
Prone Positioning in Mechanically Ventilated COVID-19 Patients: Timing of Initiation and Outcomes
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Demographics
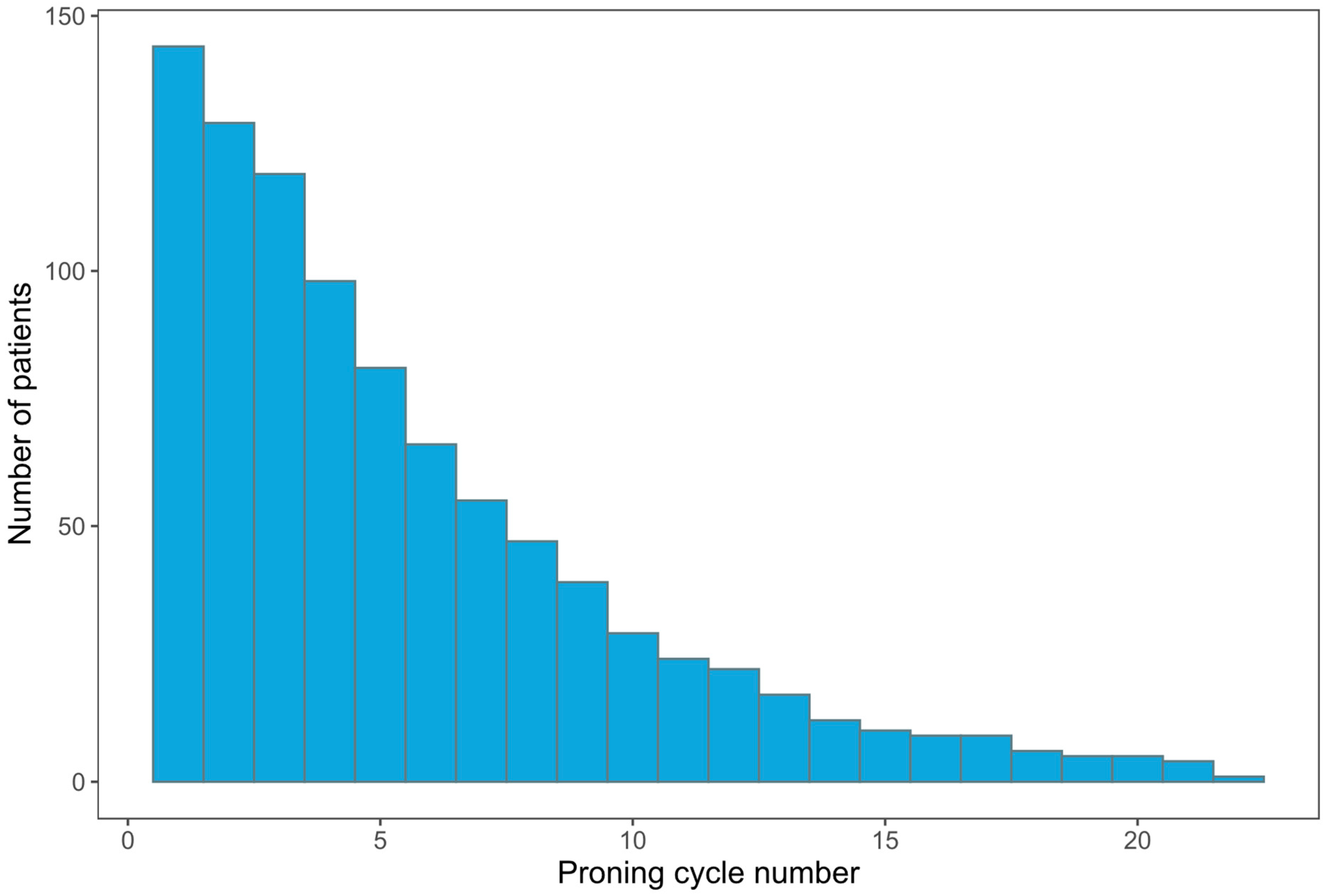
3.2. Prone Cycle Characteristics
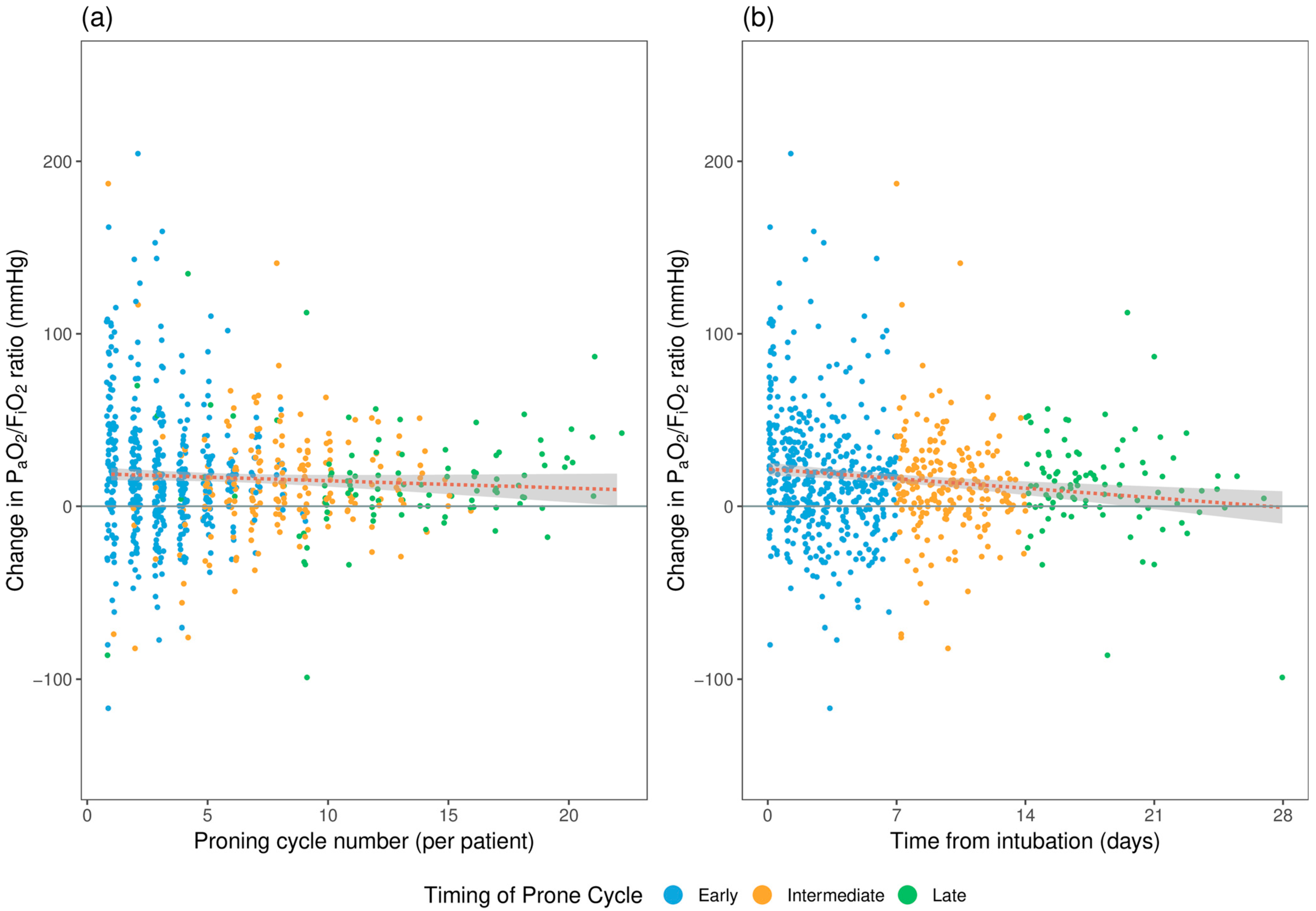
3.3. Outcome: Change in Oxygenation (∆PaO2/FiO2)
3.4. Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation [Internet]. WHO Coronavirus (COVID-19) Dashboard, 2021. Available online: https://covid19.who.int/ (accessed on 17 April 2023).
