
Identifying Patients with Nonalcoholic Fatty Liver Disease in Primary Care: How and for What Benefit?

1
Department of Medicine, Medical University of South Carolina, 171 Ashley Ave, Charleston, SC 29425, USA
2
Institute of Cardiovascular & Medical Sciences, University of Glasgow, 126 University Place, Glasgow G12 8TA, UK
*
Authors to whom correspondence should be addressed.
J. Clin. Med. 2023, 12(12), 4001; https://doi.org/10.3390/jcm12124001
Submission received: 28 February 2023
/
Revised: 31 May 2023
/
Accepted: 1 June 2023
/
Published: 12 June 2023
(This article belongs to the Section Gastroenterology & Hepatopancreatobiliary Medicine)
Abstract
:Despite its increasing prevalence, nonalcoholic fatty liver disease (NAFLD) remains under-diagnosed in primary care. Timely diagnosis is critical, as NAFLD can progress to nonalcoholic steatohepatitis, fibrosis, cirrhosis, hepatocellular carcinoma, and death; furthermore, NAFLD is also a risk factor linked to cardiometabolic outcomes. Identifying patients with NAFLD, and particularly those at risk of advanced fibrosis, is important so that healthcare practitioners can optimize care delivery in an effort to prevent disease progression. This review debates the practical issues that primary care physicians encounter when managing NAFLD, using a patient case study to illustrate the challenges and decisions that physicians face. It explores the pros and cons of different diagnostic strategies and tools that physicians can adopt in primary care settings, depending on how NAFLD presents and progresses. We discuss the importance of prescribing lifestyle changes to achieve weight loss and mitigate disease progression. A diagnostic and management flow chart is provided, showing the key points of assessment for primary care physicians. The advantages and disadvantages of advanced fibrosis risk assessments in primary care settings and the factors that influence patient referral to a hepatologist are also reviewed.
1. Introduction
Nonalcoholic fatty liver disease (NAFLD) is a leading cause of chronic liver disease worldwide [1], with an estimated global prevalence of around 32.4% [2]; however, further studies are needed to provide more accurate prevalence data. While regional prevalence estimates may vary [1,2,3,4], NAFLD is a major contributor to liver-related morbidity and mortality worldwide [5]. Alongside a rise in prevalence, NAFLD has emerged as a driver of cirrhosis and hepatocellular carcinoma (HCC) and is increasing the need for liver transplantation [6,7,8]. NAFLD is characterized by the buildup of fat in the liver, or “steatosis”, in the absence of other causes of secondary hepatic steatosis, such as alcohol consumption, viral hepatitis, or other chronic liver diseases [9]. In this way, NAFLD is a form of ectopic fat, often linked to excess fat in other ectopic tissues such as the blood vessels, the heart, and the pancreas [10], although steatosis alone does not define liver disease. Excess ectopic fat perturbs triglyceride synthesis and glucose metabolism and is linked to a higher vascular risk [10]. Consequently, NAFLD is associated with conditions of metabolic dysfunction, including type 2 diabetes (T2D), obesity, hypertension, and dyslipidemia [1,11]. The coexistence of these metabolic conditions with NAFLD, specifically T2D and obesity, is associated with severe liver-related outcomes, such as nonalcoholic steatohepatitis (NASH), advanced fibrosis, cirrhosis, and mortality [9,12,13,14,15,16,17].
Despite the prevalence and growing burdens of morbidity and mortality, NAFLD is under-diagnosed in real-world primary care settings [18,19,20]. The factors contributing to this under recognition likely include the absence of recommendations for systematic routine NAFLD screening, the uncertainties related to the currently available diagnostic tests, and the lack of pharmacologic therapies that are specifically approved for the reversal of NAFLD/NASH [9,21,22,23]. In addition, recommendations for NAFLD care have predominantly appeared in specialty journals [24], and many countries do not have primary care follow-up algorithms [25]. Thus, primary care physicians (PCPs) report unfamiliarity with, and limited access to, the currently available tools for assessing NAFLD disease progression and identifying patients at greatest risk of future poor health outcomes [26,27]. Due to the progressive nature of NAFLD, a timely diagnosis of the disease is considered important to provide healthcare practitioners the opportunity to motivate patients to make lifestyle changes that could mitigate disease progression and related conditions, such as diabetes. As the prevalence of NAFLD and related metabolic conditions is rising [28,29], patients with these conditions are becoming an increasingly larger cohort in primary care settings. Monitoring patients with known risk factors in primary care will, in turn, become increasingly important. PCPs, therefore, play a critical role in identifying and diagnosing patients with NAFLD, which will help to inform treatment management plans and may prevent disease progression.
This review will address the challenges that NAFLD presents and will reinforce the critical diagnosis and management strategies that physicians can perform in primary care settings. Specifically, we will emphasize the importance of diagnosing NAFLD, prescribing weight-loss interventions, addressing cardiovascular risk, and assessing for advanced fibrosis in patients diagnosed with NAFLD. A longitudinal, representative case study will illustrate the application of these management concepts in a primary care patient. The patient case described in this publication is fictional and does not represent actual events or a response from an actual patient. The authors developed this fictional case for educational purposes only.
2. Pathophysiology of NAFLD
The pathophysiology of NAFLD spans a continuum from simple steatosis with no, or minor, inflammation (nonalcoholic fatty liver (NAFL)) to steatosis, accompanied by inflammation (NASH), fibrosis, and cirrhosis [30]. However, Medicare claims data from the US indicate that, among patients initially diagnosed with NAFLD/NASH, there is a 39% probability of it progressing to more severe liver disease over an 8-year follow-up period [19]. It is worth noting that the relatively low incidence of NAFLD reported in the Medicare sample (5.7%) [19] may bias this estimated risk of disease progression. Steatosis is the key defining histologic feature across the NAFLD spectrum [30], and guidelines recommend evidence of steatosis for diagnosis (see review [31]). Metabolic dysfunction appears to be central to the pathological processes, including the progression of NAFL to NASH, fibrosis, cirrhosis, and HCC [10,30,32]. When there is an oversupply of calories and/or insufficient expenditure causing weight gain, an excess of fatty acids leads to the buildup of toxic lipids in the liver [10,33]. Such toxic lipids accumulate at different body mass index (BMI) thresholds, depending on individuals’ underlying comorbidities, genetics, ethnicity, sex, age, and body fat distribution [10]. Over time, these toxic lipids can trigger the inflammatory pathways that contribute to the development of steatosis, inflammation, and progressive liver damage [10]. Prognostically, advanced fibrosis is the most important histological feature that is looked for in patients with NAFLD, with liver-related morbidity and mortality increasing with each progressive fibrosis stage [34,35,36,37]. Thus, advanced fibrosis is a warning sign of serious liver disease.
In real-world settings, patients with NAFLD exhibit heterogeneity in the clinical presentation and disease course of their fatty liver disease [38]. Multiple factors, including age, biological sex, hormonal status, alcohol intake, smoking, and metabolic status, can contribute to NAFLD progression, with factors potentially working synergistically to contribute toward the disease course [38]. A recent review panel has suggested that the nomenclature of NAFLD may not be fully reflective of the complexities of factors influencing the metabolism and disease progression, suggesting that NAFLD be renamed as metabolic-associated fatty liver disease (MAFLD) [38], although this new abbreviation has not had a wide uptake.
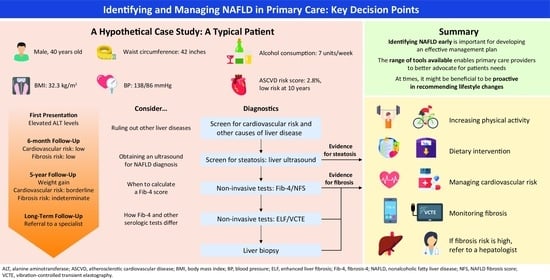
Case Study. First presentation: A new male patient attends clinic for an annual checkup (Figure 1).
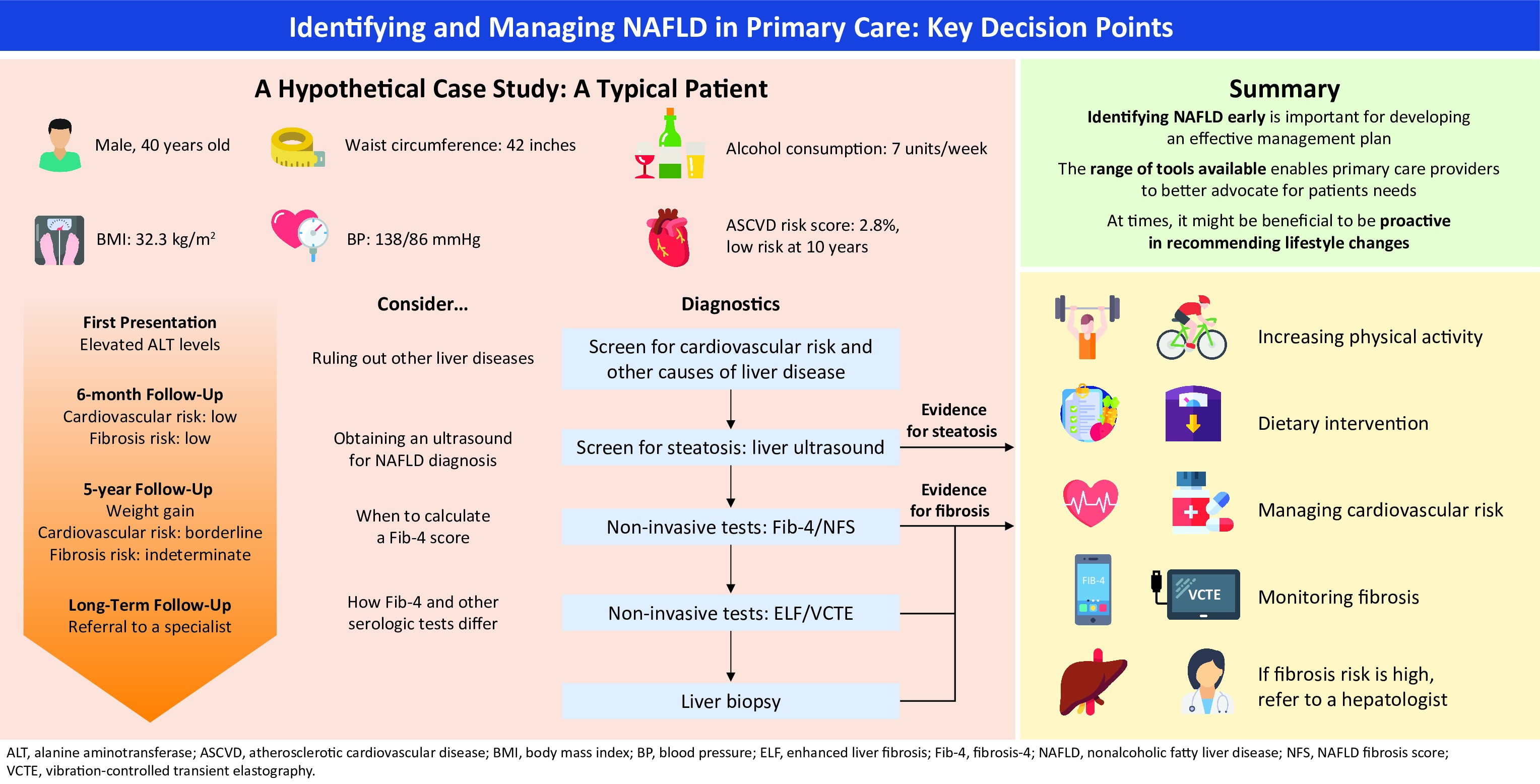
- Age: 40, BMI: 32.3 kg/m2, waist circumference: 42 inches, blood pressure: 138/86 mmHg, and consuming 7 units of alcohol per week;
- Cholesterol: 210 mg/dL, triglyceride: 174 mg/dL, high-density lipoprotein (HDL)-cholesterol: 31 mg/dL, and low-density lipoprotein (LDL)-cholesterol: 144 mg/dL;
- Alanine aminotransferase (ALT): 54 U/L, aspartate aminotransferase (AST): 44 U/L, and platelets: 220 K;
- Hemoglobin A1c (HbA1c): 6.1%;
- He is not taking any medications.
