
The Multifold Etiologies of Limbal Stem Cell Deficiency: A Comprehensive Review on the Etiologies and Additional Treatment Options for Limbal Stem Cell Deficiency
 , , , and
, , , and 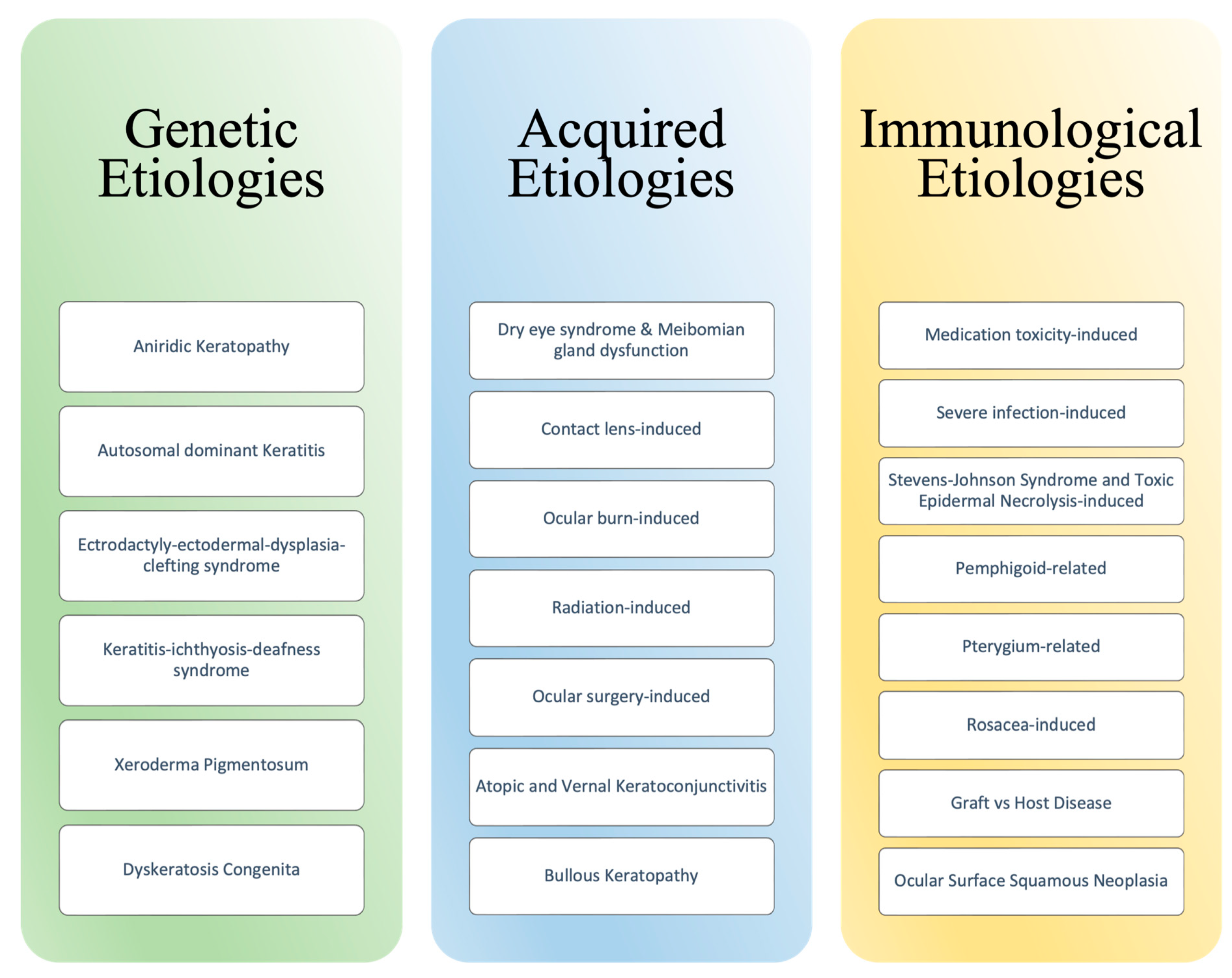{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Limbal Stem Cells
3. Pathophysiology
4. Incidence and Prevalence
5. Clinical Presentation
6. Diagnosis and Prognosis
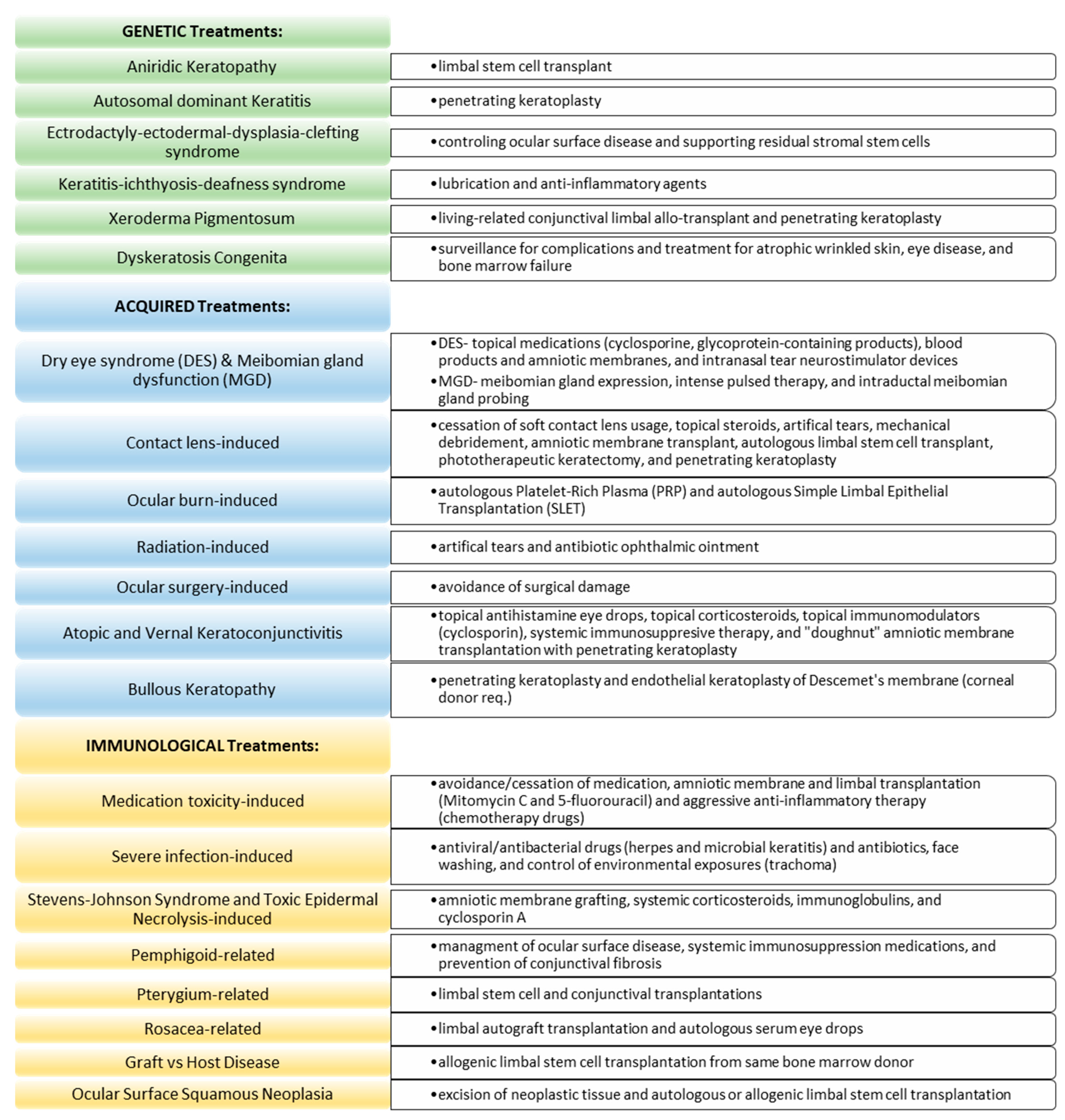
7. Treatment Overview
8. Etiologies and Additional Treatments
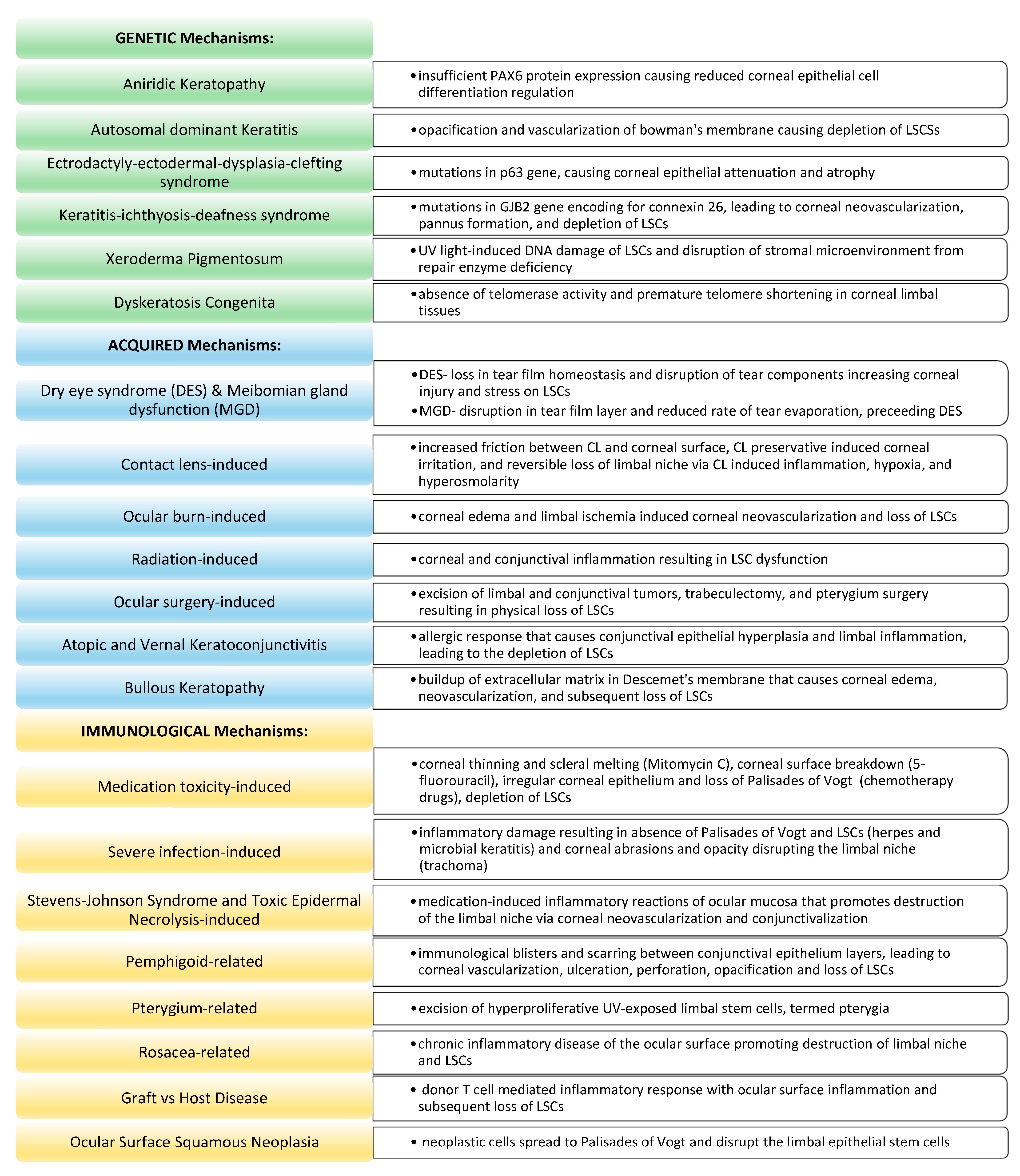
8.1. Genetic Etiologies of LSCD
8.1.1. Aniridic Keratopathy
8.1.2. Autosomal Dominant Keratitis
8.1.3. Ectrodactyly–Ectodermal Dysplasia–Clefting Syndrome
8.1.4. Keratitis–Ichthyosis–Deafness Syndrome
8.1.5. Xeroderma Pigmentosum
8.1.6. Dyskeratosis Congenita
8.2. Acquired Etiologies of LSCD
8.2.1. Dry Eye Syndrome and Meibomian Gland Dysfunction
8.2.2. Contact Lens-Induced LSCD
8.2.3. Ocular Burn-Induced LSCD
8.2.4. Radiation-Induced LSCD
8.2.5. Ocular Surgery-Induced LSCD
8.2.6. Atopic and Vernal Keratoconjunctivitis
8.2.7. Bullous Keratopathy
8.3. Immunologic Etiologies of LSCD
8.3.1. Medication Toxicity-Induced LSCD
8.3.2. Severe Infection-Induced LSCD
8.3.3. Stevens–Johnson Syndrome and Toxic Epidermal Necrolysis-Induced LSC
8.3.4. Pemphigoid-Related LSCD
8.3.5. Pterygium-Related LSCD
8.3.6. Rosacea-Induced LSCD
8.3.7. Graft vs. Host Disease
8.3.8. Ocular Surface Squamous Neoplasia
9. Conclusions
10. Literature Search
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Nurkovic, J.S.; Vojinovic, R.; Dolicanin, Z. Corneal Stem Cells as a Source of Regenerative Cell-Based Therapy. Stem Cells Int. 2020, 2020, 8813447. [Google Scholar] [CrossRef]
- Le, Q.; Xu, J.; Deng, S.X. The diagnosis of limbal stem cell deficiency. Ocul. Surf. 2018, 16, 58–69. [Google Scholar] [CrossRef]
- Puangsricharern, V.; Tseng, S.C.G. Cytologlogic Evidence of Corneal Diseases with Limbal Stem Cell Deficiency. Ophthalmology 1995, 102, 1476–1485. [Google Scholar] [CrossRef]
- Liu, X.N.; Mi, S.L.; Chen, Y.; Wang, Y. Corneal stromal mesenchymal stem cells: Reconstructing a bioactive cornea and repairing the corneal limbus and stromal microenvironment. Int. J. Ophthalmol. 2021, 14, 448–455. [Google Scholar] [CrossRef]
