
Study of Modifications Induced by Continued Direct Oral Anticoagulant Therapy during Atrial Fibrillation Ablation Procedures on Standard Hemostasis Parameters
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Procedure Protocol
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Population and Procedural Characteristics
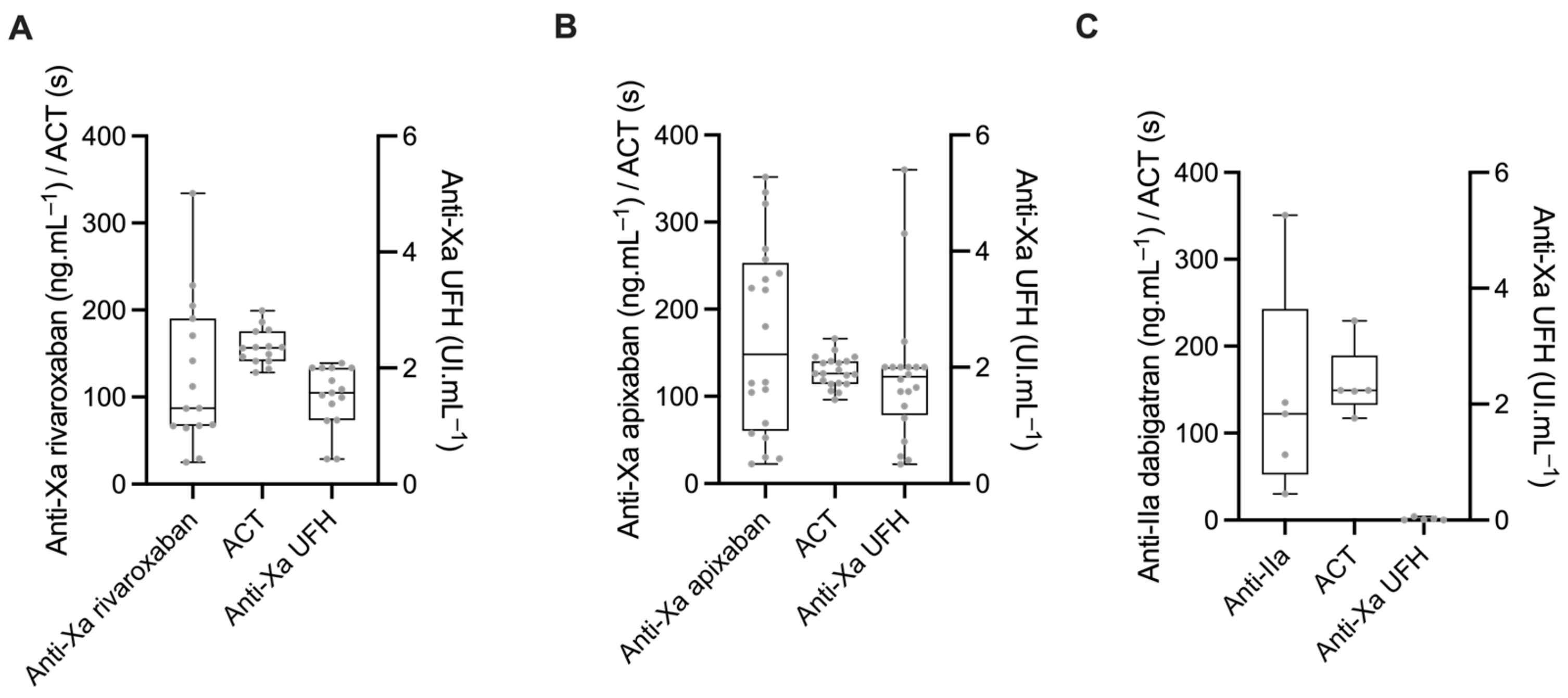
3.2. Baseline Anticoagulation State
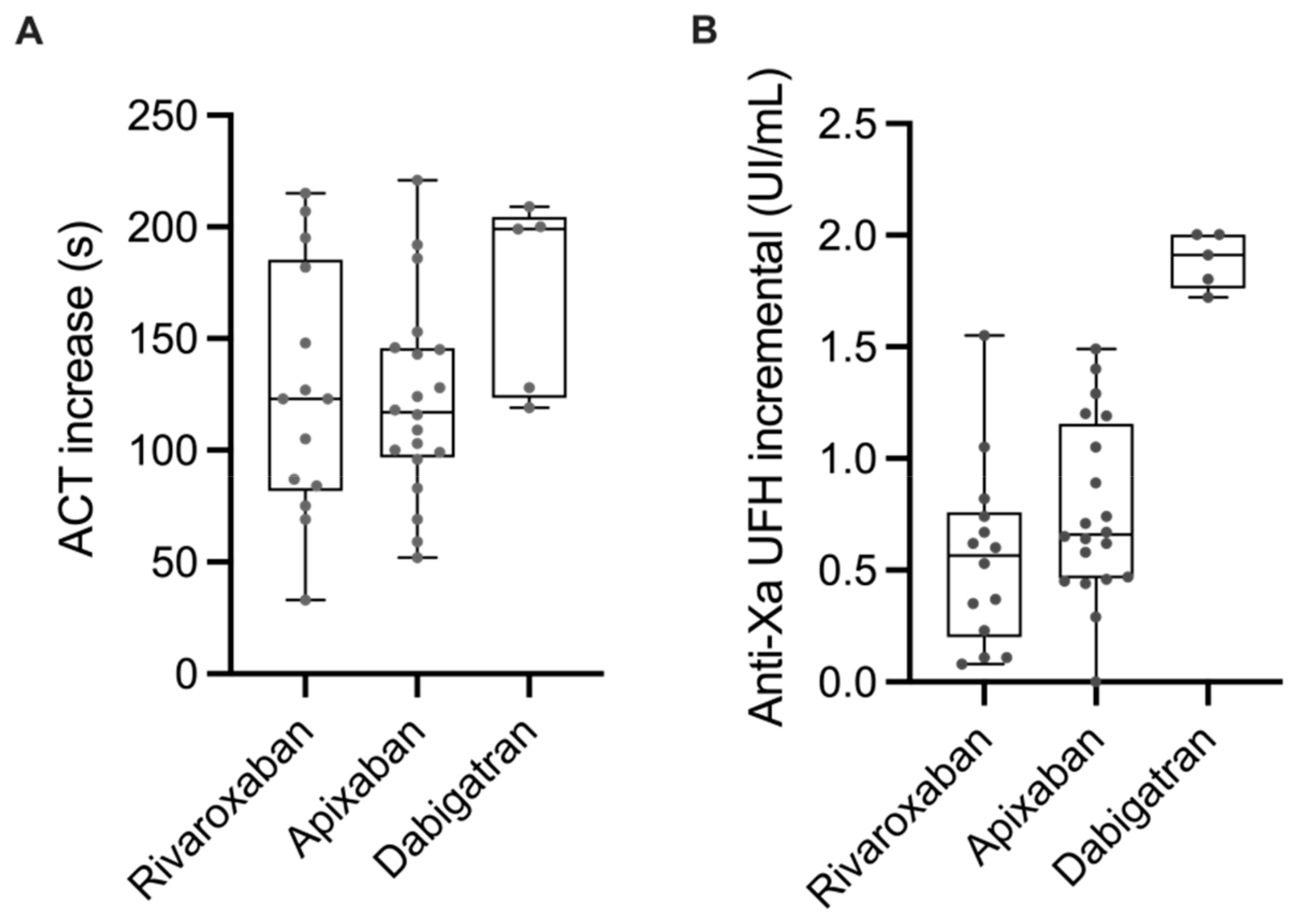
3.3. Effect of the Initial Bolus of UFH
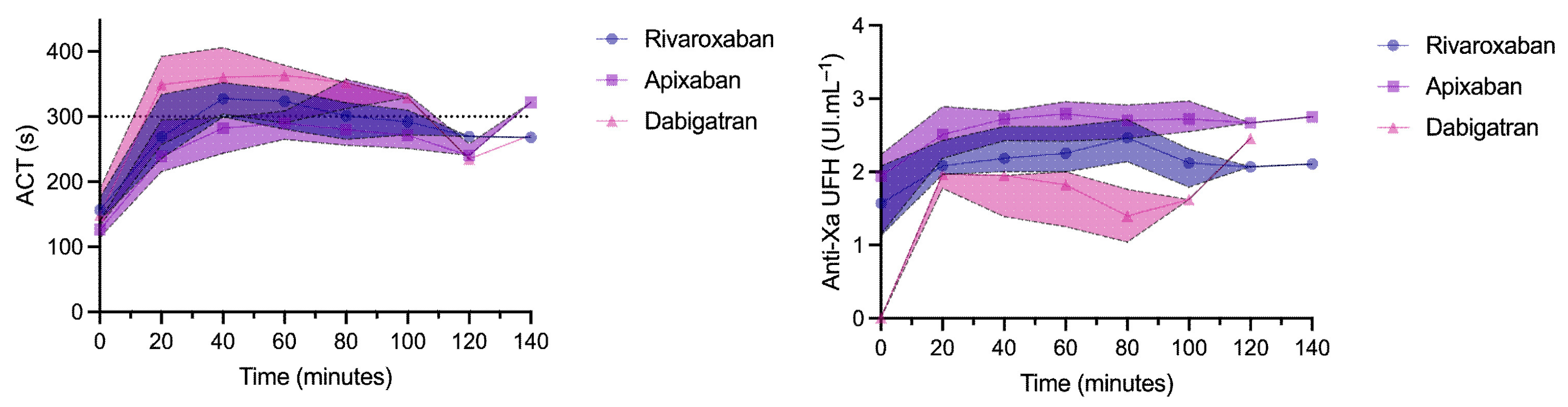
3.4. Anticoagulation during the Procedure
3.5. Correlation between ACT and Anti-Xa UFH during the Procedure (after the Initial Bolus of UFH)
3.6. Complications after the Procedure
4. Discussion
Main Findings
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Chugh, S.S.; Havmoeller, R.; Narayanan, K.; Singh, D.; Rienstra, M.; Benjamin, E.J.; Gillum, R.F.; Kim, Y.H.; McAnulty, J.H., Jr.; Zheng, Z.J.; et al. Worldwide epidemiology of atrial fibrillation: A Global Burden of Disease 2010 Study. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staerk, L.; Sherer, J.A.; Ko, D.; Benjamin, E.J.; Helm, R.H. Atrial Fibrillation: Epidemiology, Pathophysiology, and Clinical Outcomes. Circ. Res. 2017, 120, 1501–1517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar]
- Chang, R.J.; Doherty, T.M.; Goldberg, S.L. How does warfarin affect the activated coagulation time? Am. Heart J. 1998, 136, 477–479. [Google Scholar] [CrossRef]
- Di Biase, L.; Burkhardt, J.D.; Santangeli, P.; Mohanty, P.; Sanchez, J.E.; Horton, R.; Gallinghouse, G.J.; Themistoclakis, S.; Rossillo, A.; Lakkireddy, D.; et al. Periprocedural stroke and bleeding complications in patients undergoing catheter ablation of atrial fibrillation with different anticoagulation management: Results from the Role of Coumadin in Preventing Thromboembolism in Atrial Fibrillation (AF) Patients Undergoing Catheter Ablation (COMPARE) randomized trial. Circulation 2014, 129, 2638–2644. [Google Scholar]
- Kirchhof, P.; Haeusler, K.G.; Blank, B.; De Bono, J.; Callans, D.; Elvan, A.; Fetsch, T.; Van Gelder, I.C.; Gentlesk, P.; Grimaldi, M.; et al. Apixaban in patients at risk of stroke undergoing atrial fibrillation ablation. Eur. Heart J. 2018, 39, 2942–2955. [Google Scholar] [CrossRef] [Green Version]
