% | ||||
| AL-Riyami et al. | 18.80% | Males: 27% | Gender and geographic region | There were no differences in the prevalence by age, but males had a higher prevalence than females. Also, prevalence varied according to the geographic region, with a higher prevalence in Al Dakhiliyah, followed by South Batinah, Muscat, and North Batinah. |
| Females: 11% | ||||
| Alharbi et al. | 4.76% | Not applicable, as all were males | Not studied | In total, 100 males (4.76%) were found to have G6PD deficiency. The G6PD A-mutation was present in 2% of the 100 subjects who were G6PD deficient. However, there was no significant difference in the frequency of this mutation between men with and without G6PD deficiency. |
| Muzaffer et al. | 2% | Males: 3.05% | Male sex | Six babies (5 males and 1 female) developed neonatal jaundice |
| Females: 0.9% | ||||
| Male to female ratio: 3:1 | ||||
| Albagshi et al. | 25% | Males: 33.8% | Male sex | The overall prevalence among all pediatric patients was 25%, whereas it was 18.8% in newborns, with a higher prevalence among males in both newborns and other kids. |
| Females: 13.2% | ||||
| Albsheer et al. | Low-to-moderate but with high heterogeneity. 5.5–27.3% | Males: Median G6PD activity is 4.2 compared to 4.3 in females. | Body weight, region, and use of antibiotics were studied, and body weight was found to be a significant protective factor | 5.5% had severe or moderately severe G6PD deficiency. One kg increase in body weight lowered the OR of being G6PD deficient by 3%. |
| Miller et al. | 9.10% | One out of five were females, and one out of four were males | Not studied | Hereditary disorders, mainly G6PD deficiency, are common in Emirati children. G6PD deficiency was more common among male Emirati children than females. |
| Hussein et al. | 14.50% | Among those who were deficient, 75.5% were males, and 24.5% females | Not studied | 53.8% of the adults had a WHO class-II enzyme variant, 46.2% had a class-III variant, and no class-V variant was detected. Whereas 85.5% showed normal enzyme activity |
| Ghani et al. | Prevalence varied between 2.3–12.0% depending upon two varying cut-offs of ≤60 and ≤10%, respectively | Males: 2.7–14.2% | Male gender, district of residence and consanguineous marriage | 12.1% of children were G6PD deficient, and 2.3% were severely deficient. |
| Females: 1.7–9.4% | Males had a higher prevalence of G6PD deficiency at all cut-off values with significant differences at <20–40% of normal activity | |||
| Al Nood | 22.60% | Not reported | Not studied | The burden of G6PD deficiency was high among patients with sickle cell anemia. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alangari, A.S.; El-Metwally, A.A.; Alanazi, A.; Al Khateeb, B.F.; Al Kadri, H.M.; Alshdoukhi, I.F.; Aldubikhi, A.I.; Alruwaili, M.; Alshahrani, A. Epidemiology of Glucose-6-Phosphate Dehydrogenase Deficiency in Arab Countries: Insights from a Systematic Review. J. Clin. Med. 2023, 12, 6648. https://doi.org/10.3390/jcm12206648
Alangari AS, El-Metwally AA, Alanazi A, Al Khateeb BF, Al Kadri HM, Alshdoukhi IF, Aldubikhi AI, Alruwaili M, Alshahrani A. Epidemiology of Glucose-6-Phosphate Dehydrogenase Deficiency in Arab Countries: Insights from a Systematic Review. Journal of Clinical Medicine. 2023; 12(20):6648. https://doi.org/10.3390/jcm12206648
Chicago/Turabian StyleAlangari, Abdulaziz S., Ashraf A. El-Metwally, Abdullah Alanazi, Badr F. Al Khateeb, Hanan M. Al Kadri, Ibtehaj F. Alshdoukhi, Aljohrah I. Aldubikhi, Muzun Alruwaili, and Awad Alshahrani. 2023. "Epidemiology of Glucose-6-Phosphate Dehydrogenase Deficiency in Arab Countries: Insights from a Systematic Review" Journal of Clinical Medicine 12, no. 20: 6648. https://doi.org/10.3390/jcm12206648