

Is It Necessary to Cross the Cervicothoracic Junction in Posterior Cervical Decompression and Fusion for Multilevel Degenerative Cervical Spine Disease? A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Assessment of Study Quality
2.4. Outcomes
2.5. Data Extraction
2.6. Data Analysis
2.7. Assessment of Publication Bias
3. Results
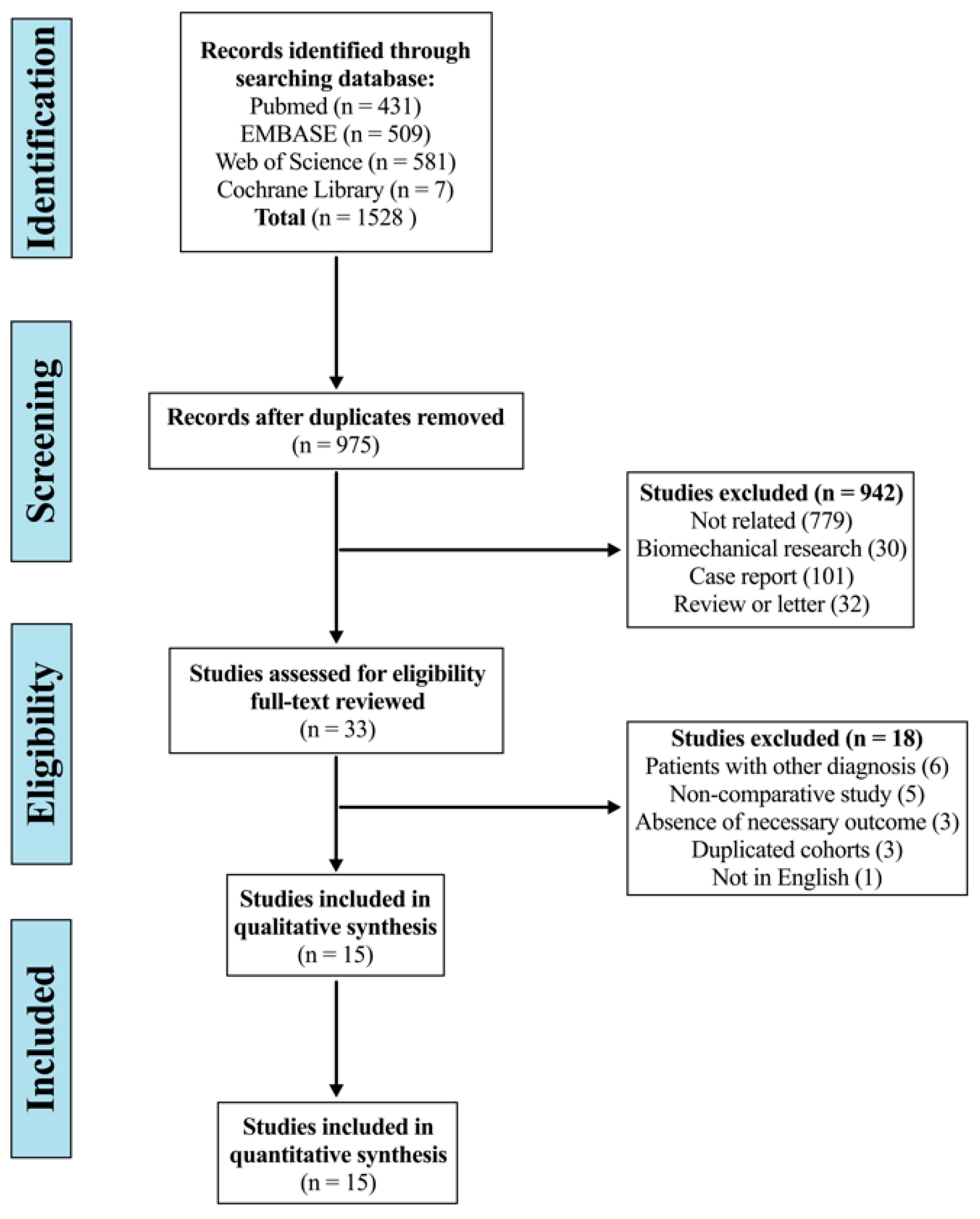
3.1. Study Selection
3.2. Assessment of Study Quality and Publication Bias
3.3. Characteristics of Included Studies
3.4. Mechanical Complications
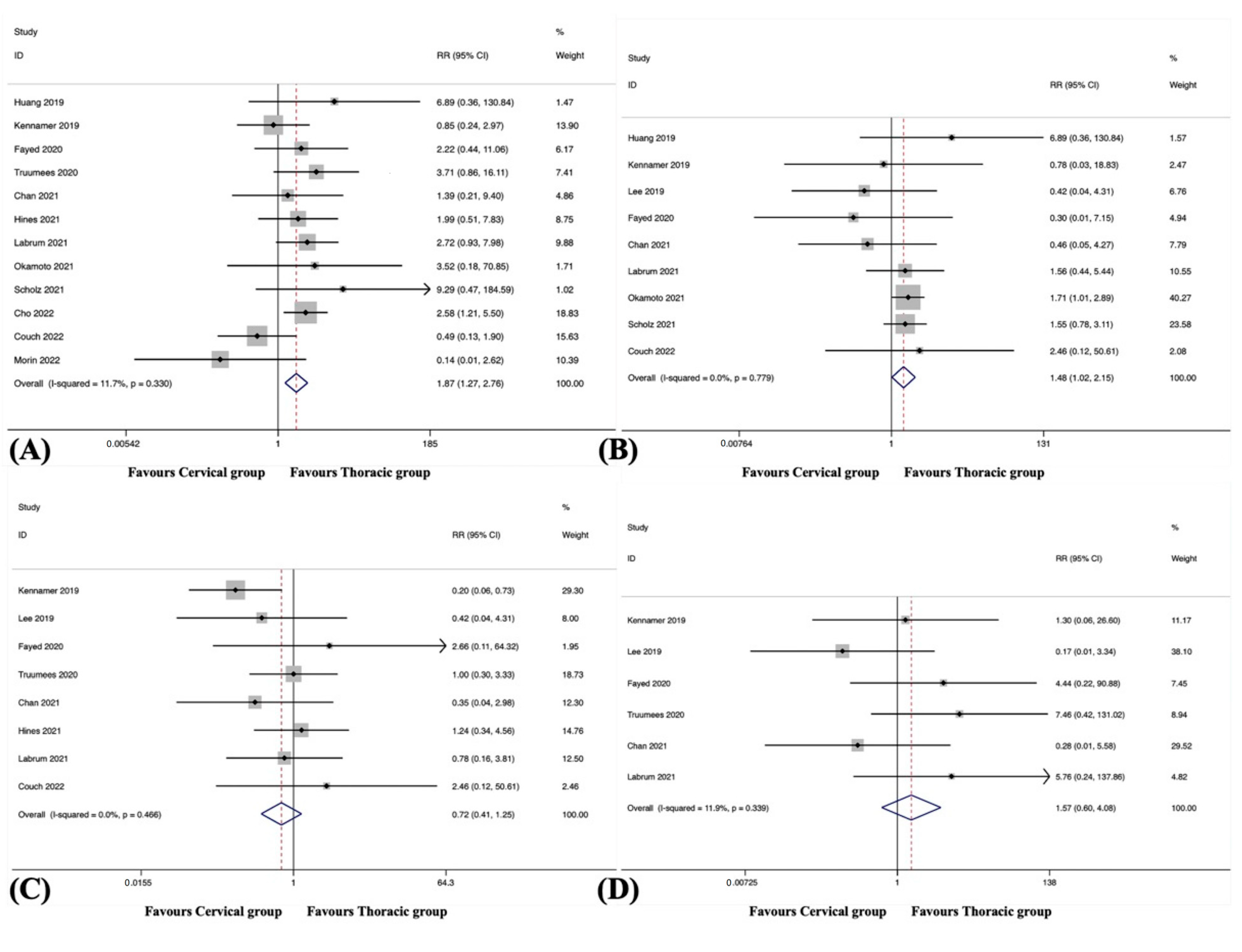
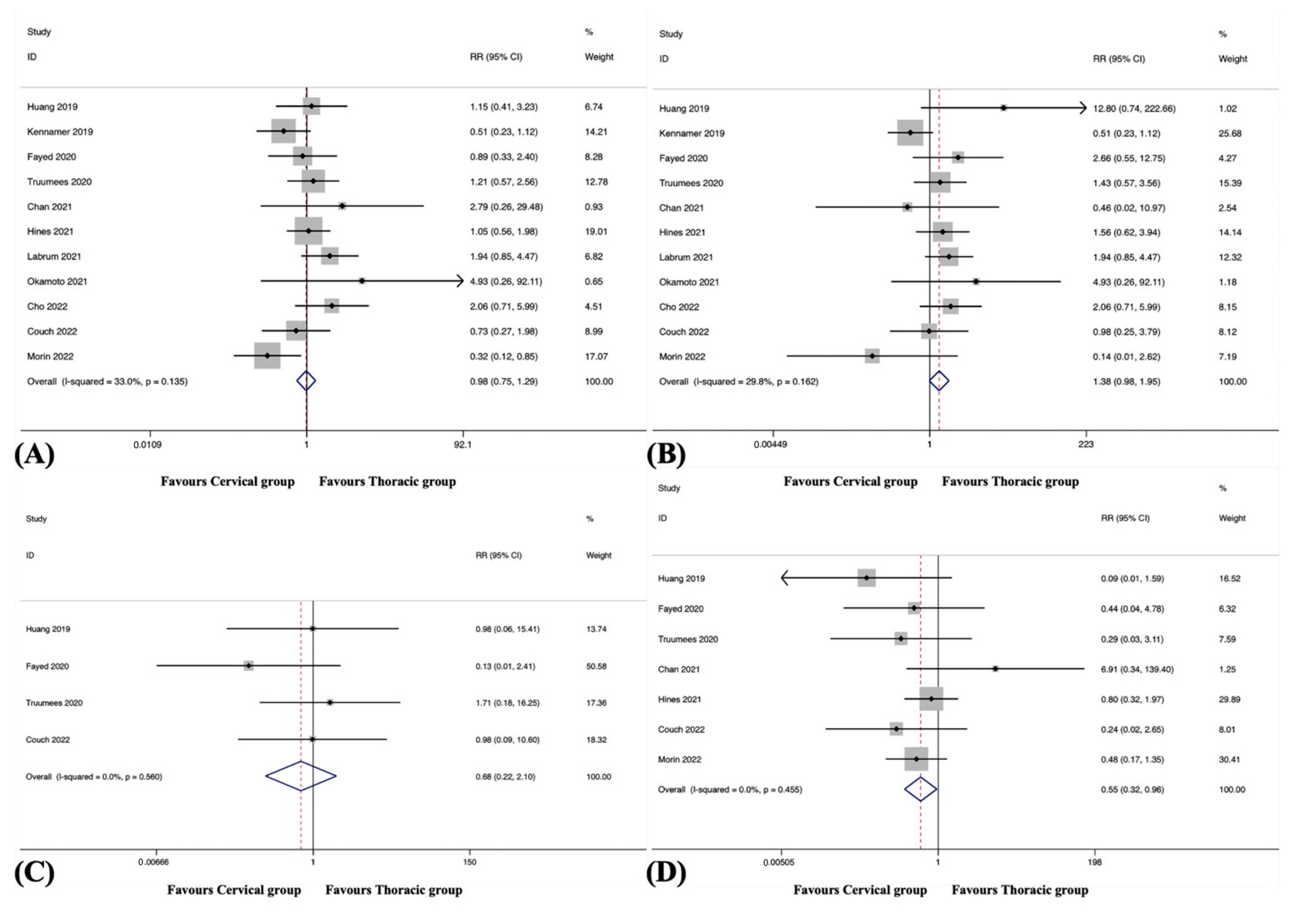
3.4.1. Overall Adjacent Segment Disease
3.4.2. Distal Adjacent Segment Disease
3.4.3. Proximal Adjacent Segment Disease
3.4.4. Overall Hardware Failure
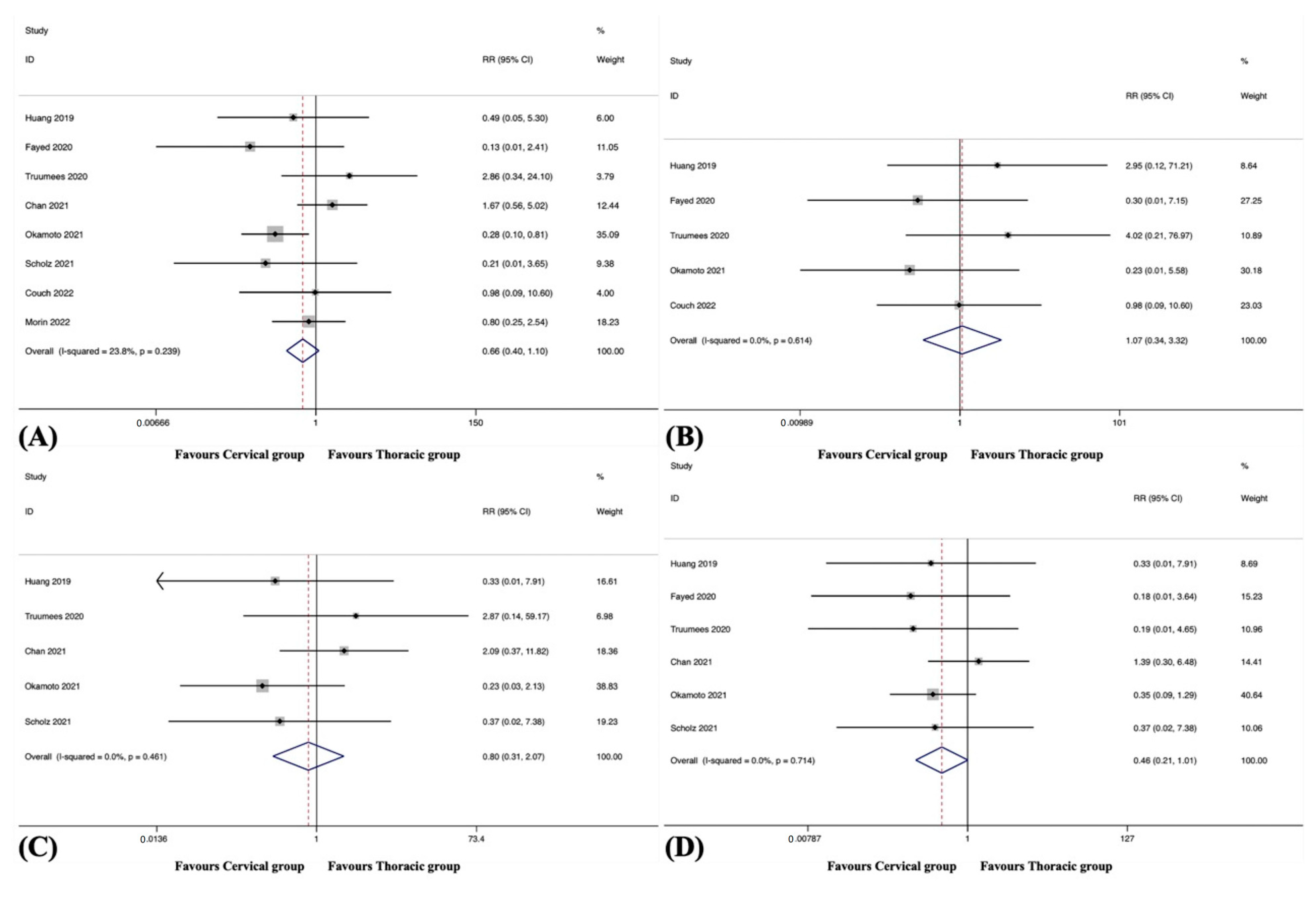
3.4.5. Hardware Failure of LIV
3.4.6. Pseudarthrosis
3.4.7. Distal Junctional Kyphosis
3.5. Surgical Complications
3.5.1. Overall
3.5.2. Epidural Haematoma
3.5.3. Dural Tears
3.5.4. Neurologic Deficits
3.5.5. Wound-Related Complications
3.5.6. Systemic Complications
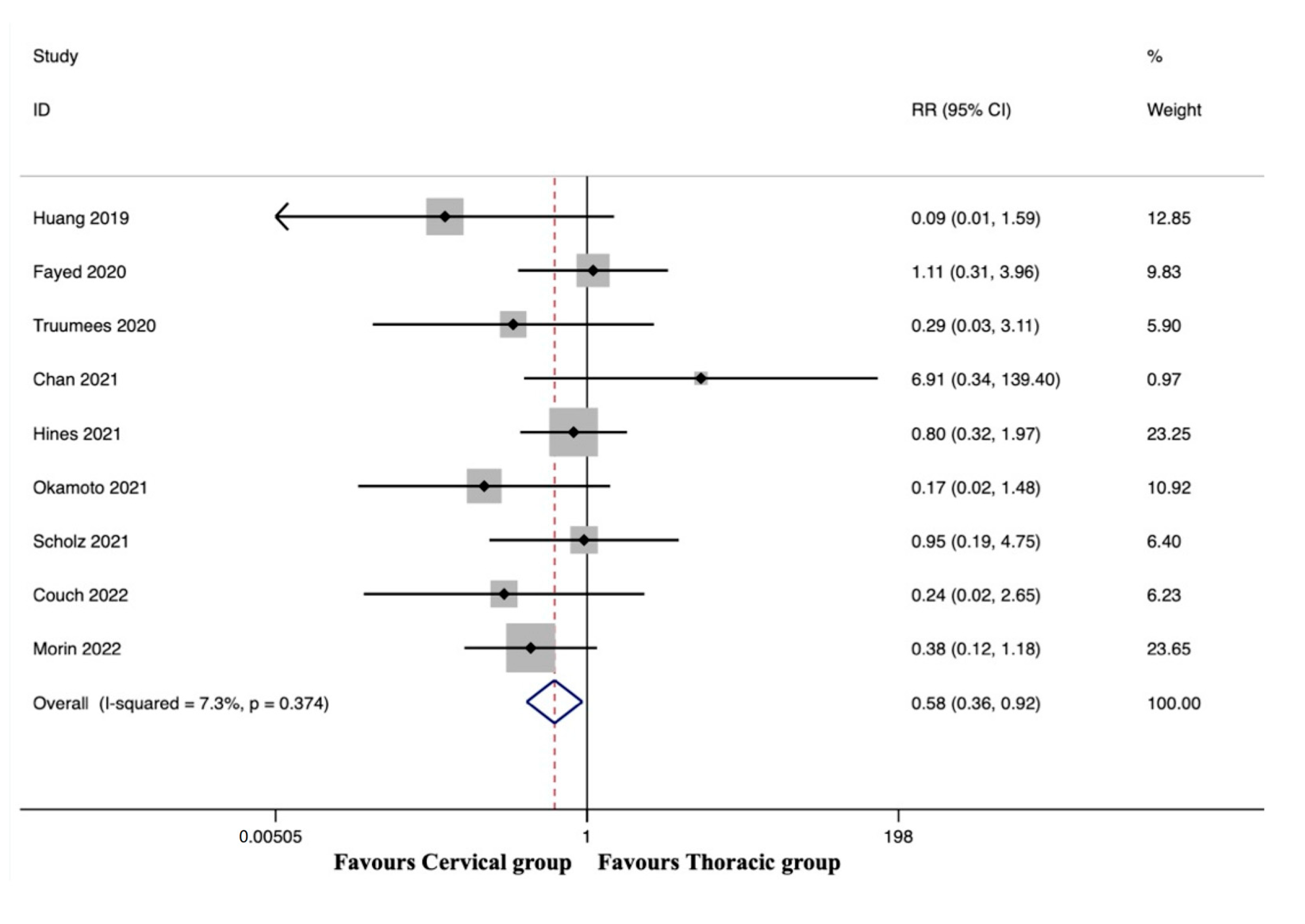
3.6. Reoperation
3.6.1. Overall
3.6.2. Reoperation Rate following Mechanical Complications
3.6.3. Reoperation Rate following Surgical Complications
3.6.4. Reoperation Rate following Wound-Related Complications
3.7. Surgical Data
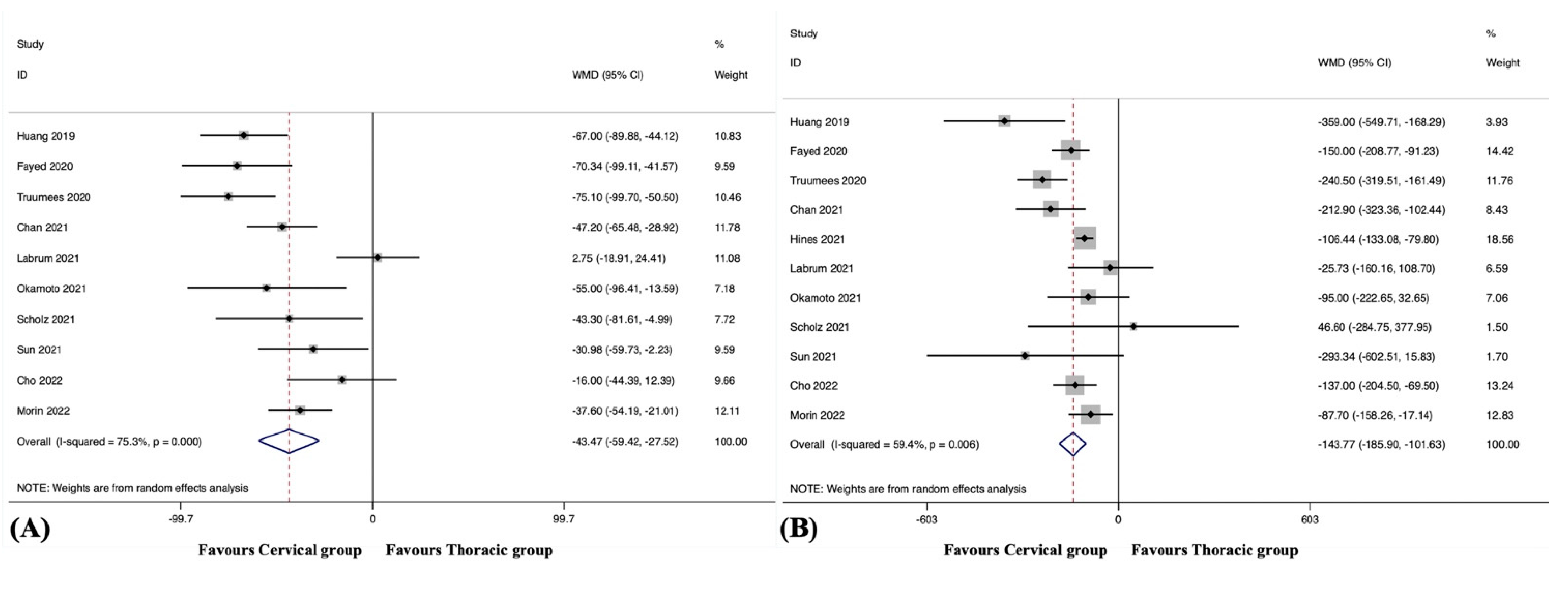
3.7.1. Operating Time
3.7.2. Estimated Blood Loss
3.7.3. Length of Hospital Stay
3.8. Patient-Reported Outcomes
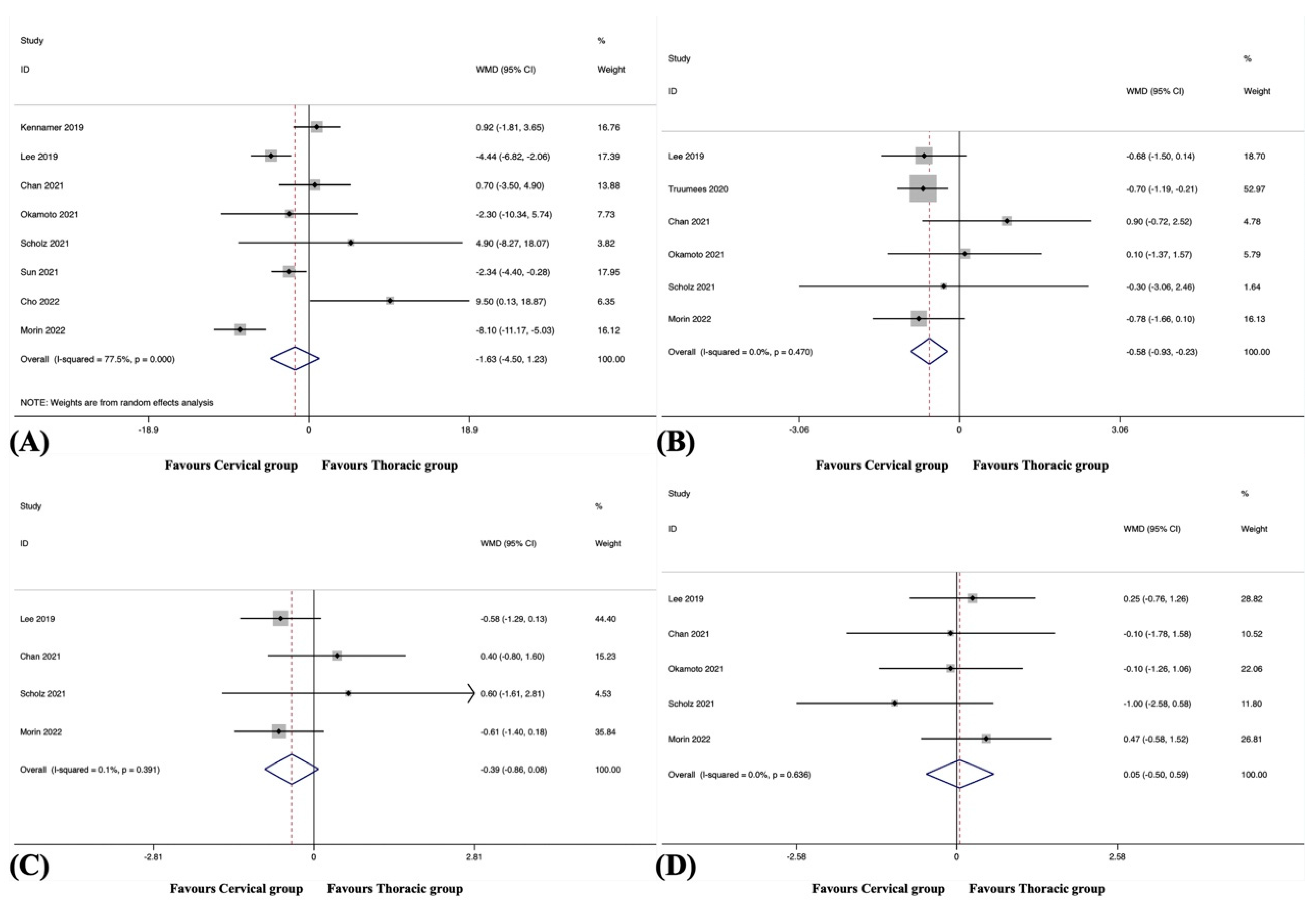
3.8.1. Neck Disability Index
3.8.2. Numeric Rating Scale for Neck Pain
3.8.3. Numeric Rating Scale for Arm Pain
3.8.4. Japanese Orthopaedic Association Score
3.9. Radiographic Outcome
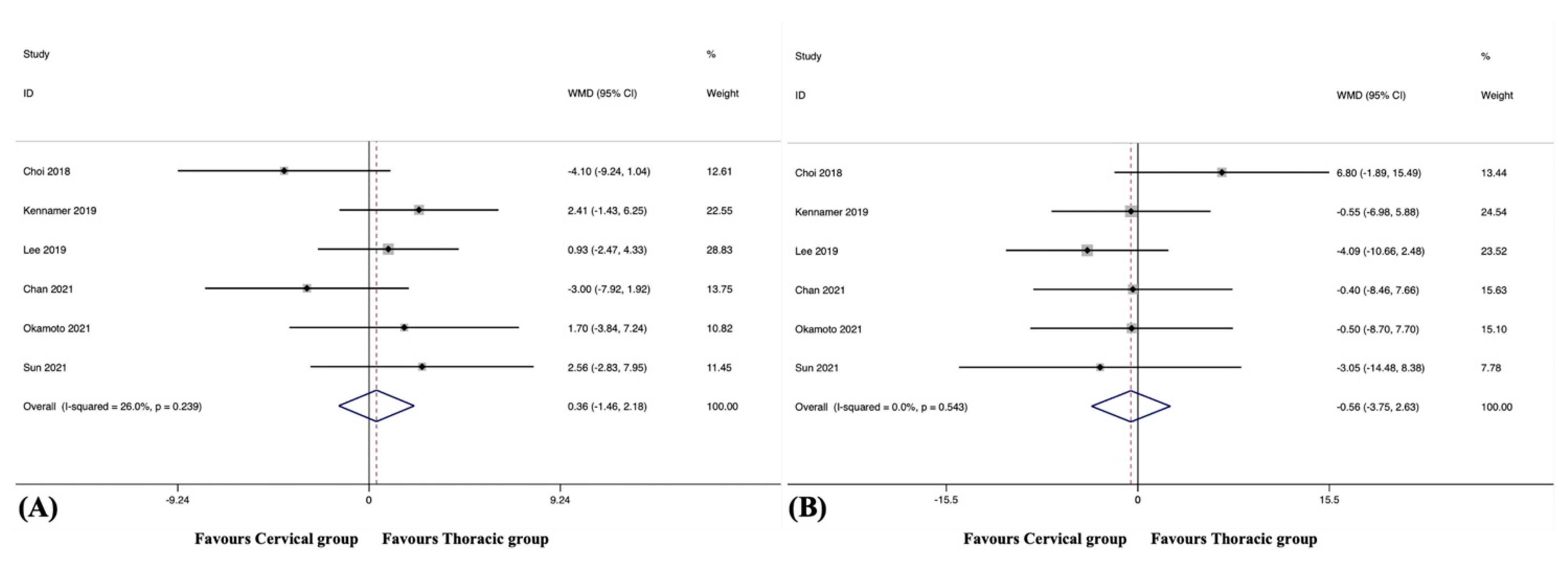
3.9.1. C2-7 Cervical Lordosis
3.9.2. C2-7 Cervical Sagittal Vertical Axis
3.9.3. T1 Slope
3.10. Subgroup Analysis
3.10.1. Subgroup Analysis Based on Surgical Techniques
3.10.2. Subgroup Analysis Based on Indications of Surgery
3.11. Sensitivity Analyses
3.12. Meta-Regression
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nouri, A.; Tetreault, L.; Singh, A.; Karadimas, S.K.; Fehlings, M.G. Degenerative Cervical Myelopathy: Epidemiology, Genetics, and Pathogenesis. Spine 2015, 40, E675–E693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iyer, S.; Kim, H.J. Cervical radiculopathy. Curr. Rev. Musculoskelet. Med. 2016, 9, 272–280. [Google Scholar] [CrossRef] [Green Version]
