

A Change in Global Sagittal Alignment after Transforaminal Epidural Steroid Injections in Lumbar Spinal Stenosis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Radiological Measurement
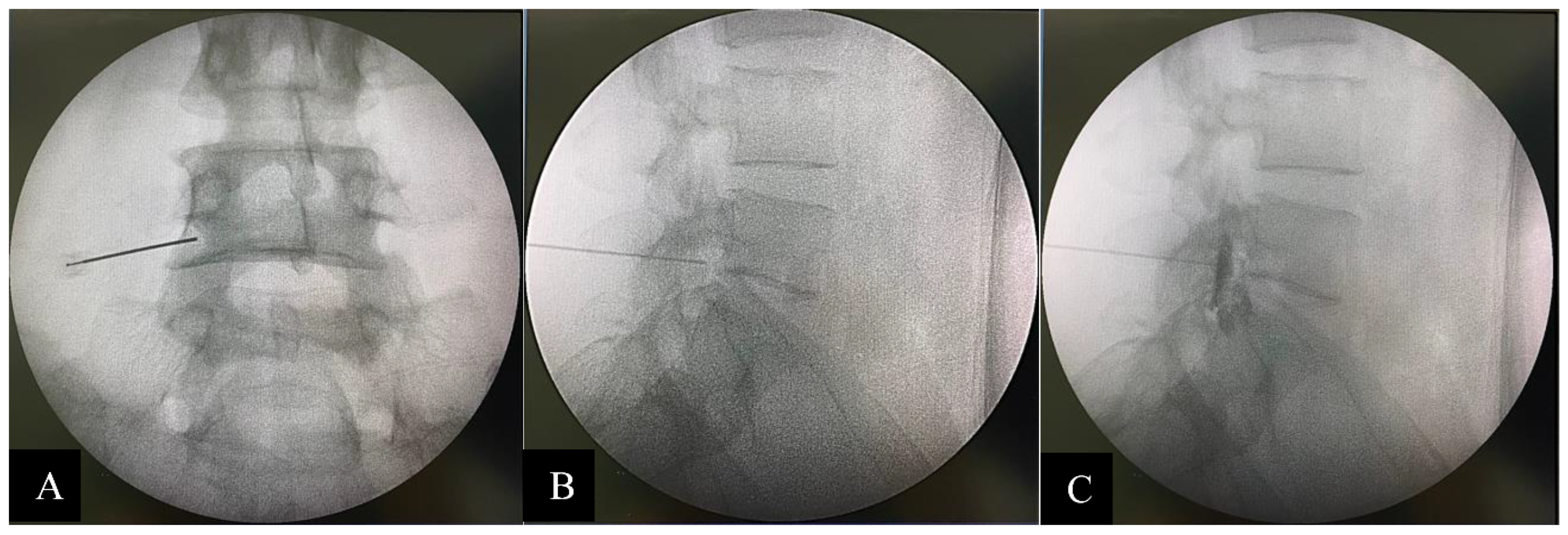
2.2. Intervention
2.3. Statistical Analysis
3. Results
3.1. Pre-Intervention and Post-Intervention Outcomes
3.2. Difference between the Number of Injection Levels and Sagittal Parameters
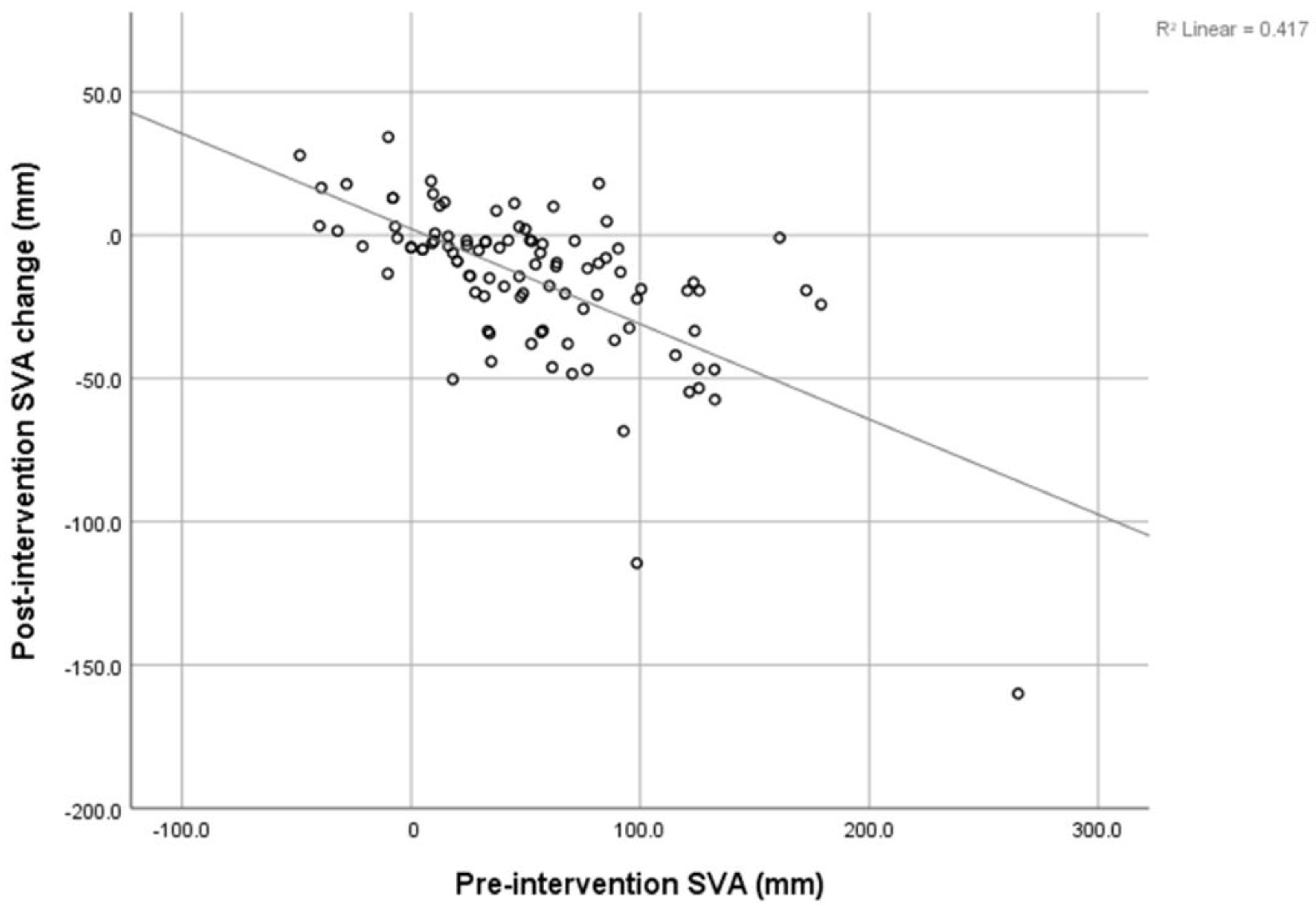
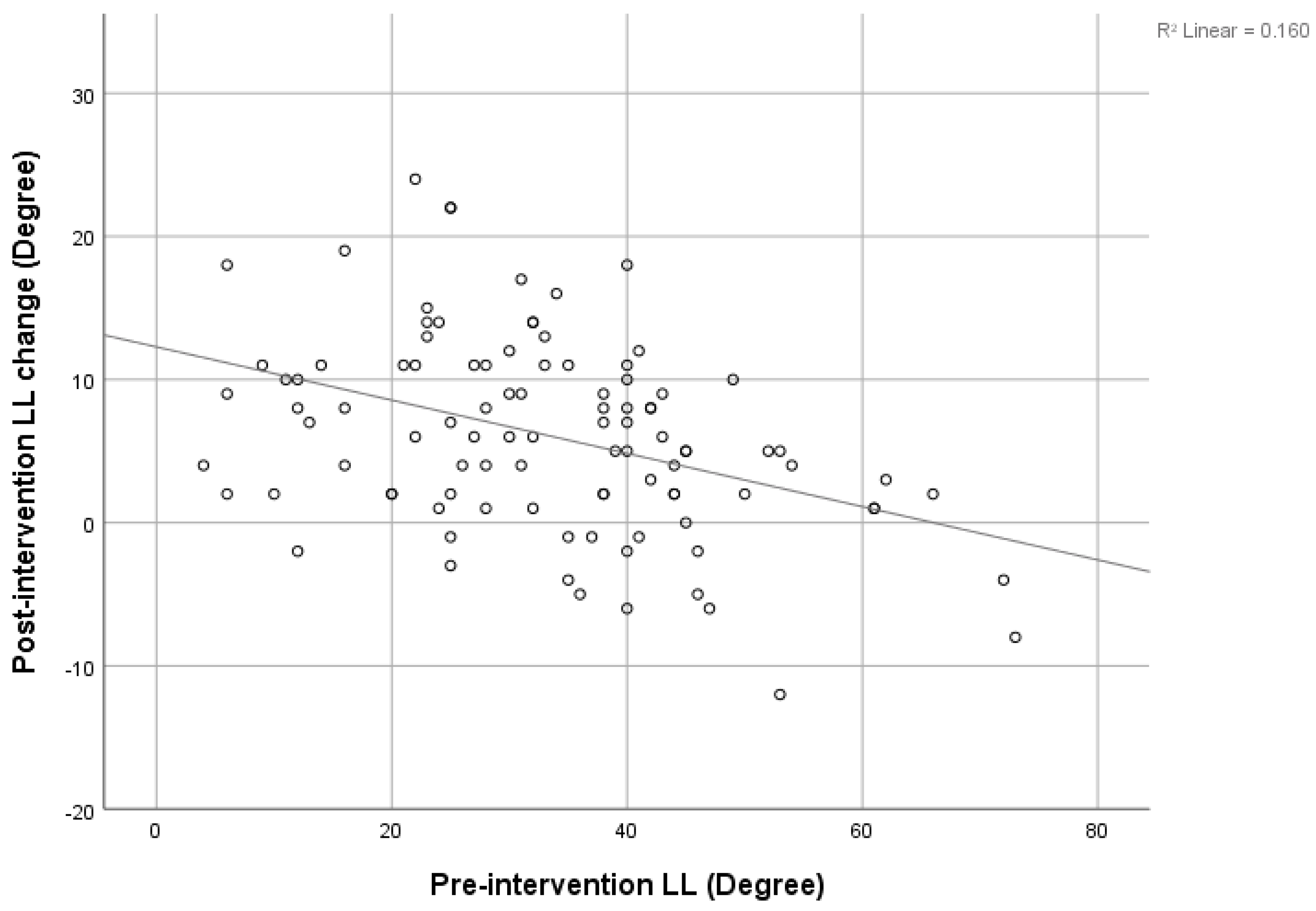
3.3. Correlation between Sagittal Parameters
3.4. Interobserver Reliability
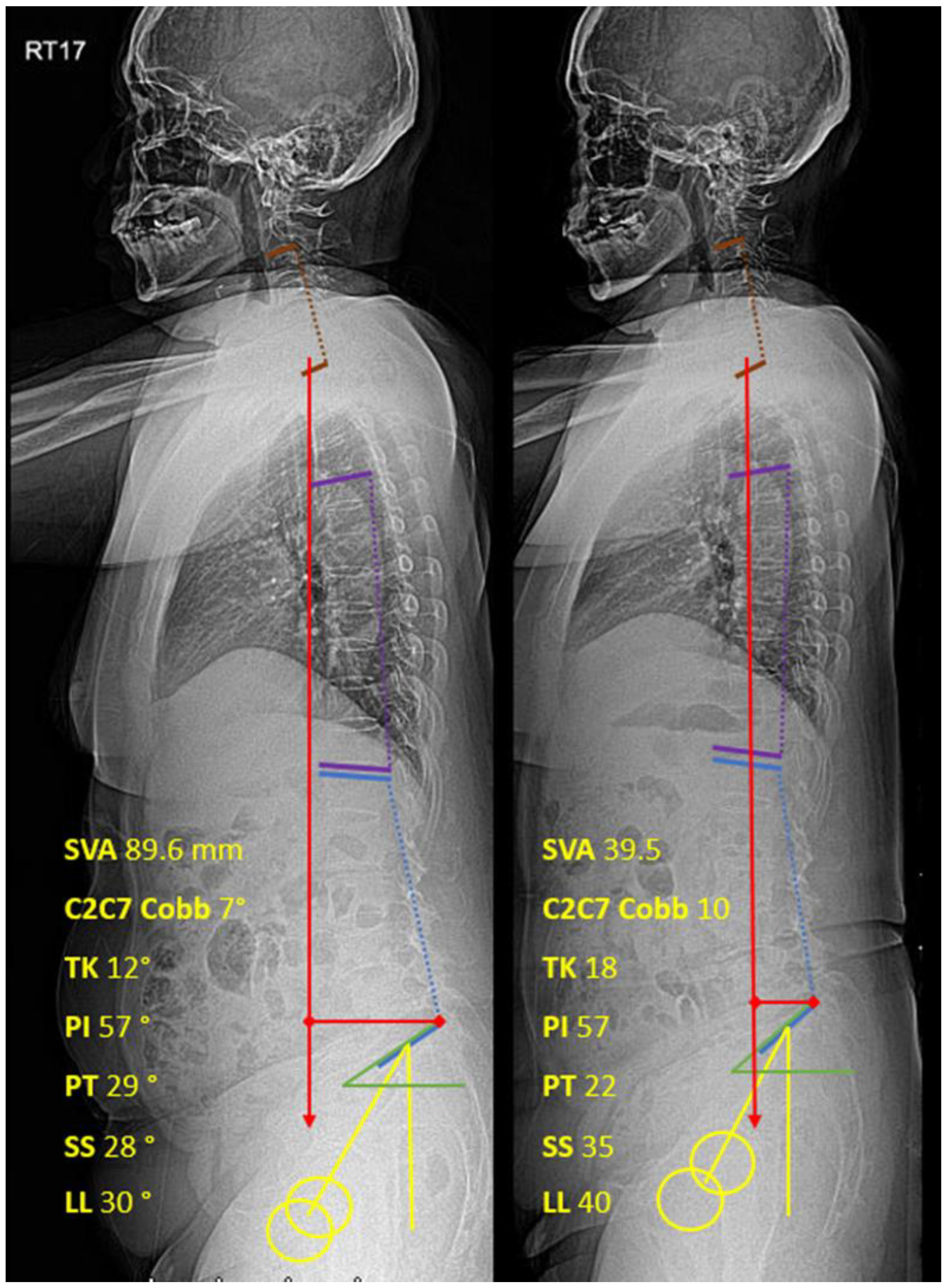
3.5. Case Example
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Iyer, S.; Sheha, E.; Fu, M.C.; Varghese, J.; Cunningham, M.E.; Albert, T.J.; Schwab, F.J.; Lafage, V.C.; Kim, H.J. Sagittal Spinal Alignment in Adult Spinal Deformity: An Overview of Current Concepts and a Critical Analysis Review. JBJS Rev. 2018, 6, e2. [Google Scholar] [CrossRef] [PubMed]
- Harroud, A.; Labelle, H.; Joncas, J.; Mac-Thiong, J.M. Global sagittal alignment and health-related quality of life in lumbosacral spondylolisthesis. Eur. Spine J. 2013, 22, 849–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwab, F.; Lafage, V.; Patel, A.; Farcy, J.P. Sagittal plane considerations and the pelvis in the adult patient. Spine 2009, 34, 1828–1833. [Google Scholar] [CrossRef]
- Yeh, K.T.; Lee, R.P.; Chen, H.; Yu, T.C.; Liu, K.L.; Peng, C.H.; Wang, J.H.; Wu, W.T. Correlation of Functional Outcomes and Sagittal Alignment After Long Instrumented Fusion for Degenerative Thoracolumbar Spinal Disease. Spine 2018, 43, 1355–1362. [Google Scholar] [CrossRef] [PubMed]
