

Biomechanical Implications of Mandibular Flexion on Implant-Supported Full-Arch Rehabilitations: A Systematic Literature Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Search Strategy
- -
- English language on the MEDLINE/PubMed database.
2.3. Study Selection and Eligibility Criteria
- -
- Studies published in the English language.
- -
- In vivo and in vitro studies.
- -
- Studies examining the effects of mandibular flexion on fixed rehabilitations and the factors influencing it.
- -
- Studies highlighting suitable clinical techniques to be adopted to minimise the negative effects of mandibular flexion.
- -
- Studies not published in the English language.
- -
- Reviews, systematic reviews, and case reports.
- -
- Studies about the mandibular flexure along with any other physiological or pathological problems.
- -
- Articles that review removable prosthodontic treatments.
2.4. Data Extraction and Collection
- -
- Author(s), year and journal of publication, and kind of study;
- -
- Type of rehabilitation, and sample size;
- -
- Factors that can increase mandibular flexure;
- -
- Preventive measures and suitable techniques to be adopted to minimise the negative effects of this phenomenon on oral rehabilitations.
2.5. Data Synthesis
2.6. Quality Assessment
- -
- Low risk of bias: the study is judged to be at low risk of bias for all domains.
- -
- Moderate risk of bias: the study is judged to be at low or moderate risk of bias for all domains.
- -
- Serious risk of bias: the study is judged to be at serious risk of bias in at least one domain, but not at critical risk of bias in any domain.
- -
- Critical risk of bias: the study is judged to be at critical risk of bias in at least one domain.
3. Results
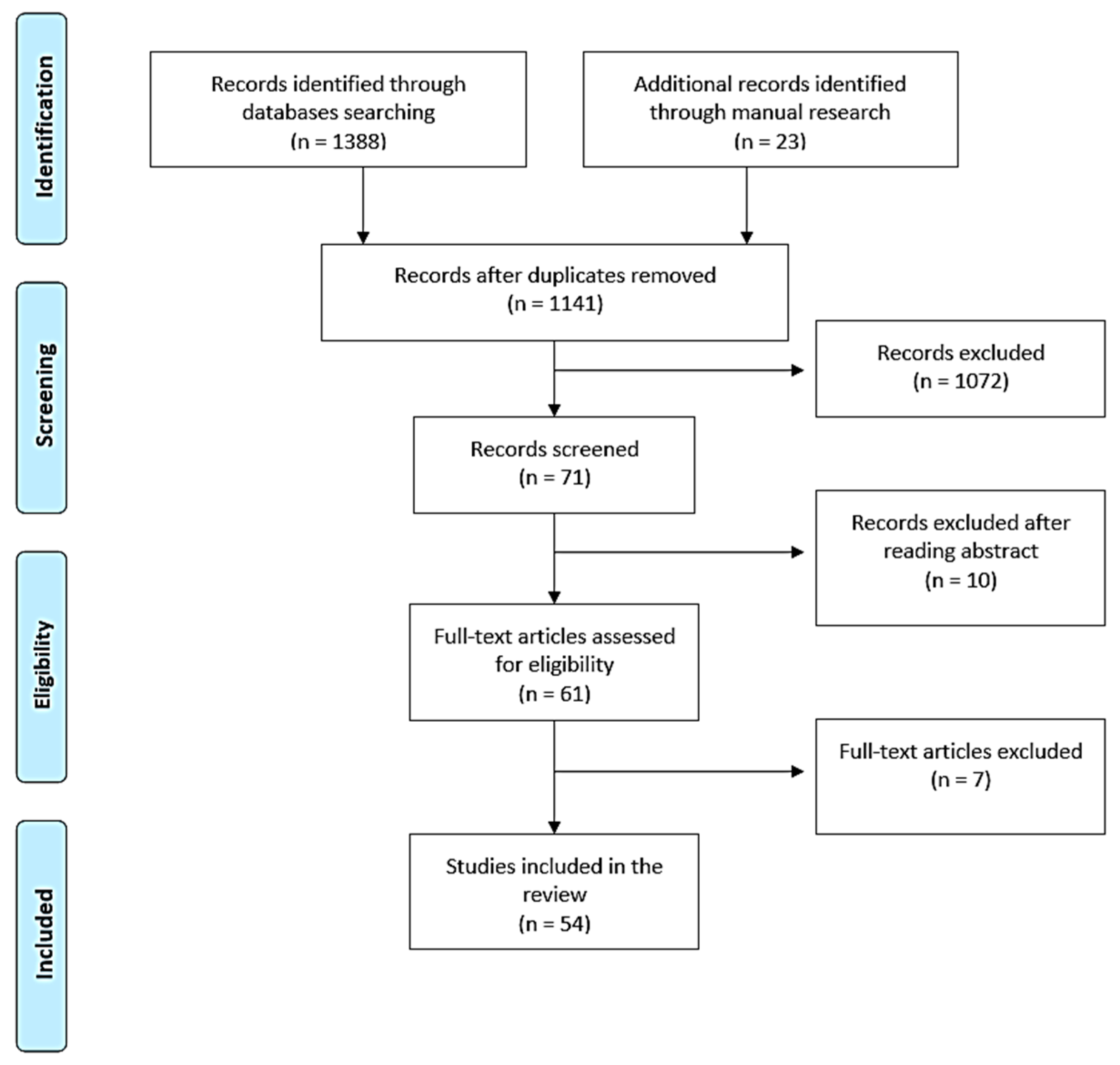
3.1. Study Selection
3.2. Data Extraction and Synthesis
3.3. Quality Assessment of the Included Studies
4. Discussion
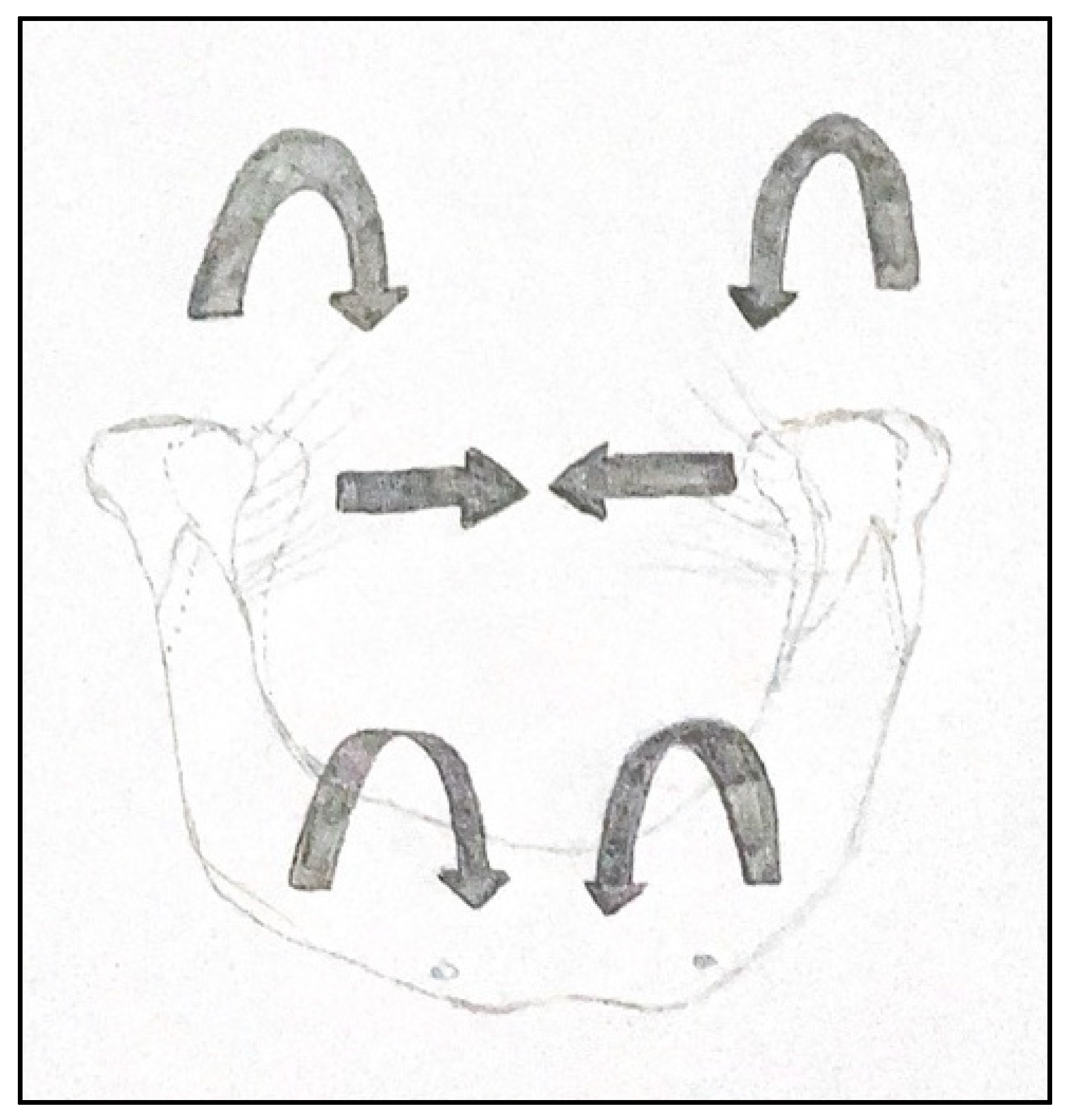
4.1. Measurement of Mandibular Flexion
- -
- Individual factors: facial type, mandibular structure, gonial angle, and symphysis characteristics (density, length, and bone surface). Some authors have also proposed age, gender, maximum occlusal force (MOF), height, weight, BMI, muscle pain, bruxism, and tooth wear as parameters that may influence mandibular flexion values.