- Matsunaga, S.; Sakou, T. Ossification of the posterior longitudinal ligament of the cervical spine: Etiology and natural history. Spine 2012, 37, E309–E314. [Google Scholar] [CrossRef]
- Scheer, J.K.; Tang, J.A.; Smith, J.S.; Acosta, F.L., Jr.; Protopsaltis, T.S.; Blondel, B.; Bess, S.; Shaffrey, C.I.; Deviren, V.; Lafage, V.; et al. Cervical spine alignment, sagittal deformity, and clinical implications: A review. J. Neurosurg. Spine 2013, 19, 141–159. [Google Scholar] [CrossRef] [Green Version]
- Neifert, S.N.; Martini, M.L.; Yuk, F.; McNeill, I.T.; Caridi, J.M.; Steinberger, J.; Oermann, E.K. Predicting Trends in Cervical Spinal Surgery in the United States from 2020 to 2040. World Neurosurg. 2020, 141, e175–e181. [Google Scholar] [CrossRef]
- Youssef, J.A.; Heiner, A.D.; Montgomery, J.R.; Tender, G.C.; Lorio, M.P.; Morreale, J.M.; Phillips, F.M. Outcomes of posterior cervical fusion and decompression: A systematic review and meta-analysis. Spine J. 2019, 19, 1714–1729. [Google Scholar] [CrossRef] [Green Version]
- Wang, V.Y.; Chou, D. The cervicothoracic junction. Neurosurg. Clin. N. Am. 2007, 18, 365–371. [Google Scholar] [CrossRef]
- Steinmetz, M.P.; Miller, J.; Warbel, A.; Krishnaney, A.A.; Bingaman, W.; Benzel, E.C. Regional instability following cervicothoracic junction surgery. J. Neurosurg. Spine 2006, 4, 278–284. [Google Scholar] [CrossRef]
- Wu, D.Z.; Gu, Z.F.; Meng, D.J.; Hou, S.B.; Ren, L.; Sun, X.Z. Bridging the cervicothoracic junction during posterior cervical laminectomy and fusion for the treatment of multilevel cervical ossification of the posterior longitudinal ligament: A retrospective case series. BMC Musculoskelet. Disord. 2022, 23, 446. [Google Scholar] [CrossRef]
- Ibaseta, A.; Rahman, R.; Andrade, N.S.; Uzosike, A.C.; Byrapogu, V.K.; Ramji, A.F.; Skolasky, R.L.; Reidler, J.S.; Kebaish, K.M.; Riley, L.H., 3rd; et al. Crossing the Cervicothoracic Junction in Cervical Arthrodesis Results in Lower Rates of Adjacent Segment Disease Without Affecting Operative Risks or Patient-Reported Outcomes. Clin. Spine Surg. 2019, 32, 377–381. [Google Scholar] [CrossRef]
- Schroeder, G.D.; Kepler, C.K.; Kurd, M.F.; Mead, L.; Millhouse, P.W.; Kumar, P.; Nicholson, K.; Stawicki, C.; Helber, A.; Fasciano, D.; et al. Is It Necessary to Extend a Multilevel Posterior Cervical Decompression and Fusion to the Upper Thoracic Spine? Spine 2016, 41, 1845–1849. [Google Scholar] [CrossRef] [PubMed]