- Funderburgh, J.L.; Funderburgh, M.L.; Du, Y. Stem Cells in the Limbal Stroma. Ocul. Surf. 2016, 14, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, G.; Sasamoto, Y.; Ksander, B.R.; Frank, M.H.; Frank, N.Y. Limbal stem cells: Identity, developmental origin, and therapeutic potential. Wiley Interdiscip. Rev. Dev. Biol. 2018, 7, e303. [Google Scholar] [CrossRef]
- Altshuler, A.; Amitai-Lange, A.; Tarazi, N.; Dey, S.; Strinkovsky, L.; Hadad-Porat, S.; Bhattacharya, S.; Nasser, W.; Imeri, J.; Ben-David, G.; et al. Discrete limbal epithelial stem cell populations mediate corneal homeostasis and wound healing. Cell Stem Cell 2021, 28, 1248–1261.e8. [Google Scholar] [CrossRef]
- Pajoohesh-Ganji, A.; Pal-Ghosh, S.; Tadvalkar, G.; Stepp, M.A. Corneal goblet cells and their niche: Implications for corneal stem cell deficiency. Stem Cells 2012, 30, 2032–2043. [Google Scholar] [CrossRef] [Green Version]
- Ramos, T.; Scott, D.; Ahmad, S. An Update on Ocular Surface Epithelial Stem Cells: Cornea and Conjunctiva. Stem Cells Int. 2015, 2015, 601731. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, S. Concise Review: Limbal Stem Cell Deficiency, Dysfunction, and Distress. Stem Cells Transl. Med. 2012, 1, 110–115. [Google Scholar] [CrossRef]
- Shanbhag, S.S.; Chanda, S.; Donthineni, P.R.; Basu, S. Surgical Management of Unilateral Partial Limbal Stem Cell Deficiency: Conjunctival Autografts versus Simple Limbal Epithelial Transplantation. Clin. Ophthalmol. 2021, 15, 4389–4397. [Google Scholar] [CrossRef]
- Lim, P.; Fuchsluger, T.A.; Jurkunas, U.V. Limbal stem cell deficiency and corneal neovascularization. Semin. Ophthalmol. 2009, 24, 139–148. [Google Scholar] [CrossRef]
- Tseng, S.C. Concept and application of limbal stem cells. Eye 1989, 3, 141–157. [Google Scholar] [CrossRef] [Green Version]
- Vazirani, J.; Nair, D.; Shanbhag, S.; Wurity, S.; Ranjan, A.; Sangwan, V. Limbal Stem Cell Deficiency-Demography and Underlying Causes. Am. J. Ophthalmol. 2018, 188, 99–103. [Google Scholar] [CrossRef]
- Cheung, A.Y.; Sarnicola, E.; Denny, M.R.; Sepsakos, L.; Auteri, N.J.; Holland, E.J. Limbal Stem Cell Deficiency: Demographics and Clinical Characteristics of a Large Retrospective Series at a Single Tertiary Referral Center. Cornea 2021, 40, 1521–1531. [Google Scholar] [CrossRef]
- Bonnet, C.; Roberts, J.S.; Deng, S.X. Limbal stem cell diseases. Exp. Eye Res. 2021, 205, 108437. [Google Scholar] [CrossRef]
- Lee, S.C.; Hyon, J.Y.; Jeon, H.S. Contact Lens Induced Limbal Stem Cell Deficiency: Clinical Features in Korean Patients. Korean J. Ophthalmol. 2019, 33, 500–505. [Google Scholar] [CrossRef] [Green Version]
