
Caregivers’ Expectations on Possible Functional Changes following Disease-Modifying Treatment in Type II and III Spinal Muscular Atrophy: A Comparative Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
- Caregivers
- -
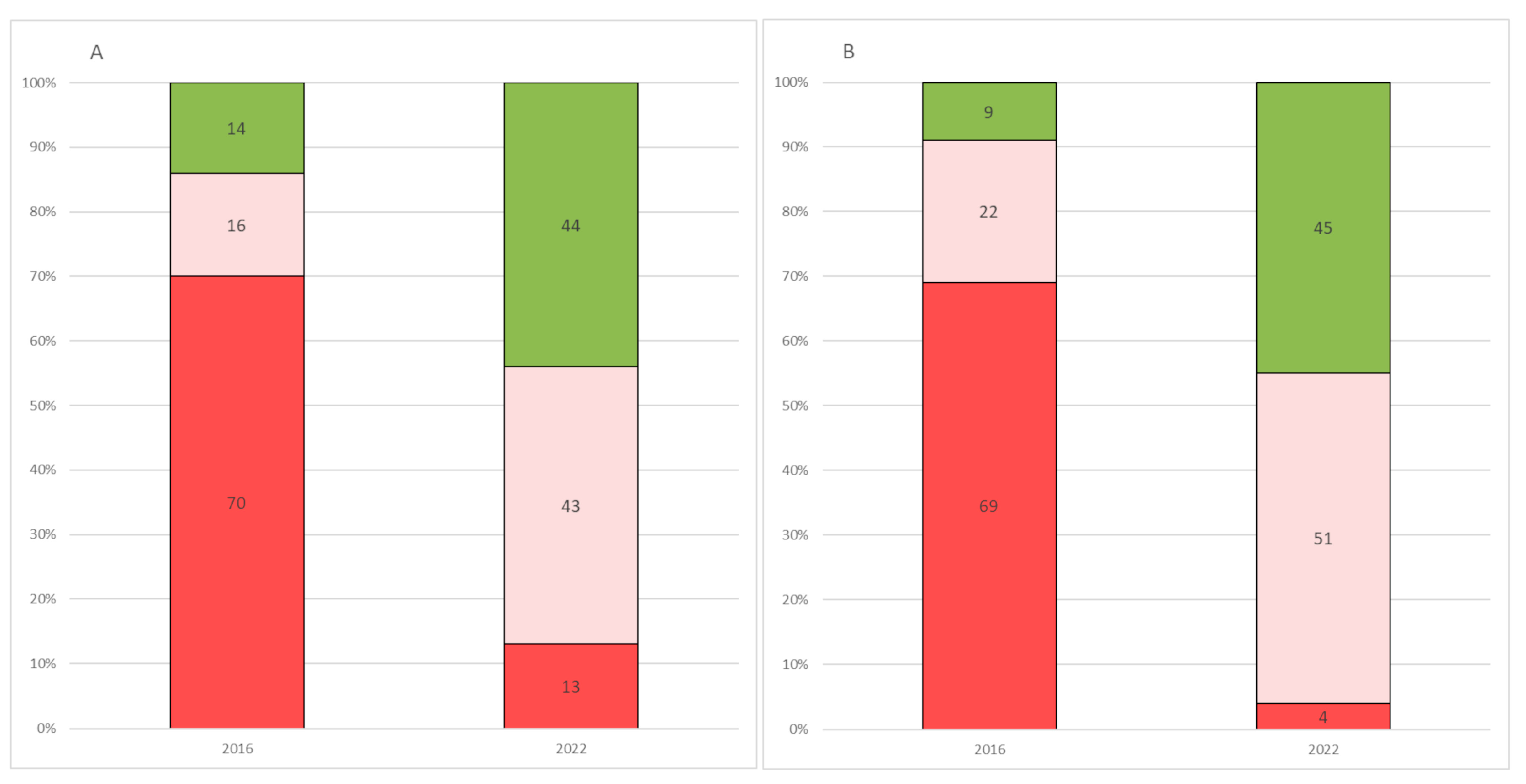
- Speaking of motor skills, please indicate if, in the last year, your child remained stable, deteriorated, or improved: 50% of the caregivers reported stability, 16.67% deterioration, and 33.33% improvement.
- -
- What do you expect in the next two years? 51.33% of the caregivers anticipated a stable course, 6.67% a deterioration, and 42% an improvement.
- -
- Would you agree to have your child participate in a potential clinical trial if, in the absence of side effects or with the possibility of minimal side effects, the prospect was to slow down or to improve or stop the deterioration of motor function? 68.67% of the caregivers would participate if the treatment slowed down deterioration, 77.33% if it would stop deterioration, and 96% if the treatment would produce an improvement.