- Armstrong, R.A.; Kane, A.D.; Cook, T.M. Decreasing mortality rates in ICU during the COVID-19 pandemic. Anaesthesia 2021, 76 (Suppl. S3), 10. [Google Scholar] [CrossRef]
- Roberts, C.M.; Levi, M.; McKee, M.; Schilling, R.; Lim, W.S.; Grocott, M.P.W. COVID-19: A complex multisystem disorder. Br. J. Anaesth. 2020, 125, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, R.A.; Kane, A.D.; Cook, T.M. Outcomes from intensive care in patients with COVID-19: A systematic review and meta-analysis of observational studies. Anaesthesia 2020, 75, 1340–1349. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk factors and disease profile of post-vaccination SARS-CoV-2 infection in UK users of the COVID Symptom Study app: A prospective, community-based, nested, case-control study. Lancet Infect Dis. 2022, 22, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Pairo-Castineira, E.; Clohisey, S.; Klaric, L.; Bretherick, A.D.; Rawlik, K.; Pasko, D.; Walker, S.; Parkinson, N.; Fourman, M.H.; Russell, C.D.; et al. Genetic mechanisms of critical illness in COVID-19. Nature 2021, 591, 92–98. [Google Scholar] [CrossRef]
- Group, R.C.; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Severe Covid, G.G.; Ellinghaus, D.; Degenhardt, F.; Bujanda, L.; Buti, M.; Albillos, A.; Invernizzi, P.; Fernandez, J.; Prati, D.; Baselli, G.; et al. Genomewide Association Study of Severe COVID-19 with Respiratory Failure. N. Engl. J. Med. 2020, 383, 1522–1534. [Google Scholar] [CrossRef]
- Twohig, K.A.; Nyberg, T.; Zaidi, A.; Thelwall, S.; Sinnathamby, M.A.; Aliabadi, S.; Seaman, S.R.; Harris, R.J.; Hope, R.; Lopez-Bernal, J.; et al. Hospital admission and emergency care attendance risk for SARS-CoV-2 delta (B.1.617.2) compared with alpha (B.1.1.7) variants of concern: A cohort study. Lancet Infect Dis. 2022, 22, 35–42. [Google Scholar] [CrossRef]
- Piehl, M.A.; Brown, R.S. Use of extreme position changes in acute respiratory failure. Crit. Care Med. 1976, 4, 13–14. [Google Scholar] [CrossRef]
- Bloomfield, R.; Noble, D.W.; Sudlow, A. Prone position for acute respiratory failure in adults. Cochrane Database Syst. Rev. 2015, 2015, CD008095. [Google Scholar] [CrossRef]
- Guerin, C.; Reignier, J.; Richard, J.C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef]
- Gattinoni, L.; Busana, M.; Giosa, L.; Macri, M.M.; Quintel, M. Prone Positioning in Acute Respiratory Distress Syndrome. Semin Respir. Crit. Care Med. 2019, 40, 94–100. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Luo, J.; Pavlov, I.; Perez, Y.; Tan, W.; Roca, O.; Tavernier, E.; Kharat, A.; McNicholas, B.; Ibarra-Estrada, M.; et al. Awake prone positioning for non-intubated patients with COVID-19-related acute hypoxaemic respiratory failure: A systematic review and meta-analysis. Lancet Respir. Med. 2022, 10, 573–583. [Google Scholar] [CrossRef]
- Ashra, F.; Chen, R.; Kang, X.L.; Chiang, K.J.; Pien, L.C.; Jen, H.J.; Liu, D.; Hsiao, S.S.; Chou, K.R. Effectiveness of prone position in acute respiratory distress syndrome and moderating factors of obesity class and treatment durations for COVID-19 patients: A meta-analysis. Intensive Crit. Care Nurs. 2022, 72, 103257. [Google Scholar] [CrossRef]
- Chua, E.X.; Wong, Z.Z.; Hasan, M.S.; Atan, R.; Yunos, N.M.; Yip, H.W.; Teoh, W.Y.; Ramli, M.A.S.; Ng, K.T. Prone ventilation in intubated COVID-19 patients: A systematic review and meta-analysis. Braz. J. Anesthesiol. 2022, 72, 780–789. [Google Scholar] [CrossRef]
- Available online: https://ics.ac.uk/resource/prone-position-in-adult-critical-care.html (accessed on 17 April 2023).