3. When to Pursue a NAFLD Diagnosis
3.1. Pursuing a NAFLD Diagnosis following Abnormalities in Aminotransferases or in Liver Imaging
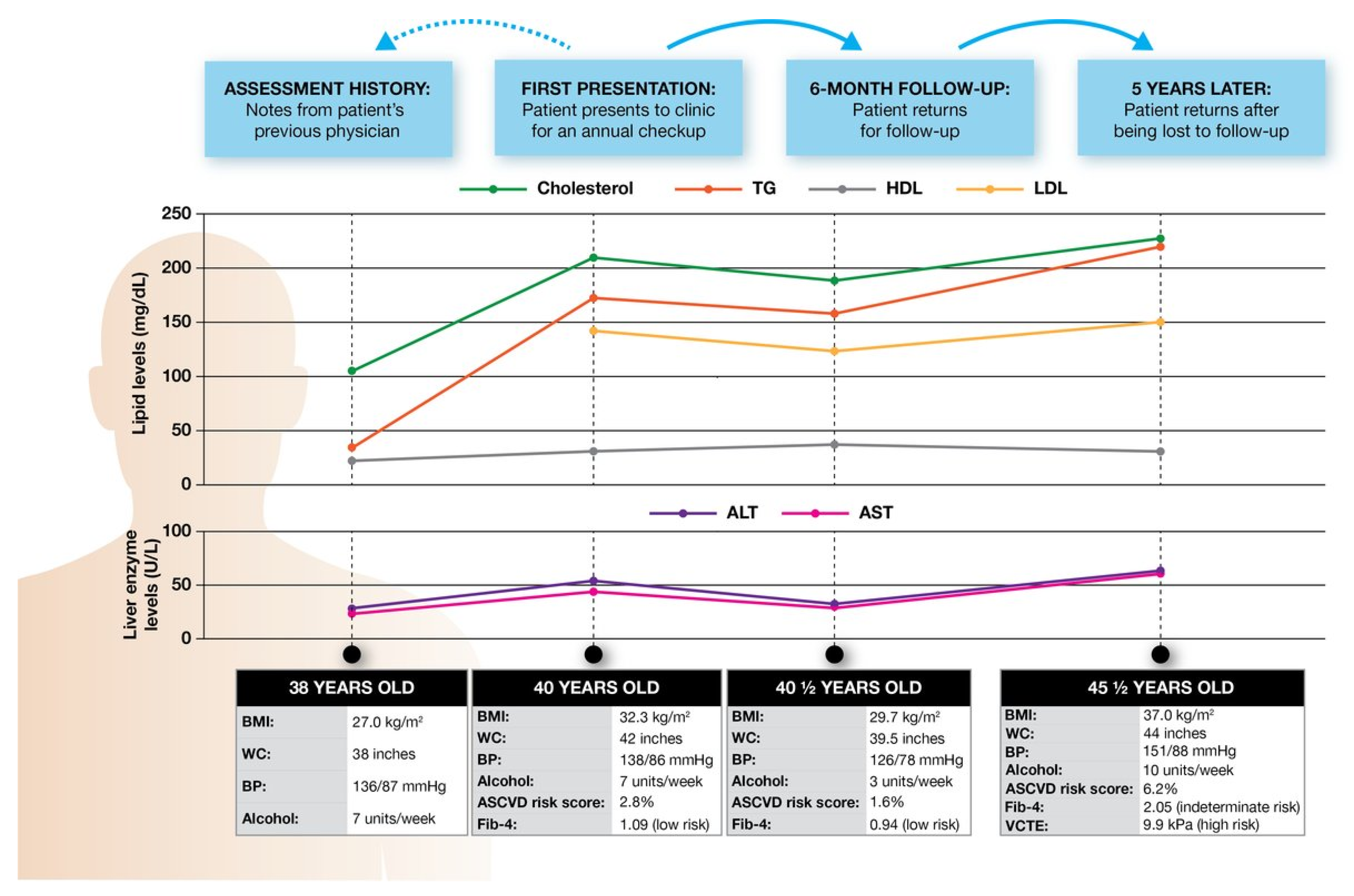
NAFLD is generally suspected during routine clinical care when abnormalities are detected in serum aminotransferases (alanine aminotransferase (ALT) and, to a lesser extent, aspartate aminotransferase (AST)) or steatosis is identified through liver imaging (Figure 2) [18,39,40]. NAFLD is a common cause of incidentally detected aminotransferase abnormalities [41,42]. The British Society of Gastroenterology and the American College of Gastroenterology (ACG) guidelines for addressing ALT and AST abnormalities recommend excluding competing liver disease diagnoses by obtaining a thorough exposure (alcohol and drug), medication (including herbal supplements), and travel history [43,44]. Additionally, these specialty society guidelines recommend viral hepatitis testing (hepatitis B surface antigen and hepatitis C antibody), a serologic hemochromatosis assessment (ferritin and transferrin saturation), autoimmune hepatitis testing (anti-mitochondrial, anti-smooth-muscle, and anti-nuclear antibodies, as well as serum immunoglobulins), and imaging with an abdominal ultrasound (US) (Box 1) [43,44]. Furthermore, the ACG guidelines recommend serologic evaluations for Wilson’s disease and alpha-1 antitrypsin deficiency [44]; however, ceruloplasmin testing for Wilson’s disease may be unnecessary in patients >55 years of age, given the rarity of late-onset Wilson’s disease and the monetary costs involved in testing [45,46]. A more focused testing strategy that incorporates the pre-test probability of liver diseases has been studied and the results suggested that testing limited to assessing viral hepatitis, alcohol history, and US imaging can reduce the costs and limit the occurrence of false-positive test results [46].
Box 1. Is it necessary to rule out other liver diseases before diagnosing NAFLD?
The current guidelines on abnormal liver function tests have adopted a “diagnosis of exclusion” strategy, recommending screening for and ruling out various causes of liver disease systematically. In primary care, the cost, waiting times, and availability may limit the utility of extensive screening strategies, particularly in patients at high risk for NAFLD. Taking a clinical history and recognizing risk factors is a practical first step to identifying at-risk patients and can help to determine how to proceed. In patients with abnormal serum ALT levels (or ALT levels near the high end of the normal range) and other features potentially consistent with NAFLD (such as excess adiposity or elevated triglyceride or HbA1c levels), one approach can be to recommend lifestyle changes without conducting further assessments. If the patients lose weight, and the ALT levels normalize or clinically meaningfully improve, a NAFLD diagnosis can be strongly suspected, especially if there are parallel improvements in related factors such as triglyceride and HbA1c levels [33]. If so, such findings would help to provide biochemical evidence of lower liver fat and alleviate the need for multiple expensive tests and the ensuing burden on the patient.
An alternative approach in at-risk patients can be to limit testing to the most common causes of disease (i.e., performing a viral hepatitis assessment, an alcohol and medication history, and a liver US). NAFLD can then be diagnosed if the viral hepatitis assessments are negative, the alcohol history is not suggestive of alcohol-related liver disease, the medication history shows the patient is not on steatogenic medication, and steatosis is detected by the US.
Although elevated ALT and AST levels may be a useful signal for pursuing a NAFLD diagnosis, a portion of patients with NAFLD may also present with normal aminotransferase levels, along with other metabolic features. A recent systematic review estimated that 25% of patients with NAFLD present with ALT values within the “normal” range, mainly in females and patients with diabetes [47]. Therefore, while abnormalities in serum aminotransferases may indicate the presence of NAFLD, they should not be used as the sole diagnostic criterion.
Incidental identification of hepatic steatosis on abdominal imaging can also prompt the pursuit of a NAFLD diagnosis. However, several small studies suggest that, even when steatosis is noted on radiographic imaging reports in patients with metabolic risk factors, a formal diagnosis is infrequently made [20,48]. Once hepatic steatosis is identified, physicians can assess for metabolic risk factors and evaluate for secondary causes of hepatic steatosis, including alcohol consumption, viral hepatitis, and medications (e.g., tamoxifen, amiodarone, and corticosteroids) [9].