- Cappato, R.; Marchlinski, F.E.; Hohnloser, S.H.; Naccarelli, G.V.; Xiang, J.; Wilber, D.J.; Ma, C.-S.; Hess, S.; Wells, D.S.; Juang, G.; et al. Uninterrupted rivaroxaban vs. uninterrupted vitamin K antagonists for catheter ablation in non-valvular atrial fibrillation. Eur. Heart J. 2015, 36, 1805–1811. [Google Scholar] [CrossRef] [Green Version]
- Nagao, T.; Inden, Y.; Yanagisawa, S.; Kato, H.; Ishikawa, S.; Okumura, S.; Mizutani, Y.; Ito, T.; Yamamoto, T.; Yoshida, N.; et al. Differences in activated clotting time among uninterrupted anticoagulants during the periprocedural period of atrial fibrillation ablation. Heart Rhythm. 2015, 12, 1972–1978. [Google Scholar] [CrossRef]
- Konduru, S.V.; Cheema, A.A.; Jones, P.; Li, Y.; Ramza, B.; Wimmer, A.P. Differences in intraprocedural ACTs with standardized heparin dosing during catheter ablation for atrial fibrillation in patients treated with dabigatran vs. patients on uninterrupted warfarin. J. Interv. Card. Electrophysiol. 2012, 35, 277–284. [Google Scholar] [CrossRef]
- Godier, A.; Dincq, A.-S.; Martin, A.-C.; Radu, A.; Leblanc, I.; Antona, M.; Vasse, M.; Golmard, J.-L.; Mullier, F.; Gouin-Thibault, I. Predictors of pre-procedural concentrations of direct oral anticoagulants: A prospective multicentre study. Eur. Heart J. 2017, 38, 2431–2439. [Google Scholar] [CrossRef] [Green Version]
- Dincq, A.-S.; Lessire, S.; Chatelain, B.; Gourdin, M.; Dogné, J.-M.; Mullier, F.; Douxfils, J. Impact of the Direct Oral Anticoagulants on Activated Clotting Time. J. Cardiothorac. Vasc. Anesth. 2017, 31, e24–e27. [Google Scholar] [CrossRef] [Green Version]
- Calkins, H.; Hindricks, G.; Cappato, R.; Kim, Y.H.; Saad, E.B.; Aguinaga, L.; Akar, J.G.; Badhwar, V.; Brugada, J.; Camm, J.; et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace 2018, 20, e1–e160. [Google Scholar] [CrossRef]
- Kubitza, D.; Roth, A.; Becka, M.; Alatrach, A.; Halabi, A.; Hinrichsen, H.; Mueck, W. Effect of hepatic impairment on the pharmacokinetics and pharmacodynamics of a single dose of rivaroxaban, an oral, direct Factor Xa inhibitor. Br. J. Clin. Pharmacol. 2013, 76, 89–98. [Google Scholar] [CrossRef]