- Osei-Bempong, C.; Figueiredo, F.C.; Lako, M. The limbal epithelium of the eye–A review of limbal stem cell biology, disease and treatment. BioEssays 2013, 35, 211–219. [Google Scholar] [CrossRef]
- Deng, S.X.; Borderie, V.; Chan, C.C.; Dana, R.; Figueiredo, F.C.; Gomes, J.A.P.; Pellegrini, G.; Shimmura, S.; Kruse, F.E. Global Consensus on Definition, Classification, Diagnosis, and Staging of Limbal Stem Cell Deficiency. Cornea 2019, 38, 364–375. [Google Scholar] [CrossRef]
- Kate, A.; Basu, S. A Review of the Diagnosis and Treatment of Limbal Stem Cell Deficiency. Front. Med. 2022, 9, 836009. [Google Scholar] [CrossRef]
- Le, Q.; Chauhan, T.; Yung, M.; Tseng, C.H.; Deng, S.X. Outcomes of Limbal Stem Cell Transplant. JAMA Ophthalmol. 2020, 138, 660. [Google Scholar] [CrossRef]
- Masood, F.; Chang, J.-H.; Akbar, A.; Song, A.; Hu, W.-Y.; Azar, D.T.; Rosenblatt, M.I. Therapeutic Strategies for Restoring Perturbed Corneal Epithelial Homeostasis in Limbal Stem Cell Deficiency: Current Trends and Future Directions. Cells 2022, 11, 3247. [Google Scholar] [CrossRef]
- Gupta, N.; Joshi, J.; Farooqui, J.; Mathur, U. Results of simple limbal epithelial transplantation in unilateral ocular surface burn. Indian J. Ophthalmol. 2018, 66, 45. [Google Scholar] [CrossRef]
- Thokala, P.; Singh, A.; Singh, V.K.; Rathi, V.M.; Basu, S.; Singh, V.; MacNeil, S.; Sangwan, V.S. Economic, clinical and social impact of simple limbal epithelial transplantation for limbal stem cell deficiency. Br. J. Ophthalmol. 2022, 106, 923–928. [Google Scholar] [CrossRef]
- Jurkunas, U.; Johns, L.; Armant, M. Cultivated Autologous Limbal Epithelial Cell Transplantation: New Frontier in the Treatment of Limbal Stem Cell Deficiency. Am. J. Ophthalmol. 2022, 239, 244–268. [Google Scholar] [CrossRef]
- Nagai, N.; Otake, H. Novel drug delivery systems for the management of dry eye. Adv. Drug Deliv. Rev. 2022, 191, 114582. [Google Scholar] [CrossRef]
- Mayer, K.L.; Nordlund, M.L.; Schwartz, G.S.; Holland, E.J. Keratopathy in Congenital Aniridia. Ocul. Surf. 2003, 1, 74–79. [Google Scholar] [CrossRef]
- Lee, H.; Khan, R.; O’Keefe, M. Aniridia: Current pathology and management. Acta Ophthalmol. 2008, 86, 708–715. [Google Scholar] [CrossRef]
- Kivlin, J.D.; Apple, D.J.; Olson, R.J.; Manthey, R. Dominantly inherited keratitis. Arch Ophthalmol. 1986, 104, 1621–1623. [Google Scholar] [CrossRef]
