
Plasma Soluble Fibrin Is Useful for the Diagnosis of Thrombotic Diseases
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thachil, J.; Lippi, G.; Favaloro, E.J. D-Dimer Testing: Laboratory Aspects and Current Issues. Methods Mol. Biol. 2017, 1646, 91–104. [Google Scholar] [PubMed]
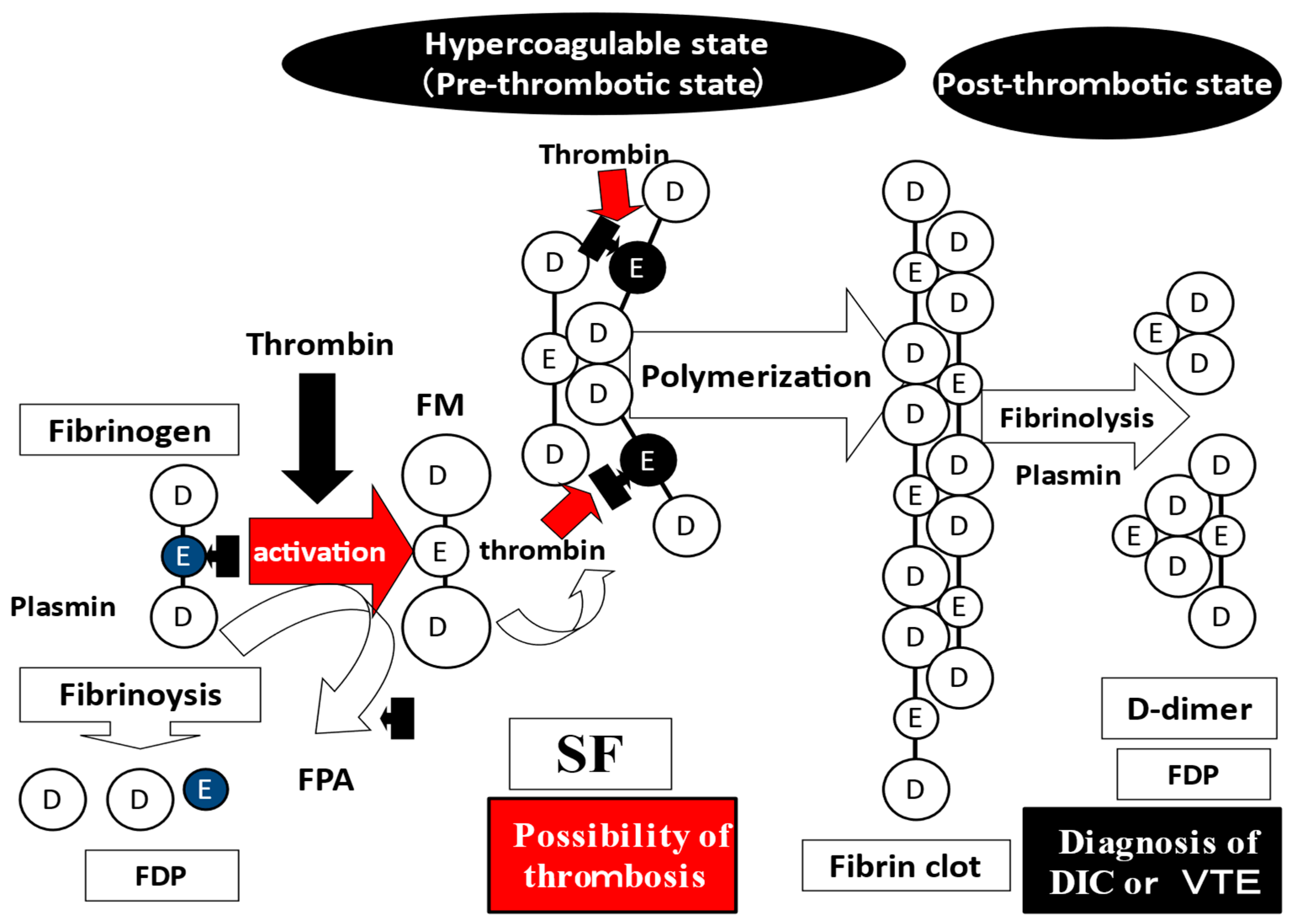
- Dempfle, C.E. The use of soluble fibrin in evaluating the acute and chronic hypercoagulable state. Thromb. Haemost. 1999, 82, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Wada, H.; Sakuragawa, N. Are fibrin-related markers useful for the diagnosis of thrombosis? Semin. Thromb. Hemost. 2008, 34, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Sidelmann, J.J.; Gram, J.; Jespersen, J.; Kluft, C. Fibrin clot formation and lysis: Basic mechanisms. Semin. Thromb. Hemost. 2000, 26, 605–618. [Google Scholar] [CrossRef]
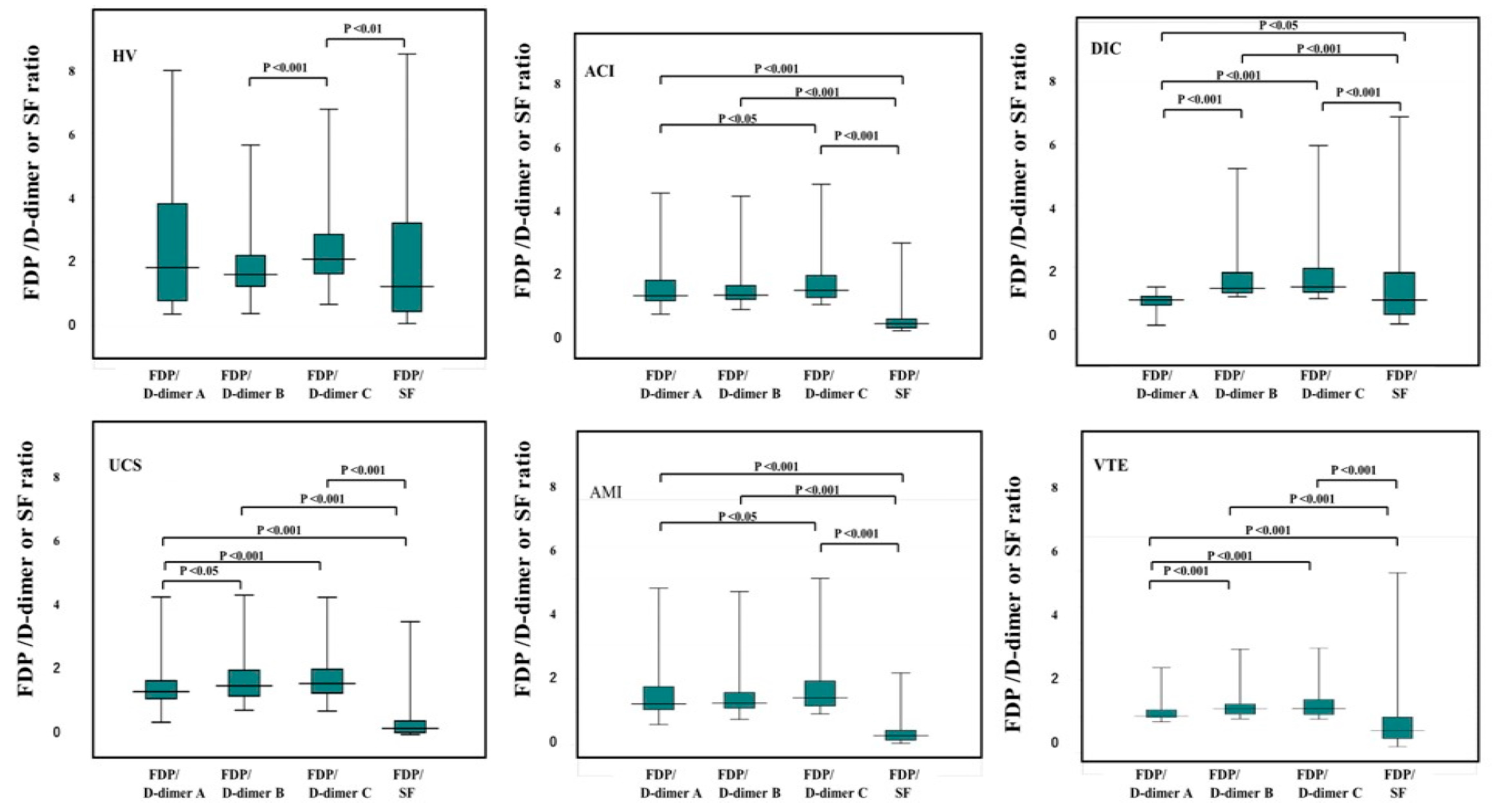
- Ikeda, N.; Wada, H.; Ichikawa, Y.; Ezaki, M.; Tanaka, M.; Hiromori, S.; Shiraki, K.; Moritani, I.; Yamamoto, A.; Shimpo, H.; et al. D-dimer kit with a High FDP/D-Dimer Ratio is Useful for Diagnosing Thrombotic Diseases. Clin. Appl. Thromb. Hemost. 2022, 28, 10760296211070584. [Google Scholar] [CrossRef]
- Wada, H.; Matsumoto, T.; Yamashita, Y.; Hatada, T. Disseminated Intravascular Coagulation: Testing and Diagnosis. Clin. Chim. Acta 2014, 436C, 130–134. [Google Scholar] [CrossRef]
- Wada, H.; Thachil, J.; Di Nisio, M.; Mathew, P.; Kurosawa, S.; Gando, S.; Kim, H.K.; Nielsen, J.D.; Dempfle, C.E.; Levi, M.; et al. The Scientific Standardization Committee on DIC of the International Society on Thrombosis Haemostasis.: Guidance for diagnosis and treatment of DIC from harmonization of the recommendations from three guidelines. J. Thromb. Haemost. 2013, 11, 761–767. [Google Scholar] [CrossRef]
