
Efficacy of a Cognitive Behavioral Intervention for the Prevention of Depression in Nonprofessional Caregivers Administered through a Smartphone App: A Randomized Controlled Trial
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
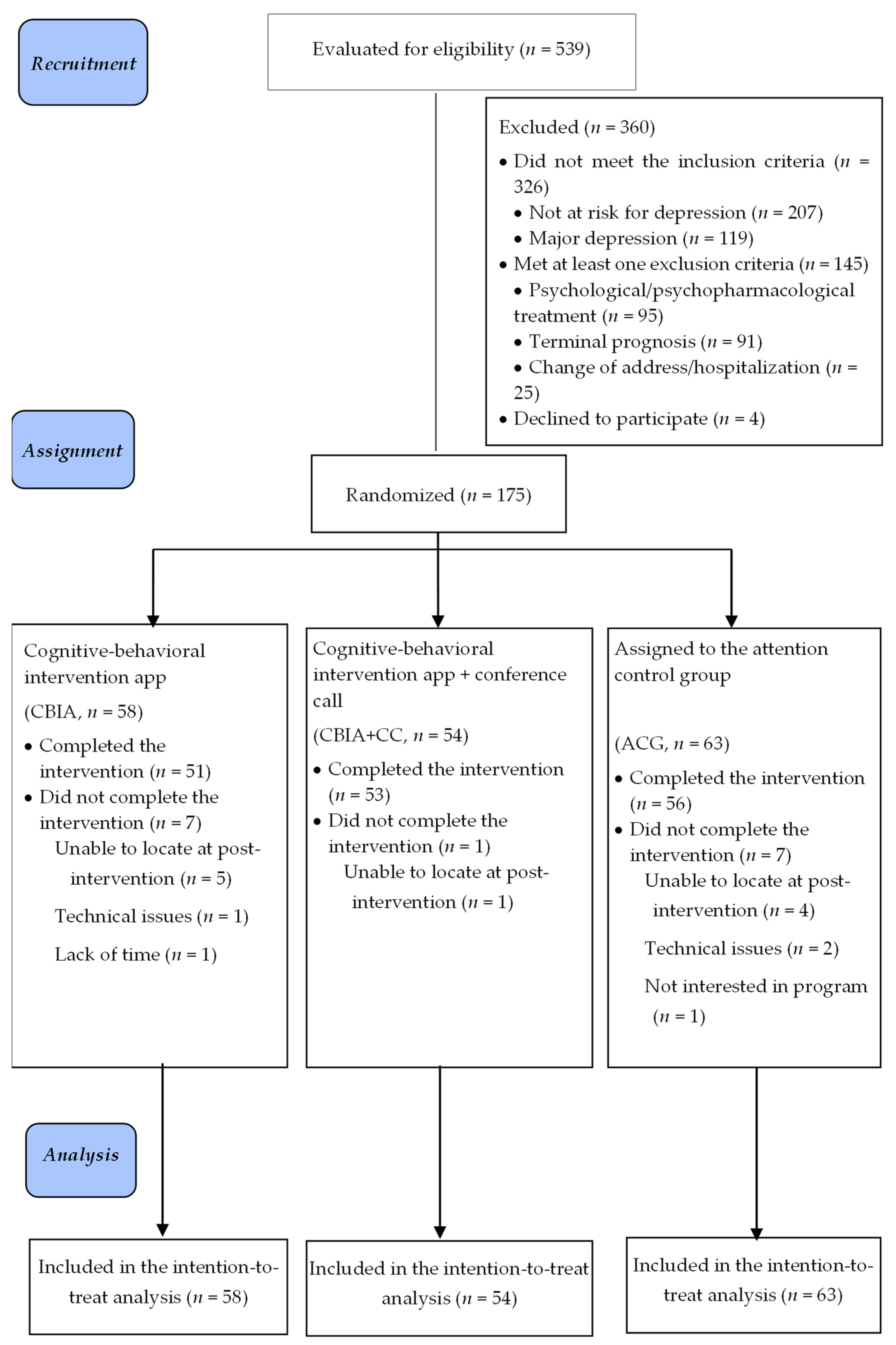
2.1. Design
2.2. Participants
2.3. Sample Size
2.4. Instruments
2.5. Intervention and Control Groups
2.6. Data Analysis
3. Results
3.1. Characteristics of the Participants
3.2. Incidence of Depression
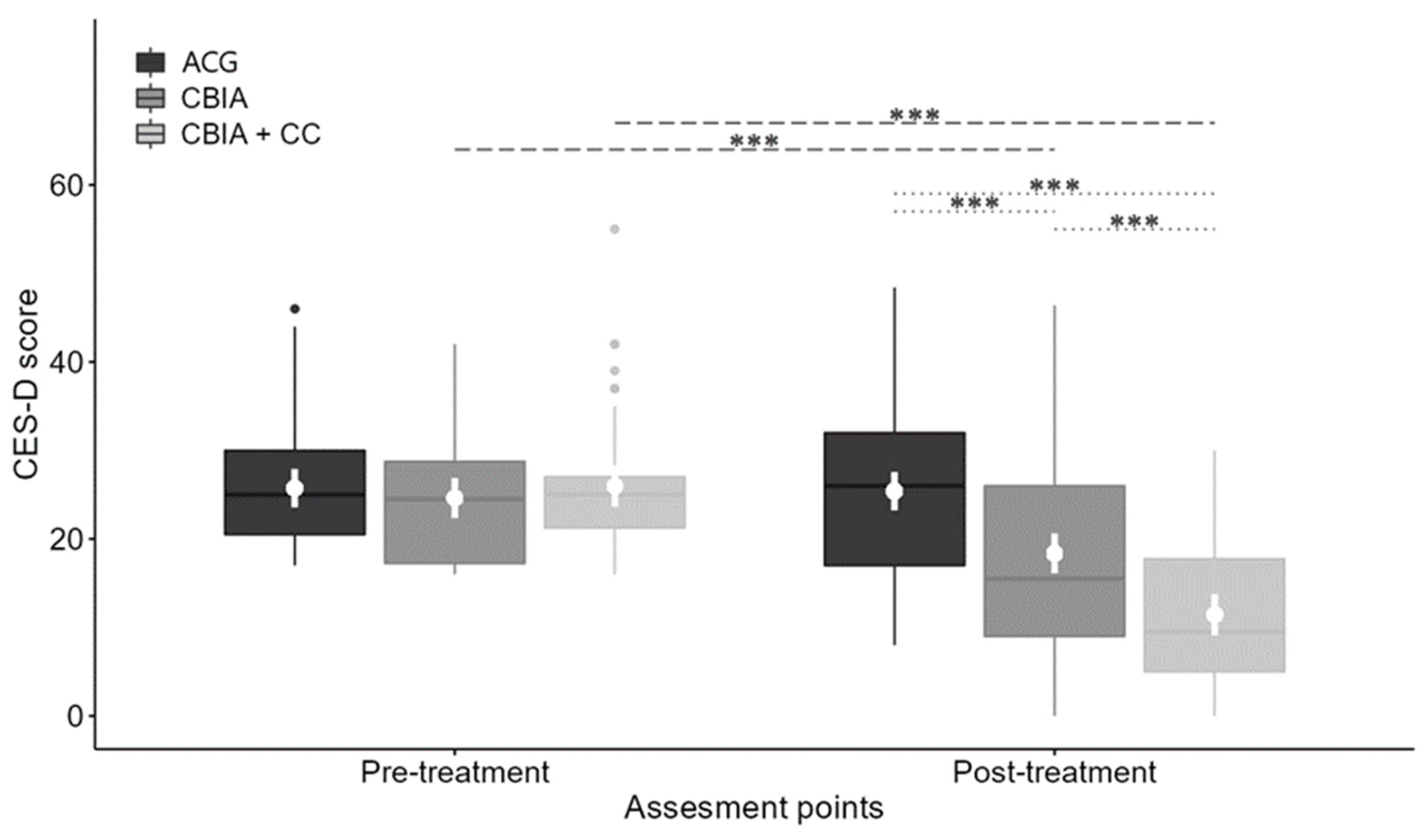
3.3. Depressive Symptoms
3.4. Impact of Caregiver Age and Years Caring on Depressive Symptoms
3.5. Acceptability and Satisfaction
Adherence as a Potential Moderator of the Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. International Classification of Functioning, Disability and Health (ICF); WHO: Geneva, Switzerland, 2001. [Google Scholar]
- World Health Organization. World Report on Disability; WHO and The World Bank: Geneva, Switzerland, 2011. [Google Scholar]
- Hosseinpoor, A.R.; Bergen, N.; Kostanjsek, N.; Kowal, P.; Officer, A.; Chatterji, S. Socio-demographic patterns of disability among older adult populations of low-income and middle-income countries: Results from World Health Survey. Int. J. Public Health 2016, 61, 337–354. [Google Scholar] [CrossRef] [PubMed]
- Triantafillou, J.; Naiditch, M.; Repkova, K.; Stiehr, K.; Carretero, S.; Emilsson, T.; Vlantoni, D. Informal Care in the Long-Term Care System; European Overview Paper; European Centre for Social Welfare Policy and Research: Athens, Greece; Vienna, Austria, 2010; Available online: https://www.euro.centre.org/downloads/detail/768 (accessed on 10 May 2023).
- Verbakel, E.; Tamlagsrønning, S.; Winstone, L.; Fjær, E.L.; Eikemo, T.A. Informal care in Europe: Findings from the European Social Survey (2014) special module on the social determinants of health. Eur. J. Public Health 2017, 27, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Bom, J.; Bakx, P.; Schut, F.; van Doorslaer, E. The impact of informal caregiving for older adults on the health of various types of caregivers: A systematic review. Gerontologist 2019, 59, e629–e642. [Google Scholar] [CrossRef]