- -
- Would you consider having your child participate in a clinical trial if it was offered the prospect of achieving at least 1, 2, or more than 2 of the following activities on the HFMSE/RULM? At the time of this question, the first three items that had not been fully achieved on the scale were shown to the caregivers as the activities that could be possibly achieved. Approximately 60% would participate in a clinical trial if at least 1 or 2 of the 3 activities could be achieved, with 99% agreeing to participate if more than 2 activities could be achieved.
- New questions:
- -
- With the advent of new pharmacological therapies, how has your perception of your child’s disease changed?: 22% of the caregivers reported no change, 74% felt more positive, 0% felt more negative, and 4% was uncertain.
- -
- What are your expectations regarding the new pharmacological therapies?: 16% reported no change, 78.77% were more positive, 2% were more negative and 3.33% were uncertain.
- Caregivers subdivided by patient’s age
- -
- Clinical course perception over the previous year: (x2 (2,N = 150)= 7.906, p = 0.019), with the carers of pediatric patients reporting more cases of improvement than the carers of adult patients.
- -
- Perception of the disease has changed with the advent of new therapies: (x2 (2, N = 150) = 7.357, p = 0.025), with carers of pediatric patients having a more positive approach than the carers of adult patients.
- Comparison between patients’ and caregivers’ responses
- Comparison between 2016 and 2022 caregivers’ responses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Questionnaire
- -
- Speaking of motor skills, please indicate if in the last year your child:
- (1)
- remained stable
- (2)
- deteriorated
- (3)
- improved
- -
- What do you expect in the next two years?
- (1)
- to remain stable
- (2)
- to deteriorate
- (3)
- to improve
- -
- Would you consider having your child participate in a clinical trial if it was offered the prospect of achieving at least 1, 2, or more than 2 of the following activities on the HFMSE from score 0?
- (1)
- yes:
- (a)
- at least 1 activity
- (b)
- at least 2 activities
- (c)
- more than 2 activities
- (2)
- no
- (3)
- unknown
- -
- Would you consider having your child participate in a clinical trial if it was offered the prospect of achieving at least 1, 2, or more than 2 of the following activities on the HFMSE from score 1?
- (1)
- yes:
- (a)
- at least 1 activity
- (b)
- at least 2 activities
- (c)
- more than 2 activities
- (2)
- no
- (3)
- unknown
- -
- Would you consider having your child participate in a clinical trial if it was offered the prospect of achieving at least 1, 2, or more than 2 of the following activities on the RULM from score 0?
- (1)
- yes:
- (a)
- at least 1 activity
- (b)
- at least 2 activities
- (c)
- more than 2 activities
- (2)
- no
- (3)
- unknown
- -
- Would you consider having your child participate in a clinical trial if it was offered the prospect of achieving at least 1, 2, or more than 2 of the following activities on the RULM from score 1?
- (1)
- yes:
- (a)
- at least 1 activity
- (b)
- at least 2 activities
- (c)
- more than 2 activities
- (2)
- no
- (3)
- unknown
- -
- Would you agree to have your child participate in a potential clinical trial if, in the absence of side effects or with the possibility of minimal side effects, the prospect was
- (1)
- to slow down deterioration of motor function? Yes/No/Unknown
- (2)
- to improve motor function? Yes/No/Unknown
- (3)
- to stop the deterioration of motor function? Yes/No/Unknown
- -
- Would you consider having your child take part in a potential trial in the presence of mild side-effects defined as
- (1)
- headache? Yes/No/Unknown
- (2)
- abdominal discomfort? Yes/No/Unknown
- (3)
- tachycardia? Yes/No/Unknown
- New Questions
- -
- With the advent of new pharmacological therapies, how has your perception of your child’s disease changed?
- (1)
- It has not changed
- (2)
- Has changed, I am more positive
- (3)
- Has changed, I am more negative
- (4)
- I do not know
- -
- What are your expectations regarding the new pharmacological therapies?