- -
- Measurement techniques: in vivo or in vitro.
- -
- Type of movement performed during measurement: protrusion, mouth opening, laterality, and retrusion.
- -
- Area of the mandible where the measurement is performed: incisor-canine, premolar, and molar area.
- -
- Clinical condition of the mandible: jaw with teeth or edentulous.
4.1.1. Individual Factors
- -
- Brachifacial is characterised by a reduced angle of the mandibular plane, reduced vertical facial height, and a horizontal growth pattern, with maximum muscle anchorage. Brachifacial patients present a short and wide face, a square jaw and strong muscle chains.
- -
- Mesofacial is characterised by a medium mandibular plane angle, medium vertical facial height, and a mixed growth pattern, with medium muscle anchorage. Mesofacial patients are referred to as “neutral subjects” because no skeletal or muscular features prevail in them, showing a harmonious balance of the vertical and horizontal components of the face.
- -
- Dolichofacial is characterised by a high mandibular plane angle, high vertical facial height, and a vertical growth pattern, with minimal muscle anchorage. Dolichofacial patients have a long, narrow face with a convex profile [79].
4.1.2. Measurement Techniques
4.1.3. Type of Movement Performed during Measurement
4.1.4. Area of the Mandible Where the Measurement Is Performed
4.1.5. Clinical Condition of the Mandible
4.1.6. Potential Recoil of a Mandibular Flexion with a Release of Muscular Tension
4.2. Clinical Effects of MMF
4.2.1. MMF and Impression Taking
4.2.2. MMF and Fixed-Teeth-Supported Rehabilitation
4.2.3. MMF and Implant-Supported Full-Arch Fixed Rehabilitations
- -
- Type of prosthesis: single or segmented structure.
- -
- Material of the superstructure.
- -
- Number and position of implants.
Type of Prosthesis: Single or Segmented Structure
Material of the Superstructure
Number and Position of Implants
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Burch, J.G. Patterns of Change in Human Mandibular Arch Width during Jaw Excursions. Arch. Oral Biol. 1972, 17, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Wall, J.C.; Chatterji, S.K.; Jeffery, J.W. The Influence That Bone Density and the Orientation and Particle Size of the Mineral Phase Have on the Mechanical Properties of Bone. J. Bioeng. 1978, 2, 517–526. [Google Scholar] [PubMed]
- Bonfield, W. Elasticity and Viscoelasticity of Cortical Bone. In Natural and Living Biomaterials; CRC Press: Boca Raton, FL, USA, 1984; ISBN 978-1-351-07490-2. [Google Scholar]
- Ashman, R.B.; Van Buskirk, W.C. The Elastic Properties of a Human Mandible. Adv. Dent. Res. 1987, 1, 64–67. [Google Scholar] [CrossRef]
- Katz, J.L.; Meunier, A. The Elastic Anisotropy of Bone. J. Biomech. 1987, 20, 1063–1070. [Google Scholar] [CrossRef]
- Gates, G.N.; Nicholls, J.I. Evaluation of Mandibular Arch Width Change. J. Prosthet. Dent. 1981, 46, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Hylander, W.L. Stress and Strain in the Mandibular Symphysis of Primates: A Test of Competing Hypotheses. Am. J. Phys. Anthropol. 1984, 64, 1–46. [Google Scholar] [CrossRef] [PubMed]
- van Eijden, T.M. Biomechanics of the Mandible. Crit. Rev. Oral Biol. Med. 2000, 11, 123–136. [Google Scholar] [CrossRef]
- Goodkind, R.J.; Heringlake, C.B. Mandibular Flexure in Opening and Closing Movements. J. Prosthet. Dent. 1973, 30, 134–138. [Google Scholar] [CrossRef]
- Regli, C.P.; Kelly, E.K. The Phenomenon of Decreased Mandibular Arch Width in Opening Movements. J. Prosthet. Dent. 1967, 17, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Omar, R.; Wise, M.D. Mandibular Flexure Associated with Muscle Force Applied in the Retruded Axis Position. J. Oral Rehabil. 1981, 8, 209–221. [Google Scholar] [CrossRef]
- Canabarro, S.D.A.; Shinkai, R.S.A. Medial Mandibular Flexure and Maximum Occlusal Force in Dentate Adults. Int. J. Prosthodont. 2006, 19, 177–182. [Google Scholar] [PubMed]
- Röhrle, O.; Pullan, A.J. Three-Dimensional Finite Element Modelling of Muscle Forces during Mastication. J. Biomech. 2007, 40, 3363–3372. [Google Scholar] [CrossRef]
- De Marco, T.J.; Paine, S. Mandibular Dimensional Change. J. Prosthet. Dent. 1974, 31, 482–485. [Google Scholar] [CrossRef] [PubMed]
- Fischman, B. The Rotational Aspect of Mandibular Flexure. J. Prosthet. Dent. 1990, 64, 483–485. [Google Scholar] [CrossRef] [PubMed]
- Linkow, L.I.; Ghalili, R. Ramus Hinges for Excessive Movements of the Condyles: A New Dimension in Mandibular Tripodal Subperiosteal Implants. J. Oral Implantol. 1999, 25, 11–17. [Google Scholar] [CrossRef]
- Shinkai, R.S.A.; Canabarro, S.D.A.; Schmidt, C.B.; Sartori, E.A. Reliability of a Digital Image Method for Measuring Medial Mandibular Flexure in Dentate Subjects. J. Appl. Oral Sci. 2004, 12, 358–362. [Google Scholar] [CrossRef] [Green Version]
- Wenzel, A.; Gröndahl, H.G. Direct Digital Radiography in the Dental Office. Int. Dent. J. 1995, 45, 27–34. [Google Scholar]
- Borg, E.; Gröndahl, H.G. On the Dynamic Range of Different X-Ray Photon Detectors in Intra-Oral Radiography. A Comparison of Image Quality in Film, Charge-Coupled Device and Storage Phosphor Systems. Dentomaxillofac. Radiol. 1996, 25, 82–88. [Google Scholar] [CrossRef] [Green Version]