- Johnson, E.D.; Schell, J.C.; Rodgers, G.M. The D-dimer assay. Am. J. Hematol. 2019, 94, 833–839. [Google Scholar] [CrossRef]
- Righini, M.; Van Es, J.; Den Exter, P.L.; Roy, P.M.; Verschuren, F.; Ghuysen, A.; Rutschmann, O.T.; Sanchez, O.; Jaffrelot, M.; Trinh-Duc, A.; et al. Age-adjusted D-dimer cutoff levels to rule out pulmonary embolism: The ADJUST-PE study. JAMA 2014, 311, 1117–1124. [Google Scholar] [CrossRef]
- Wells, P.S.; Anderson, D.R.; Rodger, M.; Forgie, M.; Kearon, C.; Dreyer, J.; Kovacs, G.; Mitchell, M.; Lewandowski, B.; Kovacs, M.J. Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis. N. Engl. J. Med. 2003, 349, 1227–1235. [Google Scholar] [CrossRef] [Green Version]
- Wada, H.; Kobayashi, T.; Abe, Y.; Hatada, T.; Yamada, N.; Sudo, A.; Uchida, A.; Nobori, T. Elevated levels of soluble fibrin or D-dimer indicate high risk of thrombosis. J. Thromb. Haemost. 2006, 4, 1253–1258. [Google Scholar] [CrossRef] [PubMed]
- Sudo, A.; Wada, H.; Nobori, T.; Yamada, N.; Ito, M.; Niimi, R. Cut-off values of D-dimer and soluble fibrin for prediction of deep vein thrombosis after orthopaedic surgery. Int. J. Hematol. 2009, 89, 572–576. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T.; Wada, H.; Miyazaki, S.; Hasegawa, M.; Wakabayashi, H.; Asanuma, K.; Fujimoto, N.; Matsumoto, T.; Ohishi, K.; Sakaguchi, A.; et al. Fibrin related markers for diagnosing acute or chronic venous thromboembolism in patients with major orthopedic surgery. Int. J. Hematol. 2016, 103, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Wada, H.; Hasegawa, M.; Wakabayashi, H.; Ando, H.; Oshima, S. Monitoring for anti-Xa activity for prophylactic administration of fondaparinux in patients with artificial joint replacement. Int. J. Hematol. 