- Pearce, W.G.; Mielke, B.W.; Hassard, D.T.; Climenhaga, H.W.; Climenhaga, D.B.; Hodges, E.J. Autosomal dominant keratitis: A possible aniridia variant. Can. J. Ophthalmol. 1995, 30, 131–137. [Google Scholar]
- Di Iorio, E.; Kaye, S.B.; Ponzin, D.; Barbaro, V.; Ferrari, S.; Böhm, E.; Nardiello, P.; Castaldo, G.; McGrath, J.A.; Willoughby, C.E. Limbal stem cell deficiency and ocular phenotype in ectrodactyly-ectodermal dysplasia-clefting syndrome caused by p63 mutations. Ophthalmology 2012, 119, 74–83. [Google Scholar] [CrossRef]
- Trevisan, M.; Alvisi, G.; Barbaro, V.; Barzon, L.; Raffa, P.; Migliorati, A.; Desole, G.; Ruzittu, S.; Masi, G.; Di Iorio, E.; et al. Oral Mucosa-Derived Induced Pluripotent Stem Cells from Patients with Ectrodactyly-Ectodermal Dysplasia-Clefting Syndrome. Cell Reprogram 2018, 20, 215–224. [Google Scholar] [CrossRef]
- Yildirim, M.; Yorgancilar, E.; Gun, R.; Topcu, I. Ectodermal dysplasia: Otolaryngologic evaluation of 23 cases. Ear Nose Throat J. 2012, 91, E28–E33. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, M.E.; Tlougan, B.E.; Price, H.N.; Patel, R.; Kamino, H.; Schaffer, J.V. Keratitis-ichthyosis-deafness (KID) syndrome. Dermatol. Online J. 2009, 15, 11. [Google Scholar] [CrossRef]
- Gicquel, J.J.; Lami, M.C.; Catier, A.; Balayre, S.; Dighiero, P. Limbal stem cell deficiency associated with KID syndrome, about a case. J. Fr. Ophtalmol. 2002, 25, 1061–1064. [Google Scholar]
- Brooks, B.P.; Thompson, A.H.; Clayton, J.A.; Chan, C.-C.; Tamura, D.; Zein, W.M.; Blain, D.; Hadsall, C.; Rowan, J.; Bowles, K.E.; et al. Ocular manifestations of trichothiodystrophy. Ophthalmology 2011, 118, 2335–2342. [Google Scholar] [CrossRef] [Green Version]
- Kraemer, K.H.; Patronas, N.J.; Schiffmann, R.; Brooks, B.P.; Tamura, D.; Di Giovanna, J. Xeroderma pigmentosum, trichothiodystrophy and Cockayne syndrome: A complex genotype-phenotype relationship. Neuroscience 2007, 145, 1388–1396. [Google Scholar] [CrossRef] [Green Version]
- Ramkumar, H.L.; Brooks, B.P.; Cao, X.; Tamura, D.; DiGiovanna, J.J.; Kraemer, K.H.; Chan, C.-C. Ophthalmic manifestations and histopathology of xeroderma pigmentosum: Two clinicopathological cases and a review of the literature. Surv. Ophthalmol. 2011, 56, 348–361. [Google Scholar] [CrossRef] [Green Version]
- AlSabbagh, M.M. Dyskeratosis congenita: A literature review. J. Dtsch. Dermatol. Ges. 2020, 18, 943–967. [Google Scholar] [CrossRef]