3.2. Pursuing a NAFLD Diagnosis in High-Risk Patients
The clinical practice guidelines for NAFLD recommend that PCPs should consider screening patients who are at high risk for NAFLD, specifically those with metabolic risk factors such as obesity and diabetes [21,22], or be aware of the higher risk of NAFLD in such patients [9,49], while diabetes guidelines recommend evaluating high-risk patients for NAFLD and fibrosis when they present with elevated ALT levels or hepatic steatosis on a US [50]. The key risk factors mentioned in the guidelines include T2D, obesity, dyslipidemia, hypertriglyceridemia, elevated ALT and gamma-glutamyl transferase, and male sex [31]. Recent machine learning studies have verified and identified several clinical characteristics that are significant predictors of NAFLD, including male sex and increased waist circumference, age, hemoglobin A1c (HbA1c), BMI, AST, alkaline phosphatase, high-density lipoprotein (HDL)-cholesterol, triglycerides, and diastolic blood pressure [51,52].
4. How to Pursue a Diagnosis
Evidence of steatosis is required for a formal diagnosis of NAFLD across guidelines [31]. There are various noninvasive tests that can be used, each harboring their own advantages and disadvantages, with several key diagnostic tools discussed below.
4.1. Conventional US
Conventional US is commonly used and accepted as a first-line diagnostic tool for steatosis [22,53,54]. A US can reliably and accurately diagnose a moderate-to-severe fatty liver [55] and is widely available, relatively inexpensive, noninvasive, and radiation-free [53]. Despite its advantages, however, US has limited sensitivity in patients with low levels of liver fat (<10%) [56,57,58], meaning such patients with NAFLD are often not diagnosed. In addition, obesity can increase the technical difficulty of conducting a US, there is potential for inter/intraobserver variability in US interpretation, and the wait times for imaging can be lengthy in primary care [58,59,60]. For these reasons, PCPs may choose not to use conventional US as a first-line tool (Box 2); nonetheless, conventional US remains an important diagnostic tool for NAFLD diagnosis in primary care.
Box 2. Do all patients need a liver ultrasound for diagnosing NAFLD?
The guidelines recommend that evidence of steatosis is required for diagnosing NAFLD, with conventional US being recommended as a first-line diagnostic tool, as it is cheaper and more widely available than other imaging modalities, specifically, controlled attenuation parameter (CAP) and magnetic resonance imaging (MRI) methods (listed below). When NAFLD is suspected, visualizing steatosis provides PCPs and patients with a confirmatory result, which offers a level of certainty that will prompt a management plan.
Alternatively, initially recommending lifestyle changes prior to a confirmatory diagnosis allows for earlier intervention and avoids the costs and waiting times associated with diagnostic tests. If a patient shows improvement with lifestyle changes (e.g., a lowered ALT level and, if relevant, lowered triglyceride and/or HbA1c levels, alongside weight loss), a confirmatory test may not be needed, as the parallel improvements in several measures lend strong confidence to the diagnosis of NAFLD. A weight-loss--first approach can be considered when patients have features of metabolic dysfunction. However, more extensive testing should be considered in patients without these risk factors for NAFLD, or when weight loss does not improve ALT, triglyceride, and/or HbA1c levels.
4.2. CAP Method
CAP is a measure of liver steatosis that is obtained through the use of a transient elastography device, which is an accurate, noninvasive, and feasible technique, with a value of >275 dB/m having good sensitivity for detecting steatosis [53]. However, the limitations of CAP include its suboptimal performance for quantifying steatosis, in which it is outperformed by MRI-proton density fat fraction [53]; high skin-to-capsule distance potentially, causing an overestimation of steatosis level [61]; and CAP measurements potentially being affected by the intake of meals prior to the examination, meaning that there may be precedent for patients to fast for a minimum of 150 min prior to examination [62]. Furthermore, due to the limited availability of CAP and lack of head-to-head studies with a US, conventional US remains the recommended first-line diagnostic tool for NAFLD [53].
4.3. MRI Methods
MRI methods, including magnetic resonance spectroscopy (MRS), provide a means to diagnose steatosis quantitatively. These methods have high diagnostic accuracy, including for low-grade steatosis (5–33%), and have low interobserver variability compared with other imaging modalities [58,63,64,65]. However, a high cost and limited availability mean they are not widely used for diagnosing steatosis in routine clinical care [22]. The guidelines state that MRI and MRS are more suitable in clinical research and trial settings [9,22,53,54].
4.4. Noninvasive Scores
Several noninvasive scores composed of clinical and laboratory parameters have been developed for predicting steatosis; examples include the SteatoTest™, the fatty liver index, the hepatic steatosis index, the lipid accumulation product index, and the NAFLD liver fat score (see review [66]). However, these scores are not recommended by the guidelines for diagnosing NAFLD due to their limited accuracy and availability, and, thus, their discussion is beyond the scope of this review [9,22,53,54].
Case Study. Assessment history: You receive notes from 2 years ago from the patient’s previous physician (Figure 1), as follows:
- Previous values: Age: 38, BMI: 27.0 kg/m2, waist circumference: 38 inches, blood pressure: 136/87 mmHg, and consuming 7 units of alcohol per week;
- −
- Current values: Age: 40, BMI: 32.3 kg/m2, waist circumference: 42 inches, blood pressure: 138/86 mmHg, and consuming 7 units of alcohol per week;
- Previous values: Cholesterol: 105 mg/dL, triglyceride: 32 mg/dL, and HDL-cholesterol: 22 mg/dL;
- −
- Current values: Cholesterol: 210 mg/dL, triglyceride: 174 mg/dL, HDL-cholesterol: 31 mg/dL, and LDL-cholesterol: 144 mg/dL;
- Previous values: ALT: 28 U/L and AST: 24 U/L;
- −
- Current values: ALT: 54 U/L, AST: 44 U/L, and platelets: 220 K.
You note that the patient must have undergone substantial weight gain (~5 BMI units) alongside the recent onset of abnormal aminotransferases.
Approach 1
Presuming a diagnosis of NAFLD, you offer options for weight loss and recommend that they reduce their intake of refined sugar and alcohol and try to cut caloric intake in general in order to help aid weight loss.
Approach 2
In line with the current and previous results, you screen the patient for cardiovascular risk and liver disease (Figure 1), with the following results:
- Atherosclerotic cardiovascular disease (ASCVD) risk score: 2.8%, with a 10-year risk of an ASCVD event;
- Negative viral hepatitis B and C testing;
- Liver ultrasound (US) demonstrating hepatic steatosis;
- Fibrosis-4 (Fib-4): 1.09 (low risk).
You diagnose the patient with NAFLD, provide options for weight loss, and recommend that they reduce their intake of sugar and alcohol.
5. Interventions: What Are the Options?
Once NAFLD is diagnosed, the care interventions include prescriptions for weight loss, cardiovascular risk management, advanced fibrosis risk assessments, and referral to a hepatologist.
5.1. Weight-Loss Interventions
Lifestyle interventions aimed at weight loss are key to the management of NAFLD (Figure 2) and fall under the following two main categories: increased physical activity and diet. Increasing physical activity on its own, including both aerobic and resistance exercise, can reduce liver fat content [67,68]. The benefits of exercise on liver fat content are more pronounced the higher an individual’s BMI [69]. Even in the absence of weight loss or dietary changes, exercise has been shown to reduce liver fat content, markers of liver disease (ALT and AST), and lipid levels [69,70,71,72,73]. Exercise is, therefore, a key recommended intervention in NAFLD [9,21,49,74], with 30–60 min of activity three to four times per week having been shown to improve liver fat content [74]. However, exercise alone seldom leads to sustained weight loss, and many people are not able to sustain large elevations in activity levels [75]. That said, even modest sustained increases in activity levels offer some benefits, as noted above, and may help to prevent weight regain after diet-induced weight loss. It can also be easier for some individuals to be more active following weight loss.
Dietary intervention is an important care intervention in NAFLD [9,21,49,74] and, combined with exercise, may be more effective in reducing liver fat content than exercise alone [70]. Hypocaloric diets and the Mediterranean diet have been shown to improve liver fat content and levels of aminotransferase and inflammatory markers [76,77,78]. As dietary changes are one of the key factors in preventing and reversing NAFLD, this is an area where physicians should support their patients by offering a range of options. Often, trial and error may be needed to find the optimal dietary changes for an individual patient. Discussing the variety of options available to patients is critical to devising a realistic management plan that is tailored to the patient’s needs and preferences, with numerous tools now at hand to help them to lose weight.
5.2. Cardiovascular Risk Management
The cardiovascular/metabolic risk factors for NAFLD include T2D, obesity, hypertension, and dyslipidemia [31]. In turn, patients with NAFLD are at an increased risk of cardiovascular events [79], including myocardial infarction, ischemic stroke, atrial fibrillation, heart failure, coronary artery disease, hypertension, and atherosclerosis [80,81], compared to patients without NAFLD. Moreover, patients with NAFLD with T2D, obesity, hypertension, and dyslipidemia are at an increased risk of advanced liver fibrosis, NASH, cirrhosis, and liver-related and overall mortality [13,14,15,16]. Hence, monitoring patients with NAFLD for cardiovascular risk factors and events is important (Figure 2). A tight association has been identified between NAFLD and T2D; as such, several anti-diabetic drugs, such as glucagon-like peptide-1 receptor agonists, thiazolidinedione insulin sensitizers, and sodium/glucose cotransporter-2 inhibitors, have been the subject of clinical trials for NAFLD and have shown potential for improving the outcomes in patients with NAFLD, both with and without comorbid T2D [82]. Various tools are available to physicians to calculate cardiovascular disease risk, such as the Atherosclerotic Cardiovascular Disease Risk Estimator Plus (ASCVD Risk Estimator; https://tools.acc.org/ascvd-risk-estimator-plus/#!/calculate/estimate/ (accessed on 25 March 2022)) and HeartScore (HeartScore®; https://www.heartscore.org/en_GB (accessed on 25 March 2022)) (Table 1). For managing patients at risk of cardiovascular disease, the guidelines recommend use of statins, as they do not present any safety issues in patients with NAFLD [9,21]. Finally, weight-loss interventions can also improve the cardiovascular risk profiles of patients with NAFLD [83,84].