- (1)
- Have not changed
- (2)
- They have changed, I have more positive expectations
- (3)
- They have changed, I have more negative expectations
- (4)
- I do not know
References
- Keinath, M.C.; Prior, D.E.; Prior, T.W. Spinal Muscular Atrophy: Mutations, Testing, and Clinical Relevance. Appl. Clin. Genet. 2021, 14, 11–25. [Google Scholar] [CrossRef]
- Lefebvre, S.; Bürglen, L.; Reboullet, S.; Clermont, O.; Burlet, P.; Viollet, L.; Benichou, B.; Cruaud, C.; Millasseau, P.; Zeviani, M.; et al. Identification and characterization of a spinal muscular atrophy-determining gene. Cell 1995, 80, 155–165. [Google Scholar] [CrossRef] [Green Version]
- Dubowitz, V. Chaos in classification of the spinal muscular atrophies of childhood. Neuromuscul. Disord. 1991, 1, 77–80. [Google Scholar] [CrossRef]
- Dubowitz, V. Chaos in the classification of SMA: A possible resolution. Neuromuscul. Disord. 1995, 5, 3–5. [Google Scholar] [CrossRef]
- Mercuri, E.; Finkel, R.S.; Muntoni, F.; Wirth, B.; Montes, J.; Main, M.; Mazzone, E.S.; Vitale, M.; Snyder, B.; Quijano-Roy, S.; et al. Diagnosis and management of spinal muscular atrophy: Part 1, Recommendations for diagnosis, rehabilitation, orthopedic and nutritional care. Neuromuscul. Disord. 2017, 28, 103–115. [Google Scholar] [CrossRef] [Green Version]
- Messina, S.; Sframeli, M. New Treatments in Spinal Muscular Atrophy: Positive Results and New Challenges. J. Clin. Med. 2020, 9, 2222. [Google Scholar] [CrossRef]
- Jedrzejowska, M.; Kostera-Pruszczyk, A. Spinal muscular atrophy—New therapies, new challenges. Neurol. Neurochir. Pol. 2020, 54, 8–13. [Google Scholar] [CrossRef]
- Pacione, M.; Siskind, C.E.; Day, J.W.; Tabor, H.K. Perspectives on Spinraza (Nusinersen) Treatment Study: Views of Individuals and Parents of Children Diagnosed with Spinal Muscular Atrophy. J. Neuromuscul. Dis. 2018, 6, 119–131. [Google Scholar] [CrossRef]
- Van Kruijsbergen, M.; Schröder, C.D.; Ketelaar, M.; van der Pol, W.L.; Cuppen, I.; van der Geest, A.; Asselman, F.L.; Fischer, M.J.; Visser-Meily, J.M.A.; Kars, M.C. Parents’ perspectives on nusinersen treatment for children with spinal muscular atrophy. Dev. Med. Child. Neurol. 2021, 63, 816–823. [Google Scholar] [CrossRef]
- US Food and Drug Administration. FDA Staff Manual Guides; Directives, A., Ed.; US Food and Drug Administration: Silver Spring, MD, USA, 2022. Available online: https://www.fda.gov/media/131716/download (accessed on 10 May 2022).
- US Food and Drug Administration. Statement from FDA Commissioner Scott Gottlieb, M.D.; on FDA’s Efforts to Enhance the Patient Perspective and Experience in Drug Development and Review. 2018. Available online: https://www.fda.gov/news-events/press-announcements/statement-fda-commissioner-scott-gottlieb-md-fdas-efforts-enhance-patient-perspective-and-experience?utm_campaign=03302018_Statement_risk+benefit&utm_medium=email&utm_source=Eloqua (accessed on 29 March 2018).
- Ruperto, N.; Eichler, I.; Herold, R.; Vassal, G.; Giaquinto, C.; Hjorth, L.; Valls-i-Soler, A.; Peters, C.; Helms, P.J.; Saint Raymond, A. A European Network of Paediatric Research at the European Medicines Agency (Enpr-EMA). Arch. Dis. Child. 2012, 97, 185–188. [Google Scholar] [CrossRef]
- Pera, M.C.; Coratti, G.; Forcina, N.; Mazzone, E.S.; Scoto, M.; Montes, J.; Pasternak, A.; Mayhew, A.; Messina, S.; Sframeli, M.; et al. Content validity and clinical meaningfulness of the HFMSE in spinal muscular atrophy. BMC Neurol. 2017, 17, 39. [Google Scholar] [CrossRef] [Green Version]