- Frost, C.E.; Ly, V.; Garonzik, S.M. Apixaban Pharmacokinetics and Pharmacodynamics in Subjects with Mild or Moderate Hepatic Impairment. Drugs R&D 2021, 21, 375–384. [Google Scholar] [CrossRef]
- Padrini, R. Clinical Pharmacokinetics and Pharmacodynamics of Direct Oral Anticoagulants in Patients with Renal Failure. Eur. J. Drug Metab. Pharmacokinet. 2019, 44, 1–12. [Google Scholar] [CrossRef]
- Kubitza, D.; Becka, M.; Mueck, W.; Halabi, A.; Maatouk, H.; Klause, N.; Lufft, V.; Wand, D.D.; Philipp, T.; Bruck, H. Effects of renal impairment on the pharmacokinetics, pharmacodynamics and safety of rivaroxaban, an oral, direct Factor Xa inhibitor. Br. J. Clin. Pharmacol. 2010, 70, 703–712. [Google Scholar] [CrossRef] [Green Version]
- Cirincione, B.; Kowalski, K.; Nielsen, J.; Roy, A.; Thanneer, N.; Byon, W.; Boyd, R.; Wang, X.; Leil, T.; LaCreta, F.; et al. Population Pharmacokinetics of Apixaban in Subjects With Nonvalvular Atrial Fibrillation. CPT Pharmacomet. Syst. Pharmacol. 2018, 7, 728–738. [Google Scholar] [CrossRef] [Green Version]
- Leil, T.; Frost, C.; Wang, X.; Pfister, M.; LaCreta, F. Model-Based Exposure-Response Analysis of Apixaban to Quantify Bleeding Risk in Special Populations of Subjects Undergoing Orthopedic Surgery. CPT Pharmacomet. Syst. Pharmacol. 2014, 3, e136. [Google Scholar] [CrossRef]
- Martin, A.C.; Kyheng, M.; Foissaud, V.; Duhamel, A.; Marijon, E.; Susen, S.; Godier, A. Activated Clotting Time Monitoring during Atrial Fibrillation Catheter Ablation: Does the Anticoagulant Matter? J. Clin. Med. 2020, 9, 350. [Google Scholar] [CrossRef] [Green Version]
- Yamaji, H.; Murakami, T.; Hina, K.; Higashiya, S.; Kawamura, H.; Murakami, M.; Kamikawa, S.; Hirohata, S.; Kusachi, S. Activated clotting time on the day of atrial fibrillation ablation for minimally interrupted and uninterrupted direct oral anticoagulation therapy: Sequential changes, differences among direct oral anticoagulants, and ablation safety outcomes. J. Cardiovasc. Electrophysiol. 