Case Study. Six-month follow-up: Your patient returns six months later for a follow-up, having lost 8 kg with dietary changes and an alcohol reduction (Figure 1), as follows:
- BMI: 29.7 kg/m2, waist circumference: 39.5 inches, blood pressure: 126/78 mmHg, and consuming 3 units of alcohol per week;
- Cholesterol: 190 mg/dL, triglyceride: 158 mg/dL, HDL-cholesterol: 35 mg/dL, and LDL-cholesterol: 123 mg/dL;
- ALT: 32 U/L, AST: 30 U/L, and platelets: 225 K;
- HbA1c: 5.8%;
- Fib-4: 0.94 (low risk);
- ASCVD risk score: 1.6%, with a 10-year risk of an ASCVD event.
You congratulate your patient on their healthy lifestyle changes and encourage them to continue their healthy behaviors.
Case Study. Five years later.
Your patient returns after being lost to follow-up for 5 years (now age 45). During that time, they have gained 22 kg since their last visit (Figure 1), with the following results:
- BMI: 37.0 kg/m2, waist circumference: 44 inches, blood pressure: 151/88 mmHg, and consuming 10 units of alcohol per week;
- Cholesterol: 225 mg/dL, triglyceride: 220 mg/dL, HDL-cholesterol: 30 mg/dL, and LDL-cholesterol: 151 mg/dL;
- ALT: 64 U/L, AST: 60 U/L, and platelets: 165 K;
- HbA1c: 6.4%;
- Fib-4: 2.05 (indeterminate risk);
- ASCVD risk: 6.2%, with 10-year risk of an ASCVD event.
In this visit, you recognize the changes in the metabolic profile accompanying the increases in weight and alcohol intake. It is important to note the increased risk of advanced fibrosis by Fib-4 and the climbing ASCVD risk, as well as the increased risk of diabetes by the elevated HbA1c levels. You recommend weight loss with a range of evidence-based dietary options and a reduced alcohol intake. You order a confirmatory advanced fibrosis risk assessment with VCTE or consider whether to refer the patient to a hepatologist. You also note the raised blood pressure and make a note to check this again at the next follow-up, having recommended lifestyle changes including reducing their salt intake.
5.3. Fibrosis Risk Assessments
Advanced fibrosis is the main prognostic factor for liver-related morbidity and mortality in NAFLD and should, therefore, be assessed in a primary care setting once a diagnosis has been made (Figure 2) [30,34,35,36,37]. A liver biopsy remains as the gold standard for fibrosis assessment [9,22,53,54]; however, it is invasive, expensive, and shows variability in interpretation [9,22,54]. Thus, a liver biopsy is impractical in a primary care setting. Over the past two decades, noninvasive fibrosis risk assessments have emerged that can facilitate fibrosis risk prediction in primary care and identify patients who are in need of a referral to a hepatology specialist.
Noninvasive Scores for Fibrosis
Serologic Tests: Fibrosis-4 (Fib-4) Index and NAFLD Fibrosis Score (NFS). The Fib-4 index is a score that is calculated based on a patient’s age, aminotransferase levels (AST and ALT), and platelet count (Fibrosis-4 Score) [85] (Table 1), the latter of which can be obtained by performing a routine blood test [86]. Fib-4, therefore, represents a relatively-easy-to-implement score in a primary care setting (Box 3). It is validated for screening patients at risk of fibrosis and has a high negative predictive value in detecting advanced fibrosis in low-risk populations, meaning that it can accurately exclude advanced fibrosis [86,87,88,89].
NFS is another, slightly more complex, scoring system that is based on routinely collected demographic, clinical, and laboratory variables (such as age, BMI, presence of impaired fasting glycemia/diabetes, AST/ALT ratio, platelet count, and albumin levels) (NAFLD fibrosis score calculator (nafldscore.com (accessed on 1 December 2021)) [90] (Table 1). NFS is validated for diagnosing fibrosis stages and diagnosing/excluding advanced fibrosis in patients with NAFLD [90].
Several guidelines recommend using Fib-4 (Box 4) as the first-line noninvasive scoring system to screen for fibrosis in clinical practice [9,53,74,91,92], due to its low cost, wide availability, and ability to accurately exclude advanced fibrosis [93,94]. Meta-analyses show that Fib-4 and NFS outperform other commonly used noninvasive scores such as the AST/platelet ratio index and the BARD (BMI ≥ 28 = 1 point, AST/ALT ratio of ≥ 0.8 = 2 points, diabetes mellitus = 1 point) score in predicting fibrosis progression, liver-related events, and mortality [95,96]. The limitations of Fib-4 and NFS include low sensitivity, differing predictive probabilities, the risk of false positives, and reduced accuracy with increasing steatosis severity, patient age, obesity, and diabetes [88,97,98,99,100].
Box 3. When to check Fib-4 score.
Assessing for advanced fibrosis is a critical component of NAFLD management once the diagnosis has been made. Fib-4 is a high-performing, cheap, and easily accessible test based on readily available lab parameters and is the cornerstone of the most recent guidelines for NAFLD fibrosis risk assessment in clinical care [24]. The guidelines recommend reassessing Fib-4 scores every 2 to 3 years, including in low-risk patients [24,43]. Checking scores every year may help to identify patients who are at risk of advanced fibrosis/NASH earlier (Box 2); however, this would increase the cost and risk of false positives. Doctors should take a pragmatic approach and assess Fib-4 depending on patients’ progress. When, for example, weight loss is sustained and Fib-4 scores have previously declined, the need to repeat Fib-4 testing would be lower compared to an individual who has gained weight and had elevated Fib-4 scores in the past.
Serologic Test: Enhanced Liver Fibrosis (ELF™). The ELF™ test is a blood test that measures three markers of liver fibrosis (hyaluronic acid, procollagen III amino-terminal peptide, and the tissue inhibitor of matrix metalloproteinase 1), from which a score is computed [101]. The ELF™ test can accurately diagnose fibrosis stages [102,103,104]. In low-risk populations, it has a high negative predictive value but low positive predictive value in detecting advanced fibrosis, meaning that it can accurately exclude, but not diagnose, advanced fibrosis in low-prevalence settings [105]. The National Institute for Health and Care Excellence guidelines recommend using ELF™ to assess advanced liver fibrosis, citing its accuracy and cost-effectiveness [49,54]. However, ELF™ is not recommended by the American Association for the Study of Liver Diseases or the Asia–Pacific Working Party guidelines for clinical use, due to its limited availability [9,22]. The European Association for the Study of Liver (EASL) guidelines recommend its use but acknowledge this limitation [53].
Imaging: Vibration-controlled Transient Elastography (VCTE). VCTE using a controlled attenuation parameter measured with FibroScan® represents a US-based tool for assessing liver stiffness and, in turn, fibrosis. It is relatively quick (~10–20 min) and easy to perform by trained individuals, producing reliable and reproducible results that are immediately available [22,106,107,108]. VCTE is validated for diagnosing fibrosis stages, its diagnostic accuracy increases alongside fibrosis severity, and it can exclude advanced fibrosis [109,110,111]. For detecting the fibrosis stages, VCTE has shown a greater sensitivity than Fib-4 and NFS and a greater specificity than ELF™, but lower accuracy than MRI methods [87,96,102]. However, given the cost and limited availability of MRI methods, these are not recommended for first-line use in clinical practice [31]. VCTE is widely recommended for diagnosing/excluding advanced fibrosis in clinical practice [9,22,53]. According to the EASL Clinical Practice Guidelines, VCTE is recommended for diagnosing/excluding advanced fibrosis in patients with intermediate- and high-risk Fib-4 scores, with the EASL recommending a <8–10 kPa threshold for excluding advanced fibrosis [53]. The limitations of VCTE include uncertainty regarding cutoffs [22] and a reduced diagnostic accuracy in the lower fibrosis stages, in patients with obesity, and with limited operator experience [109,112]. It should also be noted that VCTE is primarily available to specialists, although a recent portable version has been developed for, and is available in, primary care [113].
Box 4. Fib-4 or NFS?
Fib-4 is more cost-effective than NFS for diagnosing advanced fibrosis [54,114]. Meta-analyses show NFS is more accurate in predicting the risk of mortality [115], while Fib-4 is more accurate in diagnosing fibrosis and fibrosis stages [116,117]. One meta-analysis found similar prognostic accuracies for Fib-4 and NFS in terms of liver-related events and mortality, but inconsistent accuracies for predicting the fibrosis stages [95]. Given the cost-effectiveness and diagnostic accuracy of Fib-4 compared with NFS, Fib-4 represents a valuable first-line noninvasive scoring method and has emerged as the preferred initial test for advanced fibrosis in recent guidelines [91,92].
5.4. Referral to a Hepatologist
If Fib-4, NFS, ELF™, or VCTE (if performed) suggest that the patient is at high risk of NAFLD with fibrosis (Table S1), the patient should be referred to a hepatologist (Figure 2) [24,43]. Hepatologists can then evaluate the need for additional assessments or a liver biopsy. In patients with noninvasive test results indicating a low risk for advanced fibrosis, the recent guidelines recommend repeating a Fib-4 assessment every 1–2 years in patients with type 2 diabetes, pre-diabetes, or ≥2 metabolic risk factors. These guidelines also recommend that all other patients with NAFLD have a repeat Fib-4 assessment every 2–3 years [91,92]. More evidence is needed to determine the optimal timing of repeat fibrosis assessments.
Case Study. Long-term prognosis: Your patient’s (vibration-controlled transient elastography) VCTE results come in, showing that they are at high risk for advanced fibrosis and, in turn, poor future outcomes (Figure 1), with the following result:
- VCTE: 9.9 kPa (high risk).
You refer your patient to a hepatologist and continue to reinforce weight loss and cardiovascular risk reduction as you co-manage this patient.
6. Conclusions
PCPs have various tools available at their fingertips for early diagnosis and management of NAFLD (a form of ectopic fat) in primary care settings. In this review, a diagnostic flow chart demonstrates the key points for assessment to identify NAFLD and those at risk. Suspecting and identifying NAFLD is important in developing a management plan, as this enables PCPs to better advocate the need for weight-loss interventions and address cardiovascular risk factors, if not previously carried out. In patients who are at high risk of advanced fibrosis, such as men or those with metabolic risk factors, or in those where NAFLD does not improve through lifestyle change, PCPs should perform advanced fibrosis risk assessments using noninvasive blood-based scores (Fib-4 or NFS) or other evidence-based scores (ELF™ or VCTE) to identify patients with elevated scores who are most in need of a referral to hepatologists for further investigation. Lifestyle modifications early on can improve patient outcomes and may mitigate disease progression, including for both NAFLD and cardiovascular conditions. As such, weight-loss interventions and increased awareness of NAFLD, as well as what risk patterns may constitute NAFLD, are key to identifying and then managing patients with NAFLD in primary care.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm12124001/s1, Table S1: Cutoff values for fibrosis assessments.