- European Union. Ethical considerations for clinical trials on medicinal products conducted with the paediatric population. Eur. J. Health Law. 2008, 15, 223–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glanzman, A.M.; Mazzone, E.S.; Young, S.D.; Gee, R.; Rose, K.; Mayhew, A.; Nelson, L.; Yun, C.; Alexander, K.; Darras, B.T.; et al. Evaluator Training and Reliability for SMA Global Nusinersen Trials1. J. Neuromuscul. Dis. 2018, 5, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Main, M.; Kairon, H.; Mercuri, E.; Muntoni, F. The Hammersmith functional motor scale for children with spinal muscular atrophy: A scale to test ability and monitor progress in children with limited ambulation. Eur. J. Paediatr. Neurol. 2003, 7, 155–159. [Google Scholar] [CrossRef]
- Mazzone, E.S.; Mayhew, A.; Montes, J.; Ramsey, D.; Fanelli, L.; Young, S.D.; Salazar, R.; De Sanctis, R.; Pasternak, A.; Glanzman, A.; et al. Revised upper limb module for spinal muscular atrophy: Development of a new module. Muscle Nerve 2016, 55, 869–874. [Google Scholar] [CrossRef]
- Mercuri, E.; Messina, S.; Battini, R.; Berardinelli, A.; Boffi, P.; Bono, R.; Bruno, C.; Carboni, N.; Cini, C.; Colitto, F.; et al. Reliability of the Hammersmith functional motor scale for spinal muscular atrophy in a multicentric study. Neuromuscul. Disord. 2006, 16, 93–98. [Google Scholar] [CrossRef] [PubMed]
- O’Hagen, J.M.; Glanzman, A.M.; McDermott, M.P.; Ryan, P.A.; Flickinger, J.; Quigley, J.; Riley, S.; Sanborn, E.; Irvine, C.; Martens, W.B.; et al. An expanded version of the Hammersmith Functional Motor Scale for SMA II and III patients. Neuromuscul. Disord. 2007, 17, 693–697. [Google Scholar]
- Coratti, G.; Ricci, M.; Capasso, A.; D’amico, A.; Sansone, V.; Bruno, C.; Messina, S.; Ricci, F.; Mongini, T.; Coccia, M.; et al. Prevalence of Spinal Muscular Atrophy in the Era of Disease-Modifying Therapies: An Italian Nationwide Survey. Neurology 2023, 100, 522–528. [Google Scholar] [CrossRef]
- Mercuri, E.; Baranello, G.; Boespflug-Tanguy, O.; De Waele, L.; Goemans, N.; Kirschner, J.; Masson, R.; Mazzone, E.S.; Pechmann, A.; Pera, M.C.; et al. Risdiplam in types 2 and 3 spinal muscular atrophy: A randomised, placebo-controlled, dose-finding trial followed by 24 months of treatment. Eur. J. Neurol. 2022, 30, 1945–1956. [Google Scholar] [CrossRef]
- Mercuri, E.; Deconinck, N.; Mazzone, E.S.; Nascimento, A.; Oskoui, M.; Saito, K.; Vuillerot, C.; Baranello, G.; Boespflug-Tanguy, O.; Goemans, N.; et al. Safety and efficacy of once-daily risdiplam in type 2 and non-ambulant type 3 spinal muscular atrophy (SUNFISH part 2): A phase 3, double-blind, randomised, placebo-controlled trial. Lancet Neurol. 2022, 21, 42–52. [Google Scholar] [CrossRef]
- Maggi, L.; Bello, L.; Bonanno, S.; Govoni, A.; Caponnetto, C.; Passamano, L.; Grandis, M.; Trojsi, F.; Cerri, F.; Ferraro, M.; et al. Nusinersen safety and effects on motor function in adult spinal muscular atrophy type 2 and 3. J. Neurol. Neurosurg. Psychiatry 2020, 91, 1166–1174. [Google Scholar] [CrossRef] [PubMed]
- Scheijmans, F.E.V.; Cuppen, I.; van Eijk, R.P.A.; Wijngaarde, C.A.; Schoenmakers, M.A.G.C.; van der Woude, D.R.; Bartels, B.; Veldhoen, E.S.; Oude Lansink, I.L.B.; Groen, E.J.N.; et al. Population-based assessment of nusinersen efficacy in children with spinal muscular atrophy: A 3-year follow-up study. Brain Commun. 2022, 4, fcac269. [Google Scholar] [CrossRef] [PubMed]
- Hagenacker, T.; Wurster, C.D.; Günther, R.; Schreiber-Katz, O.; Osmanovic, A.; Petri, S.; Weiler, M.; Ziegler, A.; Kuttler, J.; Koch, J.C.; et al. Nusinersen in adults with 5q spinal muscular atrophy: A non-interventional, multicentre, observational cohort study. Lancet Neurol. 2020, 19, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Coratti, G.; Cutrona, C.; Pera, M.C.; Bovis, F.; Ponzano, M.; Chieppa, F.; Antonaci, L.; Sansone, V.; Finkel, R.; Pane, M.; et al. Motor function in type 2 and 3 SMA patients treated with Nusinersen: A critical review and meta-analysis. Orphanet J. Rare Dis. 2021, 16, 430. [Google Scholar] [CrossRef]