2019, 30, 2823–2833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weitz, D.S.; Weitz, J.I. Update on heparin: What do we need to know? J. Thromb. Thrombolysis 2010, 29, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Smythe, M.A.; Priziola, J.; Dobesh, P.P.; Wirth, D.; Cuker, A.; Wittkowsky, A.K. Guidance for the practical management of the heparin anticoagulants in the treatment of venous thromboembolism. J. Thromb. Thrombolysis 2016, 41, 165–186. [Google Scholar] [CrossRef] [Green Version]
- Gosselin, R.C.; Douxfils, J. Laboratory Assessment of Direct Oral Anticoagulants. Semin. Thromb. Hemost. 2017, 43, 277–290. [Google Scholar] [CrossRef] [PubMed]
- Douxfils, J.; Ageno, W.; Samama, C.; Lessire, S.; Cate, H.T.; Verhamme, P.; Dogné, J.; Mullier, F. Laboratory testing in patients treated with direct oral anticoagulants: A practical guide for clinicians. J. Thromb. Haemost. 2018, 16, 209–219. [Google Scholar] [CrossRef] [Green Version]
- Macedo, K.A.; Tatarian, P.; Eugenio, K.R. Influence of Direct Oral Anticoagulants on Anti–Factor Xa Measurements Utilized for Monitoring Heparin. Ann. Pharmacother. 2018, 52, 154–159. [Google Scholar] [CrossRef]
- Zeljkovic, I.; Brusich, S.; Scherr, D.; Velagic, V.; Traykov, V.; Pernat, A.; Anic, A.; Nossan, J.S.; Jan, M.; Bakotic, Z.; et al. Differences in activated clotting time and total unfractionated heparin dose during pulmonary vein isolation in patients on different anticoagulation therapy. Clin. Cardiol. 2021, 44, 1177–1182. [Google Scholar] [CrossRef]
- Payne, J.E.; Koerber, S.M.; Bickel, T.; Ghadban, R.; Flaker, G.; Gautam, S. Higher initial weight-based heparin dosing is required with direct oral anticoagulants during catheter ablation for atrial fibrillation. J. Interv. Card. Electrophysiol. 2020, 58, 185–191. [Google Scholar] [CrossRef]
- Briceno, D.F.; Villablanca, P.A.; Lupercio, F.; Kargoli, F.; Jagannath, A.; Londono, A.; Patel, J.; Otusanya, O.; Brevik, J.; Maraboto, C.; et al. Clinical Impact of Heparin Kinetics During Catheter Ablation of Atrial Fibrillation: Meta-Analysis and Meta-Regression. J. Cardiovasc. Electrophysiol. 2016, 27, 683–693. [Google Scholar] [CrossRef]