- Frost, H.M. Bone “Mass” and the “Mechanostat”: A Proposal. Anat. Rec. 1987, 219, 1–9. [Google Scholar] [CrossRef]
- Frost, H.M. A 2003 Update of Bone Physiology and Wolff’s Law for Clinicians. Angle Orthod. 2004, 74, 3–15. [Google Scholar]
- Pantaleo, G.; Acerra, A.; Giordano, F.; D’Ambrosio, F.; Langone, M.; Caggiano, M. Immediate Loading of Fixed Prostheses in Fully Edentulous Jaws: A 7-Year Follow-Up from a Single-Cohort Retrospective Study. Appl. Sci. 2022, 12, 12427. [Google Scholar] [CrossRef]
- Hobkirk, J.A.; Havthoulas, T.K. The Influence of Mandibular Deformation, Implant Numbers, and Loading Position on Detected Forces in Abutments Supporting Fixed Implant Superstructures. J. Prosthet. Dent. 1998, 80, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Korioth, T.W.; Hannam, A.G. Deformation of the Human Mandible during Simulated Tooth Clenching. J. Dent. Res. 1994, 73, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, Y.; Fujisawa, K.; Takechi, M.; Momota, Y.; Yuasa, T.; Tatehara, S.; Nagayama, M.; Yamauchi, E. Effect of the Additional Installation of Implants in the Posterior Region on the Prognosis of Treatment in the Edentulous Mandibular Jaw. Clin. Oral Implant. Res. 2003, 14, 727–733. [Google Scholar] [CrossRef]
- Hobkirk, J.A.; Schwab, J. Mandibular Deformation in Subjects with Osseointegrated Implants. Int. J. Oral Maxillofac. Implant. 1991, 6, 319–328. [Google Scholar]
- Horiuchi, M.; Ichikawa, T.; Noda, M.; Matsumoto, N. Use of Interimplant Displacement to Measure Mandibular Distortion during Jaw Movements in Humans. Arch. Oral Biol. 1997, 42, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Paez, C.Y.; Barco, T.; Roushdy, S.; Andres, C. Split-Frame Implant Prosthesis Designed to Compensate for Mandibular Flexure: A Clinical Report. J. Prosthet. Dent. 2003, 89, 341–343. [Google Scholar] [CrossRef] [Green Version]
- Custodio, W.; Gomes, S.G.F.; Faot, F.; Garcia, R.C.M.R.; Del Bel Cury, A.A. Occlusal Force, Electromyographic Activity of Masticatory Muscles and Mandibular Flexure of Subjects with Different Facial Types. J. Appl. Oral Sci. 2011, 19, 343–349. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.C.; Lai, Y.L.; Chi, L.Y.; Lee, S.Y. Contributing Factors of Mandibular Deformation during Mouth Opening. J. Dent. 2000, 28, 583–588. [Google Scholar] [CrossRef]
- Favot, L.-M.; Berry-Kromer, V.; Haboussi, M.; Thiebaud, F.; Ben Zineb, T. Numerical Study of the Influence of Material Parameters on the Mechanical Behaviour of a Rehabilitated Edentulous Mandible. J. Dent. 2014, 42, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Arenal, A.; Lasheras, F.S.; Fernández, E.M.; González, I. A Jaw Model for the Study of the Mandibular Flexure Taking into Account the Anisotropy of the Bone. Math. Comput. Model. 2009, 50, 695–704. [Google Scholar] [CrossRef]
- Shinkai, R.S.; Lazzari, F.L.; Canabarro, S.A.; Gomes, M.; Grossi, M.L.; Hirakata, L.M.; Mota, E.G. Maximum Occlusal Force and Medial Mandibular Flexure in Relation to Vertical Facial Pattern: A Cross-Sectional Study. Head Face Med. 2007, 3, 18. [Google Scholar] [CrossRef] [Green Version]
- Prasad, M.; Hussain, M.Z.; Shetty, S.K.; Kumar, T.A.; Khaur, M.; George, S.A.; Dalwai, S. Median Mandibular Flexure at Different Mouth Opening and Its Relation to Different Facial Types: A Prospective Clinical Study. J. Nat. Sci. Biol. Med. 2013, 4, 426–430. [Google Scholar] [CrossRef] [Green Version]
- Scandurra, C.; Gasparro, R.; Dolce, P.; Bochicchio, V.; Muzii, B.; Sammartino, G.; Marenzi, G.; Maldonato, N.M. The Role of Cognitive and Non-Cognitive Factors in Dental Anxiety: A Mediation Model. Eur. J. Oral Sci. 2021, 129, e12793. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Oliveira, R.M.; Emtiaz, S. Mandibular Flexure and Dental Implants: A Case Report. Implant. Dent. 2000, 9, 90–95. [Google Scholar] [CrossRef]
- Law, C.; Bennani, V.; Lyons, K.; Swain, M. Mandibular Flexure and Its Significance on Implant Fixed Prostheses: A Review. J. Prosthodont. 2012, 21, 219–224. [Google Scholar] [CrossRef]
- Marin, D.O.M.; Dias, K.D.C.; Paleari, A.G.; Pero, A.C.; Arioli Filho, J.N.; Compagnoni, M.A. Split-Framework in Mandibular Implant-Supported Prosthesis. Case Rep. Dent. 2015, 2015, 502394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sivaraman, K.; Chopra, A.; Venkatesh, S.B. Clinical Importance of Median Mandibular Flexure in Oral Rehabilitation: A Review. J. Oral Rehabil. 2016, 43, 215–225. [Google Scholar] [CrossRef]
- Mijiritsky, E.; Shacham, M.; Meilik, Y.; Dekel-Steinkeller, M. Clinical Influence of Mandibular Flexure on Oral Rehabilitation: Narrative Review. Int. J. Environ. Res. Public. Health 2022, 19, 16748. [Google Scholar] [CrossRef]
- James, A.; McDowell, C.P. Quantitative Analysis of the Decrease in Width of the Mandibular Arch during Forced Movements of the Mandible. J. Dent. 1961, 40, 1183–1185. Available online: https://journals.sagepub.com/doi/abs/10.1177/00220345610400061201 (accessed on 20 May 2023).