- Belter, L.; Cruz, R.; Jarecki, J. Quality of life data for individuals affected by spinal muscular atrophy: A baseline dataset from the Cure SMA Community Update Survey. Orphanet J. Rare Dis. 2020, 15, 217. [Google Scholar] [CrossRef]
- De Oliveira, C.M.; Araujo, A. Self-reported quality of life has no correlation with functional status in children and adolescents with spinal muscular atrophy. Eur. J. Paediatr. Neurol. 2011, 15, 36–39. [Google Scholar] [CrossRef]
- Sansone, V.A.; Pirola, A.; Lizio, A.; Greco, L.C.; Coratti, G.; Casiraghi, J.; Pane, M.; Pera, M.C.; Italiano, C.; Messina, S.; et al. The Spinal Muscular Atrophy Health Index: Italian validation of a disease-specific outcome measure. Neuromuscul. Disord. 2021, 31, 409–418. [Google Scholar] [CrossRef]
- Madruga-Garrido, M.; Vázquez-Costa, J.F.; Medina-Cantillo, J.; Brañas, M.; Cattinari, M.G.; de Lemus, M.; Díaz-Abós, P.; Sánchez-Menéndez, V.; Terrancle, Á.; Rebollo, P.; et al. Design of a Non-Interventional Study to Validate a Set of Patient- and Caregiver-Oriented Measurements to Assess Health Outcomes in Spinal Muscular Atrophy (SMA-TOOL Study). Neurology 2021, 10, 361–373. [Google Scholar] [CrossRef]
- Messina, S.; Frongia, A.L.; Antonaci, L.; Pera, M.C.; Coratti, G.; Pane, M.; Pasternak, A.; Civitello, M.; Montes, J.; Mayhew, A.; et al. A critical review of patient and parent caregiver oriented tools to assess health-related quality of life, activity of daily living and caregiver burden in spinal muscular atrophy. Neuromuscul. Disord. 2019, 29, 940–950. [Google Scholar] [CrossRef]
- McGraw, S.; Qian, Y.; Henne, J.; Jarecki, J.; Hobby, K.; Yeh, W.S. A qualitative study of perceptions of meaningful change in spinal muscular atrophy. BMC Neurol. 2017, 17, 68. [Google Scholar] [CrossRef] [Green Version]
- Rouault, F.; Christie-Brown, V.; Broekgaarden, R.; Gusset, N.; Henderson, D.; Marczuk, P.; Schwersenz, I.; Bellis, G.; Cottet, C. Disease impact on general well-being and therapeutic expectations of European Type II and Type III spinal muscular atrophy patients. Neuromuscul. Disord. 2017, 27, 428–438. [Google Scholar] [CrossRef] [PubMed]
- Weaver, M.S.; Hanna, R.; Hetzel, S.; Patterson, K.; Yuroff, A.; Sund, S.; Schultz, M.; Schroth, M.; Halanski, M.A. A Prospective, Crossover Survey Study of Child- and Proxy-Reported Quality of Life According to Spinal Muscular Atrophy Type and Medical Interventions. J. Child. Neurol. 2020, 35, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, A.J.; Thompson, R.; Gallop, K.; Teynor, M. Estimation Of The Quality Of Life Benefits Associated With Treatment For Spinal Muscular Atrophy. Clin. Outcomes Res. 2019, 11, 615–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mix, L.; Winter, B.; Wurster, C.D.; Platen, S.; Witzel, S.; Uzelac, Z.; Graf, H.; Ludolph, A.C.; Lulé, D. Quality of Life in SMA Patients Under Treatment With Nusinersen. Front. Neurol. 2021, 12, 626787. [Google Scholar] [CrossRef] [PubMed]
- Osmanovic, A.; Ranxha, G.; Kumpe, M.; Müschen, L.; Binz, C.; Wiehler, F.; Paracka, L.; Körner, S.; Kollewe, K.; Petri, S.; et al. Treatment expectations and patient-reported outcomes of nusinersen therapy in adult spinal muscular atrophy. J. Neurol. 2020, 267, 2398–2407. [Google Scholar] [CrossRef] [PubMed]
- Cruz, R.; Lenz, M.; Belter, L.; Hobby, K.; Jarecki, J. The Voice of the Patient Report for Spinal Muscular Atrophy. 2018. Available online: https://www.curesma.org/wp-content/uploads/2018/01/SMA-VoP-for-publication-1-22-2018.pdf (accessed on 10 January 2018).
- Gusset, N.; Stalens, C.; Stumpe, E.; Klouvi, L.; Mejat, A.; Ouillade, M.C.; de Lemus, M. Understanding European patient expectations towards current therapeutic development in spinal muscular atrophy. Neuromuscul. Disord. 2021, 31, 419–430. [Google Scholar] [CrossRef] [PubMed]
- SMA-EUROPE. SMA Daily Life Study. 2022. Available online: https://www.sma-europe.eu/sma-daily-life-study (accessed on 1 March 2023).