- Pourtaheri, S.; Sharma, A.; Savage, J.; Kalfas, I.; Mroz, T.E.; Benzel, E.; Steinmetz, M.P. Pelvic retroversion: A compensatory mechanism for lumbar stenosis. J. Neurosurg. Spine 2017, 27, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Schonstrom, N.; Lindahl, S.; Willen, J.; Hansson, T. Dynamic changes in the dimensions of the lumbar spinal canal: An experimental study in vitro. J. Orthop. Res. 1989, 7, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Miao, J.; Wang, S.; Park, W.M.; Xia, Q.; Fang, X.; Torriani, M.P.; Wood, K.B.; Li, G. Segmental spinal canal volume in patients with degenerative spondylolisthesis. Spine J. 2013, 13, 706–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujii, K.; Kawamura, N.; Ikegami, M.; Niitsuma, G.; Kunogi, J. Radiological improvements in global sagittal alignment after lumbar decompression without fusion. Spine 2015, 40, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Endo, K.; Suzuki, H.; Tanaka, H.; Kang, Y.; Yamamoto, K. Sagittal spinal alignment in patients with lumbar disc herniation. Eur. Spine J. 2010, 19, 435–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, C.; Sun, J.; Cui, X.; Jiang, Z.; Zhang, W.; Li, T. Spinal sagittal imbalance in patients with lumbar disc herniation: Its spinopelvic characteristics, strength changes of the spinal musculature and natural history after lumbar discectomy. BMC Musculoskelet. Disord. 2016, 17, 305. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.H.; Chung, C.K.; Park, S.B.; Yang, S.H.; Kim, J.H. A Change in Lumbar Sagittal Alignment After Single-level Anterior Lumbar Interbody Fusion for Lumbar Degenerative Spondylolisthesis with Normal Sagittal Balance. Clin. Spine Surg. 2017, 30, 291–296. [Google Scholar] [CrossRef]
- Manchikanti, L.; Kaye, A.D.; Manchikanti, K.; Boswell, M.; Pampati, V.; Hirsch, J. Efficacy of epidural injections in the treatment of lumbar central spinal stenosis: A systematic review. Anesth. Pain Med. 2015, 5, e23139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, N.; Hourigan, P.; Clarke, A. Transforaminal epidural steroid injection in lumbar spinal stenosis: An observational study with two-year follow-up. Br. J. Neurosurg. 2017, 31, 205–208. [Google Scholar] [CrossRef]
- Bartleson, J.D.; Maus, T.P. Diagnostic and therapeutic spinal interventions: Epidural injections. Neurol. Clin. Pract. 2014, 4, 347–352. [Google Scholar] [CrossRef] [Green Version]
- Sanjaroensuttikul, N. The Oswestry low back pain disability questionnaire (version 1.0) Thai version. J. Med. Assoc. Thai. 2007, 90, 1417–1422. [Google Scholar] [PubMed]
- Lafage, V.; Schwab, F.; Vira, S.; Patel, A.; Ungar, B.; Farcy, J.P. Spino-pelvic parameters after surgery can be predicted: A preliminary formula and validation of standing alignment. Spine 2011, 36, 1037–1045. [Google Scholar] [CrossRef] [PubMed]
- Alijani, B.; Rasoulian, J. The Sagittal Balance of the Cervical Spine: Radiographic Analysis of Interdependence between the Occipitocervical and Spinopelvic Alignment. Asian Spine J. 2020, 14, 287. [Google Scholar] [CrossRef] [Green Version]