- Burke, H.; Freeman, A.; Dushianthan, A.; Celinski, M.; Batchelor, J.; Phan, H.; Borca, F.; Kipps, C.; Thomas, G.J.; Faust, S.N.; et al. Research Evaluation Alongside Clinical Treatment in COVID-19 (REACT COVID-19): An observational and biobanking study. BMJ Open 2021, 11, e043012. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonca, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- The Acute Respiratory Distress Syndrome Network; Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar]
- Swindin, J.; Sampson, C.; Howatson, A. Airway pressure release ventilation. BJA Educ. 2020, 20, 80–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whebell, S.; Zhang, J.; Lewis, R.; Berry, M.; Ledot, S.; Retter, A.; Camporota, L. Survival benefit of extracorporeal membrane oxygenation in severe COVID-19: A multi-centre-matched cohort study. Intensive Care Med. 2022, 48, 467–478. [Google Scholar] [CrossRef] [PubMed]
- Kallet, R.H. A Comprehensive Review of Prone Position in ARDS. Respir. Care 2015, 60, 1660–1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, Z.; Yang, Z.; Liang, Z.; Cen, Q.; Zhang, Z.; Liang, H.; Liu, R.; Zeng, L.; Xie, Y.; Wang, Y. Prone versus Supine Position Ventilation in Adult Patients with Acute Respiratory Distress Syndrome: A Meta-Analysis of Randomized Controlled Trials. Emerg. Med. Int. 2020, 2020, 4973878. [Google Scholar] [CrossRef] [PubMed]
- Shelhamer, M.C.; Wesson, P.D.; Solari, I.L.; Jensen, D.L.; Steele, W.A.; Dimitrov, V.G.; Kelly, J.D.; Aziz, S.; Gutierrez, V.P.; Vittinghoff, E.; et al. Prone Positioning in Moderate to Severe Acute Respiratory Distress Syndrome Due to COVID-19: A Cohort Study and Analysis of Physiology. J. Intensive Care Med. 2021, 36, 241–252. [Google Scholar] [CrossRef]
- Camporota, L.; Sanderson, B.; Chiumello, D.; Terzi, N.; Argaud, L.; Rimmele, T.; Metuor, R.; Verstraete, A.; Cour, M.; Bohe, J.; et al. Prone Position in COVID-19 and -COVID-19 Acute Respiratory Distress Syndrome: An International Multicenter Observational Comparative Study. Crit. Care Med. 2022, 50, 633–643. [Google Scholar] [CrossRef]
- Accoce, M.; Calvo Delfino, M.; Cardoso, G.; Castro, L.; Perez, J.; Dorado, J.H. Successive prone positioning sessions in mechanically ventilated patients with moderate and severe acute respiratory distress syndrome secondary to COVID-19: Case series. Med. Intensiv. 2022, 46, 652–654. [Google Scholar] [CrossRef]
- Griffiths, M.J.D.; McAuley, D.F.; Perkins, G.D.; Barrett, N.; Blackwood, B.; Boyle, A.; Chee, N.; Connolly, B.; Dark, P.; Finney, S.; et al. Guidelines on the management of acute respiratory distress syndrome. BMJ Open Respir. Res. 2019, 6, e000420. [Google Scholar] [CrossRef] [Green Version]
- Hochberg, C.H.; Psoter, K.J.; Sahetya, S.K.; Nolley, E.P.; Hossen, S.; Checkley, W.; Kerlin, M.P.; Eakin, M.N.; Hager, D.N. Comparing Prone Positioning Use in COVID-19 Versus Historic Acute Respiratory Distress Syndrome. Crit. Care Explor. 2022, 4, e0695. [Google Scholar] [CrossRef]
- Bell, J.; William Pike, C.; Kreisel, C.; Sonti, R.; Cobb, N. Predicting Impact of Prone Position on Oxygenation in Mechanically Ventilated Patients with COVID-19. J. Intensive Care Med. 2022, 37, 883–889. [Google Scholar] [CrossRef]