- Fischer, M.J.; Ketelaar, M.; van der Veere, P.J.; Verhoef, M.; Wadman, R.L.; Visser-Meily, J.M.A.; van der Pol, M.L.; Schröder, C.D. Illness perceptions in pediatric spinal muscular atrophy: Agreement between children and their parents, and its association with quality of life. J. Dev. Phys. Disabil. 2020, 33, 297–310. [Google Scholar] [CrossRef]
- Qian, Y.; McGraw, S.; Henne, J.; Jarecki, J.; Hobby, K.; Yeh, W.S. Understanding the experiences and needs of individuals with spinal muscular atrophy and their parents: A qualitative study. BMC Neurol. 2015, 15, 217. [Google Scholar] [CrossRef] [Green Version]
- Mongiovi, P.; Dilek, N.; Garland, C.; Hunter, M.; Kissel, J.T.; Luebbe, E.; McDermott, M.P.; Johnson, N.; Heatwole, C. Patient reported impact of symptoms in spinal muscular atrophy (PRISM-SMA). Neurology 2018, 91, e1206–e1214. [Google Scholar] [CrossRef]
- Belter, L.; Jarecki, J.; Hobby, K.; Teynor, M. Family impact and health-related quality of life (HRQoL) of parents and individuals with SMA. Neuromuscul. Disord. 2017, 27, S224. [Google Scholar] [CrossRef]
- Sonney, J.; Insel, K.C.; Segrin, C.; Gerald, L.B.; Ki Moore, I.M. Association of asthma illness representations and reported controller medication adherence among school-aged children and their parents. J. Pediatr. Health Care 2017, 31, 703–712. [Google Scholar] [CrossRef] [PubMed]
- Szentes, A.; Kokonyei, G.; Bekesi, A.; Bokretas, I.; Torok, S. Differences in illness perception between children with cancer and other chronic diseases and their parents. Clin. Child. Psychol. Psychiatry 2018, 23, 365–380. [Google Scholar] [CrossRef] [PubMed]
- Giannousi, Z.; Karademas, E.C.; Dimitraki, G. Illness representations and psychological adjustment of Greek couples dealing with a recently-diagnosed cancer: Dyadic, interaction and perception-dissimilarity effects. J. Behav. Med. 2016, 39, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Karademas, E.C.; Zarogiannos, A.; Karamvakalis, N. Cardiac patient-spouse dissimilarities in illness perception: Associations with patient self-rated health and coping strategies. Psychol. Health 2010, 25, 451–463. [Google Scholar] [CrossRef]
- Richardson, A.E.; Morton, R.; Broadbent, E. Caregivers’ illness perceptions contribute to quality of life in head and neck Cancer patients at diagnosis. J. Psychosoc. Oncol. 2015, 33, 414–432. [Google Scholar] [CrossRef]
- Twiddy, M.; House, A.; Jones, F. The association between discrepancy in illness representations on distress in stroke patients and carers. J. Psychosom. Res. 2012, 72, 220–225. [Google Scholar] [CrossRef]


{kind=link}
| Caregiver (n = 150) | Patients (n = 45) | |||||
|---|---|---|---|---|---|---|
| All | Adult (n = 72 ) | Pediatric (n = 78) | All | Adult (n = 33) | Pediatric (n = 12) | |
| Patient’s age (years) 1 | 3–71 (20.18; 14.24) | 18–71 (31.11; 13.32) | 3–17 (10.08; 3.77) | 14–62 (24.09; 10.22) | 18–62 (27.18; 10.31) | 14–17 (15.58; 0.99) |
| Gender 2 | 82 F (54.66%) 68 M (45.33%) | 40 F (55.55%) 32 M (44.44%) | 42 F (53.84%) 36 M (46.15%) | 26 F (57.77%) 19 M (42.22%) | 18 F (54.54%) 15 M (45.45%) | 8 F (66.66%) 4 M (33.33%) |
| Sma Type 2 | ||||||
| Sma Type II | 90 (60.00%) | 36 (50%) | 54 (69.23%) | 24 (53.33%) | 17 (51.51%) | 7 (58.33%) |
| Ambulant | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) |
| Non Ambulant | 90 (100.00%) | 36 (100.00%) | 54 (100.00%) | 24 (100.00%) | 17 (100%) | 7 (100.00%) |
| Sma Type III | 60 (40.00%) | 36 (50%) | 24 (30.76%) | 21 (46.66%) | 16 (48.48%) | 5 (41.66%) |
| Ambulant | 26 (43.33%) | 11 (30.55%) | 15 (62.5%) | 13 (61.90%) | 11 (68.75%) | 2 (40%) |
| Non Ambulant | 34 (56.66%) | 25 (69.44%) | 9 (37.5%) | 8 (38.09%) | 5 (31.25%) | 3 (60%) |
| Whole Cohort (N; %) | ||
|---|---|---|
| HFMSE Acquisition from score 0 Not applicable in 11 patients | I would not participate | 1; 0.72% |
| At least 1 activity | 83; 59.71% | |
| Two activities | 92; 66.19% | |
| More than 2 activities | 138; 99.28% | |