- Sallim, A.B.; Sayampanathan, A.A.; Cuttilan, A.; Ho, R. Prevalence of mental health disorders among caregivers of patients with Alzheimer Disease. JAMDA 2015, 16, 1034–1041. [Google Scholar] [CrossRef]
- Cuijpers, P. Depressive disorders in caregivers of dementia patients: A systematic review. Aging Ment. Health 2005, 9, 325–330. [Google Scholar] [CrossRef]
- Del-Pino-Casado, R.; Rodríguez, M.; López-Martínez, C.; Orgeta, V. The association between subjective caregiver burden and depressive symptoms in carers of older relatives: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0217648. [Google Scholar] [CrossRef] [PubMed]
- Mausbach, B.T.; Chattillion, E.A.; Moore, R.C.; Roepke, S.K.; Depp, C.A.; Roesch, S. Activity restriction and depression in medical patients and their caregivers: A meta-analysis. Clin. Psychol. Rev. 2011, 31, 900–908. [Google Scholar] [CrossRef]
- Geng, H.-M.; Chuang, D.-M.; Yang, F.; Yang, Y.; Liu, W.-M.; Liu, L.-H.; Tian, H.-M. Prevalence and determinants of depression in caregivers of cancer patients: A systematic review and meta-analysis. Medicine 2018, 97, e11863. [Google Scholar] [CrossRef]
- Loh, A.Z.; Tan, J.S.; Zhang, M.W.; Ho, R.C. The global prevalence of anxiety and depressive symptoms among caregivers of stroke survivors. JAMDA 2017, 18, 111–116. [Google Scholar] [CrossRef]
- World Health Organization. Preventing Depression in the WHO European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- MacNeil, G.; Kosberg, J.I.; Durkin, D.W.; Dooley, W.K.; DeCoster, J.; Williamson, G.M. Caregiver mental health and potentially harmful caregiving behavior: The central role of caregiver anger. Gerontologist 2010, 50, 76–86. [Google Scholar] [CrossRef]
- Muñoz, R.; Cuijpers, P.; Smit, F.; Barrera, A.; Leykin, Y. Prevention of major depression. Annu. Rev. Clin. Psychol. 2010, 6, 181–212. [Google Scholar] [CrossRef]
- Vázquez, F.L.; Otero, P.; Torres, Á.; Hermida, E.; Blanco, V.; Díaz, O. A brief problem-solving indicated-prevention intervention for prevention of depression in nonprofessional caregivers. Psicothema 2013, 25, 87–92. [Google Scholar]