- Wazni, O.M.; Rossillo, A.; Marrouche, N.F.; Saad, E.B.; Martin, D.O.; Bhargava, M.; Bash, D.; Beheiry, S.; Wexman, M.; Potenza, D.; et al. Embolic Events and Char Formation During Pulmonary Vein Isolation in Patients with Atrial Fibrillation: Impact of Different Anticoagulation Regimens and Importance of Intracardiac Echo Imaging. J. Cardiovasc. Electrophysiol. 2005, 16, 576–581. [Google Scholar] [CrossRef]
- Ren, J.-F.; Marchlinski, F.E.; Callans, D.J.; Gerstenfeld, E.P.; Dixit, S.; Lin, D.; Nayak, H.M.; Hsia, H.H. Increased Intensity of Anticoagulation May Reduce Risk of Thrombus During Atrial Fibrillation Ablation Procedures in Patients with Spontaneous Echo Contrast. J. Cardiovasc. Electrophysiol. 2005, 16, 474–477. [Google Scholar] [CrossRef]
- Hohnloser, S.H.; Camm, J.; Cappato, R.; Diener, H.-C.; Heidbüchel, H.; Mont, L.; A Morillo, C.; Abozguia, K.; Grimaldi, M.; Rauer, H.; et al. Uninterrupted edoxaban vs. vitamin K antagonists for ablation of atrial fibrillation: The ELIMINATE-AF trial. Eur. Heart J. 2019, 40, 3013–3021. [Google Scholar] [CrossRef] [Green Version]
- Benali, K.; Verain, J.; Hammache, N.; Guenancia, C.; Hooks, D.; Magnin-Poull, I.; Toussaint-Hacquard, M.; de Chillou, C.; Sellal, J.-M. Running after Activated Clotting Time Values in Patients Receiving Direct Oral Anticoagulants: A Potentially Dangerous Race. Results from a Prospective Study in Atrial Fibrillation Catheter Ablation Procedures. J. Clin. Med. 2021, 10, 4240. [Google Scholar] [CrossRef]
- Bin Abdulhak, A.A.; Kennedy, K.F.; Gupta, S.; Giocondo, M.; Ramza, B.; Wimmer, A.P. Effect of pre-procedural interrupted apixaban on heparin anticoagulation during catheter ablation for atrial fibrillation: A prospective observational study. J. Interv. Card. Electrophysiol. 2015, 44, 91–96. [Google Scholar] [CrossRef]
- Cappato, R.; Calkins, H.; Chen, S.-A.; Davies, W.; Iesaka, Y.; Kalman, J.; Kim, Y.-H.; Klein, G.; Packer, D.; Skanes, A. Worldwide Survey on the Methods, Efficacy, and Safety of Catheter Ablation for Human Atrial Fibrillation. Circulation 2005, 111, 1100–1105. [Google Scholar] [CrossRef] [Green Version]
