
Epidemiology, Ventilation Management and Outcomes of COPD Patients Receiving Invasive Ventilation for COVID-19—Insights from PRoVENT-COVID

 , , , ,
on behalf of the PRoVENT-COVID Investigators
, , , ,
on behalf of the PRoVENT-COVID Investigators
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Patient Classification
2.4. Collected Data
2.5. Calculations
2.6. Endpoints
2.7. Power Calculation
2.8. Statistical Analysis
3. Results
3.1. Patients
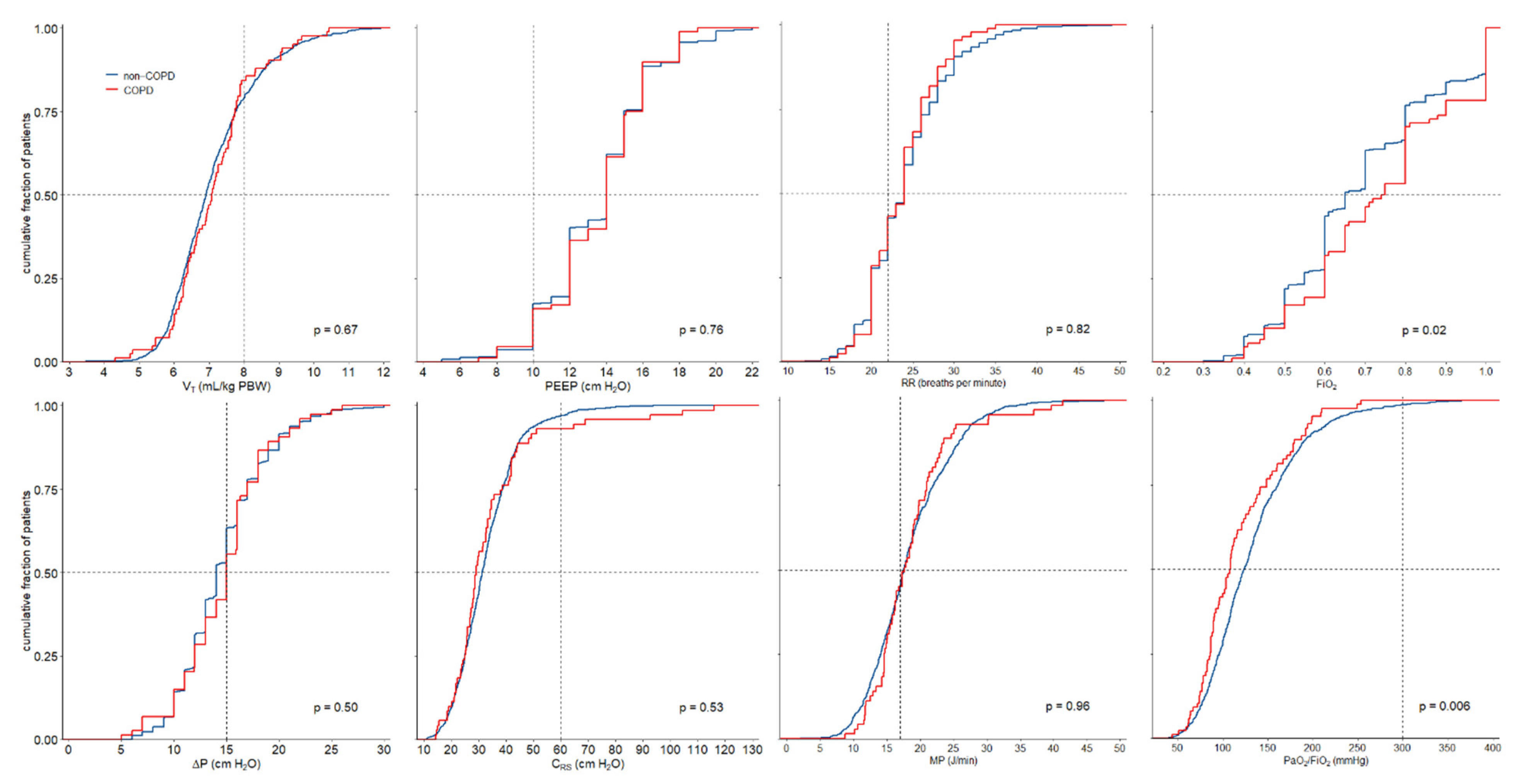
3.2. Ventilation Management
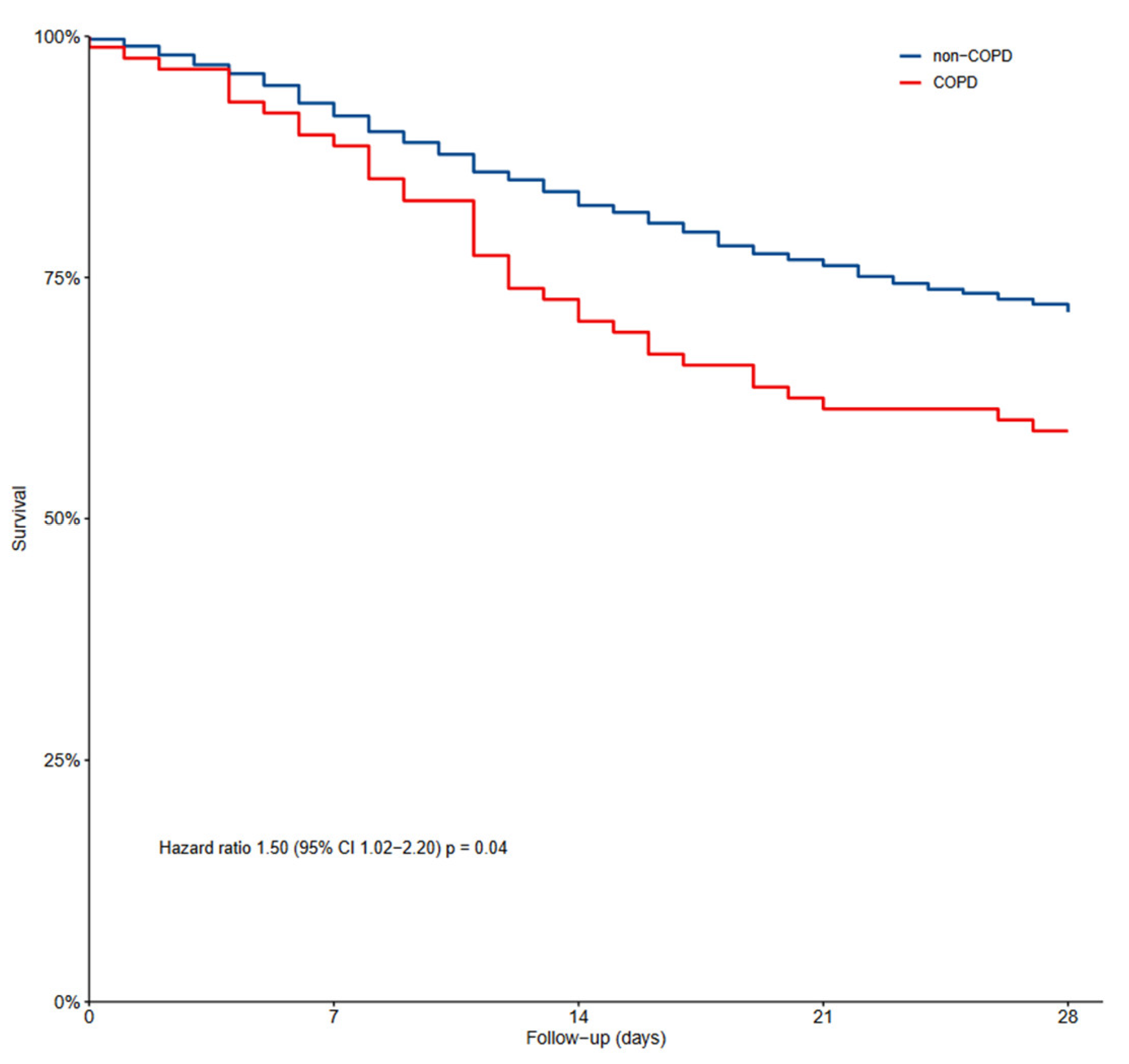
3.3. Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Registration
Appendix A
References
- Venkatesan, P. GOLD report: 2022 update. Lancet Respir. Med. 2022, 10, e20. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Menendez, R. Mortality in COPD patients with community-acquired pneumonia: Who is the third partner? Eur. Respir. J. 2006, 28, 262–263. [Google Scholar] [CrossRef] [PubMed]
- Kalil, A.C.; Thomas, P.G. Influenza virus-related critical illness: Pathophysiology and epidemiology. Crit. Care 2019, 23, 258. [Google Scholar] [CrossRef] [PubMed]
- Funk, G.-C.; Bauer, P.; Burghuber, O.C.; Fazekas, A.; Hartl, S.; Hochrieser, H.; Schmutz, R.; Metnitz, P. Prevalence and prognosis of COPD in critically ill patients between 1998 and 2008. Eur. Respir. J. 2013, 41, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Nevins, M.L.; Epstein, S.K. Predictors of outcome for patients with COPD requiring invasive mechanical ventilation. Chest 2001, 119, 1840–1849. [Google Scholar] [CrossRef] [PubMed]
- Gerayeli, F.V.; Milne, S.; Cheung, C.; Li, X.; Yang, C.W.T.; Tam, A.; Choi, L.H.; Bae, A.; Sin, D.D. COPD and the risk of poor outcomes in COVID-19: A systematic review and meta-analysis. eClinicalMedicine 2021, 33, 100789. [Google Scholar] [CrossRef] [PubMed]