- Vázquez, F.L.; Hermida, E.; Torres, A.; Otero, P.; Blanco, V.; Díaz, O. Efficacy of a cognitive-behavioral preventive intervention in caregivers with elevated depressive symptoms. Psicol. Conduct. 2014, 22, 79–96. [Google Scholar]
- Vázquez, F.L.; Torres, Á.; Blanco, V.; Otero, P.; Díaz, O.; Ferraces, M.J. Long-term follow-up of a randomized clinical trial assessing the efficacy of a brief cognitive-behavioral depression prevention intervention for caregivers with elevated depressive symptoms. Am. J. Geriatr. Psychiatry 2016, 24, 421–432. [Google Scholar] [CrossRef]
- Vázquez, F.L.; López, L.; Torres, Á.J.; Otero, P.; Blanco, V.; Díaz, O.; Páramo, M. Analysis of the components of a cognitive-behavioral intervention for the prevention of depression administered via conference call to nonprofessional caregivers: A randomized controlled trial. Int. J. Environ. Res. Public Health 2020, 17, 2067. [Google Scholar] [CrossRef]
- International Telecommunication Union. Measuring Digital Development. Facts and Figures 2021; International Telecommunication Union: Geneva, Switzerland, 2021. [Google Scholar]
- Deady, M.; Glozier, N.; Calvo, R.; Johnston, D.; Mackinnon, A.; Milne, D.; Choi, I.; Gayed, A.; Peters, D.; Bryant, R.; et al. Preventing depression using a smartphone app: A randomized controlled trial. Psychol. Med. 2022, 52, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Fuller-Tyszkiewicz, M.; Richardson, B.; Little, K.; Teague, S.; Hartley-Clark, L.; Capic, T.; Khor, S.; Cummins, R.A.; Olsson, C.A.; Hutchinson, D. Efficacy of a smartphone app intervention for reducing caregiver stress: Randomized controlled trial. JMIR Ment. Health 2020, 7, e17541. [Google Scholar] [CrossRef] [PubMed]
- Fleming, T.; Bavin, L.; Lucassen, M.; Stasiak, K.; Hopkins, S.; Merry, S. Beyond the trial: Systematic review of real-world uptake and engagement with digital self-help interventions for depression, low mood, or anxiety. JMIR 2018, 20, 11. [Google Scholar] [CrossRef]
- Rismawan, W.; Marchira, C.R.; Rahmat, I. Usability, acceptability, and adherence rates of mobile application interventions for prevention or treatment of depression: A systematic review. J. Psychosoc. Nurs. Ment. 2021, 59, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Arean, P.A.; Hallgren, K.A.; Jordan, J.T.; Gazzaley, A.; Atkins, D.C.; Heagerty, P.J.; Anguera, J.A. The use and effectiveness of mobile apps for depression: Results from a fully remote clinical trial. JMIR 2016, 18, e330. [Google Scholar] [CrossRef]