Author Contributions
Conceptualization, A.D.S. and N.S.; investigation, A.D.S. and N.S.; writing—original draft preparation, A.D.S. and N.S.; writing—review and editing, A.D.S. and N.S.; visualization, A.D.S. and N.S. All authors have read and agreed to the published version of the manuscript.
Funding
Medical writing support was funded by Pfizer Inc.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
Medical writing support, under the guidance of the authors, was provided by Sonya Frazier, CMC Connect, a division of IPG Health Medical Communications, and was funded by Pfizer Inc, New York, NY, USA, in accordance with Good Publication Practice (GPP 2022) guidelines. As noted at the beginning of this publication, the fictional case study included does not represent an actual patient case.
Conflicts of Interest
A.D.S. has no potential conflict of interest to disclose. N.S. has consulted for and/or received speaker honoraria from Abbott Laboratories, Afimmune, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Hanmi Pharmaceuticals, Janssen, Merck Sharp & Dohme, Novartis, Novo Nordisk, Pfizer, and Sanofi; and N.S.’s university has received grant funds for research from AstraZeneca, Boehringer Ingelheim, Novartis, and Roche Diagnostics.
References
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease—Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riazi, K.; Azhari, H.; Charette, J.H.; Underwood, F.E.; King, J.A.; Afshar, E.E.; Swain, M.G.; Congly, S.E.; Kaplan, G.G.; Shaheen, A.A. The prevalence and incidence of NAFLD worldwide: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2022, 7, 851–861. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.Z.; Dai, Y.N.; Wang, Y.M.; Zhou, Q.Y.; Yu, C.H.; Li, Y.M. Prevalence of nonalcoholic fatty liver disease and economy. Dig. Dis. Sci. 2015, 60, 3194–3202. [Google Scholar] [CrossRef]
- Le, M.H.; Yeo, Y.H.; Li, X.; Li, J.; Zou, B.; Wu, Y.; Ye, Q.; Huang, D.Q.; Zhao, C.; Zhang, J.; et al. 2019 global NAFLD prevalence: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2022, 20, 2809–2817. [Google Scholar] [CrossRef] [PubMed]
- Paik, J.M.; Golabi, P.; Younossi, Y.; Mishra, A.; Younossi, Z.M. Changes in the global burden of chronic liver diseases from 2012 to 2017: The growing impact of NAFLD. Hepatology 2020, 72, 1605–1616. [Google Scholar] [CrossRef]
- Global Burden of Disease Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Noureddin, M.; Vipani, A.; Bresee, C.; Todo, T.; Kim, I.K.; Alkhouri, N.; Setiawan, V.W.; Tran, T.; Ayoub, W.S.; Lu, S.C.; et al. NASH leading cause of liver transplant in women: Updated analysis of indications for liver transplant and ethnic and gender variances. Am. J. Gastroenterol. 2018, 113, 1649–1659. [Google Scholar] [CrossRef]
- Global Burden of Disease Cirrhosis Collaborators. The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 245–266. [Google Scholar] [CrossRef] [Green Version]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [Green Version]
- Cusi, K. Role of obesity and lipotoxicity in the development of nonalcoholic steatohepatitis: Pathophysiology and clinical implications. Gastroenterology 2012, 142, 711–725.e716. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J. Hepatol. 2019, 71, 793–801. [Google Scholar] [CrossRef]
- Singh, S.; Allen, A.M.; Wang, Z.; Prokop, L.J.; Murad, M.H.; Loomba, R. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: A systematic review and meta-analysis of paired-biopsy studies. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2015, 13, 643–654. [Google Scholar] [CrossRef] [Green Version]
- Yu, S.J.; Kim, W.; Kim, D.; Yoon, J.H.; Lee, K.; Kim, J.H.; Cho, E.J.; Lee, J.H.; Kim, H.Y.; Kim, Y.J.; et al. Visceral obesity predicts significant fibrosis in patients with nonalcoholic fatty liver disease. Medicine 2015, 94, e2159. [Google Scholar] [CrossRef] [PubMed]
- Stepanova, M.; Rafiq, N.; Makhlouf, H.; Agrawal, R.; Kaur, I.; Younoszai, Z.; McCullough, A.; Goodman, Z.; Younossi, Z.M. Predictors of all-cause mortality and liver-related mortality in patients with non-alcoholic fatty liver disease (NAFLD). Dig. Dis. Sci. 2013, 58, 3017–3023. [Google Scholar] [CrossRef] [PubMed]
- Stepanova, M.; Rafiq, N.; Younossi, Z.M. Components of metabolic syndrome are independent predictors of mortality in patients with chronic liver disease: A population-based study. Gut 2010, 59, 1410–1415. [Google Scholar] [CrossRef]
- Mendez-Sanchez, N.; Cerda-Reyes, E.; Higuera-de-la-Tijera, F.; Salas-Garcia, A.K.; Cabrera-Palma, S.; Cabrera-Alvarez, G.; Cortez-Hernandez, C.; Perez-Arredondo, L.A.; Puron-Gonzalez, E.; Coronado-Alejandro, E.; et al. Dyslipidemia as a risk factor for liver fibrosis progression in a multicentric population with non-alcoholic steatohepatitis. F1000Res 2020, 9, 56. [Google Scholar] [CrossRef] [Green Version]
- Jarvis, H.; Craig, D.; Barker, R.; Spiers, G.; Stow, D.; Anstee, Q.M.; Hanratty, B. Metabolic risk factors and incident advanced liver disease in non-alcoholic fatty liver disease (NAFLD): A systematic review and meta-analysis of population-based observational studies. PLoS Med. 2020, 17, e1003100. [Google Scholar] [CrossRef] [PubMed]
- Alexander, M.; Loomis, A.K.; Fairburn-Beech, J.; van der Lei, J.; Duarte-Salles, T.; Prieto-Alhambra, D.; Ansell, D.; Pasqua, A.; Lapi, F.; Rijnbeek, P.; et al. Real-world data reveal a diagnostic gap in non-alcoholic fatty liver disease. BMC Med. 2018, 16, 130. [Google Scholar] [CrossRef]
- Loomba, R.; Wong, R.; Fraysse, J.; Shreay, S.; Li, S.; Harrison, S.; Gordon, S.C. Nonalcoholic fatty liver disease progression rates to cirrhosis and progression of cirrhosis to decompensation and mortality: A real world analysis of Medicare data. Aliment. Pharm. 2020, 51, 1149–1159. [Google Scholar] [CrossRef]
- Nielsen, E.M.; Anderson, K.P.; Marsden, J.; Zhang, J.; Schreiner, A.D. Nonalcoholic fatty liver disease underdiagnosis in primary care: What are we missing? J. Gen. Intern. Med. 2022, 37, 2587–2590. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO clinical practice guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Wong, V.W.; Chan, W.K.; Chitturi, S.; Chawla, Y.; Dan, Y.Y.; Duseja, A.; Fan, J.; Goh, K.L.; Hamaguchi, M.; Hashimoto, E.; et al. Asia-Pacific Working Party on non-alcoholic fatty liver disease guidelines 2017-part 1: Definition, risk factors and assessment. J. Gastroenterol. Hepatol. 2018, 33, 70–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, P.; Symonds, A.; Barritt, A.S., 4th. Therapy for nonalcoholic fatty liver disease: Current options and future directions. Clin. 2021, 43, 500–517. [Google Scholar] [CrossRef]
- Kanwal, F.; Shubrook, J.H.; Adams, L.A.; Pfotenhauer, K.; Wong, V.W.; Wright, E.; Abdelmalek, M.F.; Harrison, S.A.; Loomba, R.; Mantzoros, C.S.; et al. Clinical care pathway for the risk stratification and management of patients with nonalcoholic fatty liver disease. Gastroenterology 2021, 161, 1657–1669. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Mark, H.E.; Villota-Rivas, M.; Palayew, A.; Carrieri, P.; Colombo, M.; Ekstedt, M.; Esmat, G.; George, J.; Marchesini, G.; et al. The global NAFLD policy review and preparedness index: Are countries ready to address this silent public health challenge? J. Hepatol. 2021, 76, 771–780. [Google Scholar] [CrossRef]
- Gracen, L.; Hayward, K.L.; Aikebuse, M.; Williams, S.; Russell, A.; O’Beirne, J.; Powell, E.E.; Valery, P.C. An exploration of barriers and facilitators to implementing a nonalcoholic fatty liver disease pathway for people with type 2 diabetes in primary care. Diabet. Med. 2022, 39, e14799. [Google Scholar] [CrossRef]
- Said, A.; Gagovic, V.; Malecki, K.; Givens, M.L.; Nieto, F.J. Primary care practitioners survey of non-alcoholic fatty liver disease. Ann. Hepatol. 2013, 12, 758–765. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: Update from the GBD 2019 study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Estes, C.; Anstee, Q.M.; Arias-Loste, M.T.; Bantel, H.; Bellentani, S.; Caballeria, J.; Colombo, M.; Craxi, A.; Crespo, J.; Day, C.P.; et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. J. Hepatol. 2018, 69, 896–904. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Makhlouf, H.R. Histology of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis in adults and children. Clin. Liver Dis. 2016, 20, 293–312. [Google Scholar] [CrossRef] [Green Version]
- Monelli, F.; Venturelli, F.; Bonilauri, L.; Manicardi, E.; Manicardi, V.; Rossi, P.; Massari, M.; Ligabue, G.; Riva, N.; Schianchi, S.; et al. Systematic review of existing guidelines for NAFLD assessment. Hepatoma Res. 2021, 7, 25. [Google Scholar] [CrossRef]
- Kanwal, F.; Kramer, J.R.; Li, L.; Dai, J.; Natarajan, Y.; Yu, X.; Asch, S.M.; El-Serag, H.B. Effect of metabolic traits on the risk of cirrhosis and hepatocellular cancer in nonalcoholic fatty liver disease. Hepatology 2020, 71, 808–819. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N.; McGuire, D.K.; Gill, J.M.R. High circulating triglycerides are most commonly a marker of ectopic fat accumulation: Connecting the clues to advance lifestyle interventions. Circulation 2022, 146, 77–79. [Google Scholar] [CrossRef] [PubMed]