- Lee, I.S.; Kim, S.H.; Lee, J.W.; Hong, S.H.; Choi, J.Y.; Kang, H.S.; Song, J.W.; Kwon, A.K. Comparison of the temporary diagnostic relief of transforaminal epidural steroid injection approaches: Conventional versus posterolateral technique. AJNR Am. J. Neuroradiol. 2007, 28, 204–208. [Google Scholar]
- Lutz, G.E.; Vad, V.B.; Wisneski, R.J. Fluoroscopic transforaminal lumbar epidural steroids: An outcome study. Arch. Phys. Med. Rehabil. 1998, 79, 1362–1366. [Google Scholar] [CrossRef]
- Mukaka, M.M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar]
- Ghahreman, A.; Ferch, R.; Bogduk, N. The efficacy of transforaminal injection of steroids for the treatment of lumbar radicular pain. Pain Med. 2010, 11, 1149–1168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabatas, S.; Cansever, T.; Yilmaz, C.; Kocyigit, O.I.; Coskun, E.; Demircay, E.; Akar, A.; Caner, H. Transforaminal epidural steroid injection via a preganglionic approach for lumbar spinal stenosis and lumbar discogenic pain with radiculopathy. Neurol. India 2010, 58, 248–252. [Google Scholar] [CrossRef]
- McCormick, Z.; Kennedy, D.J.; Garvan, C.; Rivers, E.; Temme, K.; Margolis, S.; Zander, E.; Rohr, A.; Smith, M.C.; Plastaras, C. Comparison of Pain Score Reduction Using Triamcinolone vs. Betamethasone in Transforaminal Epidural Steroid Injections for Lumbosacral Radicular Pain. Am. J. Phys. Med. Rehabil. 2015, 94, 1058–1064. [Google Scholar] [CrossRef]