- Andersson, G.; Cuijpers, P. Internet-based and other computerized psychological treatments for adult depression: A meta-analysis. Cogn. Behav. Ther. 2009, 38, 196–205. [Google Scholar] [CrossRef]
- Brouwer, W.; Kroeze, W.; Crutzen, R.; de Nooijer, J.; de Vries, N.K.; Brug, J.; Oenema, A. Which intervention characteristics are related to more exposure to internet-delivered healthy lifestyle promotion interventions? A systematic review. JMIR 2011, 13, e2. [Google Scholar] [CrossRef]
- Muñoz, R.F.; Leykin, Y.; Barrera, A.Z.; Brown, C.H.; Bunge, E.L. The impact of phone calls on follow-up rates in an online depression prevention study. Internet Interv. 2017, 8, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Miltenberger, R.G. Behavior Modification: Principles and Procedures, 5th ed.; Thomson Learning: Wadsworth, OH, USA, 2012. [Google Scholar]
- Asplund, R.; Dagöö, J.; Fjellström, I.; Niemi, L.; Hansson, K.; Zeraati, F.; Ziuzina, M.; Geraedts, A.; Ljótsson, B.; Carlbring, P.; et al. Internet-based stress management for distressed managers: Results from a randomised controlled trial. Occup. Environ. Med. 2018, 75, 105–113. [Google Scholar] [CrossRef]
- Vázquez, F.L.; Torres, Á.; Díaz, O.; Páramo, M.; Otero, P.; Blanco, V.; López, L. Cognitive behavioral intervention via a smartphone app for non-professional caregivers with depressive symptoms: Study protocol for a randomized controlled trial. Trials 2018, 19, 414. [Google Scholar] [CrossRef] [PubMed]
- Vázquez, F.L.; Blanco, V.; López, M. An adaptation of the Center for Epidemiologic Studies Depression Scale for use in non-psychiatric Spanish populations. Psychiatry Res. 2007, 149, 247–252. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5); American Psychiatric Publishing: Arlington, TX, USA, 2013. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Ly, K.H.; Trüschel, A.; Jarl, L.; Magnusson, S.; Windahl, T.; Johansson, R.; Carlbring, P.; Andersson, G. Behavioural activation versus mindfulness-based guided self-help treatment administered through a smartphone application: A randomised controlled trial. BMJ Open 2014, 4, e003440. [Google Scholar] [CrossRef]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. Structured Clinical Interview for DSM-5®—Clinician Version (SCID-5-CV); American Psychiatric Association Publishing: Washington, DC, USA, 2015. [Google Scholar]
- Osório, F.L.; Loureiro, S.R.; Hallak, J.E.C.; Machado-de-Sousa, J.P.; Ushirohira, J.M.; Baes, C.V.W.; Apolinario, T.D.; Donadon, M.F.; Bolsoni, L.M.; Guimarães, T.; et al. Clinical validity and intrarater and test-retest reliability of the Structured Clinical Interview for DSM-5—Clinician Version (SCID-5-CV). Psychiatry Clin. Neurosci. 2019, 73, 754–760. [Google Scholar] [CrossRef]
- Vázquez, F.L.; Torres, Á.; Otero, P.; Blanco, V.; Clifford, C. Psychometric properties of the castilian spanish version of the Client Satisfaction Questionnaire (CSQ-8). Curr. Psychol. 2019, 38, 829–835. [Google Scholar] [CrossRef]
- Blanco, V.; Otero, P.; Vázquez, F.L. A pilot study for a smartphone app for the prevention of depression in non-professional caregivers. Aging Ment. Health 2023, 27, 166–175. [Google Scholar] [CrossRef]
- Lewinsohn, P.M.; Hoberman, H.; Teri, L.; Hautzinger, M. An integrative theory of depression. In Theoretical Issues in Behaviour Therapy; Reiss, S., Bootzin, R.R., Eds.; Academic Press: Orlando, FL, USA, 1985; pp. 331–359. [Google Scholar]
- International Business Machines [IBM] Corporation. IBM SPSS Statistics for Windows, Version 27.0; IBM Corporation: Armonk, NY, USA, 2020. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 10 May 2023).
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomized trials. Ann. Intern. Med. 2010, 152, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Honaker, J.; King, G.; Blackwell, M. Amelia II: A program for missing data. J. Stat. Softw. 2011, 45, 1–47. [Google Scholar] [CrossRef]
- Robitzsch, A.; Grund, S.; Henke, T. Miceadds: Some Additional Multiple Imputation Functions, Especially for Mice; R Package Version 2.12-24. 2018. Available online: https://CRAN.R-project.org/package=miceadds (accessed on 15 May 2023).