- Hiyama, E.; Hiyama, K. Telomere and telomerase in stem cells. Br. J. Cancer 2007, 96, 1020–1024. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Zhang, M.C.; Hu, Y.H. Experimental research of the expression of telomerase in corneal limbal epithelial cells. Zhonghua Yan Ke Za Zhi 2005, 41, 399–402. [Google Scholar]
- Garofola, C. Dyskeratosis Congenita; StatPearls: Tampa, FL, USA, 2021. [Google Scholar]
- Zhang, R.; Pandzic, E.; Park, M.; Wakefield, D.; Di Girolamo, N. Inducing dry eye disease using a custom engineered desiccation system: Impact on the ocular surface including keratin-14-positive limbal epithelial stem cells. Ocul. Surf. 2021, 21, 145–159. [Google Scholar] [CrossRef]
- Santos, M.S.; Gomes, J.A.; Hofling-Lima, A.L.; Rizzo, L.V.; Romano, A.C.; Belfort, R., Jr. Survival analysis of conjunctival limbal grafts and amniotic membrane transplantation in eyes with total limbal stem cell deficiency. Am. J. Ophthalmol. 2005, 140, 223–230. [Google Scholar] [CrossRef]
- O’neil, E.C.; Henderson, M.; Massaro-Giordano, M.; Bunya, V.Y. Advances in dry eye disease treatment. Curr. Opin. Ophthalmol. 2019, 30, 166–178. [Google Scholar] [CrossRef]
- Chan, T.C.Y.; Chow, S.S.W.; Wan, K.H.N.; Yuen, H.K.L. Update on the association between dry eye disease and meibomian gland dysfunction. Hong Kong Med. J. 2019, 25, 38–47. [Google Scholar] [CrossRef] [Green Version]
- Albietz, J.M.; Schmid, K.L. Intense pulsed light treatment and meibomian gland expression for moderate to advanced meibomian gland dysfunction. Clin. Exp. Optom. 2018, 101, 23–33. [Google Scholar] [CrossRef] [Green Version]
- Sabeti, S.; Kheirkhah, A.; Yin, J.; Dana, R. Management of meibomian gland dysfunction: A review. Surv. Ophthalmol. 2020, 65, 205–217. [Google Scholar] [CrossRef]
- Termote, K.; Schendel, S.; Moloney, G.; Holland, S.P.; Lange, A.P. Focal limbal stem cell deficiency associated with soft contact lens wear. Can. J. Ophthalmol. 2017, 52, 552–558. [Google Scholar] [CrossRef]
- Rossen, J.; Amram, A.; Milani, B.; Park, D.; Harthan, J.; Joslin, C.; McMahon, T.; Djalilian, A. Contact Lens-induced Limbal Stem Cell Deficiency. Ocul. Surf. 2016, 14, 419–434. [Google Scholar] [CrossRef] [Green Version]
- Martin, R. Corneal conjunctivalisation in long-standing contact lens wearers. Clin. Exp. Optom. 2007, 90, 26–30. [Google Scholar] [CrossRef]