- Karppinen, J.; Malmivaara, A.; Kurunlahti, M.; Kyllönen, E.; Pienimäki, T.; Nieminen, P.; Ohinmaa, A.; Tervonen, O.; Vanharanta, H. Periradicular infiltration for sciatica: A randomized controlled trial. Spine 2001, 26, 1059–1067. [Google Scholar] [CrossRef]
- Salimi, H.; Toyoda, H.; Yamada, K.; Terai, H.; Hoshino, M.; Suzuki, A.; Takahashi, S.; Tamai, K.; Hori, Y.; Yabu, A.; et al. The effect of minimally invasive lumbar decompression surgery on sagittal spinopelvic alignment in patients with lumbar spinal stenosis: A 5-year follow-up study. J. Neurosurg. Spine 2021, 35, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.H.; Joo, Y.S.; Lim, C.; Hwang, C.J.; Lee, D.H.; Lee, C.S. Effect of one- or two-level posterior lumbar interbody fusion on global sagittal balance. Spine J. 2017, 17, 1794–1802. [Google Scholar] [CrossRef] [PubMed]
- Enomoto, M.; Ukegawa, D.; Sakaki, K.; Tomizawa, S.; Arai, Y.; Kawabata, S.; Kato, T.; Yoshii, T.; Shinomiya, K.; Okawa, A. Increase in paravertebral muscle activity in lumbar kyphosis patients by surface electromyography compared with lumbar spinal canal stenosis patients and healthy volunteers. J. Spinal Disord. Tech. 2012, 25, E167–E173. [Google Scholar] [CrossRef]
- Masaki, M.; Ikezoe, T.; Yanase, K.; Ji, X.; Umehara, J.; Aoyama, J.; Minami, S.; Fukumoto, Y.; Watanabe, Y.; Kimura, M.; et al. Association of Pain History and Current Pain with Sagittal Spinal Alignment and Muscle Stiffness and Muscle Mass of the Back Muscles in Middle-aged and Elderly Women. Clin. Spine Surg. 2019, 32, E346–E352. [Google Scholar] [CrossRef]