- Botta, M.; Tsonas, A.M.; Pillay, J.; Boers, L.S.; Algera, A.G.; Bos, L.D.; Dongelmans, D.A.; Hollmann, M.W.; Horn, J.; Vlaar, A.P.J.; et al. Ventilation management and clinical outcomes in invasively ventilated patients with COVID-19 (PRoVENT-COVID): A national, multicentre, observational cohort study. Lancet Respir. Med. 2021, 9, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Boers, N.S.; Botta, M.; Tsonas, A.M.; Algera, A.G.; Pillay, J.; Dongelmans, D.A.; Horn, J.; Vlaar, A.P.J.; Hollmann, M.W.; Bos, L.D.J.; et al. PRactice of VENTilation in Patients with Novel Coronavirus Disease (PRoVENT-COVID): Rationale and protocol for a national multicenter observational study in The Netherlands. Ann. Transl. Med. 2020, 8, 1251. [Google Scholar] [CrossRef] [PubMed]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [PubMed]
- Mowery, N.T. Ventilator Strategies for Chronic Obstructive Pulmonary Disease and Acute Respiratory Distress Syndrome. Surg. Clin. N. Am. 2017, 97, 1381–1397. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Carlesso, E.; Cressoni, M. Selecting the ‘right’ positive end-expiratory pressure level. Curr. Opin. Crit. Care 2015, 21, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Karagiannidis, C.; Waldmann, A.D.; Róka, P.L.; Schreiber, T.; Strassmann, S.; Windisch, W.; Böhm, S.H. Regional expiratory time constants in severe respiratory failure estimated by electrical impedance tomography: A feasibility study. Crit. Care 2018, 22, 221. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Liu, X.; Meng, J.; Liu, D.; Huang, Y.; Sang, L.; Xu, Y.; Xu, Z.; He, W.; Chen, S.; et al. Electrical impedance tomography for titration of positive end-expiratory pressure in acute respiratory distress syndrome patients with chronic obstructive pulmonary disease. Crit. Care 2022, 26, 339. [Google Scholar] [CrossRef] [PubMed]
- Arnal, J.M.; Garnero, A.; Novonti, D.; Demory, D.; Ducros, L.; Berric, A.; Donati, S.Y.; Corno, G.; Jaber, S.; Durand-Gasselin, J. Feasibility study on full closed-loop control ventilation (IntelliVent-ASV™) in ICU patients with acute respiratory failure: A prospective observational comparative study. Crit. Care 2013, 17, R196. [Google Scholar] [CrossRef] [PubMed]