- Hafez, A.F.; Gamal, R.; El-Rahman, A.A.; Kamal, F. Is prolonged period of prone position effective and safe in mechanically ventilated patients with SARS-CoV-2? A randomized clinical trial. Egypt. J. Anaesth. 2022, 38, 276–283. [Google Scholar] [CrossRef]
- Okin, D.; Huang, C.Y.; Alba, G.A.; Jesudasen, S.J.; Dandawate, N.A.; Gavralidis, A.; Chang, L.L.; Moin, E.E.; Ahmad, I.; Witkin, A.S.; et al. Prolonged Prone Position Ventilation Is Associated With Reduced Mortality in Intubated COVID-19 Patients. Chest 2023, 163, 533–542. [Google Scholar] [CrossRef]
- Page, D.B.; Vijaykumar, K.; Russell, D.W.; Gandotra, S.; Chiles, J.W.; Whitson, M.R.; Dransfield, M.T. Prolonged Prone Positioning for COVID-19-induced Acute Respiratory Distress Syndrome: A Randomized Pilot Clinical Trial. Ann. Am. Thorac. Soc. 2022, 19, 685–687. [Google Scholar] [CrossRef]
- Walter, T.; Zucman, N.; Mullaert, J.; Thiry, I.; Gernez, C.; Roux, D.; Ricard, J.D. Extended prone positioning duration for COVID-19-related ARDS: Benefits and detriments. Crit. Care 2022, 26, 208. [Google Scholar] [CrossRef]
- Langer, T.; Brioni, M.; Guzzardella, A.; Carlesso, E.; Cabrini, L.; Castelli, G.; Dalla Corte, F.; De Robertis, E.; Favarato, M.; Forastieri, A.; et al. Prone position in intubated, mechanically ventilated patients with COVID-19: A multi-centric study of more than 1000 patients. Crit. Care 2021, 25, 128. [Google Scholar]
- Ferrando, C.; Suarez-Sipmann, F.; Mellado-Artigas, R.; Hernandez, M.; Gea, A.; Arruti, E.; Aldecoa, C.; Martinez-Palli, G.; Martinez-Gonzalez, M.A.; Slutsky, A.S.; et al. Clinical features, ventilatory management, and outcome of ARDS caused by COVID-19 are similar to other causes of ARDS. Intensive Care Med. 2020, 46, 2200–2211. [Google Scholar]
- Zarantonello, F.; Sella, N.; Pettenuzzo, T.; Andreatta, G.; Calore, A.; Dotto, D.; De Cassai, A.; Calabrese, F.; Boscolo, A.; Navalesi, P. Early Physiologic Effects of Prone Positioning in COVID-19 Acute Respiratory Distress Syndrome. Anesthesiology 2022, 137, 327–339. [Google Scholar]



{kind=link}
{kind=link}
| Demographics | Invasive Mechanical Ventilation and Prone Position (n = 144) |
|---|---|
| Age, year | 59 (51, 66) |
| Male sex, n (%) | 95 (66%) |
| Duration of symptoms on admission to the ICU (days) | 7.0 (6.0) |
| Admission APACHE II score | 15 (11, 23) |
| Admission SOFA score | 4 (3.0, 6.3) |
| Admission Charlson comorbidity index | 2 (1, 3) |
| Admission PaO2/FiO2 (mmHg) | 114.8 (87.0, 141.0) |
| Time to intubation from ICU admission (hours) | 18.3 (1.6, 75.2) |
| BMI (kg/m2) | 31 (26, 36) |
| Specific co-morbidities, n (%) | |
| BMI ≥ 30 (kg/m2) | 79 (55%) |
| Diabetes Mellitus | 45 (31%) |
| Chronic respiratory illness | 29 (20%) |
| Ischemic heart disease | 12 (8.3%) |
| Congestive cardiac failure | 4 (2.8%) |
| Immunosuppression | 14 (9.7%) |
| ICU admission blood | |
| Bilirubin (μmol/L) | 10.0 (7.0, 14.0) |
| Creatinine (μmol/L) | 73 (56, 97) |
| eGFR | 88.5 (22.8) |
| Urea (mmol/L) | 7.0 (5.5, 10.3) |