- Toci, G.R.; Karamian, B.A.; Lambrechts, M.J.; Mao, J.; Mandel, J.; Darrach, T.; Canseco, J.A.; Kaye, I.D.; Woods, B.I.; Rihn, J.; et al. Instrumentation Across the Cervicothoracic Junction Does Not Improve Patient-reported Outcomes in Multilevel Posterior Cervical Decompression and Fusion. Clin. Spine Surg. 2022, 35, E667–E673. [Google Scholar] [CrossRef] [PubMed]
- Guppy, K.H.; Royse, K.E.; Fennessy, J.; Norheim, E.P.; Harris, J.E.; Brara, H.S. No Difference in Reoperation Rates for Adjacent Segment Disease (Operative Adjacent Segment Disease) in Posterior Cervical Fusions Stopping at C7 Versus T1/T2: A Cohort of 875 Patients-Part 1. Spine 2022, 47, 261–268. [Google Scholar] [CrossRef]
- Guppy, K.H.; Royse, K.E.; Fennessy, J.H.; Norheim, E.P.; Harris, J.E.; Brara, H.S. No difference in reoperation rates for nonunions (operative nonunions) in posterior cervical fusions stopping at C7 versus T1/2: A cohort of 875 patients. J. Neurosurg. Spine 2021, 36, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A.; Akhras, A.; Wahood, W.; Alvi, M.A.; Nassr, A.; Bydon, M. Should Multilevel Posterior Cervical Fusions Involving C7 Cross the Cervicothoracic Junction? A Systematic Review and Meta-Analysis. World Neurosurg. 2019, 127, 588–595.e585. [Google Scholar] [CrossRef]
- Chang, M.C.; Kim, G.U.; Choo, Y.J.; Lee, G.W. To cross or not to cross the cervicothoracic junction in multilevel posterior cervical fusion: A systematic review and meta-analysis. Spine J. 2022, 22, 723–731. [Google Scholar] [CrossRef] [PubMed]
- Coban, D.; Faloon, M.; Changoor, S.; Saela, S.; Sahai, N.; Record, N.; Sinha, K.; Hwang, K.; Emami, A. Should we bridge the cervicothoracic junction in long cervical fusions? A meta-analysis and systematic review of the literature. J. Neurosurg. Spine 2022, 37, 166–174. [Google Scholar] [CrossRef]
- Truumees, E.; Singh, D.; Ennis, D.; Livingston, H.; Duncan, A.; Lavelle, W.; Riesenburger, R.; Yu, A.; Geck, M.; Mroz, T.; et al. Bridging the Cervicothoracic Junction During Multi-Level Posterior Cervical Decompression and Fusion: A Systematic Review and Meta-Analysis. Glob. Spine J. 2023, 13, 197–208. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Davies, S. The importance of PROSPERO to the National Institute for Health Research. Syst. Rev. 2012, 1, 5. [Google Scholar] [CrossRef] [Green Version]
- Wright, J.G.; Swiontkowski, M.F.; Heckman, J.D. Introducing levels of evidence to the journal. J. Bone Joint Surg. Am. 2003, 85, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.T.; Yi, J.S.; Kim, J.T.; Ji, C.; Ryu, K.S.; Park, C.K. Clinical and radiologic outcome of laminar screw at C2 and C7 for posterior instrumentation--review of 25 cases and comparison of C2 and C7 intralaminar screw fixation. World Neurosurg. 2010, 73, 112–118; discussion e115. [Google Scholar] [CrossRef]