2011, 94, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, M.; Wada, H.; Wakabayashi, H.; Yoshida, K.; Miyamoto, N.; Asanuma, K. The relationships among hemostatic markers, the withdrawal of fondaparinux due to a reduction in hemoglobin and deep vein thrombosis in Japanese patients undergoing major orthopedic surgery. Clin. Chim. Acta 2013, 425, 109–113. [Google Scholar] [CrossRef]
- Suzuki, K.; Wada, H.; Imai, H.; Iba, T.; Thachil, J.; Toh, C.H. Subcommittee on Disseminated Intravascular Coagulation: A re-evaluation of the D-dimer cut-off value for making a diagnosis according to the ISTH overt-DIC diagnostic criteria: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2018, 16, 1442–1444. [Google Scholar] [CrossRef] [Green Version]
- Luo, H.C.; You, C.Y.; Lu, S.W.; Fu, Y.Q. Characteristics of coagulation alteration in patients with COVID-19. Ann. Hematol. 2021, 100, 45–52. [Google Scholar] [CrossRef]
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Li, D.; Sun, Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J. Thromb. Haemost. 2020, 18, 1094–1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Phelan, A.L.; Katz, R.; Gostin, L.O. The novel coronavirus originating in Wuhan, China: Challenges for global health governance. JAMA 2020, 323, 709–710. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, N.; Maegawa, T.; Takada, M.; Tanaka, H.; Gonmori, H. Criteria for diagnosis of DIC based on the analysis of clinical and laboratory findings in 345 DIC patients collected by the Research Committee on DIC in Japan. Bibl. Haemotol. 1983, 49, 265–275. [Google Scholar]