- Van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Sackett, D.L.M.; Cook, D.J. User’s guides to the medical literature, II. How to use an article about therapy or prevention. What were the results and will they help me in caring for my patients? JAMA 1994, 271, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Bender, R. Calculating Confidence Intervals for the Number Needed to Treat. Control. Clin. Trials 2001, 22, 102–110. [Google Scholar] [CrossRef]
- Newcombe, R.G. Interval estimation for the difference between independent proportions: Comparison of eleven methods. Stat. Med. 1998, 17, 873–890. [Google Scholar] [CrossRef]
- Jiang, J. Linear and Generalized Linear Mixed Models and Their Applications; Springer: Berlin, Germany, 2007. [Google Scholar]
- Pinheiro, J.C.; Bates, D.M. Mixed-Effects Models in S and S-Plus; Springer: Berlin, Germany, 2000. [Google Scholar]
- Enders, C.K. Applied Missing Data Analysis; Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Cliff, N. Ordinal Methods for Behavioral Data Analysis; Routledge: London, UK, 1996. [Google Scholar]
- Romano, J.; Kromrey, J.D.; Coraggio, J.; Skowronek, J. Appropriate statistics for ordinal level data: Should we really be using t-test and Cohen’s d for evaluating group differences on the NSSE and other surveys? In Proceedings of the Annual Meeting of the Florida Association of Institutional Research, New Orleans, FL, USA, 1–3 February 2006. [Google Scholar]
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; John Wiley and Sons: New York, NY, USA, 1987. [Google Scholar]
- Kraemer, H.C.; Blasey, C.M. Centring in regression analyses: A strategy to prevent errors in statistical inference. Int. J. Methods Psychiatr. Res. 2004, 13, 141–151. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Torres, A.; Vázquez, F.; Blanco, V.; Otero, P.; López, L.; Vázquez, F.L. Depression and its correlates in non-professional female caregivers caring for dependent persons. In Caregiving: Perspectives, Experiences and Challenges; Eleuteri, S., Ed.; NovaScience Publishers: New York, NY, USA, 2020; pp. 23–65. [Google Scholar]
- Crespo, M.; López, J. El Apoyo a Los Cuidadores de Familiares Mayores Dependientes en el Hogar: Desarrollo del Programa “Cómo Mantener su Bienestar” [Support to the Caregivers of Dependent Family Members at Home: Development of the Program “How to Maintain Their Wellbeing”]; Spanish Ministry of Work and Social Issues: Madrid, Spain, 2007.
- White, M.; Dorman, S.M. Receiving social support online: Implications for health education. Health Educ. Res. 2001, 16, 693–707. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Module | Contents |
|---|---|
| Module 1 | Introduction of group members Aim of the program Information on depression and active coping Mood scoring Diaphragmatic breathing training Self-reinforcement Intersession tasks: mood rating, practicing breathing techniques, and self-reinforcement |
| Module 2 | Explanation of the relationship between activities and mood Guidelines and strategies for increasing pleasurable activities Planning of enjoyable activities Behavior contract Intersession tasks: mood rating, practicing breathing techniques, self-reinforcement, and doing planned pleasurable activities |