- Makhni, M.C.; Shillingford, J.N.; Laratta, J.L.; Hyun, S.J.; Kim, Y.J. Restoration of Sagittal Balance in Spinal Deformity Surgery. J. Korean Neurosurg. Soc. 2018, 61, 167–179. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Kim, K.T.; Suk, K.S.; Lee, S.H.; Jeong, B.O.; Kim, J.S.; Eoh, J.H.; Kim, Y.J. Analysis of spinopelvic parameters in lumbar degenerative kyphosis: Correlation with spinal stenosis and spondylolisthesis. Spine 2010, 35, E1386–E1391. [Google Scholar] [CrossRef]
- Suzuki, H.; Endo, K.; Kobayashi, H.; Tanaka, H.; Yamamoto, K. Total sagittal spinal alignment in patients with lumbar canal stenosis accompanied by intermittent claudication. Spine 2010, 35, E344–E346. [Google Scholar] [CrossRef] [PubMed]
- Lafage, V.; Smith, J.S.; Bess, S.; Schwab, F.J.; Ames, C.P.; Klineberg, E.; Arlet, V.; Hostin, R.; Burton, D.C.; Shaffrey, C.I.; et al. Sagittal spino-pelvic alignment failures following three column thoracic osteotomy for adult spinal deformity. Eur. Spine J. 2012, 21, 698–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Pre-Intervention | Post-Intervention | p-Value α |
|---|---|---|---|
| VAS | 8.31 ± 1.11 | 3.38 ± 1.47 | <0.001 |
| ODI | 31.06 ± 3.48 | 18.03 ± 4.17 | <0.001 |
| SVA, mm | 53.26 ± 51.67 | 37.22 ± 40.71 | <0.001 |
| C2C7 Cobb | 12.15 ± 10.86 | 13.63 ± 10.26 | 0.004 |
| TK ๐ | 19.22 ± 10.80 | 20.9 ± 10.46 | 0.001 |
| PI ๐ | 56.25 ± 10.18 | 56.31 ± 10.13 | 0.296 |
| PT ๐ | 28.65 ± 10.17 | 23.66 ± 9.96 | <0.001 |
| SS ๐ | 27.61 ± 9.00 | 32.65 ± 8.36 | <0.001 |
| LL ๐ | 33.35 ± 14.80 | 39.56 ± 13.34 | <0.001 |
| PI—LL ๐ | 22.89 ± 16.35 | 16.75 ± 14.82 | <0.001 |