- Osborne, J. Tomlin Medial Convergence of the Mandible. Br. Dent. J. 1964, 117, 112–114. [Google Scholar]
- Burch, J.G.; Borchers, G. Method for Study of Mandibular Arch Width Change. J. Dent. Res. 1970, 49, 463. [Google Scholar] [CrossRef]
- Novak, C.A. Mandibular Dimensional Change in the Various Jaw Positions and Its Effect upon Prosthetic Appliances. Dent. Stud. 1972, 50, 19. [Google Scholar]
- Fischman, B.M. The Influence of Fixed Splints on Mandibular Flexure. J. Prosthet. Dent. 1976, 35, 643–647. [Google Scholar] [CrossRef]
- Ferrario, V.; Sforza, C. Biomechanical Model of the Human Mandible: A Hypothesis Involving Stabilizing Activity of the Superior Belly of Lateral Pterygoid Muscle. J. Prosthet. Dent. 1992, 68, 829–835. [Google Scholar] [CrossRef]
- Hart, R.T.; Hennebel, V.V.; Thongpreda, N.; Van Buskirk, W.C.; Anderson, R.C. Modeling the Biomechanics of the Mandible: A Three-Dimensional Finite Element Study. J. Biomech. 1992, 25, 261–286. [Google Scholar] [CrossRef]
- Korioth, T.W.P.; Romilly, D.P.; Hannam, A.G. Three-Dimensional Finite Element Stress Analysis of the Dentate Human Mandible. Am. J. Phys. Anthropol. 1992, 88, 69–96. [Google Scholar] [CrossRef]
- Koolstra, J.H.; van Eijden, T.M. Biomechanical Analysis of Jaw-Closing Movements. J. Dent. Res. 1995, 74, 1564–1570. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Latif, H.H.; Hobkirk, J.A.; Kelleway, J.P. Functional Mandibular Deformation in Edentulous Subjects Treated with Dental Implants. Int. J. Prosthodont. 2000, 13, 513–519. [Google Scholar] [PubMed]
- Kemkes-Grottenthaler, A.; Löbig, F.; Stock, F. Mandibular Ramus Flexure and Gonial Eversion as Morphologic Indicators of Sex. Homo 2002, 53, 97–111. [Google Scholar] [CrossRef]
- Jiang, T.; Ai, M. In Vivo Mandibular Elastic Deformation during Clenching on Pivots. J. Oral Rehabil. 2002, 29, 201–208. [Google Scholar] [CrossRef]
- Zarone, F.; Apicella, A.; Nicolais, L.; Aversa, R.; Sorrentino, R. Mandibular Flexure and Stress Build-up in Mandibular Full-Arch Fixed Prostheses Supported by Osseointegrated Implants. Clin. Oral Implant. Res. 2003, 14, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Choi, A.H.; Ben-Nissan, B.; Conway, R.C. Three-Dimensional Modelling and Finite Element Analysis of the Human Mandible during Clenching. Aust. Dent. J. 2005, 50, 42–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balci, Y.; Yavuz, M.F.; Cağdir, S. Predictive Accuracy of Sexing the Mandible by Ramus Flexure. Homo 2005, 55, 229–237. [Google Scholar] [CrossRef]
- Yokoyama, S.; Wakabayashi, N.; Shiota, M.; Ohyama, T. Stress Analysis in Edentulous Mandibular Bone Supporting Implant-Retained 1-Piece or Multiple Superstructures. Int. J. Oral Maxillofac. Implant. 2005, 20, 578–583. [Google Scholar]
- Al-Sukhun, J.; Helenius, M.; Lindqvist, C.; Kelleway, J. Biomechanics of the Mandible Part I: Measurement of Mandibular Functional Deformation Using Custom-Fabricated Displacement Transducers. J. Oral Maxillofac. Surg. 2006, 64, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Al-Sukhun, J.; Kelleway, J. Biomechanics of the Mandible: Part II. Development of a 3-Dimensional Finite Element Model to Study Mandibular Functional Deformation in Subjects Treated with Dental Implants. Int. J. Oral Maxillofac. Implant. 2007, 22, 455–466. [Google Scholar]
- El-Sheikh, A.M.; Abdel-Latif, H.H.; Howell, P.G.; Hobkirk, J.A. Midline Mandibular Deformation during Nonmasticatory Functional Movements in Edentulous Subjects with Dental Implants. Int. J. Oral Maxillofac. Implant. 2007, 22, 243–248. [Google Scholar]
- Gulsahi, A.; Yüzügüllü, B.; Imirzalioglu, P.; Genç, Y. Assessment of Panoramic Radiomorphometric Indices in Turkish Patients of Different Age Groups, Gender and Dental Status. Dentomaxillofac. Radiol. 2008, 37, 288–292. [Google Scholar] [CrossRef]
- Naini, R.B.; Nokar, S. Three-Dimensional Finite Element Analysis of the Effect of 1-Piece Superstructure on Mandibular Flexure. Implant. Dent. 2009, 18, 428–437. [Google Scholar] [CrossRef] [Green Version]
- Bellini, C.M.; Romeo, D.; Galbusera, F.; Taschieri, S.; Raimondi, M.T.; Zampelis, A.; Francetti, L. Comparison of Tilted versus Nontilted Implant-Supported Prosthetic Designs for the Restoration of the Edentuous Mandible: A Biomechanical Study. Int. J. Oral Maxillofac. Implant. 2009, 24, 511–517. [Google Scholar]
- Nokar, S.; Baghai Naini, R. The Effect of Superstructure Design on Stress Distribution in Peri-Implant Bone during Mandibular Flexure. Int. J. Oral Maxillofac. Implant. 2010, 25, 31–37. [Google Scholar]
- Zaugg, B.; Hämmerle, C.H.F.; Palla, S.; Gallo, L.M. Implant-Supported Mandibular Splinting Affects Temporomandibular Joint Biomechanics. Clin. Oral Implant. Res. 2012, 23, 897–901. [Google Scholar] [CrossRef] [PubMed]
- Madani, A.S.; Asadzadeh, N.; Hosseini, S.H. Mandibular Flexure in Anterior-Posterior and Transverse Plane on Edentulous Patients in Mashhad Faculty of Dentistry. J. Dent. Mater. Tech. 2012, 1, 24–28. [Google Scholar] [CrossRef]
- Law, C.; Bennani, V.; Lyons, K.; Swain, M. Influence of Implant Framework and Mandibular Flexure on the Strain Distribution on a Kennedy Class II Mandible Restored with a Long-Span Implant Fixed Restoration: A Pilot Study. J. Prosthet. Dent. 2014, 112, 31–37. [Google Scholar] [CrossRef]
- Lin, C.; Jiao, B.; Liu, S.; Guan, F.; Chung, N.-E.; Han, S.-H.; Lee, U.-Y. Sex Determination from the Mandibular Ramus Flexure of Koreans by Discrimination Function Analysis Using Three-Dimensional Mandible Models. Forensic Sci. Int. 2014, 236, 191.e1–191.e6. [Google Scholar] [CrossRef]
- Martin-Fernandez, E.; Gonzalez-Gonzalez, I.; deLlanos-Lanchares, H.; Mauvezin-Quevedo, M.A.; Brizuela-Velasco, A.; Alvarez-Arenal, A. Mandibular Flexure and Peri-Implant Bone Stress Distribution on an Implant-Supported Fixed Full-Arch Mandibular Prosthesis: 3D Finite Element Analysis. Biomed. Res. Int. 2018, 2018, 8241313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahriari, S.; Parandakh, A.; Khani, M.-M.; Azadikhah, N.; Naraghi, P.; Aeinevand, M.; Nikkhoo, M.; Khojasteh, A. The Effect of Mandibular Flexure on Stress Distribution in the All-on-4 Treated Edentulous Mandible: A Comparative Finite-Element Study Based on Mechanostat Theory. J. Long. Term. Eff. Med. Implant. 2019, 29, 79–86. [Google Scholar] [CrossRef]
- Wolf, L.; Bergauer, B.; Adler, W.; Wichmann, M.; Matta, R.E. Three-Dimensional Evaluation of Mandibular Deformation during Mouth Opening. Int. J. Comput. Dent. 2019, 22, 21–27. [Google Scholar]
- Tulsani, M.; Maiti, S.; Rupawat, D. Evaluation of Change in Mandibular Width During Maximum Mouth Opening and Protrusion. Int. J. Dent. Oral Sci. 2020, 5, 62–65. [Google Scholar] [CrossRef]
- Ebadian, B.; Abolhasani, M.; Heidarpour, A.; Ziaei, M.; Jowkar, M. Assessment of the Relationship between Maximum Occlusal Force and Median Mandibular Flexure in Adults: A Clinical Trial Study. J. Indian. Prosthodont. Soc. 2020, 20, 76–82. [Google Scholar] [CrossRef]