- Deng, S.X.; Kruse, F.; Gomes, J.A.P.; Chan, C.C.; Daya, S.; Dana, R.; Figueiredo, F.C.; Kinoshita, S.; Rama, P.; Sangwan, V.; et al. Global Consensus on the Management of Limbal Stem Cell Deficiency. Cornea 2020, 39, 1291–1302. [Google Scholar] [CrossRef]
- Andrasko, G.J. Corneal deswelling response to hard and hydrogel extended wear lenses. Investig. Ophthalmol. Vis. Sci. 1986, 27, 20–23. [Google Scholar]
- Kethiri, A.R.; Singh, V.K.; Damala, M.; Basu, S.; Rao, C.M.; Bokara, K.K.; Singh, V. Long term observation of ocular surface alkali burn in rabbit models: Quantitative analysis of corneal haze, vascularity and self-recovery. Exp. Eye Res. 2021, 205, 108526. [Google Scholar] [CrossRef]
- Kadar, T.; Horwitz, V.; Cohen, M.; Egoz, I.; Gutman, H.; Gez, R.; Dachir, S. Limbal stem cell deficiency (LSCD) in rats and mice following whole body exposure to sulfur mustard (SM) vapor. Exp. Eye Res. 2022, 223, 109195. [Google Scholar] [CrossRef]
- Fatima, A.; Iftekhar, G.; Sangwan, V.S.; Vemuganti, G.K. Ocular surface changes in limbal stem cell deficiency caused by chemical injury: A histologic study of excised pannus from recipients of cultured corneal epithelium. Eye 2008, 22, 1161–1167. [Google Scholar] [CrossRef]
- Dua, H.S.; King, A.J.; Joseph, A. A new classification of ocular surface burns. Br. J. Ophthalmol. 2001, 85, 1379–1383. [Google Scholar] [CrossRef] [Green Version]
- Kadar, T.; Amir, A.; Cohen, L.; Cohen, M.; Sahar, R.; Gutman, H.; Horwitz, V.; Dachir, S. Anti-VEGF Therapy (Bevacizumab) for Sulfur Mustard-Induced Corneal Neovascularization Associated with Delayed Limbal Stem Cell Deficiency in Rabbits. Curr. Eye Res. 2014, 39, 439–450. [Google Scholar] [CrossRef]
- Fujishima, H.; Shimazaki, J.; Tsubota, K. Temporary corneal stem cell dysfunction after radiation therapy. Br. J. Ophthalmol. 1996, 80, 911–914. [Google Scholar] [CrossRef] [Green Version]
- Weng, S.F.; Jan, R.L.; Wang, J.J.; Tseng, S.H.; Chang, Y.S. Association between atopic keratoconjunctivitis and the risk of keratoconus. Acta Ophthalmol. 2021, 99, e54–e61. [Google Scholar] [CrossRef]
- Zicari, A.M.; Capata, G.; Nebbioso, M.; De Castro, G.; Midulla, F.; Leonardi, L.; Loffredo, L.; Spalice, A.; Perri, L.; Duse, M. Vernal Keratoconjunctivitis: An update focused on clinical grading system. Ital. J. Pediatr. 2019, 45, 64. [Google Scholar] [CrossRef] [Green Version]
- Kaur, K.; Gurnani, B. Vernal Keratoconjunctivitis; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: http://www.ncbi.nlm.nih.gov/books/NBK576433/ (accessed on 10 April 2023).