- Angulo, P.; Kleiner, D.E.; Dam-Larsen, S.; Adams, L.A.; Bjornsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Keach, J.C.; Lafferty, H.D.; Stahler, A.; et al. Liver fibrosis, but no other histologic features, is associated with long-term outcomes of patients with nonalcoholic fatty liver disease. Gastroenterology 2015, 149, 389–397.e310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treeprasertsuk, S.; Björnsson, E.; Enders, F.; Suwanwalaikorn, S.; Lindor, K.D. NAFLD fibrosis score: A prognostic predictor for mortality and liver complications among NAFLD patients. World J. Gastroenterol. 2013, 19, 1219–1229. [Google Scholar] [CrossRef]
- Hagström, H.; Nasr, P.; Ekstedt, M.; Hammar, U.; Stål, P.; Hultcrantz, R.; Kechagias, S. Fibrosis stage but not NASH predicts mortality and time to development of severe liver disease in biopsy-proven NAFLD. J. Hepatol. 2017, 67, 1265–1273. [Google Scholar] [CrossRef]
- Dulai, P.S.; Singh, S.; Patel, J.; Soni, M.; Prokop, L.J.; Younossi, Z.; Sebastiani, G.; Ekstedt, M.; Hagstrom, H.; Nasr, P.; et al. Increased risk of mortality by fibrosis stage in nonalcoholic fatty liver disease: Systematic review and meta-analysis. Hepatology 2017, 65, 1557–1565. [Google Scholar] [CrossRef] [Green Version]
- Eslam, M.; Sanyal, A.J.; George, J. MAFLD: A consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology 2020, 158, 1999–2014.e1. [Google Scholar] [CrossRef]
- Tsochatzis, E.A.; Newsome, P.N. Non-alcoholic fatty liver disease and the interface between primary and secondary care. Lancet Gastroenterol. Hepatol. 2018, 3, 509–517. [Google Scholar] [CrossRef]
- Sattar, N.; Forrest, E.; Preiss, D. Non-alcoholic fatty liver disease. BMJ 2014, 349, g4596. [Google Scholar] [CrossRef]
- Armstrong, M.J.; Houlihan, D.D.; Bentham, L.; Shaw, J.C.; Cramb, R.; Olliff, S.; Gill, P.S.; Neuberger, J.M.; Lilford, R.J.; Newsome, P.N. Presence and severity of non-alcoholic fatty liver disease in a large prospective primary care cohort. J. Hepatol. 2012, 56, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Skelly, M.M.; James, P.D.; Ryder, S.D. Findings on liver biopsy to investigate abnormal liver function tests in the absence of diagnostic serology. J. Hepatol. 2001, 35, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Newsome, P.N.; Cramb, R.; Davison, S.M.; Dillon, J.F.; Foulerton, M.; Godfrey, E.M.; Hall, R.; Harrower, U.; Hudson, M.; Langford, A.; et al. Guidelines on the management of abnormal liver blood tests. Gut 2018, 67, 6–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwo, P.Y.; Cohen, S.M.; Lim, J.K. ACG clinical guideline: Evaluation of abnormal liver chemistries. Am. J. Gastroenterol. 2017, 112, 18–35. [Google Scholar] [CrossRef]
- Tapper, E.B.; Sengupta, N.; Lai, M.; Horowitz, G. Understanding and reducing ceruloplasmin overuse with a decision support intervention for liver disaese evaluation. Am. J. Med. 2016, 129, 115.e17–115.e22. [Google Scholar] [CrossRef]
- Tapper, E.B.; Saini, S.D.; Sengupta, N. Extensive testing or focused testing of patients with elevated liver enzymes. J. Hepatol. 2017, 66, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Liu, S.; Zhang, J.; Dong, M.; Wang, Y.; Wang, M.; Xin, Y. Proportion of NAFLD patients with normal ALT value in overall NAFLD patients: A systematic review and meta-analysis. BMC Gastroenterol. 2020, 20, 10. [Google Scholar] [CrossRef] [Green Version]
- Wright, A.P.; Desai, A.P.; Bajpai, S.; King, L.Y.; Sahani, D.V.; Corey, K.E. Gaps in recognition and evaluation of incidentally identified hepatic steatosis. Dig. Dis. Sci. 2015, 60, 333–338. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence. Non-Alcoholic Fatty Liver Disease (NAFLD): Assessment and Management. Available online: https://www.nice.org.uk/guidance/ng49/chapter/Recommendations (accessed on 3 April 2023).
- American Diabetes Association Professional Practice Committee. 4. Comprehensive medical evaluation and assessment of comorbidities: Standards of medical care in diabetes—2022. Diabetes Care 2022, 45, S46–S59. [Google Scholar] [CrossRef]
- Atsawarungruangkit, A.; Laoveeravat, P.; Promrat, K. Machine learning models for predicting non-alcoholic fatty liver disease in the general United States population: NHANES database. World J. Hepatol. 2021, 13, 1417–1427. [Google Scholar] [CrossRef]
- Noureddin, M.; Ntanios, F.; Malhotra, D.; Hoover, K.; Emir, B.; McLeod, E.; Alkhouri, N. Predicting NAFLD prevalence in the United States using National Health and Nutrition Examination Survey 2017–2018 transient elastography data and application of machine learning. Hepatol. Commun. 2022, 6, 1537–1548. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL clinical practice guidelines on non-invasive tests for evaluation of liver disease severity and prognosis—2021 update. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Non-Alcoholic Fatty Liver Disease: Assessment and Management. Available online: https://www.nice.org.uk/guidance/ng49/evidence/full-guideline-pdf-2548213310 (accessed on 3 April 2023).
- Hernaez, R.; Lazo, M.; Bonekamp, S.; Kamel, I.; Brancati, F.L.; Guallar, E.; Clark, J.M. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: A meta-analysis. Hepatology 2011, 54, 1082–1090. [Google Scholar] [CrossRef] [Green Version]
- Bril, F.; Ortiz-Lopez, C.; Lomonaco, R.; Orsak, B.; Freckleton, M.; Chintapalli, K.; Hardies, J.; Lai, S.; Solano, F.; Tio, F.; et al. Clinical value of liver ultrasound for the diagnosis of nonalcoholic fatty liver disease in overweight and obese patients. Liver Int. 2015, 35, 2139–2146. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.K.; Johnson, L.A.; Germin, B.I.; Marcos, A. One hundred consecutive hepatic biopsies in the workup of living donors for right lobe liver transplantation. Liver Transpl. 2002, 8, 1114–1122. [Google Scholar] [CrossRef]
- Saadeh, S.; Younossi, Z.M.; Remer, E.M.; Gramlich, T.; Ong, J.P.; Hurley, M.; Mullen, K.D.; Cooper, J.N.; Sheridan, M.J. The utility of radiological imaging in nonalcoholic fatty liver disease. Gastroenterology 2002, 123, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Strauss, S.; Gavish, E.; Gottlieb, P.; Katsnelson, L. Interobserver and intraobserver variability in the sonographic assessment of fatty liver. AJR Am. J. Roentgenol. 2007, 189, W320–W323. [Google Scholar] [CrossRef]
- Mottin, C.C.; Moretto, M.; Padoin, A.V.; Swarowsky, A.M.; Toneto, M.G.; Glock, L.; Repetto, G. The role of ultrasound in the diagnosis of hepatic steatosis in morbidly obese patients. Obes. Surg. 2004, 14, 635–637. [Google Scholar] [CrossRef] [PubMed]
- Shen, F.; Zheng, R.-D.; Shi, J.-P.; Mi, Y.-Q.; Chen, G.-F.; Hu, X.; Liu, Y.-G.; Wang, X.-Y.; Pan, Q.; Chen, G.-Y.; et al. Impact of skin capsular distance on the performance of controlled attenuation parameter in patients with chronic liver disease. Liver Int. 2015, 35, 2392–2400. [Google Scholar] [CrossRef] [Green Version]
- Ratchatasettakul, K.; Rattanasiri, S.; Promson, K.; Sringam, P.; Sobhonslidsuk, A. The inverse effect of meal intake on controlled attenuation parameter and liver stiffness as assessed by transient elastography. BMC Gastroenterol. 2017, 17, 50. [Google Scholar] [CrossRef] [Green Version]
- Szczepaniak, L.S.; Nurenberg, P.; Leonard, D.; Browning, J.D.; Reingold, J.S.; Grundy, S.; Hobbs, H.H.; Dobbins, R.L. Magnetic resonance spectroscopy to measure hepatic triglyceride content: Prevalence of hepatic steatosis in the general population. Am. J. Physiol. Endocrinol. Metab. 2005, 288, e462–e468. [Google Scholar] [CrossRef] [Green Version]
- Noureddin, M.; Lam, J.; Peterson, M.R.; Middleton, M.; Hamilton, G.; Le, T.A.; Bettencourt, R.; Changchien, C.; Brenner, D.A.; Sirlin, C.; et al. Utility of magnetic resonance imaging versus histology for quantifying changes in liver fat in nonalcoholic fatty liver disease trials. Hepatology 2013, 58, 1930–1940. [Google Scholar] [CrossRef] [Green Version]
- Qu, Y.; Li, M.; Hamilton, G.; Zhang, Y.N.; Song, B. Diagnostic accuracy of hepatic proton density fat fraction measured by magnetic resonance imaging for the evaluation of liver steatosis with histology as reference standard: A meta-analysis. Eur. Radiol. 2019, 29, 5180–5189. [Google Scholar] [CrossRef] [PubMed]
- Stern, C.; Castera, L. Non-invasive diagnosis of hepatic steatosis. Hepatol. Int. 2017, 11, 70–78. [Google Scholar] [CrossRef]
- Hashida, R.; Kawaguchi, T.; Bekki, M.; Omoto, M.; Matsuse, H.; Nago, T.; Takano, Y.; Ueno, T.; Koga, H.; George, J.; et al. Aerobic vs. resistance exercise in non-alcoholic fatty liver disease: A systematic review. J. Hepatol. 2017, 66, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Sabag, A.; Barr, L.; Armour, M.; Armstrong, A.; Baker, C.J.; Twigg, S.M.; Chang, D.; Hackett, D.A.; Keating, S.E.; George, J.; et al. The effect of high-intensity interval training versus moderate-intensity continuous training on liver fat: A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2022, 107, 862–881. [Google Scholar] [CrossRef] [PubMed]