- Wada, H.; Takahashi, H.; Uchiyama, T.; Eguchi, Y.; Okamoto, K.; Kawasugi, K.; Madoiwa, S.; Asakura, H. DIC subcommittee of the Japanese Society on Thrombosis and Hemostasis.: The approval of revised diagnostic criteria for DIC from the Japanese Society on Thrombosis and Hemostasis. Thromb. J. 2017, 15, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, S.; Asakura, H. Management of disseminated intravascular coagulation associated with aortic aneurysm and vascular malformations. Int. J. Hematol. 2021, 113, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Kudo, D.; Goto, T.; Uchimido, R.; Hayakawa, M.; Yamakawa, K.; Abe, T.; Shiraishi, A.; Kushimoto, S. Coagulation phenotypes in sepsis and effects of recombinant human thrombomodulin: An analysis of three multicentre observational studies. Crit. Care 2021, 25, 114. [Google Scholar] [CrossRef]
- Bai, Y.; Shi, M.; Yang, X.; Zhang, W.; Yang, R.; Wei, X.; Wei, X.; Duan, L.; Wang, C.; Mi, R.; et al. The value of FDP/FIB and D-dimer/FIB ratios in predicting high-risk APL-related thrombosis. Leuk. Res. 2019, 79, 34–37. [Google Scholar] [CrossRef]
- Ikezoe, T. Advances in the diagnosis and treatment of disseminated intravascular coagulation in haematological malignancies. Int. J. Hematol. 2021, 113, 34–44. [Google Scholar] [CrossRef]
- Ichikawa, Y.; Wada, H.; Ezaki, E.; Tanaka, M.; Hiromori, S.; Shiraki, S.; Moritani, I.; Yamamoto, A.; Tashiro, H.; Shimpo, H.; et al. Elevated D-dimer levels predict a poor outcome in critically ill patients. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029620973084. [Google Scholar] [CrossRef]
- Nomura, H.; Wada, H.; Mizuno, T.; Katayama, N.; Abe, Y.; Noda, M.; Nakatani, K.; Matsumoto, T.; Ota, S.; Yamada, N.; et al. Negative predictive value of D-dimer for diagnosis of venous thromboembolism. Int. J. Hematol. 2008, 87, 250–255. [Google Scholar] [CrossRef]