| HFMSE Improvements from score 1 Not applicable in 35 patients | I would not participate | 2; 1.74% |
| At least 1 activity | 70; 60.87% | |
| Two activities | 81; 70.43% | |
| More than 2 activities | 113; 98.26% | |
| RULM Acquisition from score 0 Not applicable in 31 patients | I would not participate | 1; 0.84% |
| At least 1 activity | 67; 56.30% | |
| Two activities | 77; 64.71% | |
| More than 2 activities | 118; 99.16% | |
| RULM Improvements from score 1 Not applicable in 30 patients | I would not participate | 1; 0.83% |
| At least 1 activity | 78; 65% | |
| Two activities | 85; 70.83% | |
| More than 2 activities | 119; 99.17% |
| Patients Cohort (N; %) | Caregivers Cohort (N; %) | x2 p Value | ||
|---|---|---|---|---|
| Question 1 | ||||
| Speaking of motor skills, please indicate if in the last year you: | Remained stable | 29; 64.44% | 28; 62.22% | (x2 (2, N = 90) = 0.461, p = 0.794) |
| Deteriorated | 4; 8.89% | 6; 13.33% | ||
| Improved | 12; 26.67% | 11; 24.44% | ||
| Question 2 | ||||
| What do you expect in the next two years | Stable course | 32; 71.11% | 22; 48.89% | (x2 (2, N = 90) = 4.977, p = 0.083) |
| Deterioration | 2; 4.44% | 2; 4.44% | ||
| Improvement | 21; 46.67% | |||
| Question 3 | ||||
| Would you agree to have participate in a potential clinical trial if, in the absence of side effects or with the possibility of minimal side effects, the prospective was: | Slow down | 29; 64.44% | 33; 73.33% | (x2 (1, N = 90) = 8.29, p = 0.362) |
| Stop deterioration | 37; 82.22% | 36; 80.00% | (x2 (1, N = 90) = 0.73, p = 0.788) | |
| Improve | 45; 100% | 45; 100.00% | N/A | |
| Questions 4–7 | ||||
| Would you consider participating in a clinical trial if it offered the prospect of achieving at least 1, 2, or more than 2 activities on the HFMSE/RULM | ||||
| HFMSE Acquisition from score 0 Not applicable in 3 patients | I would not participate | 3; 7.14% | 0; 0.00% | (x2 (3, N = 84) = 6.205, p = 0.102) |
| At least 1 activity | 21; 50% | 27; 64.29% | ||
| Two activities | 29; 69.05% | 30; 71.43% | ||
| More than 2 activities | 39; 92.86% | 42; 100.00% | ||
| HFMSE Improvements from score 1 Not applicable in 6 patients | I would not participate | 5; 12.82% | 0; 0.00% | (x2 (3, N = 78) = 7.067, p = 0.07) |
| At least 1 activity | 18; 46.15% | 22; 56.41% | ||
| Two activities | 24; 61.54% | 25; 64.10% | ||
| More than 2 activities | 34; 87.18% | 39; 100.00% | ||
| RULM Acquisition from score 0 Not applicable in 8 patients | I would not participate | 1; 2.7% | 0; 0.00% | (x2 (3,N = 74) = 4.100, p = 0.251) |
| At least 1 activity | 16; 43.24% | 24; 64.86% | ||
| Two activities | 21; 56.76% | 27; 72.97% | ||
| More than 2 activities | 36; 97.30% | 37; 100.00% | ||
| RULM Improvements from score 1 Not applicable in 12 patients | I would not participate | 1; 3.03% | 0; 0.00% | (x2 (3,N = 66) = 1.981, p = 0.576) |
| At least 1 activity | 19; 57.58% | 22; 66.67% | ||
| Two activities | 20; 60.61% | 24; 72.73% | ||
| More than 2 activities | 32; 96.97% | 33; 100.00% | ||
| Question 8 | ||||
| With the advent of new pharmacological therapies, how has your perception of the disease changed? | No change | 16; 35.56% | 13; 28.89% | (x2 (2, N = 90) = 0.796, p = 0.672) |
| More positive | 26; 57.78% | 30; 66.67% | ||
| More negative | 0; 0.00% | 0; 0.00% | ||
| Uncertain | 3; 6.67% | 2; 4.44% | ||
| Question 9 | ||||
| What are your expectations regarding the new pharmacological therapies | No change | 12; 26.67% | 6; 13.33% | (x2 (2, N = 90) = 3.362, p = 0.339) |
| More positive | 32; 71.11% | 37; 82.22% | ||
| More negative | 0; 0.00% | 1; 2.22% | ||
| Uncertain | 1; 2.22% | 1; 2.22% | ||
| Caregiver 2016 (n = 139) | Caregiver 2022 (n = 78) | |
|---|---|---|
| Age 1 | 1.5–17 y (7.38; 3.86) | 3 y–17 y (10.08; 3.77) |
| Gender 2 | 63 F (45.32%) 76 M (54.67%) | 43 F (55.10%) 35 M (44.87%) |
| SMA Type 2 | ||
| SMA Type II | 103 (74.10%) | 54 (69.23%) |