- Lee, S.; Jung, S.K.; Kim, H.B.; Roh, S.W.; Jeon, S.R.; Park, J.H. Postoperative Non-Pathological Fever Following Posterior Cervical Fusion Surgery: Is Laminoplasty a Better Preventive Method than Laminectomy? J. Korean Neurosurg. Soc. 2020, 63, 487–494. [Google Scholar] [CrossRef] [Green Version]
- Osterhoff, G.; Ryang, Y.M.; von Oelhafen, J.; Meyer, B.; Ringel, F. Posterior Multilevel Instrumentation of the Lower Cervical Spine: Is Bridging the Cervicothoracic Junction Necessary? World Neurosurg. 2017, 103, 419–423. [Google Scholar] [CrossRef] [Green Version]
- Ramieri, A.; Domenicucci, M.; Ciappetta, P.; Cellocco, P.; Raco, A.; Costanzo, G. Spine surgery in neurological lesions of the cervicothoracic junction: Multicentric experience on 33 consecutive cases. Eur. Spine J. 2011, 20 (Suppl. 1), S13–S19. [Google Scholar] [CrossRef] [Green Version]
- Ishak, B.; Abdul-Jabbar, A.; Glinski, A.V.; Yilmaz, E.; Unterberg, A.W.; Hopkins, S.; Roh, J.; Oskouian, R.; Hart, R.; Chapman, J.R. Comparing Combined Anterior and Posterior to Posterior-Only Decompression and Fusion Crossing the Cervico-Thoracic Junction in Octogenarians. Glob. Spine J. 2023, 13, 164–171. [Google Scholar] [CrossRef]
- Pinter, Z.W.; Karamian, B.; Bou Monsef, J.; Mao, J.; Xiong, A.; Bowles, D.R.; Conaway, W.K.; Reiter, D.M.; Honig, R.; Currier, B.; et al. Cervical Alignment and Proximal and Distal Junctional Failure in Posterior Cervical Fusion: A Multicenter Comparison of 2 Surgical Approaches. Clin. Spine Surg. 2022, 35, E451–E456. [Google Scholar] [CrossRef]
- Roth, S.G.; Khan, I.; Chotai, S.; Chanbour, H.; Stephens, B.; Abtahi, A.; Devin, C.J.; Zuckerman, S.L. Is it Better to Stop at C2 or C3/4 in Elective Posterior Cervical Decompression and Fusion? Spine 2022, 47, 565–573. [Google Scholar] [CrossRef]
- Tobin, M.K.; Gragnaniello, C.; Sun, F.W.; Rangwala, S.D.; Birk, D.M.; Neckrysh, S. Safety and Efficacy of Skipping C7 Instrumentation in Posterior Cervicothoracic Fusion. World Neurosurg. 2019, 130, e68–e73. [Google Scholar] [CrossRef] [PubMed]
- Perez, E.A.; Woodroffe, R.W.; Park, B.; Gold, C.; Helland, L.C.; Seaman, S.C.; Hitchon, P.W. Cervical alignment in the obese population following posterior cervical fusion for cervical myelopathy. Clin. Neurol. Neurosurg. 2022, 212, 107059. [Google Scholar] [CrossRef]