- Wada, H.; Yamamoto, A.; Tomida, M.; Ichikawa, Y.; Ezaki, M.; Masuda, J.; Yoshida, M.; Fukui, S.; Moritani, I.; Inoue, H.; et al. Proposal of Quick Diagnostic Criteria for Disseminated Intravascular Coagulation. J. Clin. Med. 2022, 11, 1028. [Google Scholar] [CrossRef]
- Taylor, F.B., Jr.; Toh, C.H.; Hoots, K.; Wada, H.; Levi, M. Towards a definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb. Haemost. 2001, 86, 1327–1330. [Google Scholar] [CrossRef] [Green Version]
- Iba, T.; Levy, J.H.; Warkentin, T.E.; Thachil, J.; van der Poll, T.; Levi, M. Scientific and Standardization Committee on DIC, and the Scientific and Standardization Committee on Perioperative and Critical Care of the International Society on Thrombosis and Haemostasis.: Diagnosis and management of sepsis-induced coagulopathy and disseminated intravascular coagulation. J. Thromb. Haemost. 2019, 17, 1989–1994. [Google Scholar] [PubMed] [Green Version]
- Wada, H.; Shiraki, K.; Shimaoka, M. The prothrombin time ratio is not a more effective marker for evaluating sepsis-induced coagulopathy than fibrin-related markers. J. Thromb. Hemost. 2020, 18, 1506–1507. [Google Scholar] [CrossRef] [PubMed]
- Nishigaki, A.; Ichikawa, Y.; Ezaki, E.; Yamamoto, A.; Suzuki, K.; Tachibana, K.; Kamon, T.; Horie, S.; Masuda, J.; Makino, K.; et al. Soluble C-type lectin-like receptor 2 elevation in patients with acute cerebral infarction. J. Clin. Med. 2021, 10, 3408. [Google Scholar] [CrossRef] [PubMed]
- Sawamura, A.; Hayakawa, M.; Gando, S.; Kubota, N.; Sugano, M.; Wada, T.; Katabami, K. Disseminated intravascular coagulation with a fibrinolytic phenotype at an early phase of trauma predicts mortality. Thromb. Res. 2009, 124, 608–613. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Median | 2.5–97.5 Percentile | ||