| Parameter | Number of TFESI Injection Levels | |||||
|---|---|---|---|---|---|---|
| 1 (n = 40) | 2 (n = 42) | 3 (n = 14) | 4 (n = 3) | p Value α | ||
| Pre-intervention | VAS | 8.30 ± 1.04 | 8.17 ± 1.15 | 8.71 ± 1.14 | 8.67 ± 1.53 | 0.42 |
| ODI | 30.93 ± 2.76 | 30.74 ± 3.78 | 32.29 ± 3.79 | 31.67 ± 7.23 | 0.53 | |
| SVA | 25.59 ± 33.29 | 64.08 ± 45.29 | 72.44 ± 57.25 | 164.76 ± 98.35 | <0.001 | |
| C2C7 cobb | 12.05 ± 8.45 | 11.12 ± 10.93 | 13.57 ± 6.76 | 19.00 ± 39.15 | 0.619 | |
| TK | 19.40 ± 8.90 | 16.60 ± 11.45 | 18.21 ± 12.25 | 10.00 ± 8.71 | 0.487 | |
| PI | 56.55 ± 8.59 | 53.81 ± 9.31 | 60.57 ± 12.15 | 67.33 ± 13.61 | 0.027 | |
| PT | 2.45 ± 9.65 | 28.19 ± 8.78 | 36.14 ± 9.21 | 44.61 ± 13.78 | <0.001 | |
| SS | 31.13 ± 8.26 | 25.69 ± 9.18 | 24.43 ± 7.98 | 22.67 ± 0.57 | 0.011 | |
| LL | 39.5 ± 13.57 | 30.90 ± 12.76 | 27.0 ± 15.80 | 12.33 ± 1.52 | <0.001 | |
| PI-LL | 17.05 ± 15.38 | 22.90 ± 12.46 | 33.57 ± 16.79 | 55.0 ± 14.93 | <0.001 | |
| Post-intervention | VAS | 3.17 ± 1.50 | 3.37 ± 1.48 | 3.69 ± 1.10 | 5.00 ± 1.73 | 0.17 |
| ODI | 17.47 ± 3.70 | 17.69 ± 4.42 | 19.84 ± 3.93 | 22.33 ± 4.93 | 0.08 | |
| SVA | 19.34 ± 28.96 | 44.8 ± 39.30 | 53.22 ± 47.44 | 97.76 ± 64.28 | 0.0002 | |
| C2C7 cobb | 13.70 ± 8.30 | 13.27 ± 10.67 | 13.5 ± 8.46 | 17.83 ± 31.05 | 0.907 | |
| TK | 21.83 ± 8.60 | 21.83 ± 10.93 | 18.19 ± 13 | 6.83 ± 4.25 | 0.071 | |
| PI | 56.7 ± 8.78 | 54.13 ± 9.98 | 59.84 ± 12.5 | 67.16 ± 11.62 | 0.067 | |
| PT | 20.8 ± 8.73 | 23.40 ± 9.24 | 29.00 ± 10.57 | 41.00 ± 10.44 | 0.0007 | |
| SS | 35.88 ± 6.75 | 30.60 ± 8.84 | 30.84 ± 9.22 | 26.16 ± 1.60 | 0.011 | |