- Sherrill, J.T.; Bumpass, D.B.; Mannen, E.M. Mechanical Analysis of 3 Posterior Fusion Assemblies Intended to Cross the Cervicothoracic Junction. Clin. Spine Surg. 2022, 35, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Horn, S.R.; Passias, P.G.; Oh, C.; Lafage, V.; Lafage, R.; Smith, J.S.; Line, B.; Anand, N.; Segreto, F.A.; Bortz, C.A.; et al. Predicting the combined occurrence of poor clinical and radiographic outcomes following cervical deformity corrective surgery. J. Neurosurg. Spine 2019, 32, 182–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Truumees, E.; Singh, D.; Geck, M.J.; Stokes, J.K. Should long-segment cervical fusions be routinely carried into the thoracic spine? A multicenter analysis. Spine J. 2018, 18, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Xun, M.A.; Rui, W.; Bin, Z.; Haoyu, F.; Jianzhong, H.; Jianghua, T. Clinical analysis of surgical reconstitution of cervicothoracic junction. Chin. J. Orthop. 2012, 32, 39–45. [Google Scholar] [CrossRef]
- Choi, S.J.; Suk, K.S.; Yang, J.H.; Kim, H.S.; Lee, H.M.; Moon, S.H.; Lee, B.H.; Park, S.J. What is a Right Distal Fusion Level for Prevention of Sagittal Imbalance in Multilevel Posterior Cervical Spine Surgery: C7 or T1? Clin. Spine Surg. 2018, 31, 441–445. [Google Scholar] [CrossRef]
- Huang, K.T.; Harary, M.; Abd-El-Barr, M.M.; Chi, J.H. Crossing the Cervicothoracic Junction in Posterior Cervical Decompression and Fusion: A Cohort Analysis. World Neurosurg. 2019, 131, e514–e520. [Google Scholar] [CrossRef]
- Kennamer, B.T.; Arginteanu, M.S.; Moore, F.M.; Steinberger, A.A.; Yao, K.C.; Gologorsky, Y. Complications of Poor Cervical Alignment in Patients Undergoing Posterior Cervicothoracic Laminectomy and Fusion. World Neurosurg. 2019, 122, e408–e414. [Google Scholar] [CrossRef]
- Lee, D.H.; Cho, J.H.; Jung, J.I.; Baik, J.M.; Jun, D.S.; Hwang, C.J.; Lee, C.S. Does stopping at C7 in long posterior cervical fusion accelerate the symptomatic breakdown of cervicothoracic junction? PLoS ONE 2019, 14, e0217792. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.K.; Badiee, R.K.; Rivera, J.; Chang, C.C.; Robinson, L.C.; Mehra, R.N.; Tan, L.A.; Clark, A.J.; Dhall, S.S.; Chou, D.; et al. Crossing the Cervicothoracic Junction During Posterior Cervical Fusion for Myelopathy Is Associated With Superior Radiographic Parameters But Similar Clinical Outcomes. Neurosurgery 2020, 87, 1016–1024. [Google Scholar] [CrossRef] [PubMed]