- Chuang, M.-L. Combining Dynamic Hyperinflation with Dead Space Volume during Maximal Exercise in Patients with Chronic Obstructive Pulmonary Disease. J. Clin. Med. 2020, 9, 1127. [Google Scholar] [CrossRef] [PubMed]
- Tusman, G.; Gogniat, E.; Madorno, M.; Otero, P.; Dianti, J.; Ceballos, I.F.; Ceballos, M.; Verdier, N.; Böhm, S.H.; Rodriguez, P.O.; et al. Effect of PEEP on Dead Space in an Experimental Model of ARDS. Respir. Care 2020, 65, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Ferluga, M.; Lucangelo, U.; Blanch, L. Dead space in acute respiratory distress syndrome. Ann. Transl. Med. 2018, 6, 388. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Rodriguez, A.; Torres, A.; Roig, J.; Sole-Violan, J.; Garnacho-Montero, J.; de la Torre, M.V.; Sirvent, J.M.; Bodi, M. Implications of COPD in patients admitted to the intensive care unit by community-acquired pneumonia. Eur. Respir. J. 2006, 27, 1210–1216. [Google Scholar] [CrossRef] [PubMed]
- Torén, K.; Murgia, N.; Olin, A.-C.; Hedner, J.; Brandberg, J.; Rosengren, A.; Bergström, G. Validity of physician-diagnosed COPD in relation to spirometric definitions of COPD in a general population aged 50–64 years—The SCAPIS pilot study. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 2269–2275. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| COPD Patients N = 88 | Non-COPD Patients N = 1002 | p-Value | |
|---|---|---|---|
| Demographics | |||
| Age, year, median [IQR] | 68 [62–72] | 65 [58–72] | 0.03 |
| Male sex, n (%) | 60 (68.2) | 735 (73.4) | 0.30 |
| BMI, kg/m2, median [IQR] | 28 [26–30] | 28 [25–31] | 0.84 |
| Severity of illness | |||
| SAPS II, median [IQR] | 35 [30–48] | 36 [29–43] | 0.32 |
| APACHE II score, median [IQR] | 15 [13–20] | 16 [12–20] | 0.41 |
| APACHE IV score, median [IQR] | 55 [49–71] | 56 [45–69] | 0.33 |
| SOFA score, median [IQR] | 8 [6–11] | 7 [6–10] | 0.73 |
| Severity of ARDS, n (%) | 0.01 | ||