- Schmidt, A.; Klussmann, L.; Schlenz, M.A.; Wöstmann, B. Elastic Deformation of the Mandibular Jaw Revisited-a Clinical Comparison between Digital and Conventional Impressions Using a Reference. Clin. Oral Investig. 2021, 25, 4635–4642. [Google Scholar] [CrossRef] [PubMed]
- Gülsoy, M.; Tuna, S.H.; Pekkan, G. Evaluation of Median Mandibular Flexure Values in Dentulous and Edentulous Subjects by Using an Intraoral Digital Scanner. J. Adv. Prosthodont. 2022, 14, 32–44. [Google Scholar] [CrossRef]
- Gao, J.; Li, X.; He, J.; Jiang, L.; Zhao, B. The Effect of Mandibular Flexure on the Design of Implant-Supported Fixed Restorations of Different Facial Types under Two Loading Conditions by Three-Dimensional Finite Element Analysis. Front. Bioeng. Biotechnol. 2022, 10, 928656. [Google Scholar] [CrossRef]
- Asadzadeh, N.; Madani, A.S.; Mirmortazavi, A.; Sabooni, M.R.; Shibani, V. Mandibular Width and Length Deformation during Mouth Opening in Female Dental Students. J. Appl. Sci. 2012, 12, 1865–1868. [Google Scholar] [CrossRef] [Green Version]
- Choi, A.H.; Conway, R.C.; Taraschi, V.; Ben-Nissan, B. Biomechanics and Functional Distortion of the Human Mandible. J. Investig. Clin. Dent. 2015, 6, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Abu Alhaija, E.S.J.; Al Zo’ubi, I.A.; Al Rousan, M.E.; Hammad, M.M. Maximum Occlusal Bite Forces in Jordanian Individuals with Different Dentofacial Vertical Skeletal Patterns. Eur. J. Orthod. 2010, 32, 71–77. [Google Scholar] [CrossRef]
- Sella Tunis, T.; May, H.; Sarig, R.; Vardimon, A.D.; Hershkovitz, I.; Shpack, N. Are Chin and Symphysis Morphology Facial Type-Dependent? A Computed Tomography-Based Study. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 84–93. [Google Scholar] [CrossRef]
- Dahlin, D.C. Bone and Bones. Fundamentals of Bone Biology. Am. J. Clin. Pathol. 1956, 26, 179. [Google Scholar] [CrossRef] [Green Version]
- Picton, D.C. Distortion of the Jaws during Biting. Arch. Oral Biol. 1962, 7, 573–580. [Google Scholar] [CrossRef]
- Standlee, J.P.; Caputo, A.A.; Ralph, J.P. Stress Trajectories within the Mandible under Occlusal Loads. J. Dent. Res. 1977, 56, 1297–1302. [Google Scholar] [CrossRef] [PubMed]
- Mongini, F.; Calderale, P.M.; Barberi, G. Relationship between Structure and the Stress Pattern in the Human Mandible. J. Dent. Res. 1979, 58, 2334–2337. [Google Scholar] [CrossRef]
- Ralph, J.P.; Caputo, A.A. Analysis of Stress Patterns in the Human Mandible. J. Dent. Res. 1975, 54, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Clelland, N.L.; Lee, J.K.; Bimbenet, O.C.; Brantley, W.A. A Three-Dimensional Finite Element Stress Analysis of Angled Abutments for an Implant Placed in the Anterior Maxilla. J. Prosthodont. 1995, 4, 95–100. [Google Scholar] [CrossRef]
- Brunski, J.B. Biomechanical Factors Affecting the Bone-Dental Implant Interface. Clin. Mater. 1992, 10, 153–201. [Google Scholar] [CrossRef]
- Cochran, D.L. The Scientific Basis for and Clinical Experiences with Straumann Implants Including the ITI Dental Implant System: A Consensus Report. Clin. Oral. Implant. Res. 2000, 11, 33–58. [Google Scholar] [CrossRef]
- Caggiano, M.; Amato, A.; Acerra, A.; D’Ambrosio, F.; Martina, S. Evaluation of Deviations between Computer-Planned Implant Position and In Vivo Placement through 3D-Printed Guide: A CBCT Scan Analysis on Implant Inserted in Esthetic Area. Appl.Sci. 2022, 12, 5461. [Google Scholar] [CrossRef]
- Flügge, T.V.; Schlager, S.; Nelson, K.; Nahles, S.; Metzger, M.C. Precision of Intraoral Digital Dental Impressions with ITero and Extraoral Digitization with the ITero and a Model Scanner. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 471–478. [Google Scholar] [CrossRef]
- Anh, J.-W.; Park, J.-M.; Chun, Y.-S.; Kim, M.; Kim, M. A Comparison of the Precision of Three-Dimensional Images Acquired by 2 Digital Intraoral Scanners: Effects of Tooth Irregularity and Scanning Direction. Korean J. Orthod. 2016, 46, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Tallgren, A. The Continuing Reduction of the Residual Alveolar Ridges in Complete Denture Wearers: A Mixed-Longitudinal Study Covering 25 Years. J. Prosthet. Dent. 1972, 27, 120–132. [Google Scholar] [CrossRef]
- Atkinson, P.J.; Woodhead, C. Changes in Human Mandibular Structure with Age. Arch. Oral Biol. 1968, 13, 1453–1464. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Caggiano, M.; Acerra, A.; Pisano, M.; Giordano, F. Is Ozone a Valid Adjuvant Therapy for Periodontitis and Peri-Implantitis? A Systematic Review. J. Pers. Med. 2023, 13, 646. [Google Scholar] [CrossRef]
- Yang, H.S.; Lang, L.A.; Felton, D.A. Finite Element Stress Analysis on the Effect of Splinting in Fixed Partial Dentures. J. Prosthet. Dent. 1999, 81, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, F.; Uno, I.; Hata, Y.; Neuendorff, G.; Kirsch, A. Analysis of Stress Distribution in a Screw-Retained Implant Prosthesis. Int. J. Oral Maxillofac. Implant. 2000, 15, 209–218. [Google Scholar]
- Torsello, F.; di Torresanto, V.M.; Ercoli, C.; Cordaro, L. Evaluation of the Marginal Precision of One-Piece Complete Arch Titanium Frameworks Fabricated Using Five Different Methods for Implant-Supported Restorations. Clin. Oral Implant. Res. 2008, 19, 772–779. [Google Scholar] [CrossRef] [PubMed]
- Lindquist, L.W.; Rockler, B.; Carlsson, G.E. Bone Resorption around Fixtures in Edentulous Patients Treated with Mandibular Fixed Tissue-Integrated Prostheses. J. Prosthet. Dent. 1988, 59, 59–63. [Google Scholar] [CrossRef]
- Korioth, T.W.; Johann, A.R. Influence of Mandibular Superstructure Shape on Implant Stresses during Simulated Posterior Biting. J. Prosthet. Dent. 1999, 82, 67–72. [Google Scholar] [CrossRef]
- Suedam, V.; Souza, E.A.C.; Moura, M.S.; Jacques, L.B.; Rubo, J.H. Effect of Abutment’s Height and Framework Alloy on the Load Distribution of Mandibular Cantilevered Implant-Supported Prosthesis. Clin. Oral Implant. Res. 2009, 20, 196–200. [Google Scholar] [CrossRef]
- Hossain, N.; Mobarak, M.H.; Hossain, A.; Khan, F.; Mim, J.J.; Chowdhury, M.A. Advances of plant and biomass extracted zirconium nanoparticles in dental implant application. Heliyon 2023, 9, e15973. [Google Scholar] [CrossRef]
- Hossain, N.; Islam, M.A.; Chowdhury, M.A. Synthesis and characterization of plant extracted silver nanoparticles and advances in dental implant applications. Heliyon 2022, 8, e12313. [Google Scholar] [CrossRef]
- Di Spirito, F.; Giudice, R.L.; Amato, M.; Di Palo, M.P.; D’ambrosio, F.; Amato, A.; Martina, S. Inflammatory, Reactive, and Hypersensitivity Lesions Potentially Due to Metal Nanoparticles from Dental Implants and Supported Restorations: An Umbrella Review. Appl. Sci. 2022, 12, 11208. [Google Scholar] [CrossRef]
- Skalak, R. Biomechanical Considerations in Osseointegrated Prostheses. J. Prosthet. Dent. 1983, 49, 843–848. [Google Scholar] [CrossRef]