|---|---|---|---|
| Soluble fibrin | µg/mL | 0.3 | 0.0–3.3 |
| FDP | µg/mL | 0.5 | 0.1–2.1 |
| D-dimer (A) | µg/mL | 0.3 | 0.1–1.0 |
| D-dimer (B) | µg/mL | 0.3 | 0.1–1.1 |
| D-dimer (C) | µg/mL | 0.2 | 0.1–0.7 |
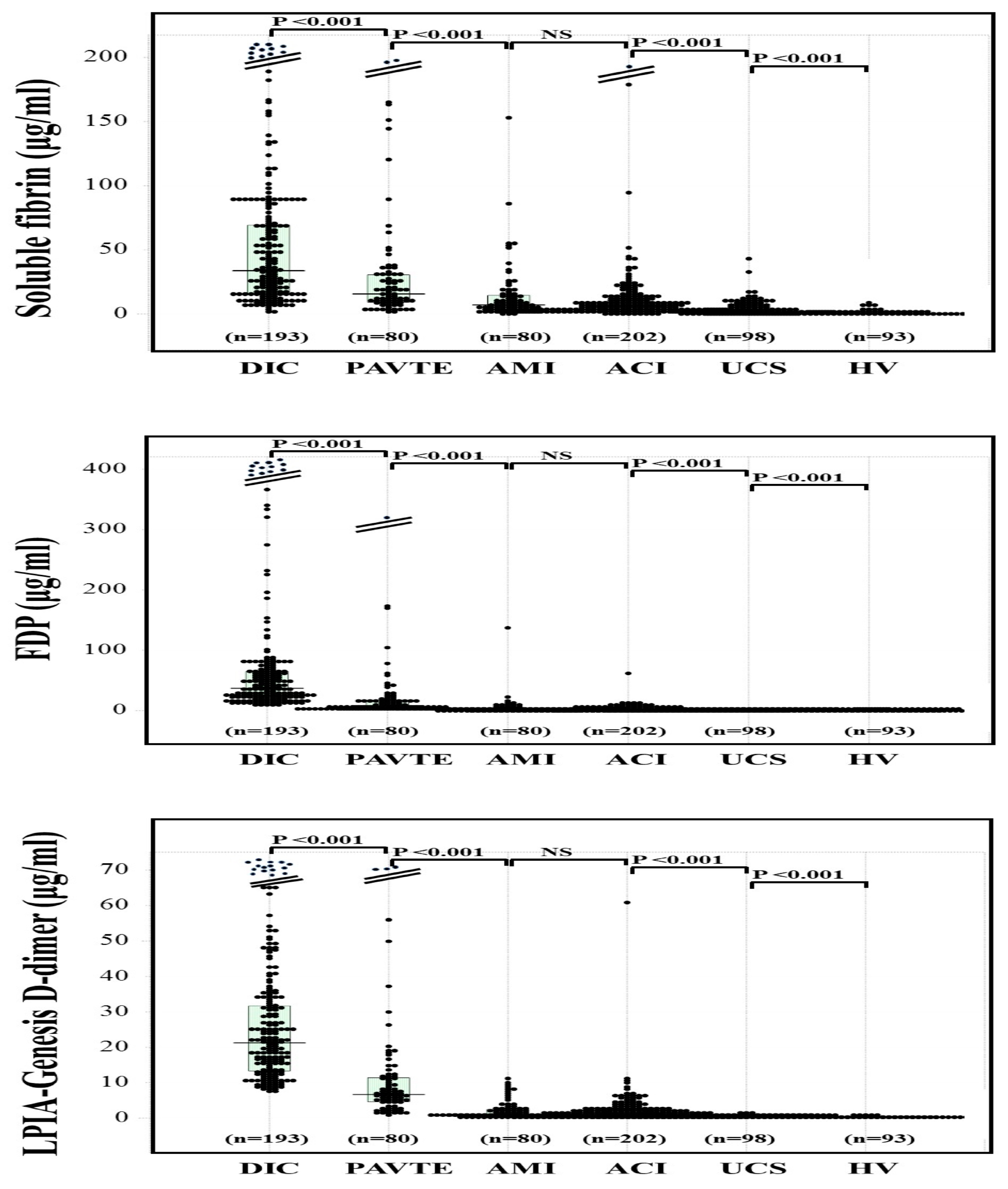
| N | Soluble Fibrin | FDP | D-Dimer (A) | D-Dimer (B) | D-Dimer (C) | |
|---|---|---|---|---|---|---|
| (µg/mL) | (µg/mL) | (µg/mL) | (µg/mL) | (µg/mL) | ||
| DIC/Pre-DIC | 181 | 35.3 (16.1–82.2) | 36.9 (22.0–64.6) | 32.3 (21.2–56.1) | 24.5 (16.5–40.0) | 22.3 (14.3–35.1) |
| VTE | 53 | 16.2 (8.7–36.5) | 10.2 (6.4–24.3) | 9.0 (6.1–18.7) | 8.4 (5.8–18.1) | 7.5 (5.7–16.8) |
| PATE | 26 | 19.4 (9.2–27.1) | 4.7 (1.8–9.1) | 4.9 (2.2–12.3) | 4.7 (2.0–9.5) | 4.7 (1.8–9.1) |
| AMI | 80 | 7.1 (3.5–14.4) | 1.5 (0.9–3.4) | 0.9 (0.5–2.8) | 1.1 (0.6–2.9) | 1.0 (0.6–2.5) |
| ACI | 202 | 5.7 (2.3–11.5) | 1.6 (1.0–10.7) | 1.2 (0.5–2.4) | 1.2 (0.7–2.3) | 1.2 (0.7–2.4) |
| UCS | 98 | 3.0 (1.5–7.6) | 0.8 (0.6–2.2) | 0.5 (0.5–0.5) | 0.5 (0.4–0.7) | 0.5 (0.3–0.7) |
| HV | 98 | 0.3 (0.1–0.9) | 0.5 (0.4–0.7) | 0.3 (0.1–0.4) | 0.4 (0.2–0.4) | 0.2 (0.1–0.4) |
| With thrombosis | 542 | 12.4 (5.2–33.3) | 6.2 (1.5–27.7) | 5.4 (1.1–25.2) | 5.3 (1.1–19.6) | 5.2 (1.1–17.2) |
| Without thrombosis | 196 | 1.2 (0.3–3.3) | 0.6 (0.4–0.8) | 0.5 (0.4–0.5) | 0.4 (0.3–0.6) | 0.3 (0.2–0.5) |
| Soluble Fibrin (μg/mL) | FDP (μg/mL) | D-Dimer A (μg/mL) | D-Dimer B (μg/mL) | D-Dimer C (μg/mL) | |
|---|---|---|---|---|---|
| Atherosclerotic or lacuna ACI | 4.7 NS (2.4–11.4) | 1.3 ** (0.8–2.5) | 1.1 * (0.5–2.0) | 1.0 ** (0.6–1.9) | 1.0 ** (0.6–1.8) |
| Other ACI | 5.9 NS (2.3–11.4) | 2.1 ** (1.1–3.5) | 1.6 * (0.6–3.0) | 1.5 ** (0.7–2.9) | 1.4 ** (0.7–2.8) |