| No ARDS | 2 (2.4) | 16 (1.6) | |
| Mild | 1 (1.2) | 104 (10.7) | |
| Moderate | 50 (59.5) | 602 (61.7) | |
| Severe | 31 (36.9) | 254 (26.0) | |
| Co-existing disorders, n (%) | |||
| Hypertension | 28 (31.8) | 351 (35.0) | 0.54 |
| Heart failure | 3 (3.4) | 45 (4.5) | 1.00 |
| Diabetes mellitus | 13 (14.8) | 236 (23.6) | 0.06 |
| Chronic kidney disease | 5 (5.7) | 41 (4.1) | 0.41 |
| Liver cirrhosis | 0 (0.0) | 3 (0.3) | 1.00 |
| Active hematological neoplasia | 0 (0.0) | 16 (1.6) | 0.63 |
| Active solid neoplasia | 4 (4.5) | 23 (2.3) | 0.27 |
| Neuromuscular disease | 0 (0.0) | 7 (0.7) | 1.00 |
| Immunosuppression | 2 (2.3) | 22 (2.2) | 1.00 |
| Current medication, n (%) | |||
| Systemic steroids | 7 (8.0) | 31 (3.1) | 0.03 |
| Inhaled steroids | 48 (54.5) | 73 (7.3) | <0.001 |
| Angiotensin-converting enzyme inhibitors | 8 (9.1) | 181 (18.1) | 0.03 |
| Angiotensin II receptor blockers | 16 (18.2) | 111 (11.1) | 0.05 |
| Beta-blockers | 21 (23.9) | 189 (18.9) | 0.25 |
| Insulin | 3 (3.4) | 75 (7.5) | 0.16 |
| Metformin | 8 (9.1) | 166 (16.6) | 0.07 |
| Statins | 30 (34.1) | 300 (29.9) | 0.42 |
| Calcium channel blockers | 19 (21.6) | 176 (17.6) | 0.35 |
| Chest imaging | |||
| Chest CT scan performed, n (%) | 25 (29.4) | 321 (33.6) | 0.43 |
| Lung parenchyma affected at chest CT, n (%) | 0.70 | ||
| <25% | 11 (44.0) | 115 (35.8) | |
| 50% | 7 (28.0) | 92 (28.7) | |
| 75% | 6 (24.0) | 95 (29.6) | |
| 100% | 1 (4.0) | 19 (5.9) | |
| Lung parenchyma affected at CXR, number of quadrants, n (%) | 0.48 | ||
| 1 | 4 (8.0) | 37 (7.0) | |
| 2 | 14 (28.0) | 118 (22.2) | |
| 3 | 16 (32.0) | 146 (27.5) | |
| 4 | 16 (32.0) | 230 (43.3) | |
| Laboratory tests | |||
| Plasma lactate, mmol/L, median [IQR] | 1.2 [0.9–1.4] | 1.2 [0.9–1.5] | 0.44 |
| Plasma creatinine, µmol/L (median [IQR]) | 77 [60–101] | 78 [63–98] | 0.89 |
| COPD Patients N = 88 | Non-COPD Patients N = 1002 | p-Value | |
|---|---|---|---|
| Mode of mechanical ventilation, n (%) | 0.12 | ||