- Itoh, H.; Caputo, A.A.; Kuroe, T.; Nakahara, H. Biomechanical Comparison of Straight and Staggered Implant Placement Configurations. Int. J. Periodontics Restor. Dent. 2004, 24, 47–55. [Google Scholar] [CrossRef]
- McCartney, J.W. Cantilever Rests: An Alternative to the Unsupported Distal Cantilever of Osseointegrated Implant-Supported Prostheses for the Edentulous Mandible. J. Prosthet. Dent. 1992, 68, 817–819. [Google Scholar] [CrossRef] [PubMed]
- Jemt, T. In Vivo Measurements of Precision of Fit Involving Implant-Supported Prostheses in the Edentulous Jaw. Int. J. Oral Maxillofac. Implant. 1996, 11, 151–158. [Google Scholar]
- Schmidt, A.; Wöstmann, B.; Schlenz, M.A. Accuracy of Digital Implant Impressions in Clinical Studies: A Systematic Review. Clin. Oral Implant. Res. 2022, 33, 573–585. [Google Scholar] [CrossRef]
- Bra-nemark, P.-I.; Zarb, G.A.; Albrektsson, T.; Rosen, H.M. Tissue-Integrated Prostheses. Osseointegration in Clinical Dentistry. Plast. Reconstr. Surg. 1986, 77, 496. [Google Scholar] [CrossRef]
- Maló, P.; Rangert, B.; Nobre, M. “All-on-Four” Immediate-Function Concept with Brånemark System Implants for Completely Edentulous Mandibles: A Retrospective Clinical Study. Clin. Implant. Dent. Relat. Res. 2003, 5, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Apicella, A.; Masi, E.; Nicolais, L.; Zarone, F.; de Rosa, N.; Valletta, G. A Finite-Element Model Study of Occlusal Schemes in Full-Arch Implant Restoration. J. Mater. Sci. Mater. Med. 1998, 9, 191–196. [Google Scholar] [CrossRef]
- Tashkandi, E.A.; Lang, B.R.; Edge, M.J. Analysis of Strain at Selected Bone Sites of a Cantilevered Implant-Supported Prosthesis. J. Prosthet. Dent. 1996, 76, 158–164. [Google Scholar] [CrossRef]
- van Zyl, P.P.; Grundling, N.L.; Jooste, C.H.; Terblanche, E. Three-Dimensional Finite Element Model of a Human Mandible Incorporating Six Osseointegrated Implants for Stress Analysis of Mandibular Cantilever Prostheses. Int. J. Oral Maxillofac. Implant. 1995, 10, 51–57. [Google Scholar]
- Shackleton, J.L.; Carr, L.; Slabbert, J.C.; Becker, P.J. Survival of Fixed Implant-Supported Prostheses Related to Cantilever Lengths. J. Prosthet. Dent. 1994, 71, 23–26. [Google Scholar] [CrossRef] [PubMed]
- White, S.N.; Caputo, A.A.; Anderkvist, T. Effect of Cantilever Length on Stress Transfer by Implant-Supported Prostheses. J. Prosthet. Dent. 1994, 71, 493–499. [Google Scholar] [CrossRef]
- Naert, I.; Quirynen, M.; van Steenberghe, D.; Darius, P. A Study of 589 Consecutive Implants Supporting Complete Fixed Prostheses. Part II: Prosthetic Aspects. J. Prosthet. Dent. 1992, 68, 949–956. [Google Scholar] [CrossRef] [PubMed]
- Fenton, A.H.; Zarb, G.A. Research Status of Prosthodontic Procedures. Int. J. Prosthodont. 1993, 6, 137–144. [Google Scholar] [PubMed]
- Agliardi, E.L.; Francetti, L.; Romeo, D.; Del Fabbro, M. Immediate Rehabilitation of the Edentulous Maxilla: Preliminary Results of a Single-Cohort Prospective Study. Int. J. Oral Maxillofac. Implant. 2009, 24, 887–895. [Google Scholar]



{kind=link}
{kind=link}
| Author, Year of Publication and Reference | Reason for Exclusion |
|---|---|
| Van Eijden, T.M., 2000 [8] | It is a review |
| Paez, C.Y., 2003 [28] | It is a case report |
| de Oliveira, R.M., 2000 [37] | It is a case report |
| Law, C., 2012 [38] | It is a review |
| Marin, D.O., 2015 [39] | It is a case report |
| Sivaraman, K., 2016 [40] | It is a review |
| Mijiritsky, E., 2022 [41] | It is a narrative review |
| Author, Year of Publication and Reference | Journal of Publication | Study Design | Outcome |
|---|---|---|---|
| Burch, J.G., 1972 [1] | Arch. Oral Biol. | Clinical trial | Influence of mandibular movements on MF values |
| Gates, G.N., 1981 [6] | J. Prosthet. Dent. | Clinical trial | Influence of mandibular movements on MF values |
| Hylander, W.L., 1984 [7] | Am. J. Phys. Anthropol. | Clinical trial | Influence of individual factors on MF values |
| Goodkind, R.J., 1973 [9] | J. Prosthet. Dent. | Clinical trial | MF measurement |
| Regli, C.P., 1967 [10] | J. Prosthet. Dent. | Clinical trial | MF measurement |
| Omar, R., 1981 [11] | J. Oral Rehabil. | Clinical trial | Influence of MF on impression taking |
| Canabarro Sde, A., 2006 [12] | Int. J. Prosthodont. | Clinical trial | Influence of mandibular movements and individual factors on MF values |
| De Marco, T.J., 1974 [14] | J. Prosthet. Dent. | Clinical trial | MF measurement |
| Fischman, B., 1990 [15] | J. Prosthet. Dent. | Clinical trial | MF measurement |
| Shinkai, R., 2004 [17] | J. Appl. Oral Sci. | Clinical trial | Influence of individual factors on MF values |
| Hobkirk, J.A., 1998 [23] | J. Prosthet. Dent. | Clinical trial | Influence of individual factors on MF values |
| Hobkirk, J.A., 1991 [26] | Int. J. Oral Maxillofac. Implant. | Clinical trial | Influence of individual factors on MF values |
| Horiuchi, M., 1997 [27] | Arch. Oral Biol. | Clinical trial | Influence of mandibular movements on MF values |
| Custodio, W., 2011 [29] | J. Appl. Oral Sci. | Clinical trial | Influence of individual factors on MF values |
| Chen, D.C., 2000 [30] | J. Dent. | Clinical trial | Influence of individual factors on MF values |
| Favot, L.M., 2014 [31] | J. Dent. | Clinical trial | MF values with different superstructure’s material and cortical bone thickness |
| Alvarez-Arenal, A., 2009 [32] | Math. Comput. Model. | Clinical trial | Influence of mandibular movements and individual factors on MF values |
| Shinkai, R.S., 2007 [33] | Head Face Med. | Clinical trial | Influence of individual factors on MF values |
| Prasad, M., 2013 [34] | J. Nat. Sci. Biol. Med. | Clinical trial | Influence of individual factors on MF values |
| McDowell, J.A., 1961 [42] | J. Dent. Res. | Clinical trial | Influence of mandibular movements on MF values |
| Osborne, J., 1964 [43] | Br. Dent. J. | Clinical trial | MF measurement |
| Burch, J.G., 1970 [44] | J. Dent. Res. | Clinical trial | Influence of mandibular movements and individual factors on MF values |
| Novak, C.A., 1972 [45] | Dent. Stud. | Clinical trial | MF measurement |
| Fischman, B.M., 1976 [46] | J. Prosthet. Dent. | Clinical trial | MF reduces when fixed splints are present in natural dentition |
| Ferrario, V., 1992 [47] | J. Prosthet. Dent. | Clinical trial | Influence of individual factors on MF values |
| Hart, R.T., 1992 [48] | J. Biomech. | Clinical trial | Influence of individual factors on MF values |
| Korioth, T.W., 1992 [49] | Am. J. Phys. Anthropol. | Clinical trial | Influence of individual factors on MF values |
| Koolstra, J.H., 1995 [50] | J. Dent. Res. | Clinical trial | Influence of individual factors on MF values |
| Abdel-Latif, H.H., 2000 [51] | Int. J. Prosthodont. | Clinical trial | MF measurement |
| Kemkes-Grottenthaler, A., 2002 [52] | Homo | Clinical trial | Influence of individual factors on MF values |