| LL | 43.78 ± 11.85 | 38.61 ± 12.8 | 33.61 ± 15.67 | 22.5 ± 3.5 | 0.006 | |
| PI-LL | 12.9 ± 13.21 | 15.52 ± 12.01 | 26.23 ± 18.3 | 44.67 ± 14.9 | 0.0001 | |
| Post-Intervention Change | VAS | ODI | SVA | PT | LL | PI-LL | |
|---|---|---|---|---|---|---|---|
| Pre-Intervention | |||||||
| VAS | −0.444 * | −0.104 | −0.04 | −0.151 | 0.034 | −0.038 | |
| ODI | −0.18 | −0.43 * | −0.255 | 0.048 | 0.104 | −0.104 | |
| SVA | 0.268 | 0.133 | −0.646 * | 0.097 | 0.34 * | −0.298 | |
| PI | 0.151 | −0.004 | −0.231 | 0.037 | 0.060 | −0.041 | |
| PT | 0.238 | 0.197 | −0.253 | −0.317 * | 0.226 | −0.226 | |
| LL | −0.236 | −0.264 | 0.260 | 0.162 | −0.4 * | 0.411 * | |
| PI-LL | 0.304 * | 0.235 | −0.374 * | −0.123 | 0.369 * | −0.394 * | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manakul, P.; Siribumrungwong, K.; Dhanachanvisith, N. A Change in Global Sagittal Alignment after Transforaminal Epidural Steroid Injections in Lumbar Spinal Stenosis. J. Clin. Med. 2023, 12, 4727. https://doi.org/10.3390/jcm12144727
Manakul P, Siribumrungwong K, Dhanachanvisith N. A Change in Global Sagittal Alignment after Transforaminal Epidural Steroid Injections in Lumbar Spinal Stenosis. Journal of Clinical Medicine. 2023; 12(14):4727. https://doi.org/10.3390/jcm12144727
Chicago/Turabian StyleManakul, Park, Koopong Siribumrungwong, and Naphakkhanith Dhanachanvisith. 2023. "A Change in Global Sagittal Alignment after Transforaminal Epidural Steroid Injections in Lumbar Spinal Stenosis" Journal of Clinical Medicine 12, no. 14: 4727. https://doi.org/10.3390/jcm12144727