| Volume-controlled | 18 (21) | 143 (14) | |
| Pressure-controlled | 41 (47) | 561 (56) | |
| Pressure support | 3 (3) | 50 (5) | |
| SIMV | 9 (10) | 72 (7) | |
| APRV | 5 (6) | 27 (3) | |
| INTELLiVENT–ASV | 5 (6) | 36 (4) | |
| Other | 6 (7) | 109 (11) | |
| Ventilation Parameters | |||
| Expiratory VT, mL, median [IQR] | 440 [387–498] | 451 [408–502] | 0.13 |
| VT per PBW, mL/kg, median [IQR] | 6.2 [5.9–7.0] | 6.4 [5.9–7.0] | 0.67 |
| PEEP, cmH2O, median [IQR] | 13 [12–15] | 13 [11–15] | 0.24 |
| Total Respiratory rate, median [IQR] | 22 [20–24] | 22 [19–24] | 0.84 |
| FiO2, median [IQR] | 0.6 [0.5–0.7] | 0.6 [0.5–0.7] | 0.01 |
| Ppeak, cmH2O, median [IQR] | 27 [24–29] | 27 [24–30] | 0.78 |
| Driving pressure, cmH2O, median [IQR] | 14 [12–16] | 14 [12–16] | 0.87 |
| Compliance, cmH2O/L, median [IQR] | 32 [26.8–39] | 33 [27–40] | 0.70 |
| Mechanical power, J/min, median [IQR] | 18 [15–20] | 19 [16–22] | 0.07 |
| Minute ventilation, L/min, median [IQR] | 9 [8–10] | 10 [8–11] | 0.07 |
| pH, median [IQR] | 7.35 [7.29–7.39] | 7.37 [7.31–7.41] | 0.02 |
| PaO2, kPa, median [IQR] | 10 [9–12] | 11 [9–13] | 0.08 |
| PaO2/FiO2, mmHg, median [IQR] | 114 [89–149] | 128 [99–168] | 0.01 |
| PaCO2, kPa, median [IQR] | 6.1 [5.5–6.5] | 5.9 [5.2–6.7] | 0.25 |
| End-tidal CO2, kPa, median [IQR] | 4.6 [4.1–5.3] | 4.9 [4.4–5.6] | 0.01 |
| Dead space fraction, median [IQR] | 0.24 [0.14–0.33] | 0.16 [0.06–0.26] | <0.001 |
| All N = 1090 | COPD N = 88 | Non-COPD N = 1002 | p-Value | |
|---|---|---|---|---|
| 28-day mortality, n (%) | 319 (29%) | 36 (41%) | 283 (28%) | 0.02 |
| 90-day mortality, n (%) | 369 (34%) | 39 (44%) | 330 (33%) | 0.04 |
| In-hospital mortality, n (%) | 364 (37%) | 39 (49%) | 325 (36%) | 0.02 |
| ICU mortality, n (%) | 354 (33%) | 38 (45%) | 316 (32%) | 0.02 |
| Length of hospital stay, days, median [IQR] | 23 [14–37] | 20 [11–31] | 24 [14–37] | 0.06 |
| Length of ICU stay, days, median [IQR] | 15 [9–26] | 12 [8–24] | 16 [9–26] | 0.11 |