- Molteni, M.; Bo, M.; Di Minno, G.; Di Pasquale, G.; Genovesi, S.; Toni, D.; Verdecchia, P. Dabigatran etexilate: Appropriate use in patients with chronic kidney disease and in the elderly patients. Intern. Emerg. Med. 2017, 12, 425–435. [Google Scholar] [CrossRef]
- Strickland, S.W.; Palkimas, S.; Acker, M.; Bazydlo, L.A.L. A Novel Laboratory Assay to Monitor Unfractionated Heparin Dosing in Patients Taking Apixaban Prior to Hospital Admission. J. Appl. Lab. Med. 2021, 6, 378–386. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Variables | Cohort (n = 40) |
|---|---|---|
| Demographics | Sex (Male) | 22 (55) |
| Age (years) | 68 (55–71) | |
| BMI (kg.m−2) | 27 (24–31) | |
| CHA2DS2-VASC score | 2 (0–3) | |
| eGFR mL.min−1.1.73 m−2 | 75 (62–91) | |
| Type of heart rhythm disorder | Paroxysmal AF | 24 (60) |
| Persistent/permanent AF | 16 (40) | |
| Left ventricular ejection fraction (%) | 65 (56–70) | |
| Indexed left atrium surface (mL.m2) | 47 (38–62) | |
| DOAC treatment | Rivaroxaban | 15 (37.5) |
| Apixaban | 20 (50.0) | |
| Dabigatran | 5 (12.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muller, M.; Godet, J.; Delabranche, X.; Sattler, L.; Millard, D.; Marzak, H.; Mertes, P.M.; Steib, A.; Grunebaum, L.; Jesel, L.; et al. Study of Modifications Induced by Continued Direct Oral Anticoagulant Therapy during Atrial Fibrillation Ablation Procedures on Standard Hemostasis Parameters. J. Clin. Med. 2023, 12, 2236. https://doi.org/10.3390/jcm12062236
Muller M, Godet J, Delabranche X, Sattler L, Millard D, Marzak H, Mertes PM, Steib A, Grunebaum L, Jesel L, et al. Study of Modifications Induced by Continued Direct Oral Anticoagulant Therapy during Atrial Fibrillation Ablation Procedures on Standard Hemostasis Parameters. Journal of Clinical Medicine. 2023; 12(6):2236. https://doi.org/10.3390/jcm12062236
Chicago/Turabian StyleMuller, Marie, Julien Godet, Xavier Delabranche, Laurent Sattler, David Millard, Halim Marzak, Paul Michel Mertes, Annick Steib, Lelia Grunebaum, Laurence Jesel, and et al. 2023. "Study of Modifications Induced by Continued Direct Oral Anticoagulant Therapy during Atrial Fibrillation Ablation Procedures on Standard Hemostasis Parameters" Journal of Clinical Medicine 12, no. 6: 2236. https://doi.org/10.3390/jcm12062236