- Fayed, I.; Toscano, D.T.; Triano, M.J.; Makariou, E.; Lee, C.; Spitz, S.M.; Anaizi, A.N.; Nair, M.N.; Sandhu, F.A.; Voyadzis, J.M. Crossing the Cervicothoracic Junction During Posterior Cervical Decompression and Fusion: Is It Necessary? Neurosurgery 2020, 86, E544–E550. [Google Scholar] [CrossRef] [PubMed]
- Hines, K.; Wilt, Z.T.; Franco, D.; Mahtabfar, A.; Elmer, N.; Gonzalez, G.A.; Montenegro, T.S.; Velagapudi, L.; Patel, P.D.; Detweiler, M.; et al. Long-segment posterior cervical decompression and fusion: Does caudal level affect revision rate? J. Neurosurg. Spine 2021, 35, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Labrum, J.T.t.; Khan, I.; Archer, K.R.; Abtahi, A.M.; Stephens, B.F., 2nd. Lowest Instrumented Vertebra Selection in Posterior Cervical Fusion: Does Cervicothoracic Junction Lowest Instrumented Vertebra Predict Mechanical Failure? Spine 2021, 46, E482–E490. [Google Scholar] [CrossRef]
- Okamoto, N.; Kato, S.; Doi, T.; Matsubayashi, Y.; Taniguchi, Y.; Yoshida, Y.; Kawamura, N.; Nakarai, H.; Higashikawa, A.; Tozawa, K.; et al. Relative Risks and Benefits of Crossing the Cervicothoracic Junction During Multilevel Posterior Cervical Fusion: A Multicenter Cohort. World Neurosurg. 2021, 153, e265–e274. [Google Scholar] [CrossRef]
- Scholz, C.; Klingler, J.H.; Masalha, W.; Hohenhaus, M.; Volz, F.; Vasilikos, I.; Roelz, R.; Scheiwe, C.; Hubbe, U. Long-Term Results after Multilevel Fusion of the Cervical Spine and the Cervicothoracic Junction: To Bridge or Not To Bridge? World Neurosurg. 2021, 148, e556–e564. [Google Scholar] [CrossRef]
- Sun, K.; Zhang, S.; Yang, B.; Sun, X.; Shi, J. The Effect of Laminectomy with Instrumented Fusion Carried into the Thoracic Spine on the Sagittal Imbalance in Patients with Multilevel Ossification of the Posterior Longitudinal Ligament. Orthop. Surg. 2021, 13, 2280–2288. [Google Scholar] [CrossRef]
- Truumees, E.; Singh, D.; Lavelle, W.; Riesenburger, R.; Geck, M.; Kurra, S.; Yu, A.; Grits, D.; Dowd, R.; Winkelman, R.; et al. Is it safe to stop at C7 during multilevel posterior cervical decompression and fusion?—multicenter analysis. Spine J. 2021, 21, 90–95. [Google Scholar] [CrossRef]
- Charest-Morin, R.; Bailey, C.S.; McIntosh, G.; Rampersaud, Y.R.; Jacobs, W.B.; Cadotte, D.W.; Paquet, J.; Hall, H.; Weber, M.H.; Johnson, M.G.; et al. Does extending a posterior cervical fusion construct into the upper thoracic spine impact patient-reported outcomes as long as 2 years after surgery in patients with degenerative cervical myelopathy? J. Neurosurg. Spine 2022, 37, 547–555. [Google Scholar] [CrossRef]