| Jiang, T., 2002 [53] | J. Oral Rehabil. | Clinical trial | Influence of MF on connected prosthesis supported by natural tooth and implants |
| Zarone, F., 2003 [54] | Clin. Oral Implant. Res. | Clinical trial | Influence of MF on implants and superstructures in different fixed full-arch rehabilitations |
| Choi, A.H., 2005 [55] | Aust. Dent. J. | Clinical trial | Influence of mandibular movements on MF values |
| Balci, Y., 2005 [56] | Homo | Clinical trial | Influence of individual factors on MF values |
| Yokoyama, S., 2005 [57] | Int. J. Oral Maxillofac. Implant. | Clinical trial | Influence of MF on different superstructures in fixed full-arch rehabilitations |
| Al-Sukhun, J., 2006 [58] | J. Oral Maxillofac. Surg. | Clinical trial | Influence of mandibular movements on MF values |
| Al-Sukhun, J., 2007 [59] | Int. J. Oral Maxillofac. Implant. | Clinical trial | Influence of mandibular movements on MF values |
| El-Sheikh, A.M., 2007 [60] | Int. J. Oral Maxillofac. Implant. | Clinical trial | Influence of mandibular movements on MF values |
| Gulsahi, A., 2008 [61] | Dentomaxillofac. Radiol. | Clinical trial | Influence of individual factors on MF values |
| Naini, R.B., 2009 [62] | Implant. Dent. | Clinical trial | Influence of MF on different superstructures in fixed full-arch rehabilitations |
| Bellini, C.M., 2009 [63] | Int. J. Oral Maxillofac. Implant. | Clinical trial | Influence of MF on tilted and nontilted implant |
| Nokar, S., 2010 [64] | Int. J. Oral Maxillofac. Implant. | Clinical trial | Influence of MF on different superstructures in fixed full-arch rehabilitations |
| Zaugg, B., 2012 [65] | Clin. Oral Implant. Res. | Clinical trial | MF values in oral rehabilitation with posterior implants and natural teeth in anterior mandible |
| Madani, A.S., 2012 [66] | J. Dent. Mater. Tech. | Clinical trial | Influence of individual factors on MF values |
| Law, C., 2014 [67] | J. Prosthet. Dent. | Clinical trial | Influence of MF on the strain distribution in unilateral distal edentulisms |
| Lin, C., 2014 [68] | Forensic Sci. Int. | Clinical trial | Influence of individual factors on MF values |
| Martin-Fernandez, E., 2018 [69] | Biomed. Res. Int. | Clinical trial | Influence of superstructure type and different mandibular movements on MF in fixed implant rehabilitations |
| Shahriari, S., 2019 [70] | J. Long. Term. Eff. Med. Implant. | Clinical trial | Influence of MF on tilted and nontilted implant |
| Wolf, L., 2019 [71] | Int. J. Comput. Dent. | Clinical trial | Influence of mandibular movements and individual factors on MF values |
| Tulsani, M., 2020 [72] | Int. J. Dent. Oral Sci. | Clinical trial | Influence of mandibular movements on MF values |
| Ebadian, B., 2020 [73] | J. Indian Prosthodont. Soc. | Clinical trial | Influence of individual factors on MF values |
| Schmidt, A., 2021 [74] | Clin. Oral Investig. | Clinical trial | Influence of MF on different techniques of impression taking |
| Gülsoy, M., 2022 [75] | J. Adv. Prosthodont. | Clinical trial | Influence of individual factors on MF values |
| Gao, J., 2022 [76] | Front. Bioeng. Biotechnol. | Clinical trial | Influence of individual factors on MF values |
| Author, Year of Publication, and Reference | Type of Rehabilitation | Sample Size | Correlation between MF and Individual Factors * |
|---|---|---|---|
| Hylander, W.L., 1984 [7] | Natural dentition | 6 macaca fascicularis | Symphysis characteristics + |
| Canabarro Sde, A., 2006 [12] | Natural dentition | 80 | Gonial angle + Length of the mandibular structure + Sex - Age - MOF and parameters that modify it - |
| Shinkai, R., 2004 [17] | Natural dentition | 7 | Symphysis characteristics + |
| Hobkirk, J.A., 1998 [23] | Natural dentition | 3 | Facial type + |
| Hobkirk, J.A., 1991 [26] | Natural dentition | 3 | Facial type + Symphysis characteristics + |
| Custodio, W., 2011 [29] | Natural dentition | 78 | Facial type + |
| Chen, D.C., 2000 [30] | Natural dentition | 62 | Facial type + Gonial angle + Symphysis characteristics + Sex - MOF and parameters that modify it - |
| Shinkai, R.S., 2007 [33] | Natural dentition | 51 | Facial type - Sex + MOF and parameters that modify it - |
| Prasad, M., 2013 [34] | Natural dentition | 60 | Facial type + Sex - |
| Burch, J.G., 1970 [44] | Natural dentition | 10 | Age + |
| Ferrario, V., 1992 [47] | Natural dentition | 3D FEM | Age + |
| Hart, R.T., 1992 [48] | Natural dentition | 3D FEM | Age + |
| Korioth, T.W., 1992 [49] | Natural dentition | 3D FEM | Age + |
| Koolstra, J.H., 1995 [50] | Natural dentition | 3D FEM | Age + |
| Kemkes-Grottenthaler, A., 2002 [52] | Forensic mandibles and archaeological mandibles | 153 forensic mandibles and 80 archaeological mandibles | Sex + |
| Balci, Y., 2005 [56] | Forensic mandibles | 120 mandibles from forensic cases | Sex + |
| Gulsahi, A., 2008 [61] | Edentulous, partially, and full dentate patients | 1.863 | Sex + |
| Madani, A.S., 2012 [66] | Natural dentition and edentulous | 50 and 70 | Age - |
| Lin, C., 2014 [68] | Natural dentition | 3D FEM | Sex + |
| Wolf, L., 2019 [71] | Natural dentition | 40 | Sex - |
| Ebadian, B., 2020 [73] | Natural dentition | 90 | Age + Sex - MOF and parameters that modify it - |
| Gülsoy, M., 2022 [75] | Natural dentition and edentulous | 56 and 35 | Age - Sex - |
| Gao, J., 2022 [76] | Implant-supported fixed restorations | 3D FEM | Facial type + |
| Author, Year of Publication, and Reference | Type of Rehabilitation | Sample Size | Type of Movement * and Values of MMF |
|---|---|---|---|
| Burch, J.G., 1972 [1] | Natural dentition | 25 | Mouth opening 0.224 mm Protrusion 0.432 mm Lateral movements 0.112/0.105 mm |
| Gates, G.N., 1981 [6] | Natural dentition | 10 | Mouth opening 0–0.3 mm Protrusion 0.1–0.5 mm |
| Goodkind, R.J., 1973 [9] | Natural dentition | 40 | Mouth opening 0.031–0.076 mm |
| Regli, C.P., 1967 [10] | Natural dentition | 62 | Mouth opening 0.03–0.09 mm |
| Omar, R., 1981 [11] | Natural dentition | 10 | Mouth opening 0.012–0.164 mm |
| Canabarro Sde, A., 2006 [12] | Natural dentition | 80 | Mouth opening 0.146 mm Protrusion 0.15 mm |
| De Marco, T.J., 1974 [14] | Natural dentition | 25 | Mouth opening 0.78 mm |
| Fischman, B., 1990 [15] | Natural dentition | 10 | Mouth opening 0.0711 mm |
| Shinkai, R., 2004 [17] | Natural dentition | 7 | Mouth opening 0.21–0.44 mm |
| Horiuchi, M., 1997 [27] | Natural dentition | 4 | Mouth opening 0.016 mm Protrusion 0.010–0.037 mm |
| Chen, D.C., 2000 [30] | Natural dentition | 62 | Mouth opening 0.145 mm |
| McDowell, J.A., 1961 [42] | Natural dentition | 20 | Mouth opening 0.4 mm Protrusion 0.5 mm |
| Osborne, J., 1964 [43] | Natural dentition | 18 | Mouth opening 0.07 mm |
| Burch, J.G., 1970 [44] | Natural dentition | 10 | Mouth opening 0.438 mm Protrusion 0.61 mm Lateral movements 0.243/0.257 mm |
| Novak, C.A., 1972 [45] | Natural dentition | 50 | Mouth opening 1.00 mm |