| Module 3 | Explanation of the relationship between thoughts and mood Thought management techniques (direct approach, priming, and distraction) Planning of enjoyable activities Behavior contract Intersession tasks: mood rating, practicing breathing techniques, self-reinforcement, doing planned pleasurable activities, and practicing thought management techniques |
| Module 4 | Explanation of the relationship between social contact and mood Strategies to increase and improve social relationships Planning enjoyable and social activities Intersession tasks: mood rating, practicing breathing techniques, self-reinforcement, doing planned pleasurable activities, practicing thought management techniques, and making social contact |
| Module 5 | Review of what has been learned. Maintain progress Relapse prevention Good-bye and wrap-up |
| Characteristics | Total (n = 175) | CBIA (n = 58) | CBIA + CC (n = 54) | ACG (n = 63) |
|---|---|---|---|---|
| Caregiver Characteristics | ||||
| Sex, n (%) | ||||
| Female | 162 (92.6) | 52 (89.7) | 52 (96.3) | 58 (92.1) |
| Male | 13 (7.4) | 6 (10.3) | 2 (3.7) | 5 (7.9) |
| Average age (SD) | 50.0 (9.8) | 47.6 (9.6) | 52.7 (9.5) | 49.8 (9.8) |
| Marital status, n (%) | ||||
| Single | 21 (12.0) | 8 (13.8) | 4 (7.4) | 9 (14.3) |
| Married/living with a partner | 119 (68.0) | 37 (63.8) | 39 (72.2) | 43 (68.3) |
| Separated/divorced/widowed | 35 (20.0) | 13 (22.4) | 11 (22.4) | 11 (17.4) |
| Social class, n (%) | ||||
| Low | 14 (8.0) | 5 (8.6) | 3 (5.6) | 6 (9.5) |
| Middle-low | 69 (39.4) | 24 (41.4) | 25 (46.3) | 20 (31.7) |
| Middle | 86 (49.2) | 27 (46.6) | 26 (48.1) | 33 (52.4) |
| Middle-high | 6 (3.4) | 2 (3.4) | 0 (0.0) | 4 (6.3) |
| Net monthly income, n (%) | ||||
| Up to EUR 999 | 34 (19.4) | 12 (20.7) | 12 (22.2) | 10 (15.9) |
| EUR 1000–1999 | 93 (53.2) | 31 (53.4) | 29 (53.7) | 33 (52.4) |
| More than EUR 2000 | 48 (27.4) | 15 (25.9) | 13 (24.1) | 20 (31.7) |
| Highest academic attainment, n (%) | ||||
| No formal schooling but can read and write | 8 (4.6) | 0 (0.0) | 3 (5.6) | 5 (7.9) |
| Primary school * | 72 (41.1) | 28 (48.3) | 23 (42.6) | 21 (33.4) |
| Secondary school * | 52 (29.7) | 17 (29.3) | 15 (27.8) | 20 (31.7) |
| University | 43 (24.6) | 13 (22.4) | 13 (24.0) | 17 (27.0) |
| Main activity, n (%) | ||||
| Self-employed or employee | 92 (52.6) | 36 (62.1) | 28 (51.9) | 28 (44.4) |
| Household chores | 68 (38.8) | 20 (34.5) | 20 (37.0) | 28 (44.4) |
| Retired or unemployed | 15 (8.6) | 2 (3.4) | 6 (11.1) | 7 (11.2) |
| Area of residence, n (%) | ||||
| Rural | 77 (44.0) | 30 (51.7) | 17 (31.5) | 30 (47.6) |
| Urban | 98 (56.0) | 28 (48.3) | 37 (68.5) | 33 (52.4) |
| Care Situation and Care Recipient Characteristics | ||||
| Number of people cared for (SD) | ||||
| A person | 127 (72.6) | 44 (75.9) | 37 (68.5) | 46 (73.0) |
| More than one | 48 (27.4) | 14 (24.1) | 17 (31.5) | 17 (27.0) |
| Sex of the care recipient, n (%) | ||||
| Female | 99 (56.6) | 29 (50.0) | 32 (59.3) | 38 (60.3) |
| Male | 76 (43.4) | 29 (50.0) | 22 (40.7) | 25 (39.7) |
| Age of the care recipient (SD) | 52.7 (31.7) | 56.6 (33.3) | 49.4 (31.0) | 52.0 (30.9) |