| SMA Type III | 36 (25.89%) | 24 (30.76%) |
| Ambulant | 30 (83.33%) | 15 (62.50%) |
| Non ambulant | 6 (16.66%) | 9 (37.50%) |
| 2016 (N; %) | 2022 (N; %) | x2 p Value | ||
|---|---|---|---|---|
| Question 1 | ||||
| Speaking of motor skills, please indicate if in the last year you: | Remained stable | 23; 16.5% | 34; 43.6% | (x2 (2, N = 217) = 66.88, p < 0.001 **) |
| Deteriorated | 98; 70.5% | 10; 12.8% | ||
| Improved | 18; 12.9% | 34; 43.6% | ||
| Question 2 | ||||
| What do you expect in the next two years | Stable course | 30; 21.6% | 40; 51.3% | (x2 (2, N = 217) = 88.740, p < 0.001 **) |
| Deterioration | 96; 69.1% | 3; 3.8% | ||
| Improvement | 13; 9.4% | 35; 44.9% | ||
| Questions 3–6 | ||||
| Would you consider participating in a clinical trial if it offered the prospect of achieving at least 1, 2, or more than 2 activities on the HFMSE/RULM | ||||
| HFMSE | I would not participate | 4; 2.9% | 1; 1.3% | (x2 (4, N = 217) = 17.623, p < 0.001 **) |
| Acquisition from score 0 | At least 1 activity | 93; 66.9% | 46; 59.0% | |
| Two activities | 112; 80.6% | 48; 61.6% | ||
| More than 2 activities | 129; 92.8% | 73; 93.7% | ||
| HFMSE | I would not participate | 8; 5.8% | 1; 1.3% | (x2 (4, N = 78,217 10.518, p = 0.039 **) |
| Improvements from score 1 | At least 1 activity | 83; 59.7% | 44; 56.4% | |
| Two activities | 104; 74.8% | 50; 64.10% | ||
| More than 2 activities | 119; 89.6% | 68; 87.2% | ||
| RULM | I would not participate | 3; 2.2% | 1; 1.3% | (x2 (4, N = 217) = 12.156, p = 0.016 **) |
| Acquisition from score 0 | At least 1 activity | 69; 49.6% | 36; 46.2% | |
| Two activities | 82; 59.00% | 40; 51.3% | ||
| More than 2 activities | 92; 66.2% | 58; 74.4% | ||
| RULM | I would not participate | 15; 10.8% | 1; 1.3% | (x2 (4, N = 217) = 30.160, p < 0.001 **) |
| Improvements from score 1 | At least 1 activity | 61; 43.9% | 46; 59.0% | |
| Two activities | 80; 57.6% | 49; 62.8% | ||
| More than 2 activities | 89; 64.1% | 68; 87.2% | ||
| Question 7 | ||||
| Would you agree to have your child participate in a potential clinical trial if, in the absence of side effects or with the possibility of minimal side effects, the prospect was to slow down or to improve or to stop deterioration of motor function: | Slow down | |||
| Yes | 99; 71.2% | 55; 70.5% | (x2 (2, N = 217) = 4.330, p = 0.115) | |
| No | 17; 12.2% | 16; 20.5% | ||
| Uncertain | 23; 16.5% | 7; 9.00% | ||
| Stop deterioration | ||||
| Yes | 121; 87.1% | 62; 79.5% | (x2 (2, N = 217) = 3.272, p = 0.195) | |
| No | 7; 5.0% | 9; 11.5% | ||
| Uncertain | 11; 7.9% | 7; 9.00% | ||
| Improvement | ||||
| Yes | 134; 96.4% | 75; 96.2% | (x2 (2; N = 217) = 0.552; p = 0.759) | |
| No | 2; 1.4% | 2; 2.6% | ||
| Uncertain | 3; 2.2% | 1; 1.3% | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pera, M.C.; Coratti, G.; Casiraghi, J.; Bravetti, C.; Fedeli, A.; Strika, M.; Albamonte, E.; Antonaci, L.; Rossi, D.; Pane, M.; et al. Caregivers’ Expectations on Possible Functional Changes following Disease-Modifying Treatment in Type II and III Spinal Muscular Atrophy: A Comparative Study. J. Clin. Med. 2023, 12, 4183. https://doi.org/10.3390/jcm12134183
Pera MC, Coratti G, Casiraghi J, Bravetti C, Fedeli A, Strika M, Albamonte E, Antonaci L, Rossi D, Pane M, et al. Caregivers’ Expectations on Possible Functional Changes following Disease-Modifying Treatment in Type II and III Spinal Muscular Atrophy: A Comparative Study. Journal of Clinical Medicine. 2023; 12(13):4183. https://doi.org/10.3390/jcm12134183
Chicago/Turabian StylePera, Maria Carmela, Giorgia Coratti, Jacopo Casiraghi, Chiara Bravetti, Alessandro Fedeli, Milija Strika, Emilio Albamonte, Laura Antonaci, Diletta Rossi, Marika Pane, and et al. 2023. "Caregivers’ Expectations on Possible Functional Changes following Disease-Modifying Treatment in Type II and III Spinal Muscular Atrophy: A Comparative Study" Journal of Clinical Medicine 12, no. 13: 4183. https://doi.org/10.3390/jcm12134183