| Choi, A.H., 2005 [55] | Edentulous mandible with implants | 3D FEM | Mouth opening 0.168 mm in the first molar region and 0.256 mm in the second molar region |
| Al-Sukhun, J., 2006 [58] | Edentulous patients with implants | 12 | Mouth opening 0.011–0.052 mm Protrusion 0.025–0.057 mm |
| Al-Sukhun, J., 2007 [59] | Edentulous patients with implants | 12 | Mouth opening 0.8 mm Protrusion 1.07 mm Lateral movements 1.1/0.9 mm |
| El-Sheikh, A.M., 2007 [60] | Edentulous patients with implants | 5 | Mouth opening 0.025–0.042 mm Protrusion 0.018–0.053 mm Lateral movements 0.010–0.021 mm |
| Madani, A.S., 2012 [66] | Natural dentition and edentulous | 50 and 70 | Mouth opening 0.078–0.751 mm |
| Wolf, L., 2019 [71] | Natural dentition | 40 | Mouth opening 0.011–0.232 mm |
| Tulsani, M., 2020 [72] | Natural dentition | 140 | Mouth opening 0.363 mm Protrusion 0.973 mm |
| Author, Year of Publication, and Reference | Type of Rehabilitation | Sample Size | Results in Favour of D/U 1 |
|---|---|---|---|
| Zarone, F., 2003 [54] | Full-arch 6-implant-supported rehabilitation | 1 | D |
| Yokoyama, S., 2005 [57] | Full-arch 8-implant-supported rehabilitation | 3D FEM | U |
| Naini, R.B., 2009 [62] | Full-arch 5-implant-supported rehabilitation | 3D FEM | D |
| Nokar, S., 2010 [64] | Full-arch 6-implant-supported rehabilitation | 3D FEM | D |
| Martin-Fernandez, E., 2018 [69] | Full-arch 6-implant-supported rehabilitation | 3D FEM | U |
| Gao, J., 2022 [76] | Full-arch implant-supported rehabilitation | 3D FEM | U |
| Studies | Bias Due to Confounding | Bias in Selection of Participants | Bias in Measurement Classification of Interventions | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias Due to Selection of the Reported Result |
|---|---|---|---|---|---|---|---|
| Burch, J.G., 1972 [1] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Gates, G.N., 1981 [6] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Hylander, W.L., 1984 [7] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Goodkind, R.J., 1973 [9] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Regli, C.P., 1967 [10] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Omar, R., 1981 [11] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Canabarro Sde, A., 2006 [12] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| De Marco, T.J., 1974 [14] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Fischman, B., 1990 [15] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Shinkai, R., 2004 [17] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Hobkirk, J.A., 1998 [23] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Hobkirk, J.A., 1991 [26] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Horiuchi, M., 1997 [27] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Custodio, W., 2011 [29] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Chen, D.C., 2000 [30] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Favot, L.M., 2014 [31] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Alvarez-Arenal, A., 2009 [32] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Shinkai, R.S., 2007 [33] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Prasad, M., 2013 [34] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| McDowell, J.A., 1961 [42] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Osborne, J., 1964 [43] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Burch, J.G., 1970 [44] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Novak, C.A., 1972 [45] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Fischman, B.M., 1976 [46] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Ferrario, V., 1992 [47] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Hart, R.T., 1992 [48] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Korioth, T.W., 1992 [49] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Koolstra, J.H., 1995 [50] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Abdel-Latif, H.H., 2000 [51] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Kemkes-Grottenthaler, A., 2002 [52] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Jiang, T., 2002 [53] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Zarone, F., 2003 [54] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Choi, A.H., 2005 [55] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Balci, Y., 2005 [56] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Yokoyama, S., 2005 [57] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Al-Sukhun, J., 2006 [58] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Al-Sukhun, J., 2007 [59] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| El-Sheikh, A.M., 2007 [60] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Gulsahi, A., 2008 [61] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Naini, R.B., 2009 [62] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Bellini, C.M., 2009 [63] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Nokar, S., 2010 [64] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Zaugg, B., 2012 [65] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Madani, A.S., 2012 [66] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Law, C., 2014 [67] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Lin, C., 2014 [68] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Martin-Fernandez, E., 2018 [69] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Shahriari, S., 2019 [70] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Wolf, L., 2019 [71] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Tulsani, M., 2020 [72] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Ebadian, B., 2020 [73] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Schmidt, A., 2021 [74] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Gülsoy, M., 2022 [75] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Gao, J., 2022 [76] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Risk of bias judgements | MODERATE | SERIOUS | MODERATE | LOW | MODERATE | MODERATE | MODERATE |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caggiano, M.; D’Ambrosio, F.; Acerra, A.; Giudice, D.; Giordano, F. Biomechanical Implications of Mandibular Flexion on Implant-Supported Full-Arch Rehabilitations: A Systematic Literature Review. J. Clin. Med. 2023, 12, 5302. https://doi.org/10.3390/jcm12165302
Caggiano M, D’Ambrosio F, Acerra A, Giudice D, Giordano F. Biomechanical Implications of Mandibular Flexion on Implant-Supported Full-Arch Rehabilitations: A Systematic Literature Review. Journal of Clinical Medicine. 2023; 12(16):5302. https://doi.org/10.3390/jcm12165302
Chicago/Turabian StyleCaggiano, Mario, Francesco D’Ambrosio, Alfonso Acerra, David Giudice, and Francesco Giordano. 2023. "Biomechanical Implications of Mandibular Flexion on Implant-Supported Full-Arch Rehabilitations: A Systematic Literature Review" Journal of Clinical Medicine 12, no. 16: 5302. https://doi.org/10.3390/jcm12165302