- Guglielmetti, S.; Dart, J.K.; Calder, V. Atopic keratoconjunctivitis and atopic dermatitis. Curr. Opin. Allergy Clin. Immunol. 2010, 10, 478–485. [Google Scholar] [CrossRef]
- Singh, A.; Murthy, S.I.; Gandhi, A.; Sangwan, V.S. ‘Doughnut’ Amniotic Membrane Transplantation With Penetrating Keratoplasty for Vernal Keratoconjunctivitis With Limbal Stem Cell Disease. Cornea 2021, 40, 914–916. [Google Scholar] [CrossRef]
- Kinoshita, S.; Koizumi, N.; Ueno, M.; Okumura, N.; Imai, K.; Tanaka, H.; Yamamoto, Y.; Nakamura, T.; Inatomi, T.; Bush, J.; et al. Injection of Cultured Cells with a ROCK Inhibitor for Bullous Keratopathy. N. Engl. J. Med. 2018, 378, 995–1003. [Google Scholar] [CrossRef]
- Ong Tone, S.; Kocaba, V.; Bohm, M.; Wylegala, A.; White, T.L.; Jurkunas, U.V. Fuchs endothelial corneal dystrophy: The vicious cycle of Fuchs pathogenesis. Prog. Retin. Eye Res. 2021, 80, 100863. [Google Scholar] [CrossRef]
- Uchino, Y.; Goto, E.; Takano, Y.; Dogru, M.; Shinozaki, N.; Shimmura, S.; Yagi, Y.; Tsubota, K.; Shimazaki, J. Long-standing bullous keratopathy is associated with peripheral conjunctivalization and limbal deficiency. Ophthalmology 2006, 113, 1098–1101. [Google Scholar] [CrossRef]
- Paris Fdos, S.; Goncalves, E.D.; Barros Jde, N.; Campos, M.S.; Sato, E.H.; Gomes, J.A. Impression cytology findings in bullous keratopathy. Br. J. Ophthalmol. 2010, 94, 773–776. [Google Scholar] [CrossRef]
- Sauder, G.; Jonas, J.B. Limbal stem cell deficiency after subconjunctival mitomycin C injection for trabeculectomy. Am. J. Ophthalmol. 2006, 141, 1129–1130. [Google Scholar] [CrossRef]
- Pires, R.T.; Chokshi, A.; Tseng, S.C. Amniotic membrane transplantation or conjunctival limbal autograft for limbal stem cell deficiency induced by 5-fluorouracil in glaucoma surgeries. Cornea 2000, 19, 284–287. [Google Scholar] [CrossRef]
- Kim, K.H.; Kim, W.S. Corneal limbal stem cell deficiency associated with the anticancer drug S-1. Optom. Vis. Sci. 2015, 92 (Suppl. S1), S10–S13. [Google Scholar] [CrossRef] [Green Version]
- Ding, X.; Bishop, R.J.; Herzlich, A.A.; Patel, M.; Chan, C.C. Limbal stem cell deficiency arising from systemic chemotherapy with hydroxycarbamide. Cornea 2009, 28, 221–223. [Google Scholar] [CrossRef] [Green Version]
- Lobo, A.M.; Agelidis, A.M.; Shukla, D. Pathogenesis of herpes simplex keratitis: The host cell response and ocular surface sequelae to infection and inflammation. Ocul. Surf. 2019, 17, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Minor, M.; Payne, E. Herpes Zoster Ophthalmicus; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: http://www.ncbi.nlm.nih.gov/books/NBK557779/ (accessed on 10 April 2023).
- Liu, X.; Xu, S.; Wang, Y.; Jin, X.; Shi, Y.; Zhang, H. Bilateral Limbal Stem Cell Alterations in Patients With Unilateral Herpes Simplex Keratitis and Herpes Zoster Ophthalmicus as Shown by In Vivo Confocal Microscopy. Investig. Ophthalmol. Vis. Sci. 2021, 62, 12. [Google Scholar] [CrossRef] [PubMed]
- Lakhundi, S.; Siddiqui, R.; Khan, N.A. Pathogenesis of microbial keratitis. Microb. Pathog. 2017, 104, 97–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lansingh, V.C. Trachoma. BMJ Clin. Evid. 2016, 2016, 706. Available online: https://www.ncbi.nlm.nih.gov/pubmed/26860629 (accessed on 10 April 2023).
- Shanbhag, S.S.; Sangwan, V.S.; Singh, A.; Donthineni, P.R.; Basu, S.; Srinivasan, B.; Agarwal, S.; Iyer, G. Clinical Aspects of Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis with Severe Ocular Complications in India. Front. Med. 2021, 8, 643955. [Google Scholar] [CrossRef]
- Lerch, M.; Mainetti, C.; Beretta-Piccoli, T.B.; Harr, T. Current Perspectives on Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis. Clin. Rev. Allergy Immunol. 2018, 54, 147–176. [Google Scholar] [CrossRef]
- Iyer, G.; Srinivasan, B.; Agarwal, S. Ocular Sequelae of Stevens-Johnson Syndrome: A Comprehensive Approach. Cornea 2020, 39 (Suppl. S1), S3–S6. [Google Scholar] [CrossRef]
- Sotozono, C.; Ueta, M.; Nakatani, E.; Kitami, A.; Watanabe, H.; Sueki, H.; Iijima, M.; Aihara, M.; Ikezawa, Z.; Aihara, Y.; et al. Predictive Factors Associated With Acute Ocular Involvement in Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis. Am. J. Ophthalmol. 2015, 160, 228–237.e2. [Google Scholar] [CrossRef]
- Ruan, Y.; Jiang, S.; Musayeva, A.; Pfeiffer, N.; Gericke, A. Corneal Epithelial Stem Cells–Physiology, Pathophysiology and Therapeutic Options. Cells 2021, 10, 2302. [Google Scholar] [CrossRef]
- Taurone, S.; Spoletini, M.; Ralli, M.; Gobbi, P.; Artico, M.; Imre, L.; Czakò, C.; Kovàcs, I.; Greco, A.; Micera, A. Ocular mucous membrane pemphigoid: A review. Immunol. Res. 2019, 67, 280–289. [Google Scholar] [CrossRef]