| CRP (mg/L) | 138 (74, 209) |
| WBC (n × 109/L) | 8.7 (6.2, 11.4) |
| Lymphocytes (n × 109/L) | 0.70 (0.50, 0.90) |
| INR | 1.10 (1.00, 1.25) |
| Ferritin (ng/mL) | 832 (448, 1343) |
| HS troponin I (ng/L) | 14 (8, 46) |
| Lactate dehydrogenase (U/L) | 1031 (816, 1311) |
| D-Dimer (μg/L) | 574 (299, 1121) |
| Creatine Kinase (U/L) | 141 (66, 444) |
| Proning Cycle Characteristics | All Proning Cycles | Early (<7 days) | Intermediate (7–14 days) | Late (>14 days) | p-Value |
|---|---|---|---|---|---|
| Total number of cycles, n | 931 | 563 | 235 | 133 | N/A |
| Number of patients proned | 144 | 137 | 72 | 39 | N/A |
| Cycles per patient * | 5 (3, 9) | 4 (3, 5) | 3 (2, 4) | 3 (1, 5) | NA |
| Duration of each cycle, hours * | 16.0 (15.0, 17.0) | 16.0 (15.0, 17.0) | 16.0 (14.0, 17.0) | 16.0 (14.0, 17.0) | 0.007 |
| Outcomes | Total Proning Cycles n = 776 | Early (<7 days) n = 469 | Intermediate (7–14 days) n = 203 | Late (>14 days) n = 104 | p-Value |
|---|---|---|---|---|---|
| Pre-prone FiO2 * | 0.69 ± 0.16 | 0.68 ± 0.16 | 0.70 ± 0.15 | 0.71 ± 0.16 | 0.12 |
| ∆PaO2/FiO2 (mmHg) * | 16.6 ± 34.4 | 18.5 ± 36.7 | 13.2 ± 30.4 | 14.8 ± 30.5 | 0.2 |
| ∆PaCO2 (mmHg) * | 2.2 ± 7.4 | 2.0 ± 6.5 | 2.2 ± 8.8 | 2.9 ± 7.9 | 0.5 |
| Frequency of Cycles † | Pre-Prone FiO2 * | ∆PaO2/FiO2 (mmHg) * | ∆PaCO2 (mmHg) * | |
|---|---|---|---|---|
| Cycle 1 | 108 | 0.72 ± 0.16 | 26.8 ± 48.4 | 2.8 ± 6.9 |
| Cycle 2 | 113 | 0.63 ± 0.15 | 19.6 ± 39.6 | 1.2 ± 5.7 |
| Cycle 3 | 100 | 0.61 ± 0.15 | 15.0 ± 39.7 | 3.0 ± 7.4 |
| Cycle 4 | 81 | 0.70 ± 0.19 | 9.0 ± 32.4 | 2.9 ± 7.9 |
| Cycle 5 | 67 | 0.69 ± 0.17 | 14.7 ± 26.7 | 1.6 ± 8.4 |
| Cycle 6 | 52 | 0.74 ± 0.16 | 14.4 ± 25.6 | 2.1 ± 8.8 |
| Cycle 7 | 45 | 0.72 ± 0.15 | 17.1 ± 24.5 | 1.5 ± 5.4 |
| Cycle 8 | 38 | 0.70 ± 0.16 | 22.5 ± 29.6 | 0.6 ± 7.9 |
| Cycle 9 | 35 | 0.71 ± 0.16 | 5.3 ± 33.2 | 4.8 ± 10.6 |
| Cycle 10 | 25 | 0.70 ± 0.14 | 15.0 ± 17.9 | 1.9 ± 8.1 |
| Outcome Characteristics | Patient Mechanically Ventilated and Proned n = 144 |
|---|---|
| Duration of mechanical ventilation (hours) | 397 (242, 746) * |
| 30-day survival | 104 (72%) ** |
| Survival to hospital discharge | 93 (65%) ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jackson, A.; Neyroud, F.; Barnsley, J.; Hunter, E.; Beecham, R.; Radharetnas, M.; Grocott, M.P.W.; Dushianthan, A. Prone Positioning in Mechanically Ventilated COVID-19 Patients: Timing of Initiation and Outcomes. J. Clin. Med. 2023, 12, 4226. https://doi.org/10.3390/jcm12134226
Jackson A, Neyroud F, Barnsley J, Hunter E, Beecham R, Radharetnas M, Grocott MPW, Dushianthan A. Prone Positioning in Mechanically Ventilated COVID-19 Patients: Timing of Initiation and Outcomes. Journal of Clinical Medicine. 2023; 12(13):4226. https://doi.org/10.3390/jcm12134226
Chicago/Turabian StyleJackson, Alexander, Florence Neyroud, Josephine Barnsley, Elsie Hunter, Ryan Beecham, Meiarasu Radharetnas, Michael P. W. Grocott, and Ahilanandan Dushianthan. 2023. "Prone Positioning in Mechanically Ventilated COVID-19 Patients: Timing of Initiation and Outcomes" Journal of Clinical Medicine 12, no. 13: 4226. https://doi.org/10.3390/jcm12134226