- Orci, L.A.; Gariani, K.; Oldani, G.; Delaune, V.; Morel, P.; Toso, C. Exercise-based interventions for nonalcoholic fatty liver disease: A meta-analysis and meta-regression. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2016, 14, 1398–1411. [Google Scholar] [CrossRef] [Green Version]
- Golabi, P.; Locklear, C.T.; Austin, P.; Afdhal, S.; Byrns, M.; Gerber, L.; Younossi, Z.M. Effectiveness of exercise in hepatic fat mobilization in non-alcoholic fatty liver disease: Systematic review. World J. Gastroenterol. 2016, 22, 6318–6327. [Google Scholar] [CrossRef]
- Babu, A.F.; Csader, S.; Lok, J.; Gómez-Gallego, C.; Hanhineva, K.; El-Nezami, H.; Schwab, U. Positive effects of exercise intervention without weight loss and dietary changes in NAFLD-related clinical parameters: A systematic review and meta-analysis. Nutrients 2021, 13, 3135. [Google Scholar] [CrossRef]
- Keating, S.E.; Hackett, D.A.; George, J.; Johnson, N.A. Exercise and non-alcoholic fatty liver disease: A systematic review and meta-analysis. J. Hepatol. 2012, 57, 157–166. [Google Scholar] [CrossRef]
- Baker, C.J.; Martinez-Huenchullan, S.F.; D’Souza, M.; Xu, Y.; Li, M.; Bi, Y.; Johnson, N.A.; Twigg, S.M. Effect of exercise on hepatic steatosis: Are benefits seen without dietary intervention? A systematic review and meta-analysis. J. Diabetes 2021, 13, 63–77. [Google Scholar] [CrossRef]
- Tokushige, K.; Ikejima, K.; Ono, M.; Eguchi, Y.; Kamada, Y.; Itoh, Y.; Akuta, N.; Yoneda, M.; Iwasa, M.; Yoneda, M.; et al. Evidence-based clinical practice guidelines for nonalcoholic fatty liver disease/nonalcoholic steatohepatitis 2020. Hepatol. Res. 2021, 51, 1013–1025. [Google Scholar] [CrossRef]
- Seagle, H.M.; Strain, G.W.; Makris, A.; Reeves, R.S.; American Dietetic Association. Position of the American Dietetic Association: Weight management. J. Am. Diet. Assoc. 2009, 109, 330–346. [Google Scholar] [CrossRef]
- Garcêz, L.S.; Avelar, C.R.; Fonseca, N.S.S.; Costa, P.R.F.; Lyra, A.C.; Cunha, C.M.; Jesus, R.P.; Oliveira, L.P.M. Effect of dietary carbohydrate and lipid modification on clinical and anthropometric parameters in nonalcoholic fatty liver disease: A systematic review and meta-analysis. Nutr. Rev. 2021, 79, 1321–1337. [Google Scholar] [CrossRef]
- Houttu, V.; Csader, S.; Nieuwdorp, M.; Holleboom, A.G.; Schwab, U. Dietary interventions in patients with non-alcoholic fatty liver disease: A systematic review and meta-analysis. Front. Nutr. 2021, 8, 716783. [Google Scholar] [CrossRef]
- Reddy, A.J.; George, E.S.; Roberts, S.K.; Tierney, A.C. Effect of dietary intervention, with or without co-interventions, on inflammatory markers in patients with nonalcoholic fatty liver disease: A systematic literature review. Nutr. Rev. 2019, 77, 765–786. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Csermely, A.; Petracca, G.; Beatrice, G.; Corey, K.E.; Simon, T.G.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: An updated systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 903–913. [Google Scholar] [CrossRef]
- Alon, L.; Corica, B.; Raparelli, V.; Cangemi, R.; Basili, S.; Proietti, M.; Romiti, G.F. Risk of cardiovascular events in patients with non-alcoholic fatty liver disease: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2022, 29, 938–946. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Wu, F.; Ding, Y.; Hou, J.; Bi, J.; Zhang, Z. Association of non-alcoholic fatty liver disease with major adverse cardiovascular events: A systematic review and meta-analysis. Sci. Rep. 2016, 6, 33386. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, D.; Finck, B.N. Emerging therapeutic approaches for the treatment of NAFLD and type 2 diabetes mellitus. Nat. Rev. Endocrinol. 2021, 17, 484–495. [Google Scholar] [CrossRef] [PubMed]
- Hallsworth, K.; Thoma, C.; Hollingsworth, K.G.; Cassidy, S.; Anstee, Q.M.; Day, C.P.; Trenell, M.I. Modified high-intensity interval training reduces liver fat and improves cardiac function in non-alcoholic fatty liver disease: A randomized controlled trial. Clin. Sci. 2015, 129, 1097–1105. [Google Scholar] [CrossRef]
- Gepner, Y.; Shelef, I.; Komy, O.; Cohen, N.; Schwarzfuchs, D.; Bril, N.; Rein, M.; Serfaty, D.; Kenigsbuch, S.; Zelicha, H.; et al. The beneficial effects of Mediterranean diet over low-fat diet may be mediated by decreasing hepatic fat content. J. Hepatol. 2019, 71, 379–388. [Google Scholar] [CrossRef] [Green Version]
- GIHep. Fibrosis 4 Score. Available online: http://gihep.com/calculators/hepatology/fibrosis-4-score/ (accessed on 3 April 2023).
- Halfon, P.; Ansaldi, C.; Penaranda, G.; Chiche, L.; Dukan, P.; Stavris, C.; Plauzolles, A.; Retornaz, F.; Bourliere, M. Prospective screening of liver fibrosis in a primary care cohort using systematic calculation of fib-4 in routine results. PLoS ONE 2021, 16, e0254939. [Google Scholar] [CrossRef] [PubMed]
- Mózes, F.E.; Lee, J.A.; Selvaraj, E.A.; Jayaswal, A.N.A.; Trauner, M.; Boursier, J.; Fournier, C.; Staufer, K.; Stauber, R.E.; Bugianesi, E.; et al. Diagnostic accuracy of non-invasive tests for advanced fibrosis in patients with NAFLD: An individual patient data meta-analysis. Gut 2022, 71, 1006–1019. [Google Scholar] [CrossRef] [PubMed]
- Mahady, S.E.; Macaskill, P.; Craig, J.C.; Wong, G.L.H.; Chu, W.C.W.; Chan, H.L.Y.; George, J.; Wong, V.W. Diagnostic accuracy of noninvasive fibrosis scores in a population of individuals with a low prevalence of fibrosis. Clin. Gastroenterol. Hepatol. 2017, 15, 1453–1460.E1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peleg, N.; Issachar, A.; Sneh-Arbib, O.; Shlomai, A. AST to platelet ratio index and fibrosis 4 calculator scores for non-invasive assessment of hepatic fibrosis in patients with non-alcoholic fatty liver disease. Dig. Liver Dis. 2017, 49, 1133–1138. [Google Scholar] [CrossRef]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Rinella, M.E.; Neuschwander-Tetri, B.A.; Siddiqui, M.S.; Abdelmalek, M.F.; Caldwell, S.; Barb, D.; Kleiner, D.E.; Loomba, R. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology 2023, 77, 1797–1835. [Google Scholar] [CrossRef]
- Tincopa, M.A.; Loomba, R. Non-invasive diagnosis and monitoring of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis. Lancet Gastroenterol. Hepatol. 2023. [Google Scholar] [CrossRef]
- Castéra, L.; Friedrich-Rust, M.; Loomba, R. Noninvasive assessment of liver disease in patients with nonalcoholic fatty liver disease. Gastroenterology 2019, 156, 1264–1281.E4. [Google Scholar] [CrossRef] [Green Version]
- Cox, B.; Trasolini, R.; Galts, C.; Yoshida, E.M.; Marquez, V. Comparing the performance of Fibrosis-4 and Non-Alcoholic Fatty Liver Disease Fibrosis Score with transient elastography scores of people with non-alcoholic fatty liver disease. Can. Liver J. 2021, 4, 275–282. [Google Scholar] [CrossRef]
- Lee, J.; Vali, Y.; Boursier, J.; Spijker, R.; Anstee, Q.M.; Bossuyt, P.M.; Zafarmand, M.H. Prognostic accuracy of FIB-4, NAFLD fibrosis score and APRI for NAFLD-related events: A systematic review. Liver Int. 2021, 41, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Xiao, G.; Zhu, S.; Xiao, X.; Yan, L.; Yang, J.; Wu, G. Comparison of laboratory tests, ultrasound, or magnetic resonance elastography to detect fibrosis in patients with nonalcoholic fatty liver disease: A meta-analysis. Hepatology 2017, 66, 1486–1501. [Google Scholar] [CrossRef] [Green Version]
- McPherson, S.; Hardy, T.; Dufour, J.F.; Petta, S.; Romero-Gomez, M.; Allison, M.; Oliveira, C.P.; Francque, S.; Van Gaal, L.; Schattenberg, J.M.; et al. Age as a confounding factor for the accurate non-invasive diagnosis of advanced NAFLD fibrosis. Am. J. Gastroenterol. 2017, 112, 740–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertot, L.C.; Jeffrey, G.P.; de Boer, B.; MacQuillan, G.; Garas, G.; Chin, J.; Huang, Y.; Adams, L.A. Diabetes impacts prediction of cirrhosis and prognosis by non-invasive fibrosis models in non-alcoholic fatty liver disease. Liver Int. 2018, 38, 1793–1802. [Google Scholar] [CrossRef]
- Petta, S.; Wong, V.W.; Bugianesi, E.; Fracanzani, A.L.; Cammà, C.; Hiriart, J.B.; Lai-Hung Wong, G.; Vergniol, J.; Wing-Hung Chan, A.; Giannetti, A.; et al. Impact of obesity and alanine aminotransferase levels on the diagnostic accuracy for advanced liver fibrosis of noninvasive tools in patients with nonalcoholic fatty liver disease. Am. J. Gastroenterol. 2019, 114, 916–928. [Google Scholar] [CrossRef]
- Joo, S.K.; Kim, W.; Kim, D.; Kim, J.H.; Oh, S.; Lee, K.L.; Chang, M.S.; Jung, Y.J.; So, Y.H.; Lee, M.S.; et al. Steatosis severity affects the diagnostic performances of noninvasive fibrosis tests in nonalcoholic fatty liver disease. Liver Int. 2018, 38, 331–341. [Google Scholar] [CrossRef]
- Siemens Healthineers. The Enhanced Liver Fibrosis (ELF) Blood Test: Literature Compendium Volume 1. Available online: https://www.siemens-healthineers.com/en-uk/laboratory-diagnostics/assays-by-diseases-conditions/liver-disease/elf-test (accessed on 3 April 2023).