| ACI without antithrombotic agents | 5.6 NS (2.2–10.7) | 1.7 NS (1.0–3.1) | 1.2 NS (0.5–2.5) | 1.2 NS (0.6–2.5) | 1.1 NS (0.7–2.4) |
| ACI with antithrombotic agents | 6.5 NS (2.6–12.7) | 1.4 NS (0.9–2.6) | 1.2 NS (0.5–2.3) | 1.1 NS (0.6–2.5) | 1.2 NS (0.7–2.4) |
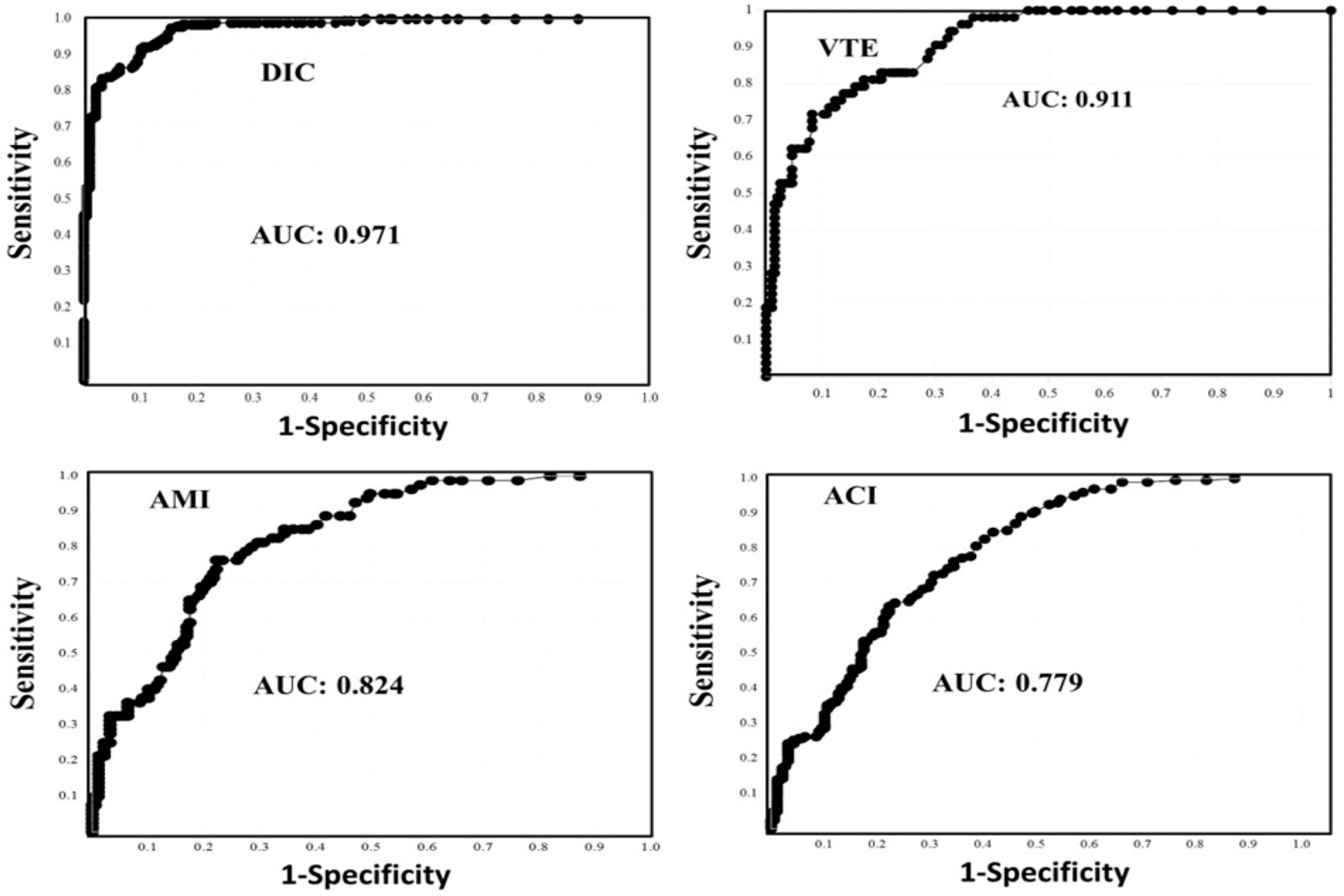
| AUC | Cutoff Value-1 | Sensitivity | Odds Ratio | Cutoff Value-2 | Sensitivity | Specificity | Odds Ratio | |
|---|---|---|---|---|---|---|---|---|
| Disseminated intravascular coagulation | ||||||||
| SF | 0.971 | 9.5 μg/mL | 90.0% | 81.9 | 3.3 μg/mL | 97.5% | 76.7% | 315 |
| FDP | 1.000 | 10.0 μg/mL | 99.5% | - | 2.1 μg/mL | 100% | 100% | - |
| D-dimer A | 1.000 | 7.8 μg/mL | 99.5% | - | 1.2 μg/mL | 100% | 100% | - |
| D-dimer B | 1.000 | 7.2 μg/mL | 99.5% | - | 1.2 μg/mL | 100% | 100% | - |
| D-dimer C | 1.000 | 7.8 μg/mL | 99.5% | - | 1.2 μg/mL | 100% | 100% | - |
| Venous thromboembolism | ||||||||
| SF | 0.911 | 6.5 μg/mL | 81.1% | 18.5 | 3.3 μg/mL | 83.0% | 76.0% | 13.9 |
| FDP | 0.997 | 2.0 μg/mL | 96.4% | 808 | 2.1 μg/mL | 96.2% | 97.4% | 974 |
| D-dimer A | 0.999 | 1.1 μg/mL | 98.1% | 2513 | 1.2 μg/mL | 98.1% | 98.6% | 3796 |
| D-dimer B | 0.997 | 1.3 μg/mL | 98.1% | 2496 | 1.2 μg/mL | 98.1% | 96.4% | 1404 |
| D-dimer C | 0.999 | 1.1 μg/mL | 98.4% | 3345 | 1.2 μg/mL | 98.1% | 99.5% | 10,140 |
| Acute myocardial infarction | ||||||||
| SF | 0.824 | 3.3 μg/mL | 76.3% | 10.6 | 3.3 μg/mL | 76.3% | 76.3% | 10.6 |
| FDP | 0.824 | 0.9 μg/mL | 77.5% | 11.6 | 2.1 μg/mL | 45.0% | 97.4% | 25.6 |
| D-dimer A | 0.832 | 0.5 μg/mL | 73.9% | 10.0 | 1.2 μg/mL | 40% | 98.6% | 48.7 |
| D-dimer B | 0.850 | 0.6 μg/mL | 75.0% | 11.3 | 1.2 μg/mL | 47.5% | 96.4% | 24.4 |
| D-dimer C | 0.872 | 0.5 μg/mL | 78.8% | 12.3 | 1.2 μg/mL | 43.8% | 99.4% | 151.7 |