| Relationship of the care recipient to the caregiver, n (%) | ||||
| Father/mother | 67 (38.3) | 17 (29.3) | 25 (46.3) | 25 (39.7) |
| Spouse/partner | 25 (14.3) | 9 (15.5) | 8 (14.8) | 8 (12.7) |
| Child | 57 (32.5) | 19 (32.8) | 15 (27.8) | 23 (36.5) |
| Other family members | 22 (12.6) | 11 (19.0) | 5 (9.3) | 6 (9.5) |
| Other non-relatives | 4 (2.3) | 2 (3.4) | 1 (1.9) | 1 (1.6) |
| Illness of the person cared for, n (%) | ||||
| Chromosomal, congenital, and perinatal abnormalities | 28 (16.0) | 7 (12.1) | 10 (18.5) | 11 (17.5) |
| Diseases of the musculoskeletal, connective tissue, cardiovascular, or respiratory systems | 26 (14.9) | 11 (19.0) | 9 (16.7) | 6 (9.5) |
| Mental disorders, neurological diseases, and brain damage | 88 (50.2) | 28 (48.3) | 26 (48.1) | 34 (54.0) |
| Cancer | 5 (2.9) | 2 (3.4) | 3 (5.6) | 0 (0.0) |
| Dementias | 28 (16.0) | 10 (17.2) | 6 (11.1) | 12 (19.0) |
| Average years providing care (SD) | 13.1 (9.8) | 10.4 (8.2) | 14.3 (11.0) | 14.6 (9.7) |
| Average daily hours providing care (SD) | 16.4 (7.4) | 16.0 (7.4) | 15.2 (7.7) | 17.9 (6.9) |
| Degree of dependence of the care recipient, n (%). | ||||
| 75–100 | 24 (13.7) | 11 (19.0) | 8 (14.8) | 5 (7.9) |
| 50–74 | 46 (26.3) | 17 (29.3) | 13 (24.1) | 16 (25.4) |
| Less than 50 | 105 (60.0) | 30 (51.7) | 33 (61.1) | 42 (66.7) |
| Comparison | t | p adj.bonf | p adj.holm | Cohen’s d (95% CI) | Cliff’s δ (95% CI) |
|---|---|---|---|---|---|
| Within-Group Effects Tests | |||||
| Pre-post CBIA | 5.211 | <0.001 | <0.001 | 0.87 (0.54, 1.20) | 0.50 (0.35, 0.62) |
| Pre-post CBIA + CC | 11.003 | <0.001 | <0.001 | 1.76 (1.42, 2.10) | 0.77 (0.69, 0.83) |
| Pre-post ACG | 1.076 | 0.283 | 0.283 | 0.17 (−0.14, 0.48) | 0.13 (−0.12, 0.32) |
| Between-Group Effects Tests | |||||
| CBIA-ACG | 4.207 | <0.001 | <0.001 | 0.84 (0.44, 1.23) | 0.49 (0.30, 0.63) |
| CBIA + CC-ACG | 7.946 | <0.001 | <0.001 | 1.56 (1.16, 1.97) | 0.72 (0.61, 0.81) |
| CBIA-CBIA + CC | 3.636 | 0.001 | <0.001 | 0.72 (0.33, 1.12) | 0.44 (0.23, 0.60) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vázquez, F.L.; Blanco, V.; Hita, I.; Torres, Á.J.; Otero, P.; Páramo, M.; Salmerón, M. Efficacy of a Cognitive Behavioral Intervention for the Prevention of Depression in Nonprofessional Caregivers Administered through a Smartphone App: A Randomized Controlled Trial. J. Clin. Med. 2023, 12, 5872. https://doi.org/10.3390/jcm12185872
Vázquez FL, Blanco V, Hita I, Torres ÁJ, Otero P, Páramo M, Salmerón M. Efficacy of a Cognitive Behavioral Intervention for the Prevention of Depression in Nonprofessional Caregivers Administered through a Smartphone App: A Randomized Controlled Trial. Journal of Clinical Medicine. 2023; 12(18):5872. https://doi.org/10.3390/jcm12185872
Chicago/Turabian StyleVázquez, Fernando L., Vanessa Blanco, Isabel Hita, Ángela J. Torres, Patricia Otero, Mario Páramo, and Mar Salmerón. 2023. "Efficacy of a Cognitive Behavioral Intervention for the Prevention of Depression in Nonprofessional Caregivers Administered through a Smartphone App: A Randomized Controlled Trial" Journal of Clinical Medicine 12, no. 18: 5872. https://doi.org/10.3390/jcm12185872