- Cho, W.; Auerbach, J.D.; Riew, K.D. Crossing the Cervico-Thoracic Junction in Long Posterior Cervical Fusions Reduces Caudal Adjacent Segment Pathology. Glob. Spine J. 2022, 12, 1636–1639. [Google Scholar] [CrossRef]
- Couch, B.K.; Patel, S.S.; Talentino, S.E.; Buldo-Licciardi, M.; Evashwick-Rogler, T.W.; Oyekan, A.A.; Gannon, E.J.; Shaw, J.D.; Donaldson, W.F.; Lee, J.Y. To Cross the Cervicothoracic Junction? Terminating Posterior Cervical Fusion Constructs Proximal to the Cervicothoracic Junction Does Not Impart Increased Risk of Reoperation in Patients With Cervical Spondylotic Myelopathy. Glob. Spine J. 2022, 21925682221083926. [Google Scholar] [CrossRef] [PubMed]
- Kretzer, R.M.; Hu, N.; Umekoji, H.; Sciubba, D.M.; Jallo, G.I.; McAfee, P.C.; Tortolani, P.J.; Cunningham, B.W. The effect of spinal instrumentation on kinematics at the cervicothoracic junction: Emphasis on soft-tissue response in an in vitro human cadaveric model. J. Neurosurg. Spine 2010, 13, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Eck, J.C.; Humphreys, S.C.; Lim, T.H.; Jeong, S.T.; Kim, J.G.; Hodges, S.D.; An, H.S. Biomechanical study on the effect of cervical spine fusion on adjacent-level intradiscal pressure and segmental motion. Spine 2002, 27, 2431–2434. [Google Scholar] [CrossRef] [PubMed]
- Cheng, I.; Sundberg, E.B.; Iezza, A.; Lindsey, D.P.; Riew, K.D. Biomechanical Determination of Distal Level for Fusions across the Cervicothoracic Junction. Glob. Spine J. 2015, 5, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Badiee, R.K.; Mayer, R.; Pennicooke, B.; Chou, D.; Mummaneni, P.V.; Tan, L.A. Complications following posterior cervical decompression and fusion: A review of incidence, risk factors, and prevention strategies. J. Spine Surg. 2020, 6, 323–333. [Google Scholar] [CrossRef]
- Yoo, S.J.; Park, J.Y.; Chin, D.K.; Kim, K.S.; Cho, Y.E.; Kim, K.H. Predictive risk factors for mechanical complications after multilevel posterior cervical instrumented fusion. J. Neurosurg. Spine 2023, 38, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.A.; Scheer, J.K.; Smith, J.S.; Deviren, V.; Bess, S.; Hart, R.A.; Lafage, V.; Shaffrey, C.I.; Schwab, F.; Ames, C.P. The impact of standing regional cervical sagittal alignment on outcomes in posterior cervical fusion surgery. Neurosurgery 2015, 76 (Suppl. 1), S14–S21; discussion S21. [Google Scholar] [CrossRef]