| Ventilator-free days at day 28, days, median [IQR] | 16 [10–28] | 14 [10–30] | 16 [10–28] | 0.92 |
| Duration of ventilation, days, median [IQR] | 14 [8–23] | 11 [8–20] | 14 [8–23] | 0.07 |
| Tracheostomy, n (%) | 187 (17%) | 14 (16%) | 173 (17%) | 0.76 |
| Pneumothorax, n (%) | 41 (4%) | 4 (5%) | 37 (4%) | 0.57 |
| Thromboembolic complications, n (%) | ||||
| Pulmonary embolism | 244 (22%) | 20 (23%) | 224 (22%) | 0.94 |
| Deep vein thrombosis | 53 (5%) | 5 (6%) | 48 (5%) | 0.61 |
| Ischemic stroke | 31 (3%) | 3 (3%) | 28 (3%) | 0.73 |
| Myocardial infarction | 16 (1%) | 0 (0%) | 16 (2%) | 0.63 |
| Systemic arterial thrombosis | 4 (0%) | 1 (1%) | 3 (0%) | 0.29 |
| Acute kidney injury, n (%) | 488 (45%) | 38 (43%) | 450 (45%) | 0.73 |
| Re-intubation, n (%) | 138 (13%) | 8 (9%) | 130 (13%) | 0.30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tripipitsiriwat, A.; Suppapueng, O.; van Meenen, D.M.P.; Paulus, F.; Hollmann, M.W.; Sivakorn, C.; Schultz, M.J., on behalf of the PRoVENT-COVID Investigators. Epidemiology, Ventilation Management and Outcomes of COPD Patients Receiving Invasive Ventilation for COVID-19—Insights from PRoVENT-COVID. J. Clin. Med. 2023, 12, 5783. https://doi.org/10.3390/jcm12185783
Tripipitsiriwat A, Suppapueng O, van Meenen DMP, Paulus F, Hollmann MW, Sivakorn C, Schultz MJ on behalf of the PRoVENT-COVID Investigators. Epidemiology, Ventilation Management and Outcomes of COPD Patients Receiving Invasive Ventilation for COVID-19—Insights from PRoVENT-COVID. Journal of Clinical Medicine. 2023; 12(18):5783. https://doi.org/10.3390/jcm12185783
Chicago/Turabian StyleTripipitsiriwat, Athiwat, Orawan Suppapueng, David M. P. van Meenen, Frederique Paulus, Markus W. Hollmann, Chaisith Sivakorn, and Marcus J. Schultz on behalf of the PRoVENT-COVID Investigators. 2023. "Epidemiology, Ventilation Management and Outcomes of COPD Patients Receiving Invasive Ventilation for COVID-19—Insights from PRoVENT-COVID" Journal of Clinical Medicine 12, no. 18: 5783. https://doi.org/10.3390/jcm12185783