- Georgoudis, P.; Sabatino, F.; Szentmary, N.; Palioura, S.; Fodor, E.; Hamada, S.; Scholl, H.P.N.; Gatzioufas, Z. Ocular Mucous Membrane Pemphigoid: Current State of Pathophysiology, Diagnostics and Treatment. Ophthalmol. Ther. 2019, 8, 5–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, E.; Meyer-Ter-Vehn, T.; Zillikens, D.; Geerling, G. Mucous membrane pemphigoid with ocular involvement. Part I: Clinical manifestations, pathogenesis and diagnosis. Ophthalmologe 2008, 105, 285–297. [Google Scholar] [CrossRef] [PubMed]
- Chui, J.; Coroneo, M.T.; Tat, L.T.; Crouch, R.; Wakefield, D.; Di Girolamo, N. Ophthalmic pterygium: A stem cell disorder with premalignant features. Am. J. Pathol. 2011, 178, 817–827. [Google Scholar] [CrossRef]
- Das, P.; Gokani, A.; Bagchi, K.; Bhaduri, G.; Chaudhuri, S.; Law, S. Limbal epithelial stem-microenvironmental alteration leads to pterygium development. Mol. Cell Biochem. 2015, 402, 123–139. [Google Scholar] [CrossRef]
- Mahdy, M.A.S.; Bhatia, J. Treatment of primary pterygium: Role of limbal stem cells and conjunctival autograft transplantation. Eur. J. Ophthalmol. 2009, 19, 729–732. [Google Scholar] [CrossRef] [PubMed]
- Rodriquez-Braz, D. Cutaneous and ocular rosacea: Common and specific physiopathogenic mechanisms and study models. Mol. Vis. 2021, 27, 323–353. [Google Scholar]
- Dua, H.S.; Azuara-Blanco, A. Allo-limbal transplantation in patients with limbal stem cell deficiency. Br. J. Ophthalmol. 1999, 83, 414–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milosevic, S.; Bachnick, B.; Karim, K.; Bornkamm, G.W.; Witter, K.; Gerbitz, A.; Mautner, J.; Behrends, U. Identification of MHC II-Restricted Minor Histocompatibility Antigens After HLA-Identical Stem-Cell Transplantation. Transplantation 2010, 90, 1030–1035. [Google Scholar] [CrossRef] [PubMed]
- Giannaccare, G.; Pellegrini, M.; Bernabei, F.; Scorcia, V.; Campos, E. Ocular surface system alterations in ocular graft-versus-host disease: All the pieces of the complex puzzle. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 1341–1351. [Google Scholar] [CrossRef]
- Busin, M.; Giannaccare, G.; Sapigni, L.; Testoni, N.; Leon, P.; Versura, P.; Campos, E. Conjunctival and Limbal Transplantation from the Same Living-Related Bone Marrow Donor to Patients with Severe Ocular Graft-vs-Host Disease. JAMA Ophthalmol. 2017, 135, 1123. [Google Scholar] [CrossRef]
- Hamam, R.; Bhat, P.; Foster, C.S. Conjunctival/corneal intraepithelial neoplasia. Int. Ophthalmol. Clin. 2009, 49, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.A.; Hirst, L.W. Ocular surface squamous neoplasia. Surv. Ophthalmol. 1995, 39, 429–450. [Google Scholar] [CrossRef] [PubMed]
- Lyall, D.A.M.; Srinivasan, S.; Roberts, F. Limbal stem cell failure secondary to advanced conjunctival squamous cell carcinoma: A clinicopathological case report. BMJ Case Rep. 2009, 2009, bcr0920092272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dua, H.; Azuara-Blanco, A. Autologous limbal transplantation in patients with unilateral corneal stem cell deficiency. Br. J. Ophthalmol. 2000, 84, 273–278. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, N.; Ohmura, T.; Suzuki, H.; Shirasawa, H. Successful treatment with 5-fluorouracil of conjunctival intraepithelial neoplasia refractive to mitomycin-C1. Ophthalmology 2002, 109, 249–252. [Google Scholar] [CrossRef]
- Meallet, M.A.; Espana, E.M.; Grueterich, M.; Ti, S.E.; Goto, E.; Tseng, S.C.G. Amniotic membrane transplantation with conjunctival limbal autograft for total limbal stem cell deficiency. Ophthalmology 2003, 110, 1585–1592. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moshirfar, M.; Masud, M.; Harvey, D.H.; Payne, C.; Bruce, E.; Ronquillo, Y.C.; Hoopes, P.C. The Multifold Etiologies of Limbal Stem Cell Deficiency: A Comprehensive Review on the Etiologies and Additional Treatment Options for Limbal Stem Cell Deficiency. J. Clin. Med. 2023, 12, 4418. https://doi.org/10.3390/jcm12134418
Moshirfar M, Masud M, Harvey DH, Payne C, Bruce E, Ronquillo YC, Hoopes PC. The Multifold Etiologies of Limbal Stem Cell Deficiency: A Comprehensive Review on the Etiologies and Additional Treatment Options for Limbal Stem Cell Deficiency. Journal of Clinical Medicine. 2023; 12(13):4418. https://doi.org/10.3390/jcm12134418
Chicago/Turabian StyleMoshirfar, Majid, Maliha Masud, Devon Hori Harvey, Carter Payne, Elayna Bruce, Yasmyne C. Ronquillo, and Philip C. Hoopes. 2023. "The Multifold Etiologies of Limbal Stem Cell Deficiency: A Comprehensive Review on the Etiologies and Additional Treatment Options for Limbal Stem Cell Deficiency" Journal of Clinical Medicine 12, no. 13: 4418. https://doi.org/10.3390/jcm12134418