- Liu, H.; Li, Y.; Chen, Y.; Wu, W.; Zou, D. Cervical curvature, spinal cord MRIT2 signal, and occupying ratio impact surgical approach selection in patients with ossification of the posterior longitudinal ligament. Eur. Spine J. 2013, 22, 1480–1488. [Google Scholar] [CrossRef] [Green Version]
- Roguski, M.; Benzel, E.C.; Curran, J.N.; Magge, S.N.; Bisson, E.F.; Krishnaney, A.A.; Steinmetz, M.P.; Butler, W.E.; Heary, R.F.; Ghogawala, Z. Postoperative cervical sagittal imbalance negatively affects outcomes after surgery for cervical spondylotic myelopathy. Spine 2014, 39, 2070–2077. [Google Scholar] [CrossRef] [Green Version]
- Medvedev, G.; Wang, C.; Cyriac, M.; Amdur, R.; O’Brien, J. Complications, Readmissions, and Reoperations in Posterior Cervical Fusion. Spine 2016, 41, 1477–1483. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Selection | Comparability | Exposure | Total Score |
|---|---|---|---|---|---|
| Choi [37] | 2018 | 3 | 2 | 2 | 7 |
| Huang [38] | 2019 | 4 | 2 | 2 | 8 |
| Kennamer [39] | 2019 | 3 | 1 | 2 | 6 |
| Lee [40] | 2019 | 3 | 2 | 2 | 7 |
| Chan [41] | 2021 | 4 | 2 | 3 | 9 |
| Fayed [42] | 2020 | 3 | 2 | 3 | 8 |
| Hines [43] | 2021 | 4 | 2 | 2 | 8 |
| Labrum [44] | 2021 | 3 | 2 | 3 | 8 |
| Okamoto [45] | 2021 | 4 | 2 | 3 | 9 |
| Scholz [46] | 2021 | 3 | 1 | 2 | 6 |
| Sun [47] | 2021 | 4 | 2 | 2 | 8 |
| Truumees [48] | 2020 | 4 | 1 | 2 | 7 |
| Morin [49] | 2022 | 4 | 2 | 2 | 8 |
| Cho [50] | 2022 | 3 | 2 | 2 | 7 |
| Couch [51] | 2022 | 4 | 1 | 2 | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, H.; Huang, J.; Hai, Y.; Fan, Z.; Zhang, Y.; Yin, P.; Yang, J. Is It Necessary to Cross the Cervicothoracic Junction in Posterior Cervical Decompression and Fusion for Multilevel Degenerative Cervical Spine Disease? A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 2806. https://doi.org/10.3390/jcm12082806
Yang H, Huang J, Hai Y, Fan Z, Zhang Y, Yin P, Yang J. Is It Necessary to Cross the Cervicothoracic Junction in Posterior Cervical Decompression and Fusion for Multilevel Degenerative Cervical Spine Disease? A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(8):2806. https://doi.org/10.3390/jcm12082806
Chicago/Turabian StyleYang, Honghao, Jixuan Huang, Yong Hai, Zhexuan Fan, Yiqi Zhang, Peng Yin, and Jincai Yang. 2023. "Is It Necessary to Cross the Cervicothoracic Junction in Posterior Cervical Decompression and Fusion for Multilevel Degenerative Cervical Spine Disease? A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 8: 2806. https://doi.org/10.3390/jcm12082806