| Acute cerebral infarction | ||||||||
| SF | 0.779 | 2.7 μg/mL | 70.3% | 5.5 | 3.3 μg/mL | 64.4% | 76.7% | 6.0 |
| FDP | 0.851 | 0.9 μg/mL | 78.2% | 12.8 | 2.1 μg/mL | 40.1% | 97.4% | 25.6 |
| D-dimer A | 0.853 | 0.5 μg/mL | 75.2% | 11.2 | 1.2 μg/mL | 46.5% | 98.6% | 63.5 |
| D-dimer B | 0.875 | 0.6 μg/mL | 79.8% | 15.8 | 1.2 μg/mL | 48.5% | 96.4% | 25.4 |
| D-dimer C | 0.892 | 0.6 μg/mL | 80.2% | 17.5 | 1.2 μg/mL | 47.5% | 99.4% | 176.6 |
| All thrombosis | ||||||||
| SF | 0.877 | 4.0 μg/mL | 78.8% | 13.6 | 3.3 μg/mL | 81.6% | 76.7% | 14.6 |
| FDP | 0.923 | 1.0 μg/mL | 84.2% | 26.2 | 2.1 μg/mL | 69.7% | 97.4% | 88.0 |
| D-dimer A | 0.922 | 0.5 μg/mL | 84.3% | 25.4 | 1.2 μg/mL | 71.5% | 98.6% | 183.4 |
| D-dimer B | 0.932 | 0.7 μg/mL | 85.0% | 33.6 | 1.2 μg/mL | 73.3% | 96.4% | 74.3 |
| D-dimer C | 0.942 | 0.7 μg/mL | 85.5% | 44.2 | 1.2 μg/mL | 72.4% | 99.5% | 512.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ezaki, M.; Wada, H.; Ichikawa, Y.; Ikeda, N.; Shiraki, K.; Yamamoto, A.; Moritani, I.; Shimaoka, M.; Shimpo, H. Plasma Soluble Fibrin Is Useful for the Diagnosis of Thrombotic Diseases. J. Clin. Med. 2023, 12, 2597. https://doi.org/10.3390/jcm12072597
Ezaki M, Wada H, Ichikawa Y, Ikeda N, Shiraki K, Yamamoto A, Moritani I, Shimaoka M, Shimpo H. Plasma Soluble Fibrin Is Useful for the Diagnosis of Thrombotic Diseases. Journal of Clinical Medicine. 2023; 12(7):2597. https://doi.org/10.3390/jcm12072597
Chicago/Turabian StyleEzaki, Minoru, Hideo Wada, Yuhuko Ichikawa, Nozomi Ikeda, Katsuya Shiraki, Akitaka Yamamoto, Isao Moritani, Motomu Shimaoka, and Hideto Shimpo. 2023. "Plasma Soluble Fibrin Is Useful for the Diagnosis of Thrombotic Diseases" Journal of Clinical Medicine 12, no. 7: 2597. https://doi.org/10.3390/jcm12072597