- Xie, Q.; Zhou, X.; Huang, P.; Wei, J.; Wang, W.; Zheng, S. The performance of enhanced liver fibrosis (ELF) test for the staging of liver fibrosis: A meta-analysis. PLoS ONE 2014, 9, e92772. [Google Scholar] [CrossRef]
- Thiele, M.; Madsen, B.S.; Hansen, J.F.; Detlefsen, S.; Antonsen, S.; Krag, A. Accuracy of the enhanced liver fibrosis test vs. FibroTest, elastography, and indirect markers in detection of advanced fibrosis in patients with alcoholic liver disease. Gastroenterology 2018, 154, 1369–1379. [Google Scholar] [CrossRef] [Green Version]
- Polyzos, S.A.; Slavakis, A.; Koumerkeridis, G.; Katsinelos, P.; Kountouras, J. Noninvasive liver fibrosis tests in patients with nonalcoholic fatty liver disease: An external validation cohort. Horm. Metab. Res. 2019, 51, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Vali, Y.; Lee, J.; Boursier, J.; Spijker, R.; Löffler, J.; Verheij, J.; Brosnan, M.J.; Böcskei, Z.; Anstee, Q.M.; Bossuyt, P.M.; et al. Enhanced liver fibrosis test for the non-invasive diagnosis of fibrosis in patients with NAFLD: A systematic review and meta-analysis. J. Hepatol. 2020, 73, 252–262. [Google Scholar] [CrossRef] [PubMed]
- Vuppalanchi, R.; Siddiqui, M.S.; Van Natta, M.L.; Hallinan, E.; Brandman, D.; Kowdley, K.; Neuschwander-Tetri, B.A.; Loomba, R.; Dasarathy, S.; Abdelmalek, M.; et al. Performance characteristics of vibration-controlled transient elastography for evaluation of nonalcoholic fatty liver disease. Hepatology 2018, 67, 134–144. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence. FibroScan for Assessing Liver Fibrosis and Cirrhosis in Primary Care. Available online: https://www.nice.org.uk/advice/mib216/chapter/Expert-comments (accessed on 3 April 2023).
- Echosens. Fibroscan®. Available online: https://www.echosens.com/fibroscan/ (accessed on 3 April 2023).
- Eddowes, P.J.; Sasso, M.; Allison, M.; Tsochatzis, E.; Anstee, Q.M.; Sheridan, D.; Guha, I.N.; Cobbold, J.F.; Deeks, J.J.; Paradis, V.; et al. Accuracy of FibroScan controlled attenuation parameter and liver stiffness measurement in assessing steatosis and fibrosis in patients with nonalcoholic fatty liver disease. Gastroenterology 2019, 156, 1717–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siddiqui, M.S.; Vuppalanchi, R.; Van Natta, M.L.; Hallinan, E.; Kowdley, K.V.; Abdelmalek, M.; Neuschwander-Tetri, B.A.; Loomba, R.; Dasarathy, S.; Brandman, D.; et al. Vibration-controlled transient elastography to assess fibrosis and steatosis in patients with nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2019, 17, 156–163.e152. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, S.A.; Alavian, S.M.; Gholami-Fesharaki, M. Assessment of transient elastography (FibroScan) for diagnosis of fibrosis in non-alcoholic fatty liver disease: A systematic review and meta-analysis. Casp. J. Intern. Med. 2016, 7, 242–252. [Google Scholar]
- Castéra, L.; Foucher, J.; Bernard, P.H.; Carvalho, F.; Allaix, D.; Merrouche, W.; Couzigou, P.; de Lédinghen, V. Pitfalls of liver stiffness measurement: A 5-year prospective study of 13,369 examinations. Hepatology 2010, 51, 828–835. [Google Scholar] [CrossRef]
- Echosens. New FibroScan® GO. Available online: https://www.flipsnack.com/98A8B8AA9F7/fibroscan-go_brochure-uk_web.html (accessed on 3 April 2023).
- Congly, S.E.; Shaheen, A.A.; Swain, M.G. Modelling the cost effectiveness of non-alcoholic fatty liver disease risk stratification strategies in the community setting. PLoS ONE 2021, 16, e0251741. [Google Scholar] [CrossRef]
- Salomone, F.; Micek, A.; Godos, J. Simple scores of fibrosis and mortality in patients with NAFLD: A systematic review with meta-analysis. J. Clin. Med. 2018, 7, 219. [Google Scholar] [CrossRef] [Green Version]
- Sun, W.; Cui, H.; Li, N.; Wei, Y.; Lai, S.; Yang, Y.; Yin, X.; Chen, D.F. Comparison of FIB-4 index, NAFLD fibrosis score and BARD score for prediction of advanced fibrosis in adult patients with non-alcoholic fatty liver disease: A meta-analysis study. Hepatol. Res. 2016, 46, 862–870. [Google Scholar] [CrossRef]
- Ismaiel, A.; Leucuta, D.C.; Popa, S.L.; Fagoonee, S.; Pellicano, R.; Abenavoli, L.; Dumitrascu, D.L. Noninvasive biomarkers in predicting nonalcoholic steatohepatitis and assessing liver fibrosis: Systematic review and meta-analysis. Panminerva Med. 2021, 63, 508–518. [Google Scholar] [CrossRef]
Figure 1.
Longitudinal case study of a patient with NAFLD. ALT, alanine aminotransferase; ASCVD, atherosclerotic cardiovascular disease; AST, aspartate aminotransferase; BMI, body mass index; BP, blood pressure; Fib-4, Fibrosis-4; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TG, triglyceride; VCTE, vibration-controlled transient elastography; WC, waist circumference.
Figure 1.
Longitudinal case study of a patient with NAFLD. ALT, alanine aminotransferase; ASCVD, atherosclerotic cardiovascular disease; AST, aspartate aminotransferase; BMI, body mass index; BP, blood pressure; Fib-4, Fibrosis-4; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TG, triglyceride; VCTE, vibration-controlled transient elastography; WC, waist circumference.

Figure 2.
Diagnostic flow chart of patients with NAFLD in primary care. ELF™, enhanced liver fibrosis; Fib-4, Fibrosis-4; LFT, liver function test; NAFLD, nonalcoholic fatty liver disease; NFS, NAFLD fibrosis score; VCTE, vibration-controlled transient elastography.
Figure 2.
Diagnostic flow chart of patients with NAFLD in primary care. ELF™, enhanced liver fibrosis; Fib-4, Fibrosis-4; LFT, liver function test; NAFLD, nonalcoholic fatty liver disease; NFS, NAFLD fibrosis score; VCTE, vibration-controlled transient elastography.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Risk and prediction models.
| Model | Risk/Prediction of Disease/Disease Stage | Predictors |
|---|---|---|
| ASCVD Risk Estimator | 10-year ASCVD risk intended for patients with LDL-cholesterol < 190 mg/dL (4.92 mmol/L), without ASCVD | Current age (years) |
| Sex (male/female) | ||
| Race (White/African American/other) | ||
| Systolic blood pressure (mmHg) | ||
| Diastolic blood pressure (mmHg) | ||
| Total cholesterol (mg/dL) | ||
| HDL-cholesterol (mg/dL) | ||
| LDL-cholesterol (mg/dL) | ||
| History of diabetes (yes/no) | ||
| Smoker (current/former/never) | ||
| On hypertension treatment (yes/no) | ||
| On a statin (yes/no) | ||
| On aspirin therapy (yes/no) | ||
| HeartScore® | 10-year risk of first-onset cardiovascular disease in European populations | Risk region (low risk/moderate risk/high risk/very high risk) |
| Age (years) | ||
| Sex (male/female) | ||
| Systolic blood pressure (mmHg) | ||
| Total cholesterol (mmol/L or mg/dL) | ||
| HDL-cholesterol (mmol/L) | ||
| Current smoker (yes/no) | ||
| Fibrosis-4 score | Prediction of liver fibrosis and cirrhosis | (Age (years) × AST (IU/L))/(Platelet count (109/L) × (square root (ALT (IU/L))) |
| NAFLD fibrosis score | Prediction of advanced fibrosis | −1.675 + 0.037 × age (years) + 0.094 × BMI (kg/m2) + 1.13 × IFG/diabetes (yes = 1, no = 0) + 0.99 × AST/ALT ratio − 0.013 × platelet (×109/L) − 0.66 × albumin (g/dL) |
ALT, alanine aminotransferase; ASCVD, atherosclerotic cardiovascular disease; AST, aspartate aminotransferase; BMI, body mass index; HDL, high-density lipoprotein; IFG, impaired fasting glucose; LDL, low-density lipoprotein.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Schreiner, A.D.; Sattar, N. Identifying Patients with Nonalcoholic Fatty Liver Disease in Primary Care: How and for What Benefit? J. Clin. Med. 2023, 12, 4001. https://doi.org/10.3390/jcm12124001
AMA Style
Schreiner AD, Sattar N. Identifying Patients with Nonalcoholic Fatty Liver Disease in Primary Care: How and for What Benefit? Journal of Clinical Medicine. 2023; 12(12):4001. https://doi.org/10.3390/jcm12124001
Chicago/Turabian StyleSchreiner, Andrew D., and Naveed Sattar. 2023. "Identifying Patients with Nonalcoholic Fatty Liver Disease in Primary Care: How and for What Benefit?" Journal of Clinical Medicine 12, no. 12: 4001. https://doi.org/10.